





Impact of COVID-19 on Post-Viral Conditions Management
The impact of COVID-19 on the understanding, management and treatment of post-viral conditions
Introduction
The COVID-19 pandemic in its initial phase presented as a huge risk to the world population with serious illness and death following Severe Acute Respiratory Syndrome-Coronavirus-2 (SARS-CoV-2) infections. The aim of the following discussion is to highlight the importance of public health measures and successful vaccine development in reducing the impact of these devastating effects and in managing the pandemic and post-viral conditions that arose. As the pandemic progressed it became clear there were serious ongoing post-viral effects from the SARS-CoV-2 virus infection in susceptible people. These were heterogeneous and were given the generic name of LONG COVID (LC). The growing knowledge of the characteristics and pathophysiology of LC are discussed here together with how the condition might be managed. Since about half the cases of LC resemble the post-viral/stressor syndrome known as Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS), the growing evidence for the close relationship between these two conditions is evaluated. As the COVID-19 pandemic has now seemingly become endemic, it is still generating continuously many cases of debilitating LC, and the need for continuing public health measures is highlighted to keep the infection rate low and thereby limit new cases of LC. Emphasised is the need to maintain the intense research investment and effort arising with the appearance of LC, aimed at finding treatment options that can give a better quality of life if not a cure for patients. The goal of being able to permanently reverse the aberrant physiology of these post-viral conditions and their regulation, now with >100million affected worldwide, should not be lost.
The pandemic
The COVID-19 pandemic has been unprecedented in human history in the number of people infected from all cultures and countries. To date almost 776 million COVID-19 infections have been reported worldwide¹ and from those has arisen an estimated 60 million cases of a post-viral debilitating syndrome generally now referred to as (LC)²˒³. The extent and rapidity of the SARS-CoV-2 spread in 2020 posed immediate challenges with high fatalities within older people in high risk housing complexes like rest homes⁴, and in the number of severe cases requiring hospitalisation and specialist treatment, overburdening many health systems even in highly developed countries⁵. It was unknown whether it would be possible to counter the devastating effects of the SARS-CoV-2 virus by developing effective vaccines and/or antivirals as powerful tools to complement sound public health measures. Fortunately highly innovative scientists among the developed world were able to draw on their ongoing work to mount a multipronged attempt to produce different vaccine types⁶, and to repurpose⁷˒⁸, and to develop new antivirals⁹ to blunt the worst effects of the SARS-CoV-2 virus.
The challenge of producing an effective vaccine
In 2020 many deaths from COVID19 were being reported worldwide initially at a rate of ~1.7% of the infections; there were graphic images of hospitals in major cities overwhelmed with patients, which required emergency storage of the bodies of the deceased. Treatments to prevent deaths and lower hospitalisation rates were desperately needed, and yet it was well known producing effective vaccines against coronaviruses had previously been incredibly challenging¹⁰˒¹¹. The time required to produce vaccines in the huge quantities that were needed, to test their effectiveness, and to validate their safety in test populations – in this case against COVID19 – seemed to be an impossible task to be able to provide immediate benefit. Yet remarkably within a relatively short time many potential vaccines were developed, including a new type using delivery of mRNA encoding the immunogen, as well as some delivering the viral spike protein directly as the antigen. Those that met the safety and efficacy criteria became available as choices for countries to mount their mass vaccination campaigns. Despite this, hoarding of large amounts (several fold over requirements) in some developed nations left a shortage for those in the developing world. An important lesson and challenge from this pandemic, to aid in the preparation for future pandemics, is the need for a universal worldwide treaty with obligations on all signees to guarantee wide and fair access to vaccines and other resources¹²˒¹³.
It was the success of the new class of vaccines based on messenger ribonucleic acid (mRNA) delivery that has revolutionised our thinking on vaccine production, now post-COVID, providing an exciting opportunity for application to widespread, or boutique endemic infections, as well as for existing diseases. Already development of an Ribonucleic acid (RNA) vaccine against a highly pathogenic clade of bird flu (avian influenza virus) has been achieved¹⁴ and there is intense activity underway on several other fronts. The speed of the production of mRNA vaccines, and the ease by which the mRNA can be modified to combat new variants as they arise, was fortunately complemented by both their relative safety and relative efficacy for those developed against COVID19. This predicts an exciting future for successful vaccine production.
An extra potential biological safety feature provided by mRNA vaccines is the ability to restrict high concentrations of an immunogen circulating within the blood that could have damaging effects. For example, the SARS-CoV-2 spike protein binds to the human Angiotensin Converting Enzyme 2 (ACE2) receptor and enhances its carboxypeptidase activity¹⁵ thereby affecting control of vasodilation and vascular permeability. With the RNA vaccines the antigen itself would be produced within the muscle cells around the injection site¹⁶ after translation from the specific mRNA. The mRNA has a limited lifetime, despite having been produced for vaccine development with stabilising modifications to extend its half life to a few days. The result of limited controlled production of the foreign antigen that the immune system could rapidly respond to and degrade suggested free circulation would be limited. Indeed, a study of vaccinated subjects who had no adverse reactions did not detect the spike protein in plasma. By contrast, the damage of relatively high concentrations of antigen in plasma unbound to antibodies was demonstrated in rare cases of patients who developed post-vaccine myocarditis¹⁷. Unfortunately, even with such successful vaccines that passed their safety tests showing a very low frequency of adverse reactions, with so many of the world’s population receiving the vaccine, the absolute number of rare adverse acute reactions like anaphylaxis and myocarditis was significant. More challenging was to highlight prior to vaccination those vulnerable groups with co-morbidities that might experience chronic ongoing debilitating effects on their health from the vaccines themselves.
Impact of the vaccines and opportunities for the future
The gold standard of hope was that the vaccines, RNA based or otherwise, would prevent COVID-19 transmission, give long lasting protection, and thereby prevent deaths and hospitalisations. For most of world’s population who could get access to the vaccines there were significant benefits as seen by the reductions in the incidence of the severe effects. A recent report on hospitalisation and fatality rates pre-vaccination in the United States deduced a hospitalisation rate of 5.7% and fatality rate of 1.7%¹⁸. A comparison of rates of these outcomes between vaccinated and non vaccinated people in 13 US states between January 2001 and April 2022 showed vaccination with three doses gave over 10-fold protection from hospitalisation, and 2.5-fold if there was no third booster, indicating the strong effect of vaccination¹⁹. After the multi dose vaccination campaigns, the cumulative fatality rate from COVID-19 infection has dropped worldwide to around now ~7 million of ~776 million reported cases¹. Perhaps surprisingly, in the 28 days of June 2024 there was a higher apparent death rate (1860 from 126,316 reported cases), but it is acknowledged there is now a significant under-reporting of infections, both because some countries are no longer reporting, and because there are less stringent reporting practices.
in those countries still collecting data so that many people with only mild symptoms not requiring clinical care no longer report their infection.
This achievement of vaccination containment led to Katalin Kariko and Drew Weissman being awarded the Nobel prize in Medicine in 2023 among many other awards for their groundbreaking developmental work on RNA vaccines that was exploited in this time of dire need²⁰.
What was less clear was the extent to which the vaccines protected against transmission from infected people, for example within families. A systematic review of 42 studies comparing the efficacy of seven COVID-19 vaccines²¹ suggested the vaccines did indeed provide benefit against COVID-19 infection for the early variants, at least for a period of time. By contrast, peak viral titers in the upper airways of the lungs have been reported as similar between vaccinated and unvaccinated individuals infected by these early variants in several studies²². While the evidence is somewhat confusing, key factors for this paradox may have been the evolution of the new variants, and/or the waning of the immunity with time.
A challenge for the future that arises is that the SARS-CoV-2 virus shows no signs of becoming dormant and has now become endemic with mini-waves of fluctuating rates of infection still frequently occurring²³. Therefore understanding whether it was the waning efficacy of the vaccine that could no longer invoke an effective immune response to prevent transmission, and/or the arrival of new variants that were less effectively neutralised, was important. New variants might be able to escape high efficacy protection from a vaccine raised to the specific spike protein sequence of the initial strains. This raised the question of whether it would require frequent production of new modified vaccines to match the rather high frequency of change observed of a new dominant variant? From April 2024, nearly all SARS-CoV-2 sequences in public data bases were derived from the JN.1 strain and the World Health Organisation (WHO) has advised “the use of a monovalent JN.1 lineage as the antigen for future formulations of COVID-19 vaccines”²⁴.
The experience in New Zealand (NZ) is that JN.1 and sub variants of it have rapidly become the predominant strain currently. As well, a significant proportion of those vaccinated have now become infected. Over 4.3 million (>95% of those of appropriate age) were vaccinated with multiple doses, the vast majority prior to infection. Now over half the population have since been infected or re-infected with the new variants, and reinfections make up a significant proportion of the new cases each week²⁵. For example, in a week in June 2024 during a new COVID-19 mini-wave there was a reported 4700 new infections of which 72% were re-infections, 385 of those were in hospital, and there were 45 fatalities with COVID-19 for the week. Internationally, Hall et al studied 35,000 highly vaccinated (97%) participants, 27% of whom had had a prior infection²⁶. Importantly, in the vaccinated group not previously infected they found protection from two doses of vaccine waned considerably after 6 months although immunity of those previously infected was boosted by such vaccination and was still high >1 year after infection. These data are consistent with the evidence that the degree of protection against SARS-CoV-2 re-infection, hospitalisation, and mortality by COVID-19 vaccines reduces over time²⁷.
Immune imprinting is a phenomenon where prior exposures to immunogen influences subsequent responses to infection or vaccination²⁸˒²⁹. Recently it has been shown when the original vaccines were used as a booster at a time of new variants, they invoked antibody responses from the historical immunisation that were against the new variant thereby driving expansion of cross neutralizing antibodies that provided more widespread protection³⁰. This provides some hope that producing vaccines against every new variant might not be so critical in the future and that new infections might not be so damaging.
For the 5-10% of the population who have genetic or co-morbidity susceptibility to develop Long COVID (LC), new infections are still likely to continue to generate this debilitating ongoing post-viral condition at a significant frequency despite the vaccinations. Early studies were contradictory whether vaccination was providing some protection against LC and lowering the rates of its occurrence. Very recent data³¹ perhaps resolves that paradox as rates of LC were similar in unvaccinated (8.4%) and people vaccinated with 2 doses (8.7%) but reduced in those who had had a third vaccination booster (5.8%). Hence, vaccination seems to provide some protection against the post-viral condition but with the significant number of infections still occurring, even in this reduced phase of the pandemic, new LC cases are occurring in significant numbers to add to the world burden of this disease. On these rates reported by Fang et al,³¹ the Long COVID case load worldwide currently would be between 45-66 million but are likely significantly under reported. A very recent study³² examined the records >400 000 US veterans who had infection during the period March 2020 to February 2022 to deduce the comparative rates of developing LC from the original COVID-19 strain, the subsequent delta variant and the omicron variant that spanned this time frame. Encouragingly at one year post infection in the unvaccinated group the rates declined from 10.4% (original) to 9.5 % (delta) to 7.7% (omicron), and in the vaccinated the rates were 5.3%(delta) and 3.5 % (omicron). These trends are very encouraging not only from the progressively lower rate with newer variants, but also the effectiveness of the vaccination to lower the rates even further. Nevertheless, the authors emphasised with the large numbers still getting infected with COVID-19 the risk is not trivial and reinforced the conclusion that a high absolute number still becoming affected by LC remains, adding to the health burden.
Tolerance of at risk people for the protective vaccine
Most people had no more than a sore arm after vaccination, while others suffered reactions like chills, fatigue, headaches and generally were feeling quite unwell for a few days. A study of those vaccinated with two doses of the Pfizer mRNA vaccine highlighted that this group had higher levels of neutralising antibodies of 1.4 and 1.6-fold at 1 and 6-months after vaccination. So this short term mildly uncomfortable symptom response was a positive feature of the efficacy of the vaccination for those individuals³³. There were also some rare acute adverse reactions that became more obvious with the sheer number of vaccinations given. Those presenting with acute life-threatening symptoms in general were recognised and could be managed immediately by a clinical response, but more difficult to manage were chronic ongoing reactions in vulnerable population subgroups that were debilitating but not life threatening. Patients reported responses from public health systems to these reactions tended to be dismissive of their condition being connected to the vaccination, adding to the difficulties of those affected to manage their condition as best as they could without good clinical support. This is summarised in Figure 1.
In the phase III clinical trials of the Pfizer and Moderna mRNA vaccines there was a rare risk of serious adverse events documented of 10 and 15 per 10 000 subjects vaccinated respectively³⁴. Thrombosis was most frequent, but strokes, myocarditis, myocardial infarction, pulmonary embolism, and arrythmias. Rarer transverse myelitis and disseminated encephalomyelitis and other severe neurological complications were also documented as well as non life threatening chronic debilitating effects³⁵˒⁴¹.
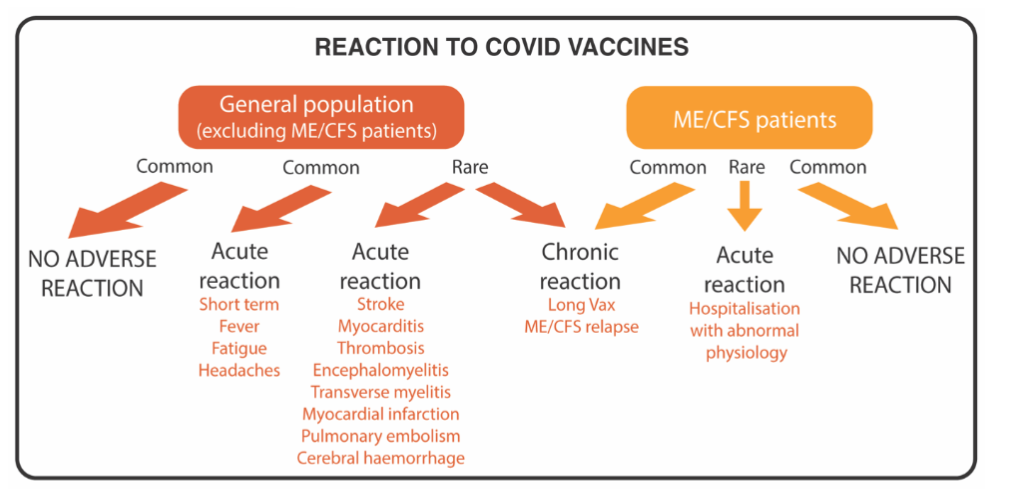
Figure 1. Reactions of the general population and those with a previous post-viral condition to the COVID vaccines. Most in the general population had only transient discomfort but rarely there were acute responses requiring medical attention. In ME/CFS patients a chronic adverse reaction with a significant worsening of their condition was common.
Vaccination has been known prior to COVID-19 to lead to the onset of a post-viral/stressor-like condition mirroring ME/CFS in a small group of susceptible people. Therefore it was not unexpected that there might be similar cases arising from the COVID-19 vaccination programme among apparently healthy individuals (see Figure 1). Indeed onset of chronic debilitating symptoms of an ME/CFS-like condition has been reported and called post-COVID-19 vaccination syndrome (PACVS)³⁶˒⁴⁴. The term Long Vax has also been coined for this condition as it has gradually gained more acceptance among scientists and clinicians, but is often now also referred to as vaccine-caused LC. The evidence for such a ‘Long Vax effect’ has been more clearly demonstrated in people already suffering from the post-viral fatigue condition ME/CFS (indicated as separate group on the right side of Figure 1). They have proved to be highly susceptible to a significant worsening of their condition, as if the vaccination is boosting a serious relapse of their pre-existing illness⁴⁵. Similar ME/CFS patient surveys completed in the United States reported frequencies of adverse reactions as high as 1 in 3 that were ongoing⁴⁶.
The challenges of post COVID health effects
Chronic health problems following COVID-19 infections are now presenting as a major ongoing challenge as we continue to live with the SARS-CoV-2 virus seemingly permanently entrenched as an endemic. There are two aspects to LC (a) organ damage occurring at the time of infection that manifests itself as a chronic consequential health issue, for example a debilitating respiratory condition particularly after infection with the early alpha and delta variants and prior to vaccination, and (b) a classic example of a post-viral fatigue syndrome from this specific virus. Additionally there is an increased susceptibility to develop other conditions, for example, the incidence of heart attacks has increased 2-fold, lung failure 4-fold, and type-2 diabetes by 1.5-fold⁴⁷.
Long COVID as originally defined encompasses the first two groups of patients but it is important to distinguish them so that each subgroup can be treated appropriately. Several significant issues must be faced: understanding (a) the subgroups falling within LC, (b) in depth the pathophysiology of each subgroup, (c) what makes the 5-10% susceptible to developing the post-viral fatigue syndrome, (d) why some people with no ongoing health problems post-COVID infection are now showing susceptibility to develop co-morbidities like diabetes, heart disease, and lung disease arising some time later, and what determines that this subgroup of people are particularly susceptible.
For the post-viral fatigue ME/CFS-like subgroup of the LC patients alone there are important issues to resolve (a) how some people recover within 1-2 years (b) why others have their condition entrenched long-term like ME/CFS patients, (c) developing treatments to provide at least a better quality of life for these long term patients, (d) understanding whether treatments have to be personally tailored to each patient, given that in ME/CFS patients potential therapies have shown the range of some benefit, no benefit or, a negative effect with individual ME/CFS patients, (e) elucidating a way by which the condition might be reversed.
The heterogeneity of Long COVID
Since the observation of ongoing health problems in some people after COVID-19 infection, the popular term Long COVID (LC) became inclusive for all of those now in poorer health. That meant they were a heterogeneous group. The World Health Organisation moved quickly and decisively to derive a clinical case definition for LC. One consequence in this process was by selecting out the most frequently experienced symptoms of the now over 200 different symptoms reported by patients, minor subgroups with a particular symptom profile would be excluded. Indeed the clinical case definition that emerged was very similar to that derived for ME/CFS, suggesting the ‘ME/CFS – like post-viral fatigue syndrome’ was likely the dominant subgroup⁴⁸. In the conclusions of the WHO report it was stated “as new evidence emerges and our understanding of the consequences of COVID-19 continues to evolve the definition would likely change”⁴⁸.
Recently, four clinical phenotypes were proposed from a study of a cohort of 1800 patients; as inferred from the WHO clinical case definition, the dominant phenotype was an ME/CFS-like syndrome (~42%), then a respiratory syndrome most likely from damage to the lungs at infection from the early variants (23%), a chronic pain syndrome, which can be found in ME/CFS but more accompanying severe pain falls within the diagnosis of fibromyalgia (22%), and a neurosensorial syndrome of loss of taste and smell (11%) – a feature specific to the SARS-CoV-2 virus⁴⁹.
Without differentiation of research cohorts of LC into such distinct subgroups for studies to understand the pathophysiology and derive potential beneficial treatments, there is the risk that different compositions within cohorts used in studies could generate inconsistent findings. Complicating this, is that the > 200 symptoms reported by ME/CFS patients whose condition arose from multiple different triggers overlapped by ~95% with those identified in LC despite the specificity of there being a single trigger virus for LC⁵⁰. Moreover, patient to patient variation has been found in the molecular changes that underpin the ME/CFS syndrome, even those with very similar symptom profiles⁵¹, suggesting symptom variation among patients was not determined primarily by the viral or stressor trigger but rather arose from the genetic profile of each individual patient. Hence each patient in a sense forms their own clinical phenotype. Despite this, it would still be hoped to be able to classify patients into a small number of subgroups. This can explain why it has been so difficult to develop any treatments for those suffering from ME/CFS that can benefit the majority. Promising targeted therapies have affected some patients positively, some negatively, and many not at all. There is the same challenge for LC patients who have the ME/CFS-like phenotype.
Understanding what makes a person susceptible to developing Long COVID
This section relates to the ME/CFS-like phenotype of LC. A quantitative survey we carried out on the first cohort of LC patients in New Zealand, showed prior health history of a highly stressful event seems to prime susceptibility. This could include a previous infection with Epstein-Barr virus that was difficult to recover from, a reaction to a vaccination that required several months to recover from, or a deeply traumatising emotional stress event⁵⁰. Additionally, a wide range of co-morbidities are a risk factor for developing LC⁵². There was also a significant familial connection with multiple members of a family developing the condition⁵⁰. There were families who reported multiple members with ME/CFS and/or other fatigue conditions. Additionally the inability to recover in the normal time frame from childhood illnesses, and their frequency seemed to signal susceptibility and that could also be explained by genetic factor(s). These observations are summarised in Figure 2A.
Linkage of genetic factors to the development of ME/CFS have been poorly understood until very recently. Genome Wide Association studies (GWAS) had failed to detect strong links between specific genes and ME/CFS. However, an advance in the GWAS technology with addition of a combinatorial platform by Precision Life in Oxford has enabled small clusters of single nucleotide polymorphisms (SNPs) in combination to be linked to ME/CFS as shown in Figure 2. Fifteen clusters of 3-5 SNPs linked to 14 genes, relevant to cellular mechanisms dysfunctional in ME/CFS, could account for 91% of the samples from ME/CFS patients in the United Kingdom Biobank⁵³. A follow up paper examining several cohorts of Long COVID gave more complex results – with 73 genes linked to the condition but 39 of the SNPs detected were also linked to 9 of the genes identified in the ME/CFS study⁵⁴.
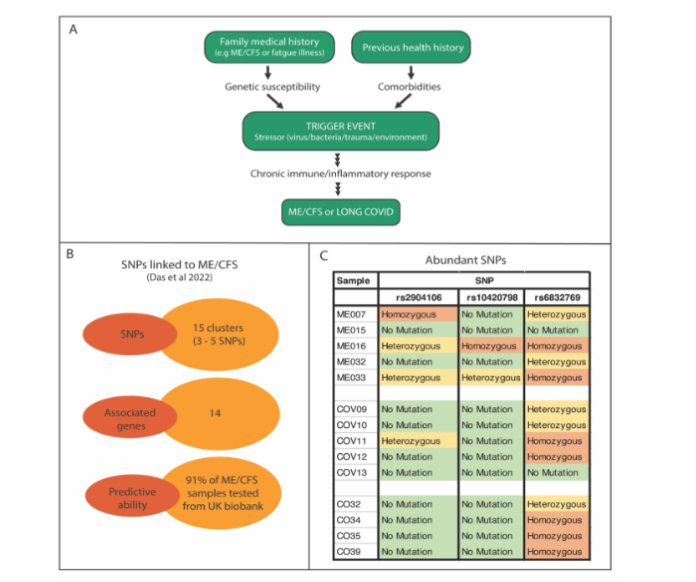
Figure 2. Factors determining susceptibility to developing Post – viral conditions.
A. Silent genetic susceptibility and personal health history, that may involve the development of co-morbidities, can prime individuals for developing the post stressor/viral fatigue condition ME/CFS after a major stress event/viral infection or with LC in response to SARS-CoV-2 infection.
B. The results reported by Dass et al⁵³ using a new combinatorial platform together with a Genome Wide Association Screen (GWAS) with ME/CFS patient samples.
C. Frequencies of three of the most abundant SNPs in small cohorts of ME/CFS, LC and Healthy controls (Griffiths and Tate unpublished).
This provides an exciting opportunity and challenge to determine whether it is possible to develop a readily accessible genomic signature utilising a fraction of the SNPs identified that could be a predictor of susceptibility in families, where there is already a member affected. We have determined whether the 5 most frequently found SNPs reported in the ME/CFS patient samples from the 15 clusters of 3-5 SNPs⁵³ were enriched singly or collectively in small sample cohorts of ME/CFS and LC over healthy controls; two SNPs were found only in some of the ME/CFS patients, but for the other three they were found at the same frequency in all groups, with a common SNP illustrating this (Figure 2C). Not surprisingly, these SNPs are all relatively common variations in the general population. If a combination of SNPs in an affected family member were sufficient to form a ‘family signature’, albeit that might vary from family to family, then identifying at risk members within the family might be possible. Prophylactic measures could then be taken within those at risk when they were exposed to a major stressor event or a viral outbreak to lower the probability of developing the post-event condition. Indeed some ME/CFS clinicians took such measures during the vaccination campaign to protect their ME/CFS patients from adverse reactions utilising antihistamines to prevent mast cell activation, and in some cases steroids, with apparent beneficial outcomes.
Pathophysiology of the subgroups of Long COVID
Using the Gentioltti et al 2023 classification⁴⁹ the respiratory syndrome characterised by coughs and dyspnoea (shortness of breath) has focussed symptoms that can be attributed to some damage to the lungs from COVID-19 infection. The chronic pain syndrome clinical phenotype involved arthalgia (joint pain) and myalgia (muscle pain) as the dominant symptoms. These forms of pain occur from multiple causes, but may be underpinned by ME/CFS-like symptoms, as in fibromyalgia, where there is widespread musculoskeletal pain but also by fatigue, sleep dysfunction, brain fog, and mood fluctuations. The ME/CFS-like subgroup of LC, as described above, has a complex plethora of symptoms. We have proposed holistic models⁵⁵ to explain how ME/CFS and LC develop, starting with a failure of the peripheral immune inflammatory response to move out of the transitory phase so that instead the response becomes chronic. There can be an inflammatory reflex where afferent neurons sense this state and communicate to the brain for activation of the separate immune/inflammatory system of the central nervous system, or the communication could be via a disturbed blood brain barrier, or vascular gateway reflex through a specific blood vessel. Neuroinflammation has been shown to occur in the brain in both LC and ME/CFS, and classic neurological symptoms appear affecting fatigue, sleep, cognition and memory (brain fog). There is then disruption to the precise regulation of body physiology (blood pressure, heart rate, temperature, blood sugar, and the gastrointestinal system)⁵⁵. A dysfunctioning stress centre in the paraventricular nucleus of the hypothalamus we postulate explains why the affected person is very sensitive to even small daily stresses and subject to relapses⁵⁸. It can then be interpreted that daily minor stresses sustain the disease so it is ongoing. Much research is now underway trying to fill in the gaps and explain the detailed mechanisms underpinning these major symptoms, particularly in LC.
Understanding and treatment of Post-viral fatigue syndromes
The rapid appearance of many cases of LC worldwide from the COVID-19 pandemic simultaneously since 2020 has provided an opportunity to understand in depth the post-viral conditions that have been with us throughout history. The first evidence of their occurrence can be dated back to descriptions of Hammurabi, a Babylonian philosopher of the eighteenth century BCE. Prominent people in history like Florence Nightingale, the ‘mother of nursing’ and Charles Darwin, have been suggested to have suffered from a similar condition⁵⁹. In the last 100 years there have been ~70 reports of “boutique” outbreaks of infectious disease that have given rise to post-infection fatigue syndromes. Each was geographically isolated, and with relatively small numbers of cases, those developing the post-event conditions were modest and so did not result in high interest among the clinical and scientific communities, nor significant investment in research. Nevertheless, the numbers of people affected world wide have gradually accumulated by stealth as the vast majority of people (~95%) diagnosed with these complex conditions have a fluctuating array of debilitating symptoms for the duration of their lives⁶⁰. It was estimated that there were 20-30 million people worldwide affected with ME/CFS before the appearance of LC.
A bewildering list of at least 34 different names have been given to the condition we now group under the collective name of ME/CFS. After a 1955 outbreak in London the post-infectious disease condition was called Myalgic Encephalomyelitis (ME), the name by which it became known in Europe, Canada, and Australasia. It has now become linked with the name Chronic Fatigue Syndrome (CFS) that was commonly used in the United States⁶¹. The same complex symptomology can occur from external toxic assaults on the body other than infectious agents such as from an agricultural chemical, or a major life stress event. This implies the complexity of the condition arises from a chronic reaction in a susceptible person trying to counter a major assault whatever the stressful trigger might be.
In 2015 The Institute (now Academy) of Medicine of the United States Academy of Sciences⁶² published an extensive report on Chronic fatigue Syndrome (CFS) concluding it was a serious condition that warranted much more attention from clinicians, and social support for patients and their carers. The name CFS was inferred to underplay the seriousness of the syndrome, and a new name, Systemic Exercise Intolerance Disease (SEID) to give the condition ‘gravitas’ was put forward in this expert report. While this ‘35th proposed name’ has not been generally used, and particularly by patients, the report was critically important in raising the public profile of ME/CFS in the US such that in 2019 the senate recognised it as a serious disease, and affirmed a commitment to support research, medical education, and promote public awareness. The importance of those health care professionals and medical researchers working to discover the causes, and working towards, diagnosis, treatments, and a cure for ME/CFS was affirmed. May 12th was recognised as International ME/CFS awareness day.
Medical education profiling ME/CFS within medical schools, even in the highly developed countries, has been sporadic so that many clinicians had limited understanding of post-viral conditions when COVID-19 arrived. For example, in the United Kingdom, of 22 medical schools that responded to a survey out of 34 contacted requesting information, only 13 taught ME/CFS but by 6 different clinical disciplines so that different perspectives of the disease were delivered at different locations⁶³.
This greater awareness of ME/CFS that had evolved just before the appearance of COVID-19, a uniquely widespread infectious disease event that suddenly generated large numbers of post-viral cases from its single viral trigger. The welcomed financial support that had been committed for research of ME/CFS just prior to COVID-19 was dwarfed by that committed by the US Congress for the ‘Recover initiative’ of the National Institutes of Health⁶⁴, with over a billion dollars given in December 2021 to find the causes and develop treatments for LC, and now in 2024 an additional half billion dollars. For the first time this would allow definitive clinical trials to be carried out on promising potential therapies. There were high but perhaps unrealistic hopes among patient groups of rapid advances in understanding and providing treatments for LC that would also be relevant to ME/CFS but, so far many of those affected have been disappointed with the progress, and with their own expected engagement, as living experts of their own illness.
Patient-inspired not for profit organisations like ‘Patient Led Research Collaboration’ (PLRC) have now been founded to provide more patient focus and funding for patient-relevant research⁶⁵. Another non-profit organisation, The Open Medicine Foundation has raised many millions of dollars to support collaborative research, which includes their first clinical trial, the Life Improvement Trial (LIFT), of two promising drugs: the anti neuroinflammatory Low Dose Naltrexone and the vagus nerve enhancer Pyridostigmine (aka Mestinon), both singly and in combination⁶⁶. So the promise still is that the LC research initiatives will give a huge boost to our understanding of how to control the debilitating effects of post-viral/stressor conditions and generate effective treatments so that those affected will have a much improved quality of life and be enabled to play a fuller part in their families and communities.
The benefit of Long COVID research for ME/CFS patients
A key question is whether ME/CFS, and the known characteristics of its pathophysiology elucidated so far, is a suitable model to give us insight to understand at least the ME/CFS-like syndrome representing ~50% of LC cases. Conversely, and importantly, will ME/CFS patients in reality benefit from the findings of the Recover initiative and the subsequent clinical trials now beginning, and those from the patient-consortiums arising from the current research effort targeted at LC. Underpinning these questions is whether the physiological response in susceptible people to the SARS-CoV-2 virus is similar or markedly different from their responses to the diverse range of triggers that lead to ME/CFS?
An excellent pointer comes from a comparison of the wide array of > 200 symptoms reported by both groups of patients. For example, while the loss of taste and smell, breathing difficulties, skin problems and effects on the voice (of singers) are more predominant in the LC syndrome, most of the 200 symptoms overlap between the two conditions. There seems to be a much lower incidence of gastrointestinal disturbances like irritable bowel syndrome in this relatively early stage of LC than in later stage ME/CFS. Indeed several authors have referred to LC as becoming ME/CFS if it lasts beyond 2 years⁶⁷. This implies, since LC has been with us for only 3-4 years, it might present biologically currently as a juvenile form of ME/CFS since the mean time of those affected with ME/CFS would be >10 years. Comparative studies of the two conditions, unless able to assemble cohorts of early stage ME/CFS to match the LC time length of their condition, must always have this factor as a limitation of their conclusions.
Nevertheless, evidence-based predictions suggest the likelihood that ME/CFS and LC will be mutually beneficial in setting the priorities for productive future studies⁶⁶˒⁶⁷. Jason and colleagues have outlined “what LC investigators can learn from four decades of ME/CFS research”⁷⁰. Komaroff in his talk at the 40th anniversary of the Massachusetts ME/CFS and FM in 2022 (his interest in ME/CFS spans this time) also strongly affirmed the similarity between the ME/CFS and LC and that ME/CFS will most likely benefit from the intensive activities to understand LC⁶⁷. Supporting this view, he listed a wide range of biological dysfunctions in common between the two conditions: dysautonomia, generation of autoantibodies, switch in energy generation, low energy/hypometabolic state, increased oxidative stress, mast cell activation, abnormal cardiopulmonary responses to exercise tests, blood vessel/coagulation disturbances, Epstein Barr virus and other herpes viral reactions, small fibre neuropathy, cognitive dysfunction, disturbed HPA axis, neuroinflammation, and gut microbiome changes. Those affected with the ME/CFS-like LC syndrome experience the same core defining symptom of ME/CFS Post-exertional malaise but some differences in expression that were attributed to the early stage of the condition in LC⁷¹.
Comparative studies of molecular changes found in LC and ME/CFS are re-inforcing those predictions. For example, our study of DNA methylome changes between ME/CFS and LC signalling gene expression changes (Peppercorn et al unpublished) have identified 13 sites in the genome where every patient within the small cohorts of both conditions showed differential methylation compared with age/gender matched controls and all were in the same direction whether hypo- or hypermethylated (Figure 3A). Three cases of hypomethylation and ten cases of hypermethylation in both conditions are shown when compared with healthy controls. The conclusion was that the changes likely caused the same change in gene regulation in ME/CFS and LC.
Figure 3. Changes in regulation at specific sites in the DNA methylome and the proteome of ME/CFS and Long COVID.
A. The 13 genomic sites where methylation changes have occurred in every patient of the ME/CFS and LC cohorts (5 patients each) compared with 5 healthy controls. Three show hypomethylation, and 10 hypermethylation.
B. Twenty one examples of the many differentially regulated immune cell proteins in LC and ME/CFS illustrating up or down regulation in common, but also in the opposite direction in the two conditions.
Our comparative study of immune cell proteins also identified a group of differentially regulated proteins in immune cells in common to both ME/CFS and LC patients. In most cases the proteins were up or down regulated similarly but in a minority of cases the differential regulation occurred in opposite directions (an illustrative subset are shown within Figure 3B). There were more differentially regulated proteins overall in the ME/CFS patient group study (346) whose illness had lasted on average 16 years, than the LC patients study (146) with an illness duration of 1 year, and that likely reflected the stages of illness of the two conditions. Nevertheless, the differentially regulated proteins identified reflected similar molecular pathways like mitochondrial functions linked to energy production (54 in ME/CFS and 21 in LC), immune system processes and cytokine regulation (83 in ME/CFS and 37 in LC).
overlapping clusters in both cases were also found among proteins related to gene expression. The conclusions from this study were that the two conditions have similar dysfunctions in their immune physiology as a prominent feature and, in both, energy production was also significantly affected⁷². The unique differences might reflect the relatively earlier stage of the LC illness or reflect the unique footprint from the SARS-CoV-2 infection.
Public health issues arising from a pandemic now downgraded to an endemic
At the height of the pandemic in NZ there were daily TV briefings from the Prime Minister and the Director General of Health giving updates on the effects of the pandemic and advocating for strong public health measures. Coupled with emergency border closures and quarantine restrictions to detect cases as they entered the country, this saved many lives among our elderly in rest homes and in the community in general, and remarkably resulted in a 95% approval rating for the Prime Minister’s actions, at least for a period of time that allowed for a comprehensive vaccination strategy to be implemented that protected ~95% of the population. A national programme was instituted to monitor not only the infections through wide spread testing of patients and of waste water that allowed an understanding of the dynamics of new viral variants as they arose.
Restrictive measures however, could only be kept in place for a finite period to ensure population compliance. The challenge then has become how to contain the ongoing waves of SARS-CoV-2 infections to prevent a significant secondary public health crisis within a population who craved for normality. When daily messaging from the leadership stopped, so did public attention to the remaining recommended health measures like mask wearing on public transport, and avoiding large gatherings that acted as nuclei for new outbreaks. Of course the majority of the population has had COVID-19 now, and most recovered from it apparently without ongoing negative health outcomes, and some have been infected multiple times. New infections are generally being treated like ‘an annoying flu’ that is tolerated among this majority, but to the susceptible group who have become new cases of LC it presented a totally different threat to their well being.
Can this understandable reaction signal that there will be ongoing waves of people developing chronic disease as SARS-CoV-2 settles into becoming a year long endemic virus, not only with the ME/CFS-like condition but also with the silent increased risk of diabetes, heart disease, kidney problems and neurological disorders? The stark reality is in NZ now with up to 5000 reported new cases of COVID-19 there would be expected to be 250 new cases of LC.
Even for the developed economies this likely will present a struggle for their health services to provide appropriate care, sufficient specialist clinics, and specialist clinicians. Clinical coding of LC in the UK between 2020 and 2023 has been shown to be very low, limiting the identification of actual cases for appropriate treatment⁷³. A citizen science approach whereby those affected by LC can direct a patient needs-based research agenda has been explored⁷⁴. For those in lower middle income societies, their public health sectors will not have the capacity and the breadth of clinicians with the knowledge and medical education to ensure good health care for those severely affected. This has been documented and described as a hidden public health crisis⁷⁵. Despite the lack of studies, the evidence suggests the incidence of LC is the same as in the wealthier countries, but there are also claims that few clinicians acknowledge it even exists⁷⁶.
Will the past experiences of ME/CFS patients be repeated worldwide with LC patients valiantly trying to have their condition recognised and validated? These infection-associated chronic conditions are predicted to grow to at least 200 million in another 10 years and there is real concern LC research may gradually lose its current intensity and momentum before effective treatments become available⁷⁷.
Conclusions
COVID-19 has not disappeared like the first COVID outbreak in 2003, and SARS-CoV-2 has likely become a non-seasonal endemic virus, with increased rates of infection when a new variant emerges to outcompete the dominant resident strain. This predicts a significant future challenge. There will have to be constant public health attention and surveillance worldwide, and continued vaccination campaigns to regulate case numbers and thereby mitigate a significant ongoing and growing health burden.
One positive highlight has been the development of the new vaccines, and now the further ongoing innovation that is being applied to their evolution. These innovations have provided highly encouraging tools along with antivirals to be able to lower the deaths and hospitalisation rates that overwhelmed health systems at the beginning of the pandemic. It is hoped however, there will be appropriate widespread readily available treatment strategies in anticipation for use with those unfortunate small minority of individuals who will develop damaging rare adverse reactions to their vaccinations, and then ongoing social and financial support if that is needed. The scale of the ongoing vaccinations required for a best public health response will mean a significant number of these adverse reactions will continue to result and must be openly acknowledged.
The good news with respect to the post viral condition Long COVID is that the later SARS-CoV-2 variants have led to a decreasing rate of long COVID, and that prior vaccination can decrease it even further. But because the ongoing COVID-19 case numbers week by week are still significant there will be many more affected people added to the growing numbers with long term illness, and with increased susceptibility to develop common serious diseases. With only a four year follow-up time, insufficient time has yet elapsed to see a comprehensive picture of how seriously LC is going to affect our public health systems but there have been many gloomy predictions. The fact that LC is known to affect all ages, apparently all ethnic groups, strike after first infection or later infections, and arise from all virus variants means preventing future COVID-19 cases is critical. In NZ public health experts have called for a comprehensive LC risk assessment, having public health settings that will reduce markedly infections and re-infections, and for the expansion of vaccine eligibility and coverage as an attempt to mitigate the serious effects on our health system⁷⁸.
Conflicts of Interest:
The authors have no conflicts of interest to declare
Funding statement:
The authors are grateful to the Associated New Zealand Myalgic Encephalomyelitis Society (ANZMES) for support, and for generous personal donations from ME/CFS families.
Acknowledgements:
None
References
1. WHO. Number of COVID-19 cases reported to WHO (cumulative total, world). Accessed 18 July 2024, 2024.
https://data.who.int/dashboards/covid19/cases?n=c
2. Davis HE, McCorkell L, Vogel JM, Topol EJ. Long COVID: major findings, mechanisms and recommendations. Nat Rev Microbiol. Mar 2023;21 (3):133-146. doi:10.1038/s41579-022-00846-2
3. National Academies of Sciences E, Medicine. Long-Term Health Effects of COVID-19: Disability and Function Following SARS-CoV-2 Infection. The National Academies Press; 2024:264.
4. Cronin CJ, Evans WN. Nursing home quality, COVID-19 deaths, and excess mortality. Journal of Health Economics. 2022/03/01/ 2022;82:102592. doi:https://doi.org/10.1016/j.jhealeco.2022.102592
5. Filip R, Gheorghita Puscaselu R, Anchidin-Norocel L, Dimian M, Savage WK. Global Challenges to Public Health Care Systems during the COVID-19 Pandemic: A Review of Pandemic Measures and Problems. J Pers Med. Aug 7 2022; 12(8)doi:10.3390/jpm12081295
6. Chakraborty C, Bhattacharya M, Dhama K. SARS-CoV-2 Vaccines, Vaccine Development Technologies, and Significant Efforts in Vaccine Development during the Pandemic: The Lessons Learned Might Help to Fight against the Next Pandemic. Vaccines (Basel). Mar 17 2023;11(3) doi:10.3390/vaccines11030682
7. Punekar M, Kshirsagar M, Tellapragada C, Patil K. Repurposing of antiviral drugs for COVID-19 and impact of repurposed drugs on the nervous system. Microb Pathog. Jul 2022;168:105608. doi:10.1016/j.micpath.2022.105608
8. Martinez MA. Efficacy of repurposed antiviral drugs: Lessons from COVID-19. Drug Discov Today. Jul 2022;27(7):1954-1960. doi:10.1016/j.drudis.2022.02.012
9. Yotsuyanagi H, Ohmagari N, Doi Y, et al. Efficacy and Safety of 5-Day Oral Ensitrelvir for Patients With Mild to Moderate COVID-19: The SCORPIO-SR Randomized Clinical Trial. JAMA Netw
Open. Feb 5 2024;7(2):e2354991. doi:10.1001/jamanetworkopen.2023.54991
10. Zhou P, Li Z, Xie L, et al. Research progress and challenges to coronavirus vaccine development. J Med Virol. Feb 2021;93(2):741-754. doi:10.1002/jmv.26517
11. Conte C, Sogni F, Affanni P, Veronesi L, Argentiero A, Esposito S. Vaccines against Coronaviruses: The State of the Art. Vaccines (Basel). Jun 17 2020;8(2) doi:10.3390/vaccines8020309
12. Park TJ. Negotiating a pandemic treaty is just the first step – how will countries comply? Nature. Jun 2024;630(8015):9. doi:10.1038/d41586-024-01586-4
13. Lenharo M. Hope for global pandemic treaty rises – despite missed deadline. Nature. Jun 2024;630(8016):282. doi:10.1038/d41586-024-01658-5
14. Furey C, Scher G, Ye N, et al. Development of a nucleoside-modified mRNA vaccine against clade 2.3.4.4b H5 highly pathogenic avian influenza virus. Nature Communications. 2024/05/23 2024; 15(1):4350. doi:10.1038/s41467-024-48555-z
15. Lu J, Sun PD. High affinity binding of SARS-CoV-2 spike protein enhances ACE2 carboxypeptidase activity. J Biol Chem. Dec 25 2020;295(52):18579-18588. doi:10.1074/jbc.RA120.015303
16. Ols S, Yang L, Thompson EA, et al. Route of Vaccine Administration Alters Antigen Trafficking but Not Innate or Adaptive Immunity. Cell Rep. Mar 24 2020;30(12):3964-3971.e7. doi:10.1016/j.celrep.2020.02.111
17. Yonker LM, Swank Z, Bartsch YC, et al. Circulating Spike Protein Detected in Post-COVID-19 mRNA Vaccine Myocarditis. Circulation. Mar 14 2023;147(11):867-876. doi:10.1161/circulationaha.122.061025
18. Griffin I, King J, Lyons BC, et al. Estimates of SARS-CoV-2 Hospitalization and Fatality Rates in the Prevaccination Period, United States. Emerg Infect Dis. Jun 2024;30(6):1144-1153. doi:10.3201/eid3006.231285
19. Havers FP, Pham H, Taylor CA, et al. COVID-19-Associated Hospitalizations Among Vaccinated and Unvaccinated Adults 18 Years or Older in 13 US States, January 2021 to April 2022. JAMA Intern Med. Oct 1 2022;182(10):1071-1081. doi:10.1001/jamainternmed.2022.4299
20. Prize TN. Press release 2023-10-02. https://www.nobelprize.org/prizes/medicine/2023/press-release/
21. Mohammed I, Nauman A, Paul P, et al. The efficacy and effectiveness of the COVID-19 vaccines in reducing infection, severity, hospitalization, and mortality: a systematic review. Hum Vaccin Immunother. Dec 31 2022;18(1):2027160. doi:10.1080/21645515.2022.2027160
22. Singanayagam A, Hakki S, Dunning J, et al. Community transmission and viral load kinetics of the SARS-CoV-2 delta (B.1.617.2) variant in vaccinated and unvaccinated individuals in the UK: a prospective, longitudinal, cohort study. Lancet Infect Dis. Feb 2022;22(2):183-195. doi:10.1016/s1473-3099(21)00648-4
23. Herrero L. As COVID cases rise again, what do I need to know about the new FLiRT variants? https://theconversation.com/as-covid-cases-rise-again-what-do-i-need-to-know-about-the-new-flirt-variants-230423
24. WHO. Statement on the antigen composition of COVID-19 vaccines. 2024;
25. Zealand TWO-HN. Covid-19 current cases. Accessed 24 June 2024, 2024.
https://www.tewhatuora.govt.nz/for-health-professionals/data-and-statistics/covid-19-data/covid-19-current-cases
26. Hall V, Foulkes S, Insalata F, et al. Protection against SARS-CoV-2 after Covid-19 Vaccination and Previous Infection. N Engl J Med. Mar 31 2022;386 (13):1207-1220. doi:10.1056/NEJMoa2118691
27. Wu N, Joyal-Desmarais K, Ribeiro PAB, et al. Long-term effectiveness of COVID-19 vaccines against infections, hospitalisations, and mortality in adults: findings from a rapid living systematic evidence synthesis and meta-analysis up to December, 2022. Lancet Respir Med. May 2023;11(5):439-452. doi:10.1016/s2213-2600(23)00015-2
28. Cobey S, Hensley SE. Immune history and influenza virus susceptibility. Current Opinion in Virology. 2017/02/01/ 2017;22:105-111. doi:https://doi.org/10.1016/j.coviro.2016.12.004
29. Knight M, Changrob S, Li L, Wilson PC. Imprinting, immunodominance, and other impediments to generating broad influenza immunity. Immunological Reviews. 2020;296(1): 191-204. doi:https://doi.org/10.1111/imr.12900
30. Liang C-Y, Raju S, Liu Z, et al. Imprinting of serum neutralizing antibodies by Wuhan-1 mRNA vaccines. Nature. 2024/06/01 2024;630(8018):950-960. doi:10.1038/s41586-024-07539-1
31. Fang Z, Ahrnsbrak R, Rekito A. Evidence Mounts That About 7% of US Adults Have Had Long COVID. JAMA. 2024;332(1):5-6. doi:10.1001/jama.2024.11370
32. Xie Y, Choi T, Al-Aly Z. Postacute Sequelae of SARS-CoV-2 Infection in the Pre-Delta, Delta, and Omicron Eras. New England Journal of Medicine. 0(0)doi:doi:10.1056/NEJMoa2403211
33. Dutcher EG, Epel ES, Mason AE, et al. COVID-19 Vaccine Side Effects and Long-Term Neutralizing Antibody Response. Annals of Internal Medicine. 2024/07/16 2024;177(7):892-900. doi:10.7326/M23-2956
34. Fraiman J, Erviti J, Jones M, et al. Serious adverse events of special interest following mRNA COVID-19 vaccination in randomized trials in adults. Vaccine. Sep 22 2022;40(40):5798-5805. doi:10.1016/j.vaccine.2022.08.036
35. Yasmin F, Najeeb H, Naeem U, et al. Adverse events following COVID-19 mRNA vaccines: A systematic review of cardiovascular complication, thrombosis, and thrombocytopenia. Immunity, Inflammation and Disease. 2023/03/01 2023;11 (3):e807. doi:https://doi.org/10.1002/iid3.807
36. Wise J. Covid-19: Two rare vaccine side effects detected in large global study. BMJ. 2024;384:
q488. doi:10.1136/bmj.q488
37. Morgan HJ, Clothier HJ, Sepulveda Kattan G, Boyd JH, Buttery JP. Acute disseminated encephalomyelitis and transverse myelitis following COVID-19 vaccination – A self-controlled case series analysis. Vaccine. Apr 2 2024;42(9):2212-2219. doi:10.1016/j.vaccine.2024.01.099
38. Garg RK, Paliwal VK. Spectrum of neurological complications following COVID-19 vaccination. Neurol Sci. Jan 2022;43(1):3-40. doi:10.1007/s10072-021-05662-9
39. Bornstad-Tuveng AR, Peder Anker. AZD-1222. Reactions Weekly. 2021/05/01 2021;1857(1): 70-70. doi:10.1007/s40278-021-96455-7
40. Oshida S, Akamatsu Y, Matsumoto Y, et al. Intracranial aneurysm rupture within three days after receiving mRNA anti-COVID-19 vaccination: Three case reports. Surg Neurol Int. 2022;13:117. doi:10.25259/sni_1144_2021
41. Yangi K, Demir DD, Uzunkol A. Intracranial Hemorrhage After Pfizer-BioNTech (BNT162b2) mRNA COVID-19 Vaccination: A Case Report. Cureus. Apr 2023;15(4):e37747. doi:10.7759/cureus.37747
42. Scholkmann F, May CA. COVID-19, post-acute COVID-19 syndrome (PACS, “long COVID”) and post-COVID-19 vaccination syndrome (PCVS, “post-COVIDvac-syndrome”): Similarities and differences. Pathol Res Pract. Jun 2023;246:154 497. doi:10.1016/j.prp.2023.154497
43. Semmler A, Mundorf AK, Kuechler AS, et al. Chronic Fatigue and Dysautonomia following COVID-19 Vaccination Is Distinguished from Normal Vaccination Response by Altered Blood Markers. Vaccines (Basel). Oct 26 2023;11(11) doi:10.3390/vaccines11111642
44. Vogel G, Couzin-Frankel J. Studies probe COVID-19 shots’ link to rare symptoms. Science. Jul 7 2023;381(6653):18-19. doi:10.1126/science.adj5607
45. ANZMES. ANZMES Preliminary survey findings. 2021;
46. Johnson C. The ME/CFS/FM Coronavirus Vaccine Side Effects Poll Update + the New Severely
Ill Vaccine Side-Effects Poll.
https://www.healthrising.org/blog/2021/03/17/coronavirus-vaccine-poll-chronic-fatigue-fibromyalgia-severely-ill/
47. Komaroff AL. MECFS and Long COVID: Emerging Similarities and Why it Matters. Massachusetts ME/CFS & FM association. https://massmecfs.org/news-events/823-mecfs-and-long-covid-emerging-similarities-and-why-it-matters
48. WHO. A clinical case definition of post COVID-19 condition by a Delphi consensus, 6 October 2021. WHO REFERENCE NUMBER: WHO/2019-nCoV/Post_COVID-19_condition/Clinical_case_definition/2021.1. https://www.who.int/publications/i/item/WHO-2019-nCoV-Post_COVID-19_condition-Clinical_case_definition-2021.1
49. Gentilotti E, Górska A, Tami A, et al. Clinical phenotypes and quality of life to define post-COVID-19 syndrome: a cluster analysis of the multinational, prospective ORCHESTRA cohort. eClinicalMedicine. 2023/08/01/ 2023;62:102107. doi:https://doi.org/10.1016/j.eclinm.2023.102107
50. Tate WP, Walker MOM, Peppercorn K, Blair ALH, Edgar CD. Towards a Better Understanding of the Complexities of Myalgic Encephalomyelitis/ Chronic Fatigue Syndrome and Long COVID. Int J Mol Sci. 2023;24(6):5124.
51. Walker MOM, Peppercorn K, Kleffmann T, Edgar CD, Tate WP. An understanding of the immune dysfunction in susceptible people who develop the post-viral fatigue syndromes Myalgic Encephalomyelitis/Chronic Fatigue Syndrome and Long COVID. Medical Research Archives. 2023-07-06 2023;11(7.1)doi:10.18103/mra.v11i7.1.4083
52. Subramanian A, Nirantharakumar K, Hughes S, et al. Symptoms and risk factors for long COVID in non-hospitalized adults. Nature Medicine. 2022/08/01 2022;28(8):1706-1714. doi:10.1038/s41591-022-01909-w
53. Das S, Taylor K, Kozubek J, Sardell J, Gardner S. Genetic risk factors for ME/CFS identified using combinatorial analysis. J Transl Med. Dec 14 2022;20(1):598. doi:10.1186/s12967-022-03815-8
54. Taylor K, Pearson M, Das S, Sardell J, Chocian K, Gardner S. Genetic risk factors for severe and fatigue dominant long COVID and commonalities with ME/CFS identified by combinatorial analysis. Journal of Translational Medicine. 2023/11/01 2023;21(1):775. doi:10.1186/s12967-023-04588-4
55. Tate W, Walker M, Sweetman E, et al. Molecular Mechanisms of Neuroinflammation in ME/CFS and Long COVID to Sustain Disease and Promote Relapses. Front Neurol. 2022;13:877772. doi:10.3389/fneur.2022.877772
56. Mackay A, Tate WP. A compromised paraventricular nucleus within a dysfunctional hypothalamus: A novel neuroinflammatory paradigm for ME/CFS. International Journal of Immunopathology and Pharmacology. 2018;32: 2058738418812342. doi:10.1177/2058738418812342
57. Mackay A. A neuro-inflammatory model can explain the onset, symptoms and flare-ups of myalgic encephalomyelitis/chronic fatigue syndrome. Journal of Primary Health Care. 2019;11(4):300-307. doi:https://doi.org/10.1071/HC19041
58. Mackay A. The long COVID conundrum from a New Zealand perspective. N Z Med J. Jun 21 2024;137(1597):79-85. doi:10.26635/6965.6419
59. Vallings R. Chronic Fatigue Syndrome M.E. Symptoms, Diagnosis, Management. Calico Publishing; 2020.
60. Shepherd C, Chaudhuri A, Association M, Association ME, Society ANZM. ME/CFS/PVFS: An Exploration of the Key Clinical Issues. ME Association; 2013.
61. Association MMCaF. History of ME/CFS/ CFIDS. Accessed 24 June 2024, 2024.
https://massmecfs.org/more-resources-for-me-cfs/131-history-of-cfscfidsme
62. Committee on the Diagnostic Criteria for Myalgic Encephalomyelitis/Chronic Fatigue S, Board on the Health of Select P, Institute of M. The National Academies Collection: Reports funded by National Institutes of Health. Beyond Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Redefining an Illness. National Academies Press (US) Copyright 2015 by the National Academy of Sciences. All rights reserved.; 2015.
63. Muirhead N, Muirhead J, Lavery G, Marsh B. Medical School Education on Myalgic Encephalomyelitis. Medicina. 2021;57(6):542.
64. NIH. Recover Covid. https://recovercovid.org
65. Fairbank R. Long COVID still has no cure – so these patients are turning to research. Nature. Apr 2024;628(8006):26-28. doi:10.1038/d41586-024-00901-3
66. David Systrom JB. The Life Improvement Trial (LIFT). https://www.omf.ngo/the-life-improvement-trial
67. Davis HE, McCorkell L, Vogel JM, Topol EJ. Long COVID: major findings, mechanisms and recommendations. Nature Reviews Microbiology. 2023:1-14.
68. Komaroff AL, Lipkin WI. Insights from myalgic encephalomyelitis/chronic fatigue syndrome may help unravel the pathogenesis of postacute COVID-19 syndrome. Trends in Molecular Medicine. 2021/09/01/ 2021;27(9):895-906. doi:https://doi.org/10.1016/j.molmed.2021.06.002
69. Marshall-Gradisnik S, Eaton-Fitch N. Understanding myalgic encephalomyelitis. Science. Sep 9 2022;377(6611):1150-1151. doi:10.1126/science.abo1261
70. Jason LA, Natelson BH, Bonilla H, et al. What Long COVID investigators can learn from four decades of ME/CFS research. Brain Behavior and Immunity Integrative. 2023/12/01/ 2023;4:100022. doi:https://doi.org/10.1016/j.bbii.2023.100022
71. Vernon SD, Hartle M, Sullivan K, et al. Post-exertional malaise among people with long COVID compared to myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS). Work. 2023;74(4): 1179-1186. doi:10.3233/wor-220581
72. Peppercorn K, Edgar CD, Kleffmann T, Tate WP. A pilot study on the immune cell proteome of long COVID patients shows changes to physiological pathways similar to those in myalgic encephalomyelitis/chronic fatigue syndrome. Sci Rep. Dec 12 2023;13(1):22068. doi:10.1038/s41598-023-49402-9
73. Henderson AD, Butler-Cole BF, Tazare J, et al. Clinical coding of long COVID in primary care 2020-2023 in a cohort of 19 million adults: an OpenSAFELY analysis. EClinicalMedicine. Jun 2024; 72:102638. doi:10.1016/j.eclinm.2024.102638
74. Ziegler S, Raineri A, Nittas V, et al. Long COVID Citizen Scientists: Developing a Needs-Based Research Agenda by Persons Affected by Long COVID. Patient. Sep 2022;15(5):565-576. doi:10.1007/s40271-022-00579-7
75. Jassat W, Reyes LF, Munblit D, et al. Long COVID in low-income and middle-income countries: the hidden public health crisis. Lancet. Sep 30 2023;402(10408):1115-1117. doi:10.1016/s0140-6736(23)01685-9
76. Ledford H. Long COVID is a double curse in low-income nations – here’s why. Nature. Jan 2024;625(7993):20-22. doi:10.1038/d41586-023-04088-x
77. McCorkell L, Peluso MJ. Long COVID research risks losing momentum – we need a moonshot. Nature. Oct 2023;622(7983):457-460. doi:10.1038/d41586-023-03225-w
78. Kvalsvig A, Brooks AES, Potter JD, et al. Long Covid in Aotearoa NZ: Risk assessment and preventive action urgently needed.
https://www.phcc.org.nz/briefing/long-covid-aotearoa-nz-risk-assessment-and-preventive-action-urgently-needed