





GPRC5D Therapies in Multiple Myeloma: Insights & Directions
Insights and Future Directions of GPRC5D Therapies in Multiple Myeloma
Stefan Longobardi¹†, Shoon Lei Oo¹† and Carolina Schinke¹
- Myeloma Center, University of Arkansas for Medical Sciences, Little Rock, AR, USA
Contributed equally
OPEN ACCESS
PUBLISHED: 31 May 2026
CITATION: Longobardi, S., et al., 2026. Insights and Future Directions of GPRC5D Therapies in Multiple Myeloma. Medical Research Archives, [online] 14(5).
COPYRIGHT: © 2026 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI: https://doi.org/10.18103/mra.v14i5.7439
ISSN 2375-1924
Abstract
Multiple myeloma (MM) is a clonal plasma cell malignancy characterized by marked biologic and clinical heterogeneity. Despite major advances with proteasome inhibitors, immunomodulatory drugs, and anti-CD38 monoclonal antibodies, MM remains largely incurable, with most patients experiencing a disease course marked by sequential relapses eventually leading to patient death. This unmet need has accelerated development of T-cell redirecting immunotherapies. G protein-coupled receptor class C group 5 member D (GPRC5D) has emerged as a promising therapeutic target because of its high expression on myeloma cells and limited expression in normal tissues. Unlike B-cell maturation antigen (BCMA), GPRC5D expression is often retained after BCMA-directed therapy, making it an attractive strategy for overcoming antigen escape and treatment resistance. Talquetamab, the first approved GPRC5D-targeting bispecific antibody, has demonstrated substantial efficacy in heavily pretreated relapsed/refractory MM. Overall response rates in the pivotal MonumenTAL-1 trial reached 74% with weekly dosing and 69% with every-two-week dosing, with rapid onset of response and durable remissions and an overall manageable safety profile. Importantly, clinically meaningful activity was also observed in patients previously treated with BCMA-directed chimeric antigen receptor T-cell therapy or bispecific antibodies. Ongoing studies are evaluating GPRC5D-targeted bispecific antibodies, chimeric antigen receptor T-cell therapies, trispecific antibodies, and rational combination approaches. These strategies may expand therapeutic sequencing options and potentially move GPRC5D-directed therapies into earlier lines of MM treatment.
Keywords
Multiple myeloma, GPRC5D, Talquetamab, immunotherapy, bispecific antibodies
Introduction
Multiple Myeloma (MM) is a clonal malignancy of plasma cells characterized by substantial clinical and genetic heterogeneity. It accounts for 1% of all the cancers and approximately 10-15% of hematological malignancies. Despite the success of legacy treatments (i.e. varying chemotherapeutic agents, proteasome inhibitors (PI), immunomodulatory drugs (IMiDs), and anti-CD38 monoclonal antibodies over the past decade, MM is largely considered incurable. The hallmark of the MM treatment paradigm is plagued by cycles of remission and relapse, which underlie the need for further development of novel pharmacologic agents.
The therapeutic landscape of multiple myeloma has undergone a profound transformation with the advent of T-cell redirecting immunotherapies. G protein-coupled receptor class C group 5 member D (GPRC5D) is an emerging therapeutic target highly expressed in MM cells. The new era of T-cell redirecting (TCRD) therapies, including bispecific antibodies and chimeric antigen receptor T-cells (CAR-T), increasingly utilize GPRC5D to treat relapsed and refractory (R/R) MM with remarkable efficacy in vivo. Recent clinical advances have validated the therapeutic potential of GPRC5D-targeted strategies.
The bispecific antibody Talquetamab has demonstrated robust activity in heavily pretreated, triple-class exposed patients, achieving overall response rates approaching 70%, significantly exceeding historical benchmarks. Unlike B-cell maturation antigen (BCMA), GPRC5D expression is largely independent and retained in many patients who relapse after BCMA-directed therapies, positioning it as a critical target for overcoming antigen escape and treatment resistance. These findings highlight the ability of GPRC5D-directed approaches to induce deep and clinically meaningful remissions in relapsed/refractory multiple myeloma.
The aim of this short review is to summarize biological knowledge and clinical efficacy of GPRC5D and its therapeutic targeting, thereby also emphasizing its unique on target off tumor adverse events including dysgeusia and nail/skin changes. Furthermore, we aim to give insights into current clinical trials of novel GPRC5D targeting agents and how the introduction of such will alter the future therapeutic landscape. To achieve this, the database PubMed was searched for terms that included, but were not limited to GPRC5D, bispecific antibodies, talquetamab, CAR T cell therapy and multiple myeloma. Eligible articles included clinical trials, original research articles, and relevant review articles evaluating the biology, efficacy, safety, and therapeutic sequencing of GPRC5D-directed therapies. Retrieved studies were reviewed and synthesized narratively, with emphasis on clinical efficacy, toxicity, and emerging combination and sequencing strategies.
Biology and mechanism of action
GPRC5D is a seven-pass transmembrane receptor protein with short extracellular domains that is highly expressed in Myeloma cells and less so in normal tissue. Structurally, this makes it less likely to be shed into the serum from target cells and allows it to form tighter immunological synapses, which drives greater response rates through augmented cytotoxicity. Currently, there is a paucity of information on its function and signaling mechanics in both normal and MM tissue. GPRC5D expression profiling also detected GPRC5D in the hair follicles, the skin, and the filiform papillae of the tongue with speculative expression in nail beds. As of this writing, Talquetamab is the first-in-class and only approved TCRD utilizing GPRC5D for triple class exposed, R/R MM. It is currently indicated for patients that received four prior lines of therapy (LOT), including a PI, IMiD, and anti-CD38 monoclonal antibody. It is a TCRD bispecific antibody (aka Bispecific T-Cell Engager, BiTE). TCRD Bispecific antibodies have two manufactured antigen binding sites, the surface marker CD3 on T-Cells and an antigen expressed on cancerous cells, in this case GPRC5D. This facilitates immunological synapse formation and killing of the tumor cells via bringing T-cells within close proximity.
As the mechanism of action involves stimulating the host’s immune system, adverse events (AE) that are immune-mediated, related to elevated cytokine levels i.e. cytokine release syndrome (CRS) and immune effector cell-associated neurotoxicity syndrome (ICANS) remain a significant risk and should be monitored meticulously.
Clinical Efficacy
Talquetamab was granted accelerated approval by the U.S. Food and Drug Administration (FDA) in August 2023 based on Monumen-TAL-1, the first in-human, multicenter, phase 1-2, open-label study of Talquetamab and can currently be used as a single agent in MM patients with at least 4 prior treatment lines. The underlying results were exceptional in a heavily pretreated population (median 5 LOT) with nearly 30% having high-risk cytogenetics, patients among the 0.4mg/kg once weekly (qW) dose subgroup had an overall response rate (ORR) of 74% (106/143) and the 0.8mg/kg every two weeks (q2W) subgroup had 69% (107/154) ORR, with 33% and 40% achieving at least a complete response (CR), respectively. The median time to response was 1.2 months and 1.3 months in the respective aforementioned groups; the time to very good partial response (VGPR) or better was 1.9 months and 2.2 months, with median progression free survival (PFS) was 7.5 months and 11.2 months in the respective cohorts. The subgroup of patients who received prior TCRD, including CAR-T (73%, 57/78), BiTE (33%, 26/78), or both (6%, 5/78) targeting BCMA antigen, with minority three patients composing other antigen targets (CD38, MAGE-A1) fared similarly well. For the TCRD group, ORR was 67% (CAR-T subgroup 72% ORR, BiTE 58% ORR); median PFS was 7.7 months. Further subcategorization reveals that those with prior bispecific antibody exposure had a median PFS of 3.9 months, as compared to a median PFS of 13.0 months with prior CAR-T exposure. At a follow up of 25.6 months, the median duration of response (mDOR) was durable in both q2W and q1W subgroups, though starkly better in the q2W subgroup at 16.9 months compared to 9.5 months in the q1W, the trend continuing as the data matures.
Safety/Toxicities
The Monumen-TAL-1 study showcased the tolerability and safety of Talquetamab. The rates of discontinuation were low, 5% in the qW subgroup and 6% in the q2W subgroup; 15% and 6% had dose reductions due to AE. No patients died due to drug-related AE. The most common immune AE in the treated populations was cytokine release syndrome (CRS), which occurred in severity as grade 1-2 in 77% (110/143) of the q1W group and 74% (114/154) of the q2W. This was confined to the step-up doses and the first full dose, with a median time to onset and duration of 48h. These patients received supportive measures, including Tocilizumab which led to resolution. Altogether, 46/143 (32%) of the patients in the qW group, 51/154 (33%) of the patients in the q2W group, and 23/78 (29%) of the previous TCRD group had more than one cytokine release syndrome event, with less than or equal to 5% progressing to worse grades of AE in their respective groups. ICANS occurred in 13/122 (11%) of patients in the qW group, 12/118 (10%) of patients in the q2W group, and two patients in the previous TCRD group; most cases were low grade occurring in conjunction with CRS. One patient in the q2W group had grade 2 cerebellar toxicity, which manifested as ataxia, necessitating discontinuation of treatment. The median time to onset and duration was more than that of CRS.
Other common AE (on-target, off tumor) included dermatologic, nail-related, and oral. The dermatologic side effects were mostly grade 1 and 2, encompassing exfoliation and dermatitis with grade 3 or higher occurring in 1% of the qW group and 6% in the q2W group. Oral AE reported include dysgeusia, dysphagia, and dry mouth. On target, off-tumor AE in early treatment cycles portended a greater likelihood of response.
Most of the grade 3 or 4 AE were hematologic side effects: most were reversible, limited to the first few cycles. These AE encompassed neutropenia, lymphopenia, anemia, and thrombocytopenia. As a result, infections occurred in 59%, 68%, and 76% of patients; grade 3 or higher in 20%, 18%, and 26% of the patients in the qW, q2W, and TCRD subgroups, respectively. Opportunistic infections occurred in approximately 5% of the aforementioned groups. A total of five patients died due to infections.
Polyclonal IgG levels decreased only transiently during the first couple of months of treatment, before rising above the baseline values for both responders and non-responders. GPRC5D is disproportionately expressed in MM cells rather than normal plasma cells, which may explain the lower incidence of severe infections (grade 3 or above) compared with BCMA BiTE. The resultant sparing of healthy plasma cells is reflected in the unchanged polyclonal IgG profiles of the treated patients. As a result, this may imply the importance of the investigation of combination therapies with Talquetamab to potentially achieve deeper and more durable clinical responses, with investigations already underway.
Future Directions
After being granted accelerated approval via Monumen-TAL-1, Talquetamab continues to show durable responses and deep clinical efficacy for heavily pretreated patients with R/R MM in post hoc analyses. This includes patients who were exposed to prior TCRD therapy, the majority of which was directed towards BCMA antigen. Further studies regarding the optimal order of therapy as it relates to GPRC5D and BCMA targeting bispecific antibodies is highly relevant and may inform sequencing strategies.
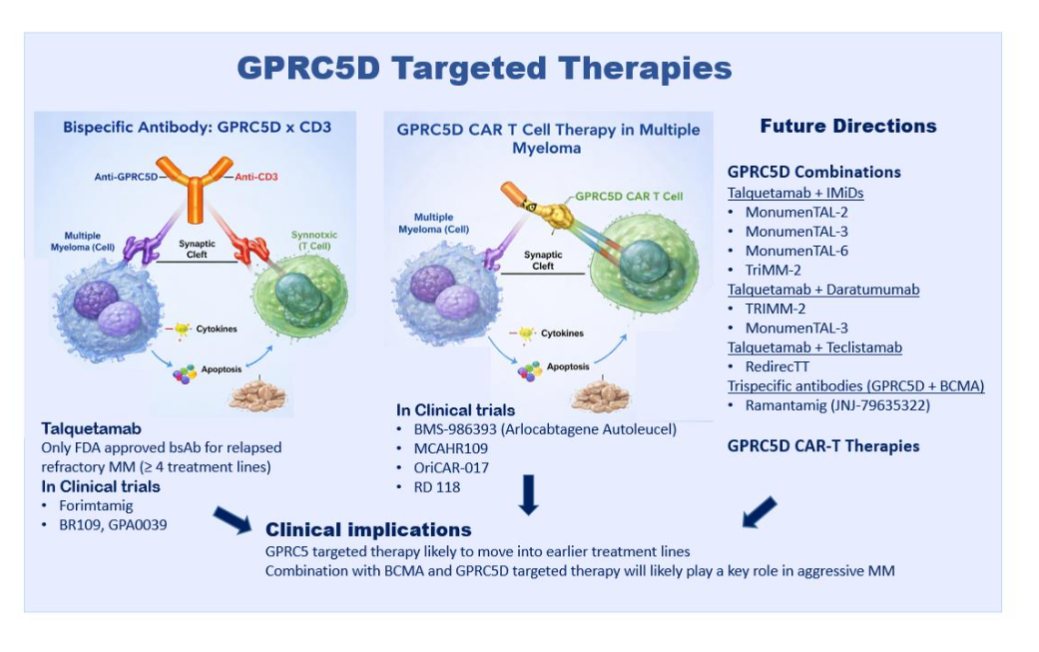
Future research is focusing on other novel TCRD targeting GPRC5D, including bispecific antibodies (Forimtamig and BR109) and CAR-T cell therapy (RD 118, OriCAR-017, BMS-986393, MCARH109) which are currently in clinical trials with promising early results. An emerging insight is the strategic integration of GPRC5D therapies within the broader immunotherapy sequencing paradigm, particularly in relationship to BCMA targeting therapy. While current practice is to perform CAR-T cell therapy before using a BiTE, as data suggests better efficacy and less immune exhaustion, the sequence of subsequent BiTEs is an area of active research.
GPRC5D-targeted BsAbs have demonstrated efficacy as salvage therapy following BCMA-directed CAR T-cell relapse, achieving high response rates and improved survival outcomes. However, with the likely introduction of further BiTEs with alternate targets (eg, FcRH5), further guidance of the sequence of therapies will be needed to achieve optimal outcomes.
Additionally, future directions in GPRC5D-targeted therapy are focused on enhancing efficacy, durability, and accessibility. Emerging clinical trials are evaluating combinations of GPRC5D with other effective agents such as IMiDs or anti CD38 monoclonal antibodies i.e. daratumumab (TRIMM-2 study) to overcome complementary immune mechanisms to elicit more robust and durable responses in R/R MM cases. For example, the MonumenTAL-3 clinical trial compares Talquetamab and daratumumab with or without pomalidomide (IMiD) to daratumumab and pomalidomide in R/R after 1 LOT. In the RedirecTT study, the combination of Talquetamab with Teclistamab, a BCMA targeting BiTE, has shown to be highly effective and induces high response rates and long remission in patients with high risk MM and extramedullary disease, a group of patients with traditionally dismal prognosis.
An extension of the aforementioned is being investigated in MonumenTAL-6, whereas Talquetamab and pomalidomide is being compared to Talquetamab and Teclistamab, as well as Elotuzumab and pomalidomide.
Given the high efficacy of combined targeting with GPRC5D and BCMA, trispecific antibodies are now being evaluated in clinical trials and suggest superior efficacy to bispecific antibodies with a similar toxicity profile. Taken together, GPRC5D-directed TCRT is highly effective in relapsed/refractory MM and can be safely combined with other anti-MM therapies. It is likely that GPRC5D based therapies will move into earlier lines of treatment in the near future. The combination of GPRC5D and BCMA targeting therapies is highly effective for aggressive MM and could become a novel treatment paradigm in this poor risk group. Continued clinical investigation and mechanistic studies will be essential to fully realize their potential and define their optimal role in achieving durable disease control and, ultimately, cure.
Conclusion
In conclusion, GPRC5D-directed immunotherapies have emerged as a highly promising strategy for patients with relapsed/refractory MM, demonstrating durable responses with a manageable safety profile even after prior BCMA-directed treatment. Ongoing studies of novel GPRC5D-targeted bispecific antibodies, CAR T-cell therapies, and combination approaches with BCMA-directed agents are likely to refine therapeutic sequencing and broaden clinical benefit. As these strategies continue to evolve, GPRC5D-based therapies may move into earlier lines of treatment and help establish a more effective framework for achieving deeper, more durable disease control in MM.
Disclosures
CS has participated in advisory board meetings of Janssen, Pfizer and Arcellx.
References
- Rajkumar SV. Multiple myeloma: 2024 update on diagnosis, risk-stratification, and management. Am J Hematol. Sep 2024;99(9):1802-1824. doi:10.1002/ajh.27422
- Elbahoty MH, Papineni B, Samant RS. Multiple myeloma: clinical characteristics, current therapies and emerging innovative treatments targeting ribosome biogenesis dynamics. Clinical & Experimental Metastasis. 2024;41(6):829-842. doi:10.1007/s10585-024-10305-2
- Portuguese AJ, Banerjee R, Chen G, Reddi S, Cowan AJ. Novel Treatment Options for Multiple Myeloma. JCO Oncol Pract. Jul 2025;21(7):950-961. doi:10.1200/OP-24-00752
- Chari A, Minnema MC, Berdeja JG, et al. Talquetamab, a T-Cell-Redirecting GPRC5D Bispecific Antibody for Multiple Myeloma. N Engl J Med. Dec 15 2022;387(24):2232-2244. doi:10.1056/NEJMoa2204591
- Zhou D, Wang Y, Chen C, Li Z, Xu K, Zhao K. Targeting GPRC5D for multiple myeloma therapy. Journal of Hematology & Oncology. 2024;17(1):88. doi:10.1186/s13045-024-01611-z
- Rodriguez-Otero P, van de Donk NWCJ, Pillarisetti K, et al. GPRC5D as a novel target for the treatment of multiple myeloma: a narrative review. Blood Cancer J. Feb 02 2024;14(1):24. doi:10.1038/s41408-023-00966-9
- Pillarisetti K, Edavettal S, Mendonça M, et al. A T-cell redirecting bispecific G-protein coupled receptor class 5 member D x CD3 antibody to treat multiple myeloma. Blood. 2020;135(15):1232-1243. doi:10.1182/blood.2019003342
- Hipp S, Tai YT, Blanset D, et al. A novel BCMA/CD3 bispecific T-cell engager for the treatment of multiple myeloma induces selective lysis in vitro and in vivo. Leukemia. 2017;31(8):1743-1751. doi:10.1038/leu.2016.388
- Chari A, Touzeau C, Schinke C, et al. Safety and activity of talquetamab in patients with relapsed or refractory multiple myeloma (MonumenTAL-1): a multicentre, open-label, phase 1-2 study. Lancet Haematol. Apr 2025;12(4):e269-e281. doi:10.1016/S2352-3026(24)00385-5
- Sedykh S, Prinz V, Buneva V, Nevinsky G. Bispecific antibodies: design, therapy, perspectives. Drug Design, Development and Therapy. 2018; Volume 12:195-208. doi:10.2147/dddt.s151282
- Strohl WR, Naso M. Bispecific T-Cell Redirection versus Chimeric Antigen Receptor (CAR)-T Cells as Approaches to Kill Cancer Cells. Antibodies. 2019;8(3):41. doi:10.3390/antib8030041
- Keam SJ. Talquetamab: First Approval. Drugs. Oct 2023;83(15):1439-1445. doi:10.1007/s40265-023-01945-x
- Bahlis LJCaNDaLRaRPaBsaJM-LaDTaTSaKCaN. Long-Term Follow-up from the Phase 1/2 Majestec-1 Trial of Teclistamab in Patients with Relapsed/Refractory Multiple Myeloma: Subgroup Analysis by Lines of Therapies. Hematology, Transfusion and Cell Therapy. 2024;46:S515. doi:https://doi.org/10.1016/j.htct.2024.09.865
- Lesokhin AM, Tomasson MH, Arnulf B, et al. Elranatamab in relapsed or refractory multiple myeloma: phase 2 MagnetisMM-3 trial results. Nat Med. Sep 2023;29(9):2259-2267. doi:10.1038/s41591-023-02528-9
- Cohen YC, Morillo D, Gatt ME, et al. First results from the RedirecTT-1 study with teclistamab (tec) + talquetamab (tal) simultaneously targeting BCMA and GPRC5D in patients (pts) with relapsed/refractory multiple myeloma (RRMM). Journal of Clinical Oncology. 2023;41(16_suppl):8002-8002. doi:10.1200/JCO.2023.41.16_suppl.8002
- Dholaria BR, Weisel K, Mateos M-V, et al. Talquetamab (tal) + daratumumab (dara) in patients (pts) with relapsed/refractory multiple myeloma (RRMM): Updated TRIMM-2 results. Journal of Clinical Oncology. 2023;41(16_suppl):8003-8003. doi:10.1200/JCO.2023.41.16_suppl.8003
- Matous J, Biran N, Perrot A, et al. Talquetamab + Pomalidomide in Patients with Relapsed/Refractory Multiple Myeloma: Safety and Preliminary Efficacy Results from the Phase 1b MonumenTAL-2 Study. Blood. 2023;142(Supplement 1):1014-1014. doi:10.1182/blood-2023-187706
- Eckmann J, Fauti T, Biehl M, et al. Forimtamig, a novel GPRC5D-targeting T-cell bispecific antibody with a 2+1 format, for the treatment of multiple myeloma. Blood. 2025;145(2):202-219. doi:10.1182/blood.2024025987
- Liu Y, Zhou Y-Q, Nie L, Zhu S-S, Li N, Wu Z-H, Wang Q, Qi J, Wu B-Y, Chen S-Q, et al. BR109, a Novel Fully Humanized T-Cell-Engaging Bispecific Antibody with GPRC5D Binding, Has Potent Antitumor Activities in Multiple Myeloma. Cancers. 2023; 15(24):5774. https://doi.org/10.3390/cancers15245774
- Mailankody S, Devlin SM, Landa J, et al. GPRC5D-Targeted CAR T Cells for Myeloma. N Engl J Med. Sep 29 2022;387(13):1196-1206. doi:10.1056/NEJMoa2209900
- Bal S, Htut M, Nadeem O, et al. BMS-986393 (CC-95266), a G Protein-Coupled Receptor Class C Group 5 Member D (GPRC5D)-Targeted Chimeric Antigen Receptor (CAR) T-Cell Therapy for Relapsed/Refractory Multiple Myeloma (RRMM): Updated Results from a Phase 1 Study. Blood. 2023;142(Supplement 1):219-219. doi:10.1182/blood-2023-181857
- Zhang M, Wei G, Zhou L, et al. GPRC5D CAR T cells (OriCAR-017) in patients with relapsed or refractory multiple myeloma (POLARIS): a first-in-human, single-centre, single-arm, phase 1 trial. The Lancet Haematology. 2026/04/03 2023;10(2):e107-e116. doi:10.1016/S2352-3026(22)00372-6
- Dima D, Banerjee R, Hansen DK. CAR T-cell therapy and bispecific antibodies in the management of multiple myeloma. Hematology. 2025;2025(1):324-333. doi:10.1182/hematology.2025000721
- Costa LJ, Banerjee R, Mian H, et al. International myeloma working group immunotherapy committee recommendation on sequencing immunotherapy for treatment of multiple myeloma. Leukemia. Mar 2025;39(3):543-554. doi:10.1038/s41375-024-02482-6
- Richter J, Thomas SK, Krishnan AY, et al. Cevostamab in Patients with Heavily Pretreated Relapsed/Refractory Multiple Myeloma (RRMM): Updated Results from an Ongoing Phase I Study Demonstrate Clinically Meaningful Activity and Manageable Safety and Inform the Doses and Regimen for Combination Studies. Blood. 2024;144(Supplement 1):1021-1021. doi:10.1182/blood-2024-199542
- Chari A, van de Donk NWCJ, Dholaria B, et al. Talquetamab plus daratumumab for the treatment of relapsed or refractory multiple myeloma in the TRIMM-2 study. Blood. 2025;146(24):2902-2913. doi:10.1182/blood.2025029360
- Wang X, Cui Y, Wang Y, Fang B. Emerging role of G protein-coupled receptor class C group 5 member D-directed immunotherapy in multiple myeloma: Advances, resistance and combination strategies. Br J Haematol. Nov 2025;207(5):1765-1778. doi:10.1111/bjh.70116
- Yaël C. Cohen, Philippe Moreau, Jaszianne Tolbert, Xiang Qin, Xuewen Ma, Diego Vieyra, Angelique Langlois, Christelle Courtoux, William Terry, Lixia Pei, Christoph Heuck, Peter Voorhees; MonumenTAL-3: Phase 3 Trial of Talquetamab + Daratumumab ± Pomalidomide Versus Daratumumab + Pomalidomide + Dexamethasone in Relapsed/Refractory Multiple Myeloma Following Line of Therapy. Blood 2022; 140 (Supplement 1): 4418 4419. doi: https://doi.org/10.1182/blood-2022-162733
- Cohen YC, Magen H, Gatt M, et al. Talquetamab plus Teclistamab in Relapsed or Refractory Multiple Myeloma. New England Journal of Medicine. 2025;392(2):138-149. doi:doi:10.1056/NEJMoa2406536
- Kumar S, Mateos M-V, Ye JC, et al. Dual Targeting of Extramedullary Myeloma with Talquetamab and Teclistamab. New England Journal of Medicine. 2026;394(1):51-61. doi:10.1056/NEJMoa2514752
- Ajay K. Nooka, Hira Mian, Cindy Lee, Paula Rodríguez-Otero, Shaji Kumar, Hermann Einsele, Deeksha Vishwamitra, Diego Vieyra, Colleen Kane, Michele Kosh, Tara J Masterson, Christoph Heuck, Ankit Kansagra, Philippe Moreau; Monumental-6: A Phase 3 Study of Talquetamab + Pomalidomide or Talquetamab + Teclistamab Vs Elotuzumab + Pomalidomide + Dexamethasone (EPd) or Pomalidomide + Bortezomib + Dexamethasone (PVd) in Patients with Relapsed/Refractory Multiple Myeloma Who Received 1-4 Prior Lines of Therapy, Including Lenalidomide and an Anti-CD38 Monoclonal Antibody. Blood 2024; 144 (Supplement 1): 4757.1. doi: https://doi.org/10.1182/blood-2024-199752
- Pillarisetti K, Yang D, Luistro L, et al. Ramantamig (JNJ-79635322), a novel T-cell-engaging trispecific antibody targeting BCMA, GPRC5D, and CD3, in multiple myeloma models. Blood. 2026;147(8):834-847. doi:10.1182/blood.2025030027
- Pillarisetti R, Yang D, Yao J, et al. Characterization of JNJ-79635322, a Novel BCMAxGPRC5DxCD3 T-Cell Redirecting Trispecific Antibody, for the Treatment of Multiple Myeloma. Blood. 2023;142(Supplement 1):456-456. doi:10.1182/blood-2023-174941