





Acute Kidney Injury in Cerebrovascular Disease Patients
Study on Acute Kidney Injury in Patients with Cerebrovascular diseases: an Overview from a Tertiary Care Hospital in Manipur
Rishav Dey¹, Gautam Chabungbam², Guliver Potsangbam³
- Dept. of Internal Medicine, Shija Hospitals and Research Institute
- Dept. of Neurosurgery, Shija Hospitals and Research Institute
- Dept. of Nephrology, Shija Hospitals and Research Institute
OPEN ACCESS
PUBLISHED: 30 September 2024
CITATION: Dey, R., et al. 2024. Study on Acute Kidney Injury in Patients with Cerebrovascular diseases: an Overview from a Tertiary Care Hospital in Manipur. Medical Research Archives, [online] 12(9).
https://doi.org/10.18103/mra.v1
2i9.5824
COPYRIGHT: © 2024 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v1 2i9.5824
ISSN 2375-1924
ABSTRACT
Acute kidney injury (AKI) is one of the several complications which patients with cerebrovascular accidents (CVA) or stroke develop during their hospital stay. It is well known that development of AKI is an indicator of poor outcomes in the inpatient. The association of stroke and AKI is poorly understood. Our study is an attempt to determine if AKI is an independent risk factor for poor outcomes in patients admitted at Shija Hospitals and Research Institute (SHRI) with stroke. This is a retrospective study done from the hospital records for the duration of one year (1st January 2023 to 1st Jan 2024). The total number of stroke patients was 177. The mean age was 60.21±13.74 years. Of these 177, 14(7.9%) had acute kidney injury. Renal replacement therapy (RRT) was necessary in 7 (50%) of the patients. Except for 2 patients in this group requiring renal replacement therapy, the rest had an adverse outcome. Thus, the development of acute kidney injury in patients of cerebrovascular diseases was associated with a poor outcome.
Introduction
Acute Kidney Injury (AKI) is the rapid deterioration of kidney function over hours to days. The Kidney Disease: Improving Global Outcomes (KDIGO) defines AKI as: increase in serum creatinine by ≥0.3 mg/dL (≥26.5 micromol/L) within 48 hours, or increase in serum creatinine to ≥1.5 times baseline, which is known or presumed to have occurred within the prior seven days, or urine volume <0.5 mL/kg/hour for six hours¹. It is associated with increased morbidity and mortality in patients². It is also associated with distant organ injury leading to worsened outcomes³.
Cerebrovascular diseases (CVD) cause loss of brain function due to occlusion of cerebral arteries. It is one of the major causes of death and debility⁴.
Patients with cerebrovascular diseases are prone to develop varied complications during their admission. A high incidence of acute kidney injury in patients admitted with cerebrovascular diseases especially acute ischemic stroke, is highlighted by several studies⁵˒⁶.
Stroke and acute kidney injury are said to share several risk factors such as hypertension and diabetes mellitus⁷. Thus several studies have revealed high incidence of kidney dysfunction in patients of CVD. A meta-analysis of eight studies showed AKI as a common complication of acute ischemic stroke, with a pooled prevalence rate of 12.9% patients developing AKI⁸. AKI was also associated with increased mortality. The mechanism of AKI in CVA patients are incompletely understood. The mechanism of simultaneous damage is felt to be as – a similar vascular structure having low resistance. This similarity could lead to simultaneous damage to both vascular beds during high blood pressure episodes⁹.
There are various geographical, etiologic and economic differences in the patterns of AKI in different parts of the world. Cerebrovascular diseases are also frequently encountered, but there is a lack of data with regard to frequency and outcomes of these patients. Economic factors also have a significant bearing on the management of patients, more so in those who have to pay out of their pockets and have less access to health insurance schemes¹⁰. Literature is sparse with regard to patients who develop AKI in a background of CVD, especially in this part of the country. This hospital based retrospective study was done in patients admitted in Shija Hospitals and Research Institute (SHRI) to study the clinical profile of patients admitted with CVD who also developed AKI during their hospital stay. SHRI is a 350 bedded tertiary care referral centre in the city of Imphal, Manipur, a state in the Union of India. It is the largest of the several privately run hospitals in the state catering to a population of approximately 2.5 million in the state and also of the neighbouring states.
Material and Methods
This was a hospital based retrospective study which included 177 patients presenting with acute cerebrovascular accident, conducted from 1st January 2023 to 1st Jan 2024. Patients admitted in Shija Hospitals and Research Institute (SHRI) with a diagnosis of acute stroke were selected and included in the study.
Inclusion criteria for patients were: 1) patients with ischemic or haemorrhagic strokes, and 2) patients admitted to the hospital within 48 hours of the onset of stroke.
Exclusion criteria: Patients admitted to the hospital with a previous history of CVA or after 48 hours of symptom onset, history of glomerulonephritis, urinary tract obstruction; exposure to radiocontrast agents were excluded from the study.
Serum creatinine and 24-hour urine output measurements were retrieved from the records for the entire duration of the hospital stay for each patient in the study. Patients who developed AKI as defined by KDIGO criteria were documented and outcomes noted.
Kidney Disease: Improving Global Outcomes (KDIGO) criteria, AKI is staged as below:
Stage 1 – Increase in serum creatinine to 1.5 to 1.9 times baseline, or increase in serum creatinine
by ≥0.3 mg/dL or reduction in urine output to <0.5 mL/kg/hour for 6 to 12 hours
Stage 2 – Increase in serum creatinine to 2.0 to 2.9 times baseline, or reduction in urine output to <0.5 mL/kg/hour for ≥12 hours.
Stage 3 – Increase in serum creatinine to 3.0 times baseline, or increase in serum creatinine to ≥4.0 mg/dL, or reduction in urine output to <0.3 mL/kg/hour for 24 hours, or anuria for ≥12 hours, or the initiation of kidney replacement therapy, or, in patients <18 years, decrease in estimated glomerular filtration rate (eGFR) to <35 mL/min/1.73 m²
This retrospective study was approved by the Hospital Ethical committee.
Multivariate logistic regression models testing the association between AKI and all-cause in hospital mortality were constructed. In the overall cohort, there was a significant interaction between mortality and AKI. Statistical analysis and all the statistical graphs were been prepared using Microsoft Excel 2016 and SPSS version 23.0.
Results
A total of 177 patients could be included in the study of which 117 were male and 60 were females with an average age of 60.2 years (Table 1). Of the total 177 patient, the majority had a haemorrhagic stroke (110; 62.1%). Of the 110 patients with haemorrhagic stroke 74 (67%) were male and 36(33%) females. Of the 61 patients with ischaemic stroke 40(65%) were male and 21(35%) were females. The majority of the patients were in the age group of 62-72 years comprising of 47(26.5%) patients.
Table 1. Gender wise distribution of the type of stroke
| Gender wise distribution of the type of stroke | Male | Female |
|---|---|---|
| Ischaemic | 40 | 21 |
| Haemorrhagic | 77 | 39 |
| Total | 117 | 60 |
It was also noted in our population that the average age of the patients with haemorrhagic stroke was 56.8 years in comparison to the average of the patients with ischaemic stroke at 72.8 years.
Of the 110 patients with haemorrhagic strokes 105 patients had ICH and of the 105 patients with ICH, 7 had associated SDH.
Of the co morbidities, Hypertension was the most common association (137) followed by Type 2 Diabetes Mellitus, CKD, Atrial fibrillation with 59, 13 and 9 patients respectively.
Hypertension was more commonly associated with haemorrhagic stroke (61%) compared to ischaemic stroke (39%) and type 2 diabetes mellitus was noted to be more common in patients with ischaemic stroke (54%). Atrial fibrillation was more common in ischaemic stroke (77%).
14 of the 177 patients developed AKI, according to the KDIGO criteria. 9 (8.1%) patients with haemorrhagic stroke suffered from AKI and 4(6.5%) patients with ischaemic stroke had AKI (Table 2). Of the 9 patients with AKI and haemorrhagic stroke, the majority (8) had intracerebral haemorrhage(ICH) on radiological imaging. Only 3 of the 177 patients had a prior report of serum creatinine and none of the three developed any episode of AKI during the hospitalization.
Table 2. Incidence of AKI in different type of strokes
| Incidence of AKI in different type of strokes | Haemorrhagic | Ischaemic |
|---|---|---|
| YES | 9 | 4 |
| NO | 106 | 57 |
Of the 14 patients who developed AKI, renal replacement therapy (RRT) was necessary in 7 (50%) of the patients, and 7 of them developed AKI secondary to sepsis. Of the 7 patients who required RRT, 2 made a complete recovery and were discharged with improvement. Of the remaining 5 patients, 4 were dialysis dependent and 1 made a partial recovery. Follow up was not possible because all 5 were discharged against medical advice (DAMA).
Table 3.
| Variables | Stroke patients (n=177) No. (%) |
|---|---|
| Age by years (Mean±std) | 60.21±13.74 |
| Gender | |
| Male | 117 (66.1) |
| Female | 60 (33.9) |
| Type of Stroke | |
| Ischemic | 61 (34.5) |
| Haemorrhagic | 110 (62.1) |
| Ischaemic to Haemorrhagic transformation | 6 (3.4) |
| Baseline creatinine at admission | |
| Mean±std | 1.22 ± 1.43 |
| Median | 0.8 |
| Minimum-Maximum | 0.4 – 9.8 |
| Acute Kidney Injury | |
| No | 163 (92.1) |
| Yes | 14 (7.9) |
| Co-Morbidities | |
| No | 24 (13.6) |
| Yes | 153 (86.4) |
| DM2 | 62 (35.0) |
| HTN | 134 (75.7) |
| CLD | 7 (4.0) |
| CKD | 13 (7.3) |
| COPD | 1 (0.6) |
| AF | 9 (5.1) |
| RHD | 3 (1.7) |
| CAD | 5 (2.8) |
| Malignancies | 1 (0.6) |
| Outcome | |
| Death | 7 (4.0) |
| Alive | 132 (74.6) |
| DAMA | 38 (21.5) |
Discussion
This study was conducted in a tertiary care centre in Manipur and total of 177 patients were enrolled. The males outnumbered the females in a ratio of (1.95 : 1) and the average age was noted to be 60.2 years. Similar studies done in other parts of India by K Bhattacharjee et. al¹¹ and M Ansaritroghi et. al¹² were noted to have a similar age and gender distribution as our study.
A total of 116 (65%) patients had haemorrhagic strokes as compared to 61(35%) of ischaemic stroke, which differed from the study done by K Bhattacharjee et. al¹¹ and M Bandyopadhyay et. al¹³ who noted in their study the incidence of acute ischemic stroke to be 74% and 53% respectively. Most of the patients in our study were in the age group of 62-72 years (Fig. 1) comprising of (26.5%) patients and was comparable to study done by K Bhattacharjee et. al¹¹ but differed to Mahdi Habibi- Koolaee et. al¹⁴ and their findings where most of the patients were >70 years old.
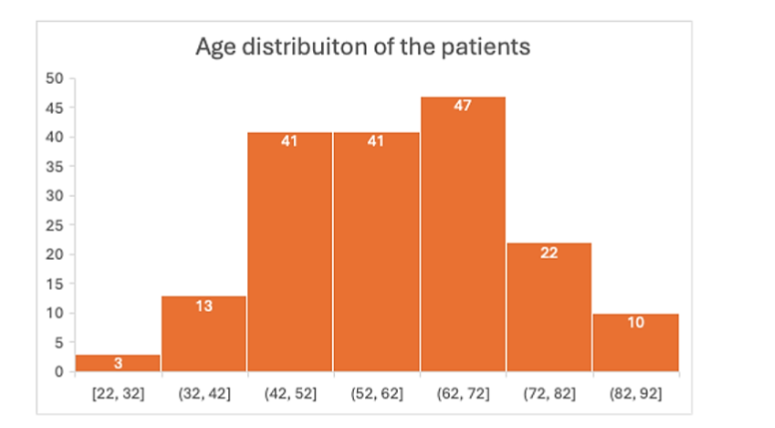
Fig.1. Age distribution of patients with cerebrovascular diseases (CVD)
The incidence of AKI in our population was 7%; which was lesser compared to the pooled prevalence rate (11.6%) in a meta-analysis by Zorrilla-Vaca et. al⁵ and was much lesser than the incidence rate (17%) in the study done by K Bhattacharjee et. al¹¹.
It was also noted that 8.1% and 6.5% of the patients with haemorrhagic stroke and ischaemic stroke developed AKI which is similar to the meta-analysis done by Zorrilla-Vaca et. al⁵ and K Bhattacharjee et. al¹¹ albeit the absolute incidence was much lesser.
Of the comorbidities, Hypertension was the most common association 134(75.7%) followed by Type 2 Diabetes Mellitus, CKD, Atrial fibrillation with 59(33%), 13(7.3%) and 9(5.1%) patients respectively. Hypertension was more commonly associated with haemorrhagic stroke and diabetes mellitus with ischaemic stroke; and was seem to be comparable to other studies done by M Katri et. al¹⁵ and K Bhattacharjee et. al¹¹.
Of the patients who developed AKI (n=14), 11 either died or were discharged against medical advice (Table 4). Similar poor outcomes were seen in patients with stroke who developed AKI in a study by Minesh Khatri and colleagues¹⁵.
Table 4. Status at discharge
| Status at discharge | AKI No | AKI Yes | Total |
|---|---|---|---|
| Death or DAMA | 34(20.9%) | 11(78.6%) | 45 |
| Alive | 129(79.1%) | 3(21.4%) | 132 |
| Total | 163 | 14 | 177 |
This study could be considered as a prelude to a further larger scale study in patients with CVD who develop AKI. We acknowledge that it was a single centre, retrospective study for a very short interval of time (1 year). This limited the study in the total number of patients. Many of the patients were discharged against medical advice (DAMA) owing to poor prognosis and poor financial condition of the family, leading to a dearth of data regarding the mortality status of those patients. It is reasonable to assume that these patients did not survive for a prolonged period due to their general condition at the time of discharge, and in all probability should be counted in the mortality group. This limited the ability of the study to reflect upon the prognostic and mortality predictors. A larger prospective study would help us in a detailed analysis of AKI in these patients, since it is associated with adverse outcomes. A concern is the number of patients leaving against medical advice. Although most of these patients had very poor prognosis and the relatives wished to have to their patient at home for the limited time they had together, it also highlights the economic hardship faced by the families and lack of financial support in the form of health insurance. A detailed analysis on the financial aspect of treatment in these patients would also help us in understanding how best to manage such patients.
Conclusion
AKI is not uncommon in patients with CVD and is associated with a variety of risk factors. Development of AKI in patients with CVD, be it ischemic or haemorrhagic, is associated with a worse outcome. Measures to prevent the development of AKI should be of paramount importance in these patient groups. Several risk factors of AKI in patients of CVD have been detailed. Further, the cause and relationship of CVD and AKI needs to explored in detail.
Conflict of Interest Statement:
None
Acknowledgements:
None
References
1. KDIGO Clinical Practice Guideline for Acute Kidney Injury; Kidney Int Suppl. 2012;2(Suppl 1):8.
2. Doyle, J.F., Forni, L.G. Acute kidney injury: short-term and long-term effects. Crit Care 20, 188 (2016)
3. Steven C. Yap, H. Thomas Lee, David S. Warner; Acute Kidney Injury and Extrarenal Organ Dysfunction: New Concepts and Experimental Evidence. Anesthesiology 2012; 116:1139–1148
4. Khaku AS, Tadi P. Cerebrovascular Disease. [Updated 2023 Aug 7]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430927/
5. Zorrilla-Vaca A, Ziai W, Connolly ES Jr, Geocadin R, Thompson R, Rivera-Lara L. Acute Kidney Injury Following Acute Ischemic Stroke and Intracerebral Hemorrhage: A Meta-Analysis of Prevalence Rate and Mortality Risk. Cerebrovasc Dis. 2018;45(1-2):1-9. doi: 10.1159/000479338. Epub 2017 Nov 24. PMID: 29176313.
6. Tsagalis G, Akrivos T, Alevizaki M, Manios E, Stamatellopoulos K, Laggouranis A, et al: Renal dysfunction in acute stroke: an independent predictor of long-term all combined vascular events and overall mortality. Nephrol Dial Transplant 2009; 24: 194–200.
7. Huang Y, Wan C, Wu G. Acute kidney injury after a stroke: A PRISMA-compliant meta-analysis. Brain Behav. 2020; 10:e01722. https://doi.org/10.1002/brb3.1722
8. Zhao Q, Yan T, Chopp M, Venkat P, Chen J. Brain-kidney interaction: Renal dysfunction following ischemic stroke. J Cereb Blood Flow Metab. 2020 Feb;40(2):246-262.
doi: 10.1177/0271678X19890931. Epub 2019 Nov 25. PMID: 31766979; PMCID: PMC7370616.
9. Fatma I. Albeladi , Iman Mohamed Wahby Salem , Saeed Ahmed Bugshan , Abdulrahman Abdulaziz Alghamdi; Acute Kidney Injury as a Risk Factor for Cerebrovascular Disease Outcome among Patients Presenting with Stroke in King Abdulaziz University Hospital, Jeddah, Saudi Arabia: A Retrospective Cohort study; Saudi J Kidney Dis Transpl 2021;32(1):60-68
10. Prasad, Narayan et al.: Community-acquired acute kidney injury in India: data from ISN-acute kidney injury registry; The Lancet Regional Health – Southeast Asia, Volume 21, 100359
11. Bhattacharjee K, Paul N, Roy S, et al. Acute kidney injury in acute stroke in relation to immediate outcome- a hospital based study. J. Evid. Based Med. Healthc. 2020; 7 (10), 475-479. DOI: 10.18410/jebmh/2020/103
12. Marzieh Ansaritoroghi, Shankar Prasad Nagaraju, Rajesh Parameshwaran Nair, Vinod Kumar, Lakshman I. Kongwad, Ravindra Prabhu Attur, Girish Menon Ramachandran, Ajay Hegde, Study on Acute Kidney Injury in Patients with Spontaneous Intracerebral Hemorrhage: an Overview from a Tertiary Care Hospital in South India, World Neurosurgery, Vol 123,2019, e740-e746, https://doi.org/10.1016/j.wneu.2018.12.018
13. Bandyopadhyay M, Jatua SK, Adhikari M, et al. Study of electrolyte abnormality in acute stroke. Ann Intern Med Dent Res 2017; 3(5):4-9.
14. Habibi-koolaee, Mahdi, Shahmoradi, Leila, Niakan Kalhori, Sharareh R., Ghannadan, Hossein, Younesi, Erfan, Prevalence of Stroke Risk Factors and Their Distribution Based on Stroke Subtypes in Gorgan: A Retrospective Hospital-Based Study—2015-2016, Neurology Research International, 2018, 2709654, 7 pages, 2018.
https://doi.org/10.1155/2018/2709654
15. Khatri M, Himmelfarb J, Adams D, Becker K, Longstreth WT, Tirschwell DL. Acute kidney injury is associated with increased hospital mortality after stroke. J Stroke Cerebrovasc Dis. 2014 Jan;23(1):25- 30. doi: 10.1016/j.jstrokecerebrovasdis.2012.06.005. Epub 2012 Jul 17. PMID: 22818389; PMCID: PMC35