





Radiotherapy Shortage in Sub-Saharan Africa: Insights and Solutions
Tackling the radiotherapy shortage in Sub-Saharan Africa by gathering and using data from Lower-Middle-Income and High-Income Countries’ facilities for designing a future robust radiotherapy facility
Abstract
Purpose: Historically, highly sophisticated medical linear accelerators (linacs) frequently experience significant additional operational failures in low- and lower-middle-income countries (LMICs) than in high-income countries (HICs). This study focuses on LMICs in Africa where there is a substantial equipment shortfall, projected to be a gap by 2040 of about 5000 linacs. The purpose of this study was to gain an insight into the poor performance of linac components, the unreliable infrastructure often encountered in LMICs and the consequent linac-related treatment downtime.
Methods and Materials: A questionnaire to obtain information on linac performance and repair experiences was sent to at least one cancer center in each of the 28 African countries that had experience treating cancer patients with linacs at the time of the survey (4 more countries have acquired linacs since we completed this survey). For comparison, questionnaires were also sent to selected facilities in four high-income countries (Canada, Switzerland, UK, US) and to Jordan, a middle-income country. To investigate factors influencing linac downtime, we first utilised flow diagrams to illustrate the dependence of linac subsystem performance on infrastructural/environmental factors, the availability of spare parts and local repair capability. Secondly, a univariate analysis correlated linac downtime with factors such as method of linac fault diagnosis and staffing. Finally, a multivariate analysis investigated the relationship between Gross Domestic Product (GDP) per capita and cancer mortality to incidence ratio statistics and compared these with the surveyed linac downtime across low-, middle- and high-income countries.
Results: Responses to the survey confirmed significant multi-factorial issues that influence the extent of linac downtime especially the performance of multi-leaf collimators, electron guns, vacuum systems, RF power and software. Other challenges include electrical power instability, inadequate national funding (GDP/capita), and workforce capability as well as a significant shortfall in formal education and training programmes for the radiation therapy (RT) workforce.
Conclusion: This survey identified numerous modes of RT equipment failure causing treatment downtime in LMICs that can be overcome by improvements in the design of RT technology but they need to be accompanied by increased RT staff training, improved broadband access and increased annual national funding for RT. The collaborative network of linac-based RT facilities in 28 African countries that was developed to conduct this study is available for further investigations as RT capacity and capability improve in Africa.
Keywords
- Radiotherapy
- Linear accelerators
- Low- and middle-income countries
- Africa
- Cancer treatment
Introduction
Radiation therapy (RT) is critical for the curative treatment or for palliation of symptoms for over half of all cancer patients with the number of patients increasing with time. In the face of this growing burden there is a global shortage in access to RT, especially in Sub-Saharan Africa where there is a shortage of RT equipment, staff, opportunities for education and training as well as innovation in treatment technology. This lack of access to RT in LMICs was articulated in 2015 by the Lancet Commission on Radiation Therapy (GTFRCC). Ideally, the RT service would be provided with linacs that offer state-of-the-art treatment that is safer than treatment with cobalt-60 with the added benefit that linacs have no radioactive sources that could be used for radiological terrorism. Currently, RT technology is of high cost to acquire and is complex to operate and service. Linacs in LMICs suffer from higher rates of downtime. The maintenance and spare parts required for operation in LMICs is very different from those in High-Income Countries (HICs). Indeed, the cost per fraction delivered is higher in LMICs than in HICs. Additionally, longer operating hours per day, maintenance and lack of training may have an impact on the downtime. It has been recognised by the vendors that radiotherapy in LMICs requires different engineering solutions. This situation has been described in the literature for decades but the solution requires a deeper dive into the basic technological issues such as is being undertaken by the International Cancer Expert Corps (ICEC) for Sub-Saharan Africa.
Preliminary data gathered by ICEC in 2019 showed a marked variation across Africa in linac-based RT capacity. The number of people served by each of the 385 linacs in Africa ranged from 1 linac per 423,000 people in Mauritius to 1 per 115 million people in Ethiopia, compared to 1 linac per 87,000 people in the US. In 2019 the majority of the linacs in Africa were found in the Mediterranean countries (227) and in South Africa (97). The lack of RT capacity is especially pronounced in the Sub-Saharan region where most of the 27 African countries that did not have linacs are located. In 2023, only four years later, the number of RT linacs has increased to just over 400. However, the distribution of linacs is still similar with the largest number of linacs being in Mediterranean countries with a total of 240 in Egypt, Morocco and Tunisia and 103 in South Africa. 32 countries now have linacs, up from 28 in 2019. The population served by each linac is a critical factor in evaluating the RT services provided by countries. The IAEA recommendation is 1 unit for every 250,000 people. None of the 54 countries in Africa is even close to being able to satisfy this recommendation. Even Mauritius which has a ratio of 1 linac per 423,000 people fails to meet this recommendation.
In recognition of both the shortfall of RT services in LMICs and the poor performance in LMICs of current linacs designed for use in the developed world, a project was initiated by ICEC and Conseil Européen pour la Recherche Nucléaire (CERN) in November 2016 and later joined and funded by the UK Science and Technology Facilities Council (STFC) to define the design parameters of a less expensive, robust, modular linac-based RT system that would function reliably with minimal operational and maintenance complexity in countries with challenging environments (power and broadband instability, lack of staff training, distance from service locations, heat and humidity, access to clean water) and infrastructures.
Materials and Methods
The design criteria for a novel linac for LMICs were discussed at a workshop at CERN in November 2016 and in subsequent workshops at CERN (2017), Manchester, UK (2018) and Gaborone, Botswana (2019), all of which were attended by representatives from LMICs. During these discussions it was recognized that greater detail regarding the performance of linacs in the challenging environments of LMICs was needed to create design specifications for a RT system to meet these challenges. In parallel, STFC funded the Innovative Technologies towards building Affordable and equitable global Radiotherapy capacity (ITAR) study. To aid this study in part, the working group agreed to distribute a questionnaire to obtain “on-the-ground” linac-performance data from facilities in Africa that had experience treating patients with linacs. The goal was to gain insight into the performance of linac components and infrastructure variables that negatively influence machine performance causing equipment downtime.
Questionnaires were sent by TAI and MD to physicists and radiation oncologists invited to the previously described workshops as well as to facilities in other African countries known to have experience treating cancer patients with external beam radiation therapy (EBRT). Completed surveys encompassing a total of 59 linacs were received from facilities in 28 African countries (Figure 1A) as well as for a total of 52 linacs in selected HIC facilities and from 4 facilities in Jordan, a Middle-Income Country (Figure 1B) and represented a variety of manufacturers. It was not the intent of this ITAR study to compare the equipment by manufacturer but rather to address the commonality of problems in infrastructure and in the RT systems that will provide information to produce effective linac design solutions.

SUBSYSTEM (LINAC COMPONENT) ANALYSIS
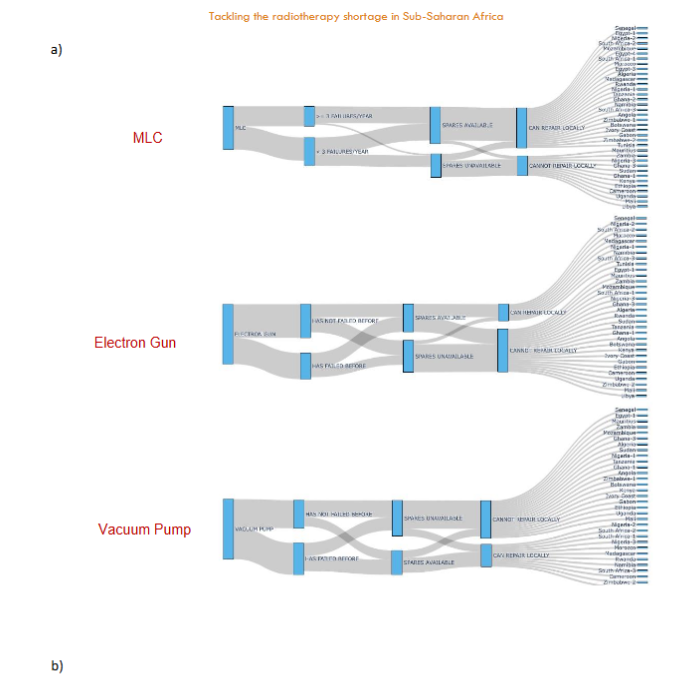
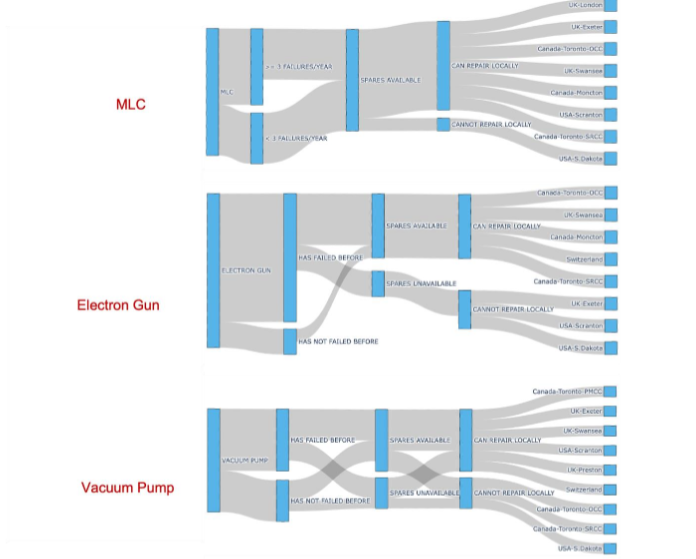
To investigate the relationship between the failure of linac components and infrastructural/environmental factors, Sankey plots (flow diagrams) for the multi-leaf collimator (MLC), electron gun and vacuum pump were used to analyze the following factors: 1) frequency of component failure, 2) availability of spare parts, and 3) local repair options (in-house or local contractor). Using this method of analysis, the frequency of responses for each factor was reported to indicate the reliability and operational efficiency of each component. In addition, flow/joint statistics between factors were derived from the Sankey plots to indicate how component failure, availability of spare parts and repair options are interdependent. Specifically, the flow statistics were used to gain insight into how often component failures coincided with a lack of spare parts and how the availability of spare parts is related to local repair options offering more nuanced insights into the infrastructural challenges faced.
This survey is composed of operational information from 59 linacs in 38 RT facilities in 28 African countries, as well as 52 linacs in 13 RT facilities in 5 higher income countries. Not all facilities answered all survey questions. Thus, because joint analysis using Sankey plots relies upon multiple consecutive questions being answered, if one answer is missing there may be some differences in the number of linacs or facilities analyzed compared to the numbers given above. In all cases, where responses have been averaged, each response is weighted equally, and there is no weighting for either linacs in a country or in the facility the response corresponds to. This prevents the results being skewed by more affluent countries with more linacs, which are likely to have better levels of servicing and hence downtime. Some countries had multiple responses from different facilities in that country and hence those countries are effectively weighted by the number of responses. In addition to component failure, the method and ease of diagnosing linac faults could impact a facility’s operational efficiency. Common methods of fault diagnosis are reported separately.
MULTIVARIATE ANALYSIS
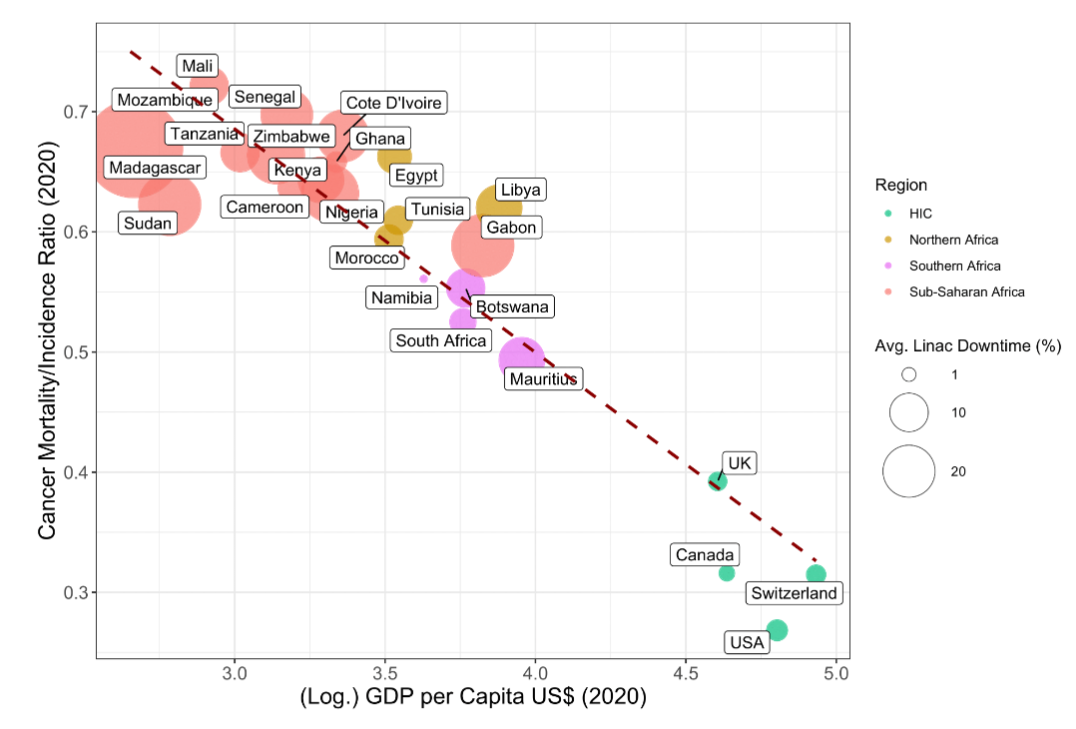
A multivariate analysis is used to observe the relationship between the ratio of the rate of cancer incidence to cancer mortality (MIR) in each of the surveyed countries to their GDP per capita and how these relate to the average percentage of linac downtime. Only the countries that responded as to how many weeks (and/or what percentage downtime) in a year each of their linacs experienced were included in this analysis. The mean was calculated for each country. Cancer mortality and cancer incidence rates by country were obtained from the World Health Organization Global Cancer Observatory Database for 2020 and were used to calculate each country’s MIR ratio. Although more recent GDP per capita data is available from the World Bank database, we used the data from 2020 to be consistent with the most recent MIR rate data (from 2020). A multivariate linear regression was then performed among these three variables to evaluate any correlations.
UNIVARIATE ANALYSIS
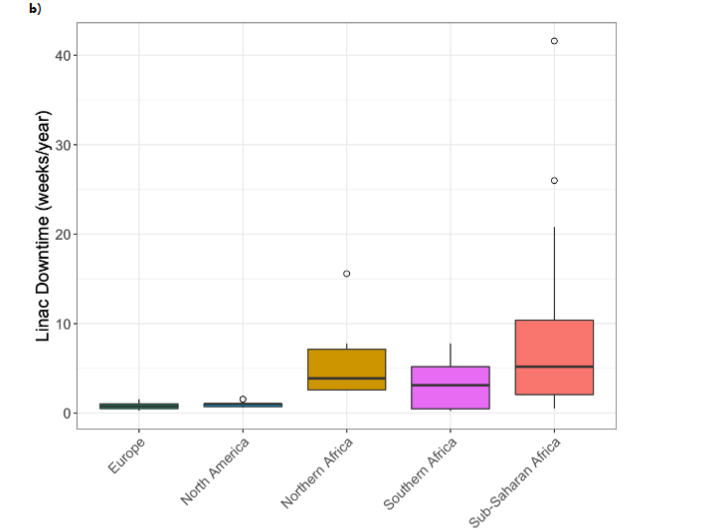
A univariate analysis of the variation of linac downtime determined as noted above among the facilities was carried out with data from the survey. This data was then plotted for each linac as well as for regional groups of linacs: Europe, N. America, Northern Africa, Sub-Saharan Africa and Southern Africa. To assess the possible importance of having spare linac components on site, both African and HIC facilities were queried regarding their access to spare MLCs, electron guns, RF sources and vacuum pumps.
Results
GENERAL OBSERVATIONS
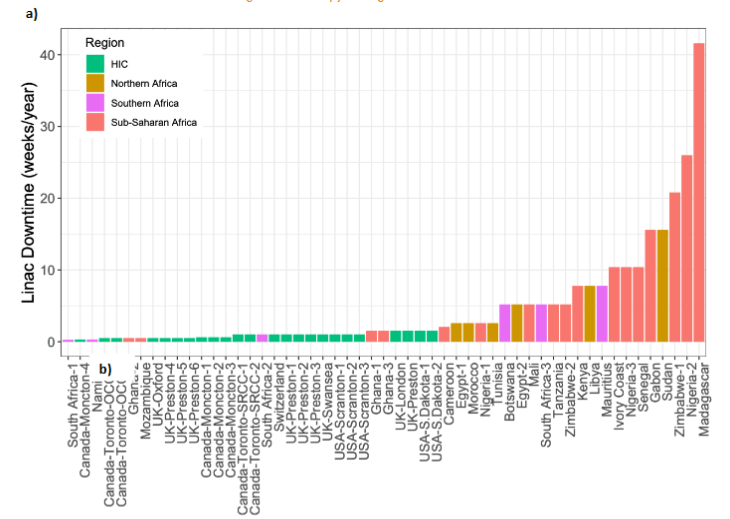
As shown in our preliminary report, the distribution of linacs throughout Africa is quite variable and correlates in large part with GDP/capita which in itself varies according to geography. As shown in Figure 2, the GDP/capita is 40K US$ in Mauritius and far less in most African countries while it ranges from 46K US$ in the UK to 86K US$ in Switzerland. The countries with the lowest GDP per capita have the least favorable range of mortality-to-incidence ratios (MIRs) (t = -11.52, p < 0.001), which is consistent with the results of our previous Balkan study. It can be seen in Figure 2 that Madagascar, the country with the lowest GDP/capita (< 500 US$), experienced the highest average percentage linac downtime (80%) out of all of the countries surveyed. For most countries with a GDP/capita of less than 3500 US$ (exceptions are Gabon and Libya) the MIR ranges from 0.6 to 0.75 regardless of the downtime. In the Southern African countries (Botswana, Mauritius, Namibia and South Africa) where the GDP/capita ranges from 4200 US$ to 9000 US$, the MIR ranges from 0.49 to 0.56 but inversely with regard to downtime. This is confirmed through the results of the linear regression between these two variables showing the correlation between linac downtime and the MIR (t = 1.875, p = 0.0735), is not statistically significant. Among the HIC countries, the MIR ranges from 0.27 (US) to 0.39 (UK), well below the range in the African countries, and the downtime is very low.
Summary of finding, observations and results from the survey
| Subsystems | Downtime | Environment | Possible Features | Services and Education |
|---|---|---|---|---|
| 41% of facilities experience MLC failures often. 62% have spares. 69% can repair locally. | Downtime may depend strongly on vacuum pump failure. Make the part very robust. | All bunkers surveyed are protected to at least 6 MV. Median Height 3.5m and floor area 42m2. | 81% of facilities find the electron mode highly valuable. 92% of facilities have a service contract. | 44% of facilities have experienced electron gun failure. 47% keep spares. 28% can repair locally. |
| Keep the mains supply as stable as possible, e.g. affordable UPS and backup generators. | Mean temperature in African bunkers: 22.6 °C. Max temp: 38°C. (Libya). Min temp: 15°C (Libya). | 26% of facilities currently have a tilting couch, many agree it would be a useful feature for advanced treatments. | 63% of facilities can troubleshoot problems with the linac. | 53% of facilities have experienced vacuum pump failure. 38% keep spares. 28% can repair locally. |
| Complicated software? Implement mission-critical software development. | Temperatures may vary significantly throughout the day. Consider optimal operating temperatures of components. | 94% of facilities have access to CT imaging close to RT machines. May need to provide this access in countries with no RT access. | 74% of facilities have staff attend a formal training course. | If a facility experiences faults with a component, they are more likely to keep spare parts for it. |
| A display/log on the machine may be easier to diagnose LINAC problems at the center, but may not affect downtime compared to remote diagnosis by manufacturer. | 87% of facilities have a humidity <= medium. Consider optimal operating humidity of components. | 93% of facilities have medium or high-speed internet. Consider the bandwidth available before opting for a full online training programme. |
SUBSYSTEM PERFORMANCE
This section presents survey results pertaining to the performance of the major linac components that frequently fail and the environmental/infrastructural factors that lead to downtime. Statistics derived from the Sankey plots in Figure 3 were used for the analysis of failure rates, access to spare parts and the ability to perform repairs locally for MLCs, electron guns and vacuum pumps.
MLCs
LMICS
Of the 29 facilities that reported on the performance of MLCs, 41% had experienced MLC failures often, 62% had spare parts available and 69% could repair MLCs locally. Notably, 91% of the facilities that frequently had experienced MLC failures had access to spare parts and 80% could repair MLCs locally. In contrast, among facilities that infrequently had MLC failures, 59% had spare parts and all could repair MLCs locally. However, only 29% of facilities that had not experienced failure of MLCs and did not keep spare parts could repair them locally. These flow statistics show that if a facility had experienced an MLC failure previously it was more likely to keep spare MLCs and to have the infrastructure necessary to repair them. The low average downtime of MLCs in HIC facilities was significantly greater in facilities where the MLC failed often. This is likely because they had the spare parts and expertise to repair locally.
HICs
Of the 12 HIC facilities that reported on the performance of MLCs, 64% had experienced MLC failures often, 89% had spare parts available and all could repair MLCs locally. Notably, all of the facilities that reported frequent MLC failures had access to spare parts and 88% of these could repair MLCs locally. In contrast to facilities in Africa, all facilities in HICs that reported infrequent MLC failures had access to spare parts and all could repair MLCs locally.
Electron gun
LMICs
The electron gun is a major source of downtime because of the difficulty in replacing that component and the general lack of trained personnel at the African RT facilities to do so. Of the 32 facilities that reported on electron gun performance, 44% had experienced failure before, 47% had spare parts available but only 28% could repair it locally. Among the group of facilities that had experienced electron gun failure, 62% had access to spare parts and 63% of these could repair the electron gun locally. On the other hand, 47% of facilities that had not experienced electron gun failure kept spare parts and 29% of these could repair it locally. However, all of the facilities that had not experienced electron gun failure and did not keep spare parts could repair it locally. Similar to the survey results regarding MLCs, the flow statistics for the electron gun show that if a facility had experienced an electron gun fault it was more likely to keep a spare and to be able to repair it locally.
HICs
Of the 12 facilities that reported on electron gun performance, 83% had experienced failure before, 71% had spare parts available and 63% could repair it locally. Among the group of facilities that had experienced electron gun failure, 67% had access to spare parts and all these facilities could repair the electron gun locally. Average downtime was significantly longer in HIC facilities that could not repair the electron gun locally (p=0.02) and when they did not have spare electron guns. Of the facilities that had not experienced electron gun failure, all kept spare parts and could repair it locally. It is noted that all facilities that did not have access to spare parts also could not repair it locally.
Vacuum pumps
LMICs
Of the 35 facilities that reported on vacuum pump performance, 53% had experienced failure of the vacuum pump, 38% had a spare and 28% could repair it locally. Among the group of facilities that had experienced vacuum pump failure, 50% also kept spare parts and 71% could repair it locally. On the contrary, only 36% of facilities that had not experienced vacuum pump failure kept spare parts and 63% could repair it locally. Of the facilities that had not experienced vacuum pump failure and did not keep a spare, only 11% could repair it locally. Downtime is longer in African facilities that experience vacuum pump failure but there is no evidence to suggest the same is true in HICs.
HICs
Of the 12 facilities that reported on vacuum pump performance, 60% had experienced failure of the vacuum pump, 70% had a spare and 67% could repair it locally. Among the group of facilities that had experienced vacuum pump failure, 60% also kept spare parts and 67% of these could repair it locally. On the contrary, 67% of facilities that had not experienced vacuum pump failure kept spare parts. Of the facilities that did not keep spare parts, 67% could repair it locally. Average downtime was greater in HIC facilities that did not have spare vacuum pumps and also was greater in HIC facilities that could not repair the RF source locally.
Fault diagnosis
Approximately two-thirds of the 28 African facilities reporting on the performance of a total of 52 linacs reported that diagnosing faults was easy, with half reporting the use of a display/log. Only 14% of faults are identified by the manufacturer, either remotely or during repair and maintenance.
DOWNTIME DUE TO FAILURE OF LINAC COMPONENTS
The detailed multi-level and multi-variate analyses of the data obtained in the survey has been used to assess the relationship between each data variable and linac downtime. The failure of major linac components leads to RT system downtime which, in turn, affects the radiation oncology department’s performance, including the number of cancer patients treated and often the success of patient treatment. The components that fall in this category are multi-leaf collimators (MLCs), the electron gun, the vacuum pump and the vacuum system. Downtime also is related to issues regarding infrastructure and the lack of staff capable of making repairs. The latter is due largely to the limited availability of education and training of RT personnel in LMICs.
Although MLCs on linacs may fail less frequently now than when first introduced, downtime in African facilities ranges from 2-12% if they can repair MLCs locally, from 3-18% if they cannot do so, from 5-10% if facilities have spare MLCs on-site and 5-15% if they do not. Downtime due to MLC failure is about 2% in HIC facilities that can repair MLCs locally and 3% if they cannot. HIC facilities experience similar percentages of downtime if they have (2%) or do not have (3%) spare MLCs on-site.
Downtime due to malfunction of the electron gun is a particular problem in African facilities where downtime ranges from 3-18% if the electron gun cannot be repaired locally and from 5-18% if spare electron guns are not available on-site. Downtime is only 2-5% if the electron gun can be repaired locally and 1-3% if spare electron guns are kept on-site. In HIC facilities, downtime due to electron gun failure is less than 3% whether repairs can be performed locally or whether spare electron guns are available on-site.
The downtime ranges from 3-8% for facilities in African countries that can repair vacuum pumps locally compared to 3-17% if they cannot. It ranges from 2-5% if they do to 5-20% if they do not have spare vacuum pumps. Linac downtime in HICs caused by vacuum pump failure is comparable in facilities that can (about 2%) or can’t (about 3%) repair vacuum pumps locally. There is little difference in downtime among HIC facilities whether spare vacuum pumps are available (2%) or not (3%). The downtime ranges from 3-7% in African facilities if the RF source can be repaired locally and from 5-17% if spare RF sources are available. Downtime ranges from 3-18% in African facilities that cannot repair RF sources locally and from 3-12% if they do not have spare RF sources on-site. The length of linac downtime in HICs due to failure of RF sources is limited to 2-3% whether repairs can be performed locally and whether spares are available on-site.
In summary, significant differences in downtime related to access to spare parts in African countries was observed only for the vacuum pump and the electron gun. Significant differences in downtime for the ability to perform repairs locally was observed only for the RF source and the electron gun.
DOWNTIME DUE TO THE ENVIRONMENT AND INFRASTRUCTURE
With regard to the environment’s affecting operations in African RT facilities, both temperature fluctuations and high humidity can be problems. Similar issues are experience in similar countries in South Asia and South America. The adverse effects of high humidity principally correlated with frequency fluctuations in electrical systems, but the low response rate to the questionnaire regarding mains fluctuations weakens conclusions. Many hospitals used a UPS to smooth the power supply. Most hospitals do not have staff that can quantify this. A future study will look into this.
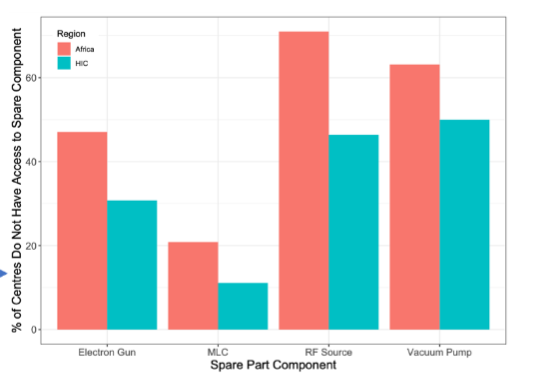
When asked what the leading cause of linac downtime was in African RT facilities, the overwhelming majority (69.2 %) said that it was due to lack of access to spare parts (Figure 5a). A comparison of access to spare parts in African and HIC centers surveyed shows that for each of the key components (MLC, electron gun, RF source and vacuum pump) the average percentage of African facilities not having access to these spare parts was higher than for facilities in HICs (Figure 5b). The greatest disparity (23.6%) was for the RF source.
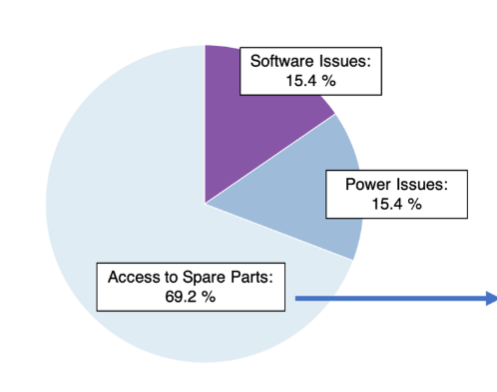
Two other major contributions to linac downtime in African RT facilities (15.4% each) are software and electrical power issues. Downtime was 12.0 ± 12.6 weeks/year in facilities that had software problems and was 4.9 ± 3.3 weeks/year in facilities that did not experience software problems. Downtime in HICs facilities was 1.0 ± 0.3 weeks/year among all facilities that experienced software problems and 0.7 ± 0.3 weeks/year in facilities that experienced software problems frequently. A two-sample T-test suggests evidence that downtime is dependent on software problems in Africa and in HICs.
Regarding education and training, including that needed to troubleshoot the linac, 20/27 (74%) of African facilities have staff who have attended a formal training course. 18/19 (95%) of the training courses were provided by the manufacturer, either on-site or online. That 28/30 (93%) African facilities were found to have a medium or high internet speed (kb/s – Mb/s), although the bandwidth varies significantly among facilities, provides an opportunity for enhanced and more frequent on-line training and mentoring.
An analysis of the number of staff capable of repairing linacs shows that downtime is shorter when there is one person on the staff who is capable of repairing linacs. The use of remote training could help to alleviate the burden of down-time.
Twenty three of the 25 (92%) African facilities so reporting had a service contract of some type. 15 of the 23 (65%) contracts were provided by the manufacturer. Downtime ranged from 2-11% if service is provided by the manufacturer, 2-20% if it is provided by a local company and 10-22% if service is provided by a subcontractor. Downtime is less when the age of the machine is 10 or fewer years. In HICs, downtime is about 2% whether service is provided by the manufacturer or a local service provider.
Discussion
The shortfall in the availability of medical linacs in LMICs has been recognized for some time as a major barrier to providing quality cancer care in those countries. A previous limited study by us comparing 3 countries: Botswana, Nigeria and Oxford showed that linacs probably have greater downtimes in LMICs in Africa than in HICs, primarily because of the time it takes to acquire spare parts and the lack of adequately trained linac engineers on-site or readily available. It appeared that linac components in LMICs may have higher failure rates than similar components in high-income countries. The current study was prompted by the need to verify our initial preliminary study by gathering extensive on-the-ground data from as many RT facilities in Africa as possible regarding the performance of their currently available linacs in order to design a RT system that will operate reliably in the challenging environments and the unreliable infrastructures encountered in LMICs where there is a lack of qualified experts to repair RT equipment. While the survey focused on Africa, similar issues are reported in the literature for other LMICs, and many of the studies are likely to apply outside of Africa.
There is a clear difference in the downtime experienced in LMICs and HICs, but there is also a spread in LMICs. There is a demarcation between Sub-Saharan Africa and Northern and Southern Africa, as well as differences within regions. Part of this may be explained by distance from major vendor service hubs in Europe and major South African cities such as Johannesburg.
This survey shows that the linac components most likely to adversely affect operational availability of the RT system by causing linac downtime are the MLCs, electron gun, RF source and vacuum system. It is clear from the data that access to spare parts locally is a major factor in the downtime of radiotherapy machines, specifically for vacuum pumps and the electron gun. Over two thirds of African respondents felt the lack of spare parts was the main reason for downtime. Another key factor was having local staff trained to make minor repairs in-house for the RF source and electron gun.
Because of the frequency of MLC failures and their negative impact on the efficiency of patient treatment, we are investigating the minimum number of MLC leaves required to deliver sophisticated radiation treatments as now can be delivered with state-of-the-art linac RT systems. The study will also investigate opportunities to increase the robustness of MLCs as well as to simplify replacement of MLCs by the local physicist or even RT technologists.
As noted earlier, failure of the electron gun is a significant cause of linac downtime. Linac downtime is greatest when the electron gun replacement time is long. The majority of LMIC RT facilities do not keep a spare electron gun on the premises because of the cost of that component and in some case limited shelf life. A majority of African facilities do not have someone capable of replacing the electron gun even if they have a spare so minimizing failure of the electron gun is a particularly crucial design feature. Minimizing the frequency of vacuum pump failures is a major consideration in the design of linacs specifically for LMIC settings. Another consideration is recommending improvements in preventive maintenance programs at facilities that have linac-based RT systems.
Another major factor is the electrical and IT infrastructure, with stability of both being poorer in many countries. Linac-based RT system design considerations to address the infrastructure and environment in African countries need to include electrical systems that are robust to voltage and frequency fluctuations as well as being insensitive to fluctuations in temperature and humidity and, often, excessive dust. Another goal is to minimize the power requirements of the linac.
In addition to targeting the development of innovative RT linac technology, an equally important aim is to use artificial intelligence (AI) and more specifically machine learning (ML) to develop intelligent software to enable the delivery of sophisticated RT treatments with fewer radiation therapy technologists and, importantly, fewer highly trained medical physicists (of whom there is often a shortage in LMICs) and maintenance engineers. One approach is to use AI and ML to predict faults to protect the linac before it has a chance to fail and simultaneously to order the appropriate replacement part(s). Also, AI should be able to identify the cause of faults that have happened. A simple feature on the RT system would be a display/log that will help staff identify faults.
Medical linac repairs are difficult and the inability to perform repairs locally reduces the availability of the linac for the treatment of patients. Having at least one person on the local staff with the ability to repair linac components and having access to spare parts are significant factors in decreasing downtime. If a facility frequently experiences failure of a component, it is more likely to keep spare parts. If a facility keeps spare parts, it is more likely to have the infrastructure in place to repair or exchange the component. With regard to providing greater availability and reliability of linacs for LMICs and minimizing the need for repairs, design considerations include choosing linac components with known long lifetimes and decreasing the cost of repairing the failures that do happen. Less expensive spare components that can be replaced by in-house staff should be selected when possible.
From the data it is clear that individual faults take significantly longer to repair in Africa than in HICs. This is due to several factors including the distance from manufacturer service hubs, lack of training and lack of spares. Even facilities that have spares and can make local repairs still have longer repair times than do facilities in HICs. In the current design of RT machines there is some evidence that design choices have been made to use components with lower lifetimes assuming that problems can be sorted during annual maintenance and repaired quickly (such as the use of magnetrons, gridded electron guns, number of MLC leaves and lack of backup vacuum pumps). While this assumption holds well in HICs, it is not clear that the same design choices are optimal in Africa. These choices should be reconsidered if a RT machine is to be developed specifically for the LMIC market. To overcome long machine downtimes that are due to the long time for repairs in LMICs with limited maintenance expertise, linac design for LMICs should prioritise components with extended lifetimes.
In order to improve the operational capability as well as the ability to maintain new sophisticated RT systems and to incentivize staff retention in most LMICs, it will be necessary to increase education, training and mentoring opportunities for all radiotherapy disciplines. There is an opportunity to leverage virtual mentoring to ensure full technical utilization of new linacs and, in many situations, to fully utilize existing linacs. In most African RT facilities there is a great need for adequately trained engineers to repair RT equipment.
All countries surveyed reported the need for additional funding to build many more RT facilities, to purchase additional RT equipment and to secure contracts to maintain the RT equipment. It was recommended by many respondents that local leaders be encouraged to increase public awareness of RT’s essential role in cancer treatment as an indirect way to garner additional government financing. Other respondents recommended that governments simplify procurement procedures for RT equipment.
As noted earlier, practitioners on-the-ground have provided unique data in response to this survey that expands significantly our knowledge regarding the shortage of RT capacity and capability in Africa. It has helped us determine those characteristics of linac-based RT systems that can be improved by technology (hardware and software) in order to enhance the capability and capacity of LMIC facilities to treat cancer patients. Other considerations include systematically exploring solutions such as ease and reliability of operation, machine self-diagnosis including a prominent display of impending or actual faults, ease of maintenance and repair, lifetime of key components, insensitivity to power interruptions, lower power requirements that reduce heat production and ease of upgrading by having a modular RT system. The comparative data from HICs clearly demonstrates that having sufficient resources, staff expertise and good infrastructure result in improved linac performance and very limited machine-downtime.
A single linac-based RT system cannot be expected to incorporate all the desirable design characteristics for operation in LMICs nor can it account for the numerous infrastructure variables. Based on the review of the various surveys, data gathering exercises, failure mode data and discussions at workshops, the working group developed linac design priorities as shown in Table 2. Great importance is given to having a well-educated technical staff, reliable linac components and both easier and less expensive repair of components if they do fail.
| High Priority | Medium Priority | Lower Priority |
|---|---|---|
| Provide staff training and skill requirements to run RT machines | Make linac robust to electrical fluctuations and minimize power requirements | Size of the linac |
| Avoid severity of and cost of repairing technical failures | Make linac robust to temperature fluctuations and dust | Total linac lifetime (as opposed to component lifetime) |
| Long component lifetime (decrease frequency of failures) | Provide x-ray delivery at high dose rate | Easy upgradability of linac |
| Decrease initial capital cost and cost of spare parts |
Conclusion
This survey represents the first major study of radiotherapy services in all 28 African countries and contrasts this to high-income countries. The study shows a major increase in mean downtime in African countries compared to HICs, and major differences between sub-Saharan Africa compared to Northern and Southern Africa. Respondents to the survey gave significant insight into environmental and infrastructure issues and capabilities that were then used to look at links between downtime and each individual factor. It was found the main factors were access to spare parts (vacuum pumps and electron gun), trained local staff being able to make repairs, (RF and electron gun), and electrical / IT infrastructure stability.
The benefits of this research to improve linac performance under difficult circumstances may enhance the care of cancer patients in LMICs indirectly as well. The availability of highly reliable equipment that allows RT facilities to establish predictable patient treatment schedules is important for those cancer patients and their families who have to travel a significant distance from home to the RT facility who otherwise might spend hours or days needlessly waiting to be treated because of linac downtime.
The trusted international network that was established to conduct this survey represents a valuable platform to conduct further important studies designed to improve the treatment of patients with cancer in LMICs as well as in remote regions in high-income countries that share some of the challenges of LMICs. We anticipate that this unique multidisciplinary collaborative platform of RT facilities in 28 African countries will be expanded as other African countries acquire linac-based RT systems.
Acknowledgements
Cameron Robertson, University of Oxford, UK
Jeffrey Buchsbaum, National Cancer Institute, USA
Lee Chin, USA
Sierra Kelleher, ICEC, USA
Author’s contributions:
All authors contributed to the conceptualization of the data, data collection and the manuscript had input from all authors.
Funding:
There was no funding or financial support for this manuscript.
Conflict of interest:
None. Note: The International Cancer Expert Corps is an official outside activity for CN Coleman and does not represent the opinion nor policy of the US National Cancer Institute.
Statement of conflict of interest
None of the co-authors declares any conflict of interest for this research.
References
- Barton M, Jacob S, Shafiq J et al. Estimating the demand for radiotherapy from the evidence: a review of changes from 2003 to 2012. Radiother Oncol 2014; 112:140-144
- Abdel-Wahab M, Bourque J-M, Pynda Y et al. Status of radiotherapy resources in Africa: an International Atomic Energy Agency analysis. Lancet Oncol 2013;4(4):168-175.
- Barton M, Zubizarreta E, Gospodarowicz M. Radiotherapy in Low- and Middle-income Countries. What Can We Do Differently? Clin Oncol 2017;29(2):69-71.
- Zubizarreta E, Van Dyk J, Lievens Y. Analysis of Global Radiotherapy Needs and Costs by Geographic Region and Income Level. Clin Oncol 2017;29(2):84-92.
- Atun R, Jaffray D, Barton M et al. Expanding global access to radiotherapy. Lancet Oncol 2015;16(10):1153-1186.
- Pomper M, Dalnoki-Veress F, Moore G. Treatment, Not Terror: Strategies to enhance external beam therapy in developing countries while permanently reducing the risk of radiological terrorism. 2016; Available at: http://www.stanleyfoundation.org/publications/report/TreatmentNotTerror212.pdf. Accessed December 2023.
- Afua A. Yorke, Vonetta M. Williams, Shekinah Elmore, Kellie Alleyne-Mike, Eric Addison, Philip Oppong Kyeremeh, Samuel Nii Adu Tagoe, Christoph Jon Trauernicht, Graeme L. Lazarus, Eric C. Ford, Radiation Therapy Physics Quality Assurance and Management Practices in Low- and Middle-Income Countries: An Initial Pilot Survey in Six Countries and Validation Through a Site Visit, Advances in Radiation Oncology, Volume 9, Issue 2, 2024, 101335, ISSN 2452-1094, https://doi.org/10.1016/j.adro.2023.101335.
- Ilupeju, Titus Adeniyi, Fatai O. Anafi, and Bassey Okon Samuel. Evaluating The Management And Maintenance Practices Of Linear Accelerator And Cobalt-60 Cancer Treatment Machines In Nigeria: A Comprehensive Assessment. Jurnal Mekanikal (2023): 175-189.
- H. Reichenvater, L. dos S. Matias, Is Africa a ‘Graveyard’ for Linear Accelerators?, Clinical Oncology, Volume 28, Issue 12, 2016, Pages e179-e183, ISSN 0936-6555, https://doi.org/10.1016/j.clon.2016.08.010.
- Van Der Giessen, Piet-Hein, Jose Alert, Cholid Badri, Matija Bistrovic, Deepak Deshpande, Dimitris Kardamakis, Debbie Van Der Merwe et al. “Multinational assessment of some operational costs of teletherapy.” Radiotherapy and Oncology 71, no. 3 (2004): 347-355.
- Vinall, Alison J. “Radiotherapy extended hours: manufacturers’ perspective.” A new approach for high precision skin cancer treatment: 17.
- Christin Elizabeth Agnew, Sergio Esteve, Glenn Whitten, William Little, Reducing treatment machine downtime with a preventative MLC maintenance procedure, Physica Medica, Volume 85, Volume 85, 2021, Pages 1-7, ISSN 1120-1797.
- Massat, Mary Beth. “A world of difference: Addressing the global need for radiation oncology systems.” Massat MB. Appl Radiat Oncol. 2019;(2):44-48. July 11, 201.
- Nwankwo, Kenneth Chima; Dawotola, David A1; Sharma, Vinay. Radiotherapy in Nigeria: Current Status and Future Challenges. West African Journal of Radiology 20(2): p 84-88, Jul–Dec 2013. | DOI: 10.4103/1115-1474.121099
- Efstathiou JA, Heunis M, Karumekayi T, Makufa R, Bvochora-Nsingo M, Gierga DP, Suneja G, Grover S, Kasese J, Mmalane M, Moffat H, von Paleske A, Makhema J, Dryden-Peterson S. Establishing and Delivering Quality Radiation Therapy in Resource-Constrained Settings: The Story of Botswana. J Clin Oncol. 2016 Jan 1;34(1):27-35. doi: 10.1200/JCO.2015.62.8412. Epub 2015 Nov 17. PMID: 26578607; PMCID: PMC5070566.
- https://indico.cern.ch/event/560969/: Design Characteristics of a Novel Linear Accelerator for Challenging Environments: “Improving global access to radiation therapy”
- Pistenmaa, D., Coleman, C.N., and Dosanjh, M.K.; Developing medical LINACs for challenging regions: http://cerncourier.com/cws/article/cern/67710 (2017)
- Pistenmaa D A, Dosanjh M and Amaldi U et al 2018 Changing the global radiation therapy paradigm Radiother. Oncol. 128 393–99
- Innovative, Robust and Affordable Medical Linear Accelerators for Challenging Environments https://indico.cern.ch/event/661597/overview
- Accelerating the Future: Designing a Robust and Affordable Radiation Therapy Treatment System for Challenging Environments https://indico.cern.ch/event/767986/overview
- Dosanjh M, Aggarwal A and Pistenmaa D et al 2019 Developing innovative, robust and affordable medical linear accelerators for challenging environments Clin. Oncol. 31 352–55
- Ige TA, Jenkins A, Burt G, Angal-Kalinin D, McIntosh P, Coleman CN, Pistenmaa DA, O’Brien D, Dosanjh M. Surveying the Challenges to Improve Linear Accelerator-based Radiation Therapy in Africa: A Unique Collaborative Platform of All 28 African Countries Offering Such Treatment. Clin Oncol (R Coll Radiol). 2021 Dec;33(12): e521-e529. doi: 10.1016/j.clon.2021.05.008. Epub 2021 Jun 9. PMID: 34116903
- International Atomic Energy Agency: Directory of Radiotherapy Centres (DIRAC). Available at http://www-naweb.iaea.org/nahu/dirac. December 2023
- Manson et al. Africa’s readiness for artificial intelligence in clinical radiotherapy delivery: Medical physicists to lead the way. Physica Medica 2023, 113(3):102653. https://doi.org/10.1016/j.ejmp.2023.102653
- Bishr MK, Zaghloul MS. Radiation therapy availability in Africa and Latin America: two models of low- and middle-income countries. International Journal of Radiation Oncology* Biology*. Physics 2018 Nov 1;102(3):490–8).
- ITAR Project https://iceccancer.org/innovative radiotherapy-technologies