





Bronchoscope Reprocessing: Enhancing Infection Prevention
Bronchoscope Reprocessing and the Value of Visualization
Christopher Yurosko DO¹; Karan Amlani MD¹; Atul Mehta MD¹
- Respiratory Institute, Cleveland Clinic, Cleveland, OH, USA
OPEN ACCESS
PUBLISHED:31 August 2024
CITATION: Yurosko, C., Amlani, K., et al., 2024. Bronchoscope Reprocessing and the Value of Visualization. Medical Research Archives,
[online] 12(8).https://doi.org/10.18103/mra.v12i8.5487
COPYRIGHT: © 2024 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v12i8.5487
ISSN 2375-1924
Abstract
The risk of infection and contamination of endoscopes is well known. Current guidelines recommend that experts perform regular audits to ensure sufficient reprocessing practices. Borescopes have a role to play in endoscope reprocessing by allowing thorough visual inspection, ensuring effective cleaning, and reducing the risk of cross-contamination. However, a greater understanding of what types of defects can be tolerated without raising infection risk and which require the endoscope to be repaired before use.
Keywords
Bronchoscopy Reprocessing, Borescope, Disinfection, Contamination
Purpose of Review:
Bronchoscopy related infection is recognized as a leading cause of healthcare hazard and this review delves into its incidence, causes and prevention.
Introduction
There is an emphasis on the now well-recognized challenge of the risk of infections and contaminations associated with endoscopic procedures and reprocessing of devices. In 2019, the Emergency Care Research Institute (ECRI), an independent healthcare technology and safety organization, identified recontamination of endoscopes after disinfection as the top 10 health technology hazards. Additionally, the Center for Disease Control (CDC) Division of Healthcare Quality Promotion (DHQP) conducted several separate investigations of bronchoscopy-associated outbreaks involving around 150 patients throughout 2014-2019. In 2021, The U.S. Food and Drug Administration (FDA) updated its safety communication on reprocessed flexible bronchoscopes to its original communication in 2015; this update came after the FDA reviewed 867 Medical device reports (MDR) associated with contamination or infection of reusable flexible bronchoscopes between 2015-2021.
A review of infections related to bronchoscope procedures highlighted factors contributing to infection, including failure to follow manufacturer instructions or continued use of devices despite integrity, maintenance, and mechanical issues. The FDA communication also outlined recommendations for bronchoscopy reprocessing and advocated for sterilization over high level disinfection (HLD). Single-use flexible bronchoscopes (SUFB) are recommended when there is an increased risk of spreading infection. A consensus statement from the American College of Physicians (ACCP) and American Association of Bronchology on the prevention of bronchoscopy-associated infections, though long due for an update, did put a big spotlight on this issue and provided strong recommendations on preventive measures and reprocessing steps for bronchoscopes.
This review article briefly summarizes the steps involved in reprocessing flexible bronchoscopes and the potential associated challenges. It aims to promote better education and implementation to reduce the risk of infection/contamination. Additionally, this article investigates using borescope as an inspection tool and its currently reported utility.
Reprocessing and its challenges
Currently, reprocessing guidelines for medical devices are based on CDC’s adopted Spaulding Classification. For more than 60 years, it has served as the framework for medical device disinfection and sterilization process. As medical technology advances, leading to the innovation and development of more complex devices, significant concerns have been raised about the continued viability of the Spaulding Classification system. Studies have acknowledged the need for an updated or revised system to promote appropriate standards for medical device reprocessing to uphold patient safety.
Based on the Spaulding classification, the bronchoscope is categorized as a semi-critical device, encompassing equipment that encounters mucous membranes or nonintact skin. This classification mandates HLD reprocessing as the acceptable minimum. In contrast to HLD, sterilization destroys all microorganisms on equipment or in liquid, while HLD destroys viruses, fungi, some bacterial spores, and vegetative bacteria.
During routine use, reusable bronchoscopes can become heavily contaminated and, if improperly or inadequately cleaned and reprocessed, can inadvertently be associated with infection. Indeed, several outbreaks of multidrug-resistant organisms have been associated with reusable bronchoscopes. The bronchoscope-associated infection has been linked to contamination even when reprocessing was done well.
Cleaning and reprocessing a bronchoscope involves several critical steps well described in the literature. The initial step for reprocessing is the pre-cleaning with the intended goal to prevent biofilm formation. The next step is leak testing, which evaluates for damage to the internal channels of the bronchoscope and the external surface. Leak testing has been suggested to reduce repair costs and extend the life of the bronchoscope. Next is manually cleaning the internal and external surfaces using specialized channel cleaning brushes, detergents, or enzymatic cleaners. Following manual cleaning is a visual inspection under high magnification and often enlists using a borescope. There are also emerging technologies using artificial intelligence to identify working channel defects and residues. After the visual inspection, HLD is carried out. This is achieved by perfusing the channels of the bronchoscope with a chemical sterilant to ensure that the entirety of the channel is in contact. Next, the bronchoscope is rinsed with either sterile water or filtered water in the case of automated endoscope reprocessor’s (AER). This is intended to remove the disinfectants used during the HLD step. Improper rinsing can harm patients as the residual chemicals cause injury and anaphylaxis. Finally, the bronchoscope is dried. This is a critical step and has been identified as a potential source for contamination and outbreak. Despite the known concern, there are no clear guidelines on approaching this step, and each institution has its approach. Following the cleaning and reprocessing, the bronchoscope is stored. This is done by hanging the bronchoscope vertically in cabinets. There is a recommendation to use cabinets with circulating high efficiency particular absorbing (HEPA) filtered air over static air to prevent recontamination.
VISUALIZATION STEP: WHY IS VISUALIZATION SO TRICKY?
Damage that goes unnoticed in the interior channels of endoscopes, like deep grooves and scratches, can operate as havens for bacteria, make manual cleaning and HLD more complex, and even increase the risk of infection transfer. With the rising awareness of endoscope-related infections, borescopes are increasingly available to diagnose and guide the repair of endoluminal defects. A borescope, like an endoscope in design, is a small optical instrument that can be inserted into the working channel of an endoscope for purposes of visual examination.
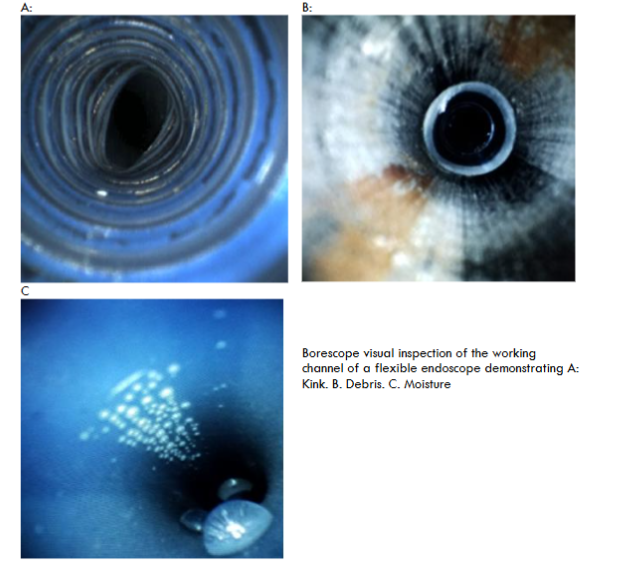
Examination of the inner aspects of the working channel is for any apparent defect or debris. Defects reported include discoloration, scratches, dents, perforations, and residual fluid within the working channel.
A study from 2018 by Barakat et al. describes a systematic approach to grading and characterizing findings during borescope examination. To assist in the evaluation, many borescopes are designed to be able to record and save both still and video images. This is an additional quality measure for assurance of endoscope reprocessing.
Most of the data evaluating the benefit of using a borescope as an additional tool for inspection and quality monitoring is based on gastrointestinal endoscopy. Alarming results were noticed in a prospective 2018 study that adopted a borescope. Twenty-four clinically used bronchoscopes (therapeutic, pediatric, and endobronchial ultrasound (EBUS)) were evaluated with culture samples from ports and distal ends. Microbiological growth was found in 55% of the manually cleaned bronchoscopes and 58% in the fully reprocessed (HLD) bronchoscopes. Internal examination with a borescope demonstrated fluid, discoloration, scratches, filamentous debris, and dented channels in all bronchoscopes (100%). They did not find any association between bronchoscopes with these irregularities and the age of the bronchoscope or the site utilized.
During the HLD process, borescopes were used to assess drying and storage practices. A study by Ofstead et al. evaluated 45 endoscopes from three different sites. Residual fluid was found in 45% (21/45) of endoscopes. Notably, all the endoscopes found to have residual fluid were from two sites, while the third had no evidence. During further investigation, those two sites with residual fluid followed substandard reprocessing practices, including drying and storage. Within the gastrointestinal literature, a review of 68 endoscopes was inspected. They noted that some form of damage was noted on all endoscopes. However, no endoscope demonstrated severe working channel damage (including deep scratches, burns, and channel perforations) that would require endoscope repair. Of the endoscopes evaluated, 67/68 had visualized scratches, and 52/68 had scratches associated with the peeling of small strips of the inner lining of the endoscope working channel. Debris was seen in 65/68, consisting of localized small linear black or white particulate matter. Residual fluid was seen in 29/68 working channels, and no biofilms were evident.
Many questions remain regarding using borescopes to assist with visual examination during reprocessing and care. Of the many, it is essential to understand the implications of each finding by a borescope and how reliably they can be identified. Additionally, considerable time for training technicians remains a barrier. There will always be interobserver heterogeneity in identifying and grading the extent of functioning channel damage. There is also an inevitable level of human error in this process. There has been interest in leveraging artificial intelligence (AI) to combat this dilemma. Combined with human efforts, it has been shown to routinely outperform human efforts alone in visual diagnosis in radiology and pathology. Recently, it has been used to increase yield in gastrointestinal endoscopy. A recent study by Barakat et al. evaluated AI’s first application and integration in the visual inspection and identification of working channel abnormalities within endoscopes. The results of the AI findings were compared to a consensus by three endoscopists. The overall sensitivity of the AI findings was 91.4%. The read-to-read variability was minimal and reported to have a test-retest.
Conclusion
Current guidelines recommend that experts perform regular audits to ensure sufficient reprocessing practices. Borescopes have a role to play in endoscope reprocessing by allowing thorough visual inspection and ensure effective cleaning and reduce the risk of cross-contamination. However, a greater understanding of what types of defects can be tolerated without raising infection risk, and which require the endoscope to be repaired before use. Looking ahead, advancements in borescope technology could lead to greater efficiency and accuracy in reprocessing procedures. Integration of features like automated image analysis could streamline inspections and enhance quality control, ultimately improving patient safety.
References
- Bardossy A, Novosad S, Perkins K, Moulton-Meissner HA, Arduino M, Benowitz I. Bronchoscope-Related Outbreaks and Pseudo-Outbreaks: CDC Consultations—United States, 2014–2019. Infect Control Hosp Epidemiol. 2020;41(S1):s144-s144. doi:10.1017/ice.2020.660
- Ofstead CL, Quick MR, Wetzler HP, et al. Effectiveness of Reprocessing for Flexible Bronchoscopes and Endobronchial Ultrasound Bronchoscopes. Chest. 2018;154(5):1024-1034. doi:10.1016/j.chest.2018.04.045
- Wendt C, Kampf B. Evidence-based spectrum of antimicrobial activity for disinfection of bronchoscopes. J Hosp Infect. 2008;70 Suppl 1:60-68. doi:10.1016/S0195-6701(08)60014-6
- Machado AP, Pimenta ATM, Contijo PP, Geocze S, Fischman O. Microbiologic profile of flexible endoscope disinfection in two Brazilian hospitals. Arq Gastroenterol. 2006;43(4):255-258. doi:10.1590/s0004-28032006000400002
- Gillespie EE, Kotsanas D, Stuart RL. Microbiological monitoring of endoscopes: 5-year review. J Gastroenterol Hepatol. 2008;23(7 Pt 1):1069-1074. doi:10.1111/j.1440-1746.2007.05264.x
- Gavaldà L, Olmo AR, Hernández R, et al. Microbiological monitoring of flexible bronchoscopes after high-level disinfection and flushing channels with alcohol: Results and costs. Respir Med. 2015;109(8):1079-1085. doi:10.1016/j.rmed.2015.04.015
- Mughal MM, Minai OA, Culver DA, Mehta AC. Reprocessing the bronchoscope: the challenges. Semin Respir Crit Care Med. 2004;25(4):443-449. doi:10.1055/s-2004-832717
- A Brief Look at ECRI Institute’s 2019 Top 10 Health Technology Hazards. J Radiol Nurs. 2019;38(1):2-4. doi:10.1016/j.jradnu.2019.01.001
- Infections Associated with Reprocessed Flexible Bronchoscopes: FDA Safety Communication. Published September 17, 2015. Accessed April 22, 2024. https://www.fda.gov/medical-devices/medical-devices-news-and-events/fda-issues-two-warning-letters-leading-manufacturer-endoscopes
- Andersen CØ, Travis H, Dehlholm-Lambertsen E, Russell R, Jørgensen EP. The Cost of Flexible Bronchoscopes: A Systematic Review and Meta-analysis. PharmacoEconomics – Open. 2022;6(6):787-797. doi:10.1007/s41669-022-00356-0
- Mehta AC, Prakash UBS, Garland R, et al. American College of Chest Physicians and American Association for Bronchology [corrected] consensus statement: prevention of flexible bronchoscopy-associated infection. Chest. 2005;128(3):1742-1755. doi:10.1378/chest.128.3.1742
- Rutala W, Weber D, Healthcare Infection Control Practices Advisory Committee (HICPAC). Guideline for Disinfection and Sterilization in Healthcare Facilities, 2008; Miscellaneous Inactivating Agents. Published online May 2019. Accessed April 22, 2024. https://www.cdc.gov/infectioncontrol/guidelines/disinfection/index.html
- Rutala WA, Kanamori H, Sickbert-Bennett EE, Weber DJ. What’s new in reprocessing endoscopes: Are we going to ensure “the needs of the patient come first” by shifting from disinfection to sterilization? Am J Infect Control. 2019;47S:A62-A66. doi:10.1016/j.ajic.2019.01.017
- Rowan NJ, Kremer T, McDonnell G. A review of Spaulding’s classification system for effective cleaning, disinfection and sterilization of reusable medical devices: Viewed through a modern-day lens that will inform and enable future sustainability. Sci Total Environ. 2023;878:162976. doi:10.1016/j.scitotenv.2023.162976
- Zweigner J, Gastmeier P, Kola A, Klefisch FR, Schweizer C, Hummel M. A carbapenem-resistant Klebsiella pneumoniae outbreak following bronchoscopy. Am J Infect Control. 2014;42(8):936-937. doi:10.1016/j.ajic.2014.04.022
- Mehta AC, Muscarella LF. Bronchoscope-Related “Superbug” Infections. Chest. 2020;157(2):454-469. doi:10.1016/j.chest.2019.08.003
- Culver DA, Gordon SM, Mehta AC. Infection control in the bronchoscopy suite: a review of outbreaks and guidelines for prevention. Am J Respir Crit Care Med. 2003;167(8):1050-1056. doi:10.1164/rccm.200208-797CC
- Shellnutt C. Advances in Endoscope Reprocessing Technology and Its Impact on Pathogen Transmission. Gastroenterol Nurs Off J Soc Gastroenterol Nurses Assoc. 2016;39(6):457-465. doi:10.1097/SGA.0000000000000267
- Yassin MH, Hariri R, Hamad Y, Ferrelli J, McKibben L, Doi Y. Disposable Bronchoscope Model for Simulating Endoscopic Reprocessing and Surveillance Cultures. Infect Control Hosp Epidemiol. 2017;38(2):136-142. doi:10.1017/ice.2016.264
- Chhabria MS, Maldonado F, Mehta AC. Infection control in the bronchoscopy suite: effective reprocessing and disinfection of reusable bronchoscopes. Curr Opin Pulm Med. 2023;29(1):21-28. doi:10.1097/MCP.0000000000000925
- Rojo C. The Importance of Leak Testing Flexible Endoscopes: 1.6 www.aornjournal.org/content/cme. AORN J. 2018;108(6):622-632. doi:10.1002/aorn.12425
- Avasarala SK, Muscarella LF, Mehta AC. Sans Standardization: Effective Endoscope Reprocessing. Respiration. 2021;100(12):1208-1217. doi:10.1159/000517335
- Barakat MT, Girotra M, Banerjee S. Initial application of deep learning to borescope detection of endoscope working channel damage and residue. Endosc Int Open. 2022;10(01):E112-E118. doi:10.1055/a-1591-0258
- FDA-Cleared Sterilants and High Level Disinfectants with General Claims for Processing Reusable Medical and Dental Devices. Published online November 30, 2023.
- Klacik SG. Transitioning from High-Level Disinfection to Sterilization for Semicritical Devices. Biomed Instrum Technol. 2019;53(s2):23-31. doi:10.2345/0899-8205-53.s2.23
- Behm T, Robinson N. Sterilization Central: Drying and Storage of Flexible Endoscopes: An Area of Growing Concern. Biomed Instrum Technol. 2020;54(3):223-227. doi:10.2345/0899-8205-54.3.223
- VerifEye 2.0 Video Borescope | STERIS. https://www.steris.com/healthcare/products/sterile-processing-department-accessories/verifeye-2-video-borescope
- Barakat MT, Girotra M, Huang RJ, Banerjee S. Scoping the scope: endoscopic evaluation of endoscope working channels with a new high-resolution inspection endoscope (with video). Gastrointestinal Endoscopy. 2018;88(4):601-611.e1. doi:10.1016/j.gie.2018.01.018
- Ofstead CL, Heymann OL, Quick MR, Eiland JE, Wetzler HP. Residual moisture and waterborne pathogens inside flexible endoscopes: Evidence from a multisite study of endoscope drying effectiveness. American Journal of Infection Control. 2018;46(6):689-696. doi:10.1016/j.ajic.2018.03.002
- Visrodia K, Petersen BT. Borescope examination: Is there value in visual assessment of endoscope channels? Gastrointest Endosc. 2018;88(4):620-623. doi:10.1016/j.gie.2018.07.005