





Pretibial Myxedema in Hypothyroid Patients: A Case Study
Pretrial Myxedema in a Hypothyroid Patient with Grave’s Disease: A Case Report
1. Introduction
Pretibial myxedema is a part of the classical triad of Graves’ disease, which includes goiter, ophthalmopathy, and pretibial myxedema¹. It occurs due to the accumulation of hyaluronic acid in the dermis and subcutaneous tissue as a result of cytokines stimulation. Hyaluronic acid, the main glycosaminoglycan in the skin, has a high capacity to bind water and can increase in volume significantly². The lesions are typically found on the skin of the pretibial region, appearing as nonpitting edema, nodular, and plaque forms. However, it can also extend to the ankle and dorsum of the foot and may appear on the elbows, knees, upper back, and neck³˒⁴. Prevalence of pretibial myxedema is relatively rare and up to 5% of patients with Graves’ disease and 15% of those with both Graves’ disease and ophthalmopathy⁵. The presence of thyroid-stimulating hormone (TSH) receptors in skin fibroblast is a crucial factor in the development of this condition. These receptors are stimulated by antibodies to the thyroid-stimulating hormone, leading to TSHR stimulation and hyperthyroidism. These antibodies are also implicated in the extrathyroidal manifestations of Graves’ disease, including pretibial myxedema⁶˒⁷. The presence of typical pretibial lesions usually occurs in Graves’ ophthalmopathy and a history of thyrotoxicosis. However, rare cases have been reported in patients with hypothyroidism or euthyroidism⁸˒⁹.
Clinically, pretibial myxedema presents with a range of symptoms. Early signs include firm lumps under the skin that may change in size or merge. As the condition progresses, symptoms may include swelling, thick and scaly plaques, discoloration from orange to brown, red to purple, and sore or itchy skin, primarily affecting the lower legs, feet, and shins¹⁰. There are four types of pretibial myxedema: diffuse (non-fitting edema), plaque (thick scaly plaques), nodular (firm lumps), and elephantiasic (lymphatic fluid buildup creating a warty appearance)¹¹.
The diagnostic criteria for pretibial myxedema include a history of autoimmune thyroid diseases, nonpitting swelling and thickening of local skin, mucinous degeneration, and positive Alcian blue staining, distinct histopathological features¹².
Here, we present a case of a woman with hypothyroidism treated with levothyroxine for seven years, who developed pretibial myxedema associated with increased titers of TSHR antibodies (TRAbs).
2. Case report
A 42-year-old woman presented to the endocrinology clinic with a more than ten-year history of dark plaques and indurated skin lesions on the bilateral shins that expanded to involve the dorsal feet. The patient’s initial lesion consisted of asymptomatic, erythematous papules that gradually merged, and formed an infiltrative indurated plaque. Over time, the lesion enlarged to cover the pretibial region below the knee, causing associated edema and discomfort, and as a result, her movement was severely impaired. The patient was diagnosed with Grave’s disease 20 years ago and two years following antithyroid drug treatment, she underwent a subtotal thyroidectomy involving both thyroid lobes. Pretibial myxedema started to develop one year after the thyroidectomy, and she was treated with systemic glucocorticoids for several years.
Her condition remained stable for nine years post-surgery. Subsequently, she received iodine-131 therapy. Two years after the radioiodine treatment, she developed hypothyroidism, and thyroid replacement therapy with 75 mcg of levothyroxine was initiated. Her medical history also included pulmonary tuberculosis which was treated by a combination of antibacterial medications.
On physical examination, her blood pressure was 100/70 mmHg, and her heart rate was 70 beats/min with a regular rhythm. She had central obesity with a waist circumference of 97 cm, visceral fat of 9%, and body mass index of 32.1 kg/m².
In the eye examination, there were bags under the eyes, dry and watery eyes, difficulty moving the eyes, and bilateral marked proptosis. Hertel exophthalmometric values were 17 mm in the right eye, and 14 mm in the left (Figure 1).

Figure 1. Photograph of both eyes on the examination day.
The thyroid function test revealed hypothyroidism, with levels of TSH of 4.09 μIU/mL (reference range: 0.35–5.50 μIU/mL), TSH-thyroid stimulating hormone receptor antibody (TSH Ab) level of 35.65 IU/L (reference range: 0–1.75 IU/L), thyroglobulin antibody and thyroid peroxidase antibody levels were negative. Hematological and biochemical investigations were within normal limits, including serum creatinine, lipid profile, and plasma glucose. There was no heart failure, pulmonary hypertension, renal disease, or liver disease.
In the thyroid ultrasound examination, the left lobe of the thyroid was small, measuring 0.8 cm x 0.8 cm x 1.7 cm, and the right lobe was unvisualized, indicating either after thyroidectomy. The isthmus of the thyroid measured 0.2 cm and volumetric analysis showed Vs=0.5 cm³, Ve=0.5 cm³. Thyroid parenchyma exhibited a diffusely heterogeneous texture, intermingled with areas of lower echogenicity.
Amplitude color Doppler demonstrated decreased vascularization of the thyroid gland.
Thyroid scintigraphy (Tc-99m Pertechnetate) examination reported known autoimmune thyroid disease with partial thyroidectomy and RAIT status: no significant enlargement of the residual thyroid glands and mild increased activity.
The foot examination revealed hyperpigmented indurated plaques with boggy non-fitting edema on the lower shins extending to the dorsal feet bilaterally with “peau d’orange” appearance (Figure 2). Histopathological analysis was performed on two pieces of 1.5 cm samples from the lesion in the right dorsoplantar area, stained with Alcian blue and Van Giesen, revealing myxedema skin. Positive staining with Alcian blue and Van Giesen stains indicated the presence of mucopolysaccharides and increased collagen deposition.

Figure 2. Photograph of a skin lesion on foot from (A) the right side, (B) the left side (C) the front side, (D) the back side, (E) the plantar area.
In the foot X-ray report, no acute or chronic fracture, dislocation, or foot deformation was identified in either foot. Joint spaces between tarsal and metatarsal bones were within normal limits. The alignment of the bones appears anatomic. Soft tissue swelling was visualized in the tibial and dorsoplantar parts (Figure 3). Doppler ultrasound of the lower limbs was unremarkable. The lymphoscintigraphy revealed probable partial lymphatic flow obstruction in the left lower leg; otherwise, lymphatic flow was within normal limits throughout the right lower leg.
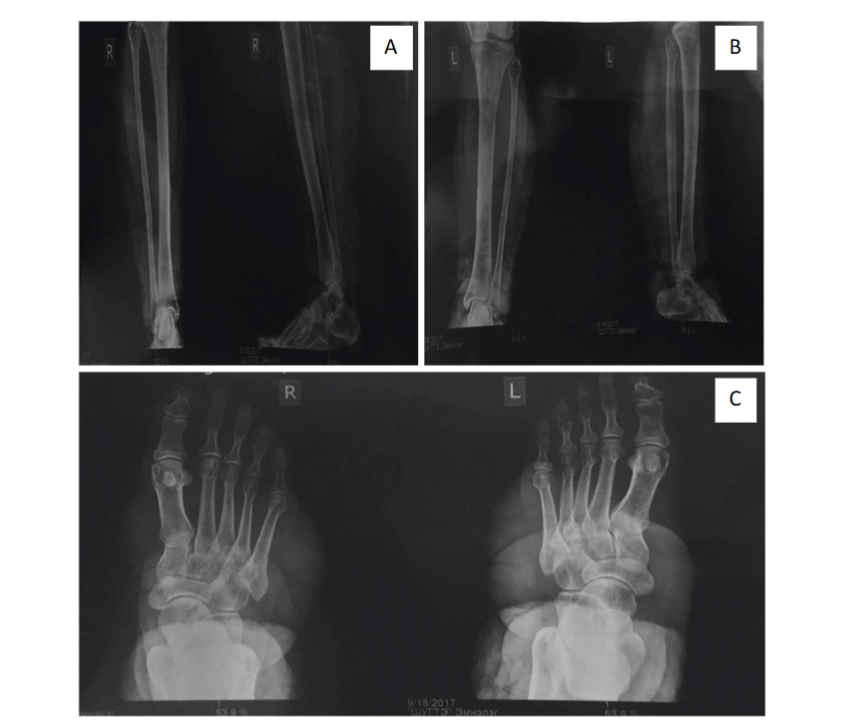
Figure 3. Foot X-rays. Anteroposterior and lateral radiographs of the right tibia and fibula (A), left tibia and fibula (B), and the dorsoplantar part (C).
3. Discussion
Pretibial myxedema is a significant and specific dermatological manifestation of Graves’s disease. Clinically, it appears as yellow-brown erythematous nodules and bilateral, asymmetrical, firm, non-pitting, and painless plaques. Pretibial myxedema may resemble skin lesions in conditions like necrobiosis lipoidica diabeticorum and various inflammatory dermatoses¹³. Lesions often appear after the onset of clinical hyperthyroidism; however, pretibial myxedema can occur at any stage of Grave’s disease, even years after the hyperthyroidism has been successfully treated¹⁴. The pathogenesis of pretibial myxedema involves lymphocytic infiltration, evident in early lesions, which leads to cytokine production. This process results in mucinous edema and fragmentation of dermal collagen fibers, with subsequent extension into deeper tissues¹⁵.
The thyroid-stimulating hormone receptor found in fibroblasts plays a crucial role with TRAb and/or antigen-specific T cells triggering an inflammatory response that increases hyaluronic acid production. Histological examination reveals abundant hyaluronic acid in biopsy specimens, a small number of lymphocytes, and a moderate increase in mast cells. The mucinous substance between collagen fibers can be identified using Alcian blue stain¹⁴.
Our case report presented the elephantiasis form of pretibial myxedema, a rare manifestation occurring in less than one percent of pretibial myxedema cases. Characteristics of elephantiasis pretibial myxedema include multiple nodular formation, massive edema, and skin hyperpigmentation¹¹. Differential diagnoses for this condition include secondary edema resulting from chronic lymphatic obstruction or venous insufficiency, diabetic dermopathy, lichen amyloidosis, hypertrophic lichen planus, and rarely pretibial epidermolysis bullosa. Several key features distinguish pretibial myxedema from lymphedema. Pretibial myxedema is associated with thyroid autoimmunity, whereas lymphedema results from lymphatic system dysfunction. Clinically, pretibial myxedema typically presents with non-pitting edema while lymphedema initially presents as pitting edema. Histopathologically, pretibial myxedema is characterized by mucin deposition and positive Alcian blue staining, unlike lymphedema, which involves lymphatic fluid accumulation and fibrosis¹⁶.
Topical and intralesional corticosteroid treatments are more commonly used than systemic treatments. Several reports investigated long-term follow-up revealed that a significant percentage of severe cases treated with local therapy as well as milder untreated cases, experienced partial or full remission⁵˒¹².
4. Conclusion
We describe a rare case of biopsy-proven pretibial myxedema in a Grave’s disease with a hypothyroid condition. Although uncommon, pretibial myxedema should be considered in the differential diagnosis when distinctive pretibial skin lesions are observed in hypothyroid patients. This is particularly important in settings where early diagnosis and immediate initiation of treatment are essential for effective management.
Conflicts of Interest Statement:
All authors have seen and approved the manuscript. The authors have no conflicts of interest to declare.
Acknowledgment:
The authors sincerely thank the patients who agreed to participate in this study. We extend our special thanks to the Department of Endocrinology at the Third Central Hospital of Mongolia, the Endomed Endocrinology Clinic, and the School of Medicine at the Mongolian National University of Medical Sciences for their invaluable support and collaboration.
References
1. Doshi, D. N.; Blyumin, M. L.; Kimball, A. B. Cutaneous manifestations of thyroid disease. Clin Dermatol 2008, 26 (3), 283-287. DOI: 10.1016/j.clindermatol.2007.10.020 From NLM.
2. Ambachew, R.; Yosef, T.; Gebremariam, A. M.; Demere, L.; Aberra, T.; Tarekegn, G.; Reja, A. Pretibial myxedema in a euthyroid patient: a case report. Thyroid Res 2021, 14 (1), 4.
DOI: 10.1186/s13044-021-00096-z From NLM.
3. Chen, M.; Ge, S.; Driscoll, M. Pretibial myxedema in a patient with HIV and hypothyroid to hyperthyroid transformation. JAAD Case Rep 2023, 36, 75-77. DOI: 10.1016/j.jdcr.2023.04.005 From NLM.
4. Nguyen, V. B.; Nguyen, V. V. H.; Van Le, C.; Linh, P. N. T.; Thi, X. N.; Vo, T. T. Pretibial myxedema in Grave’s disease: A case report and treatment review of the literature. Clin Case Rep 2024, 12 (2), e8478. DOI: 10.1002/ccr3.8478 From NLM.
5. Schwartz, K. M.; Fatourechi, V.; Ahmed, D. D.; Pond, G. R. Dermopathy of Graves’ disease (pretibial myxedema): long-term outcome. J Clin Endocrinol Metab 2002, 87 (2), 438-446. DOI: 10.1210/jcem.87.2.8220 From NLM.
6. Ajjan, R. A.; Weetman, A. P. Techniques to quantify TSH receptor antibodies. Nat Clin Pract Endocrinol Metab 2008, 4 (8), 461-468. DOI: 10.1038/ncpendmet0886 From NLM.
7. Oh, S. Y.; Cho, H. K.; Jung, Y. Y.; Lee, M.-K. A Case of Pretibial Myxedema Associated with Hypothyroidism and Thyroid-Stimulating Hormone Receptor Antibodies. Dermatologica Sinica 2019, 37 (3), 166-169. DOI: 10.4103/ds.ds_51_18.
8. Fatourechi, V. Pretibial myxedema: pathophysiology and treatment options. Am J Clin Dermatol 2005, 6 (5), 295-309. DOI: 10.2165/00128071-200506050-00003 From NLM.
9. Bruinstroop, E.; Cairo, I.; Drillenburg, P.; van Dam, P. S. Hypothyroidism to Graves’ disease and late appearance of pretibial myxoedema. Lancet 2019, 394 (10206), 1364. DOI: 10.1016/s0140-6736(19)32281-0 From NLM.
10. Sabanova, E. A.; Fadeyev, V. V.; Potekaev, N. N.; Lvov, A. N. [Pretibial myxedema: pathogenetic features and clinical aspects]. Probl Endokrinol (Mosk) 2019, 65 (2), 134-138. DOI: 10.14341/probl9848 From NLM.
11. Chen, C. T.; Lin, J. C. Elephantiasic pretibial myxoedema. Indian J Med Res 2013, 137 (3), 568. From NLM.
12. Lan, C.; Wang, Y.; Zeng, X.; Zhao, J.; Zou, X. Morphological Diversity of Pretibial Myxedema and Its Mechanism of Evolving Process and Outcome: A Retrospective Study of 216 Cases. J Thyroid Res 2016, 2016, 2652174. DOI: 10.1155/2016/2652174 From NLM.
13. Nair, P. A.; Mishra, A.; Chaudhary, A. Pretibial Myxedema Associated with Euthyroid Hashimoto’s Thyroiditis: A Case Report. J Clin Diagn Res 2014, 8 (6), Yd01-02. DOI: 10.7860/jcdr/2014/6581.4415 From NLM.
14. Bartalena, L.; Fatourechi, V. Extrathyroidal manifestations of Graves’ disease: a 2014 update. J Endocrinol Invest 2014, 37 (8), 691-700. DOI: 10.1007/s40618-014-0097-2 From NLM.
15. Kahaly, G.; Förster, G.; Hansen, C. Glycosaminoglycans in thyroid eye disease. Thyroid 1998, 8 (5), 429-432. DOI: 10.1089/thy.1998.8.429 From NLM.
16. Lebreton, O.; Seddiki, R.; Abba, S.; Vignes, S. [Pretibial myxedema after Graves’ disease: A differential diagnosis of lymphedema]. Rev Med Interne 2023, 44 (12), 641-645. DOI: 10.1016/j.revmed.2023.09.003 From NLM.
Most read articles by the same author(s)
- Davaasuren Damdindorj, Oyunbileg Bavuu, Bolormaa Ganbaatar, Sainbileg Sonomtseren, Bayasgalan Tumenbayar, A Comprehensive Analysis of Clinical and Laboratory Characteristics of Thyroid Abnormalities in a Two-Year Outpatient Cross-Sectional Study , Medical Research Archives: Vol 12 No 3 (2024): March issue, Vol.12, Issue 3