






Glycemic Index of Vidavance®: A Diabetes Snack Study
Glycemic Index of Vidavance®, a High Protein and High Fiber Oral Snack Replacement Therapy for Diabetes Patients
Sabharwal M¹, Srivastava PK², Mishra A³, Pillai P³, Mehndiratta C³
- Dharma Dibeto Clinics, Greater Kailash II, New Delhi, India 110 006
- Mediception Science Pvt Ltd, Gurgaon, India 122 018
- Signutra Inc. Nehru Place, New Delhi, India 110 019
OPEN ACCESS
PUBLISHED: 31 July 2024
CITATION: M, Sabharwal, P.K. Srivastava, et al., 2024. Glycemic Index of Vidavance®, a High Protein and High Fiber Oral Snack Replacement Therapy for Diabetes Patients. Medical Research Archives, [online] 12(7).https://doi.org/10.18103/mra.v12i7.5420
COPYRIGHT: © 2024 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v12i7.5420
ISSN 2375-1924
Abstract
Background: Food products with a low Glycemic index (GI) and low Glycemic load (GL) help control blood glucose levels, and reduce the risk of diabetes-related morbidity and mortality. Vidavance®, an oral nutritional supplement (ONS) and Medical Nutrition Therapy (MNT) for pre-diabetes and diabetes has high-quality protein blend (soy protein isolate, calcium caseinate), dietary fiber (polydextrose, soy fiber), modified maltodextrin, chromium, and zinc, which are known to influence blood glucose control.
Aim: To determine the GI and GL of the Vidavance® in 31 people with diabetes (T2DM) aged 18 to 60 years, with fasting blood glucose (FBG) >120 mg / dL.
Methodology: The study participants consumed reference food (27.5 g of glucose monohydrate dissolved in 125 ml of water) followed by a three-day washout period. Then Vidavance® test dose (53 g available carbohydrate/100 gm) was given as 47.1.g of ONS mixed in 100 ml water to make up 390 ml). Continuous Glucose Monitoring reading was taken at 0, 15, 30, 45, 60, 90, and 120 minutes after the start of the test meal. The GI was assessed using a validated protocol by FAO and ISO (2010).
Results: 30 participants completed the study, (Mean age 55.2 ± 13.0 years.). The GI of the test food (Vidavance®) was 30.57 (low GI). No hyperglycemic events were observed during the study. The GI value was not influenced by age (years), sex, previous day’s dietary intake energy (kcal), and physical activity level. The GL of the test food was 3.85 (low GL).
Conclusion: Vidavance® is a low GI and low GL ONS and hence suitable for diabetic subjects.
Keywords: Glycemic index, nutritional supplement, weight loss, diabetes, CGM
Introduction
Diabetes is a global pandemic. Globally, one in seven people with diabetes (PD) is an Indian. The global PD number is predicted to rise by 69% by 2045. Type 2 Diabetes (T2D) is a major contributor to this increase and is related to changes in lifestyle. Indians are genetically and metabolically at higher risk of developing diabetes. This is further complicated by the increased use of fast food, refined food, sweetened beverages, high-calorie food, and a mechanized low-activity/sedentary lifestyle. Together these factors contribute to the higher incidence of diet-related non-communicable diseases (DR-NCDs) like T2D and obesity (diabesity) in India. Further, the recent ICMR-INDIAB-13 study showed that only 36.3% of the PD in India had achieved good glycemic control.
Though many pharmacological strategies are available to manage diabetes, diet and exercise are important components of a diabetes care program. Medical Nutrition Therapy (MNT) is an important diabetes management strategy. MNT encompasses individualized diet plans and regular monitoring by registered dieticians and clinicians.
PD are advised to consume carbohydrates with low Glycemic index (GI) and Glycemic load (GL) as a low GI diet is associated with a decrease in glycosylated hemoglobin (HbA1c), postprandial glucose (PPG), and fewer hypoglycemic episodes than a high GI diet. Along with it, the diet should contain good quality proteins, fats, and micronutrients in the right proportion.
Vidavance® is a proprietary oral nutritional supplement (ONS; Signutra Inc) designed to fulfill the dietary needs of PD and/or people at risk of these (T2DM and pre-diabetes). It comprises of a high-quality protein blend (soy protein isolate, calcium caseinate), dietary Fiber (polydextrose, soy fiber), modified maltodextrin, chromium, and zinc, which are known to influence blood glucose control.
The primary objective of the study was to estimate the GI and GL value of Vidavance®, in subjects with diabetes (T2DM). The secondary objective was to capture any hypoglycemic event (blood sugar level <70 mg/dl) within a period of 24 hours after giving Vidavance®.
Methodology
Study Subjects
Thirty-one participants from the participant roster of Glycemic Index Testing Centre – Dharma Diabeto Center, New Delhi, aged 18-60 years, with a fasting blood glucose (FBG) >120 mg / dL, no known food allergy or intolerance, and who were not taking any medications known to affect glucose tolerance were included in the analysis. The study excluded participants who had dietary restrictions required to manage diabetes, pregnant and lactating women, individuals recently diagnosed with impaired glucose tolerance, those with any acute or chronic conditions, individuals on medications that could affect nutrient absorption or carbohydrate metabolism, and those who had experienced a major medical or surgical event within the past three months. Study subjects may or may not have been receiving diabetes treatment.
Study Design
This was an observational, single-center, single-arm, study to determine the GI and GL value of Vidavance®, in patients with diabetes. Vidavance® is a scientifically designed Medical Nutrition Therapy (MNT) that helps decrease postprandial glycemia and supports diabetes control in T2DM and prediabetic patients. The primary investigator followed the Internationally recognized GI protocol issued by the Food and Agriculture Organization (FAO) / World Health Organization (WHO), 1998, and guidelines endorsed by the International Dietary Carbohydrate Task Force for GI methodology. Additionally, also followed the International Organization for Standardization (ISO) method (ISO 26642‑2010), which is validated and published elsewhere.
Test and Reference Food
Vidavance®, the test food for the study is an ONS (diabetic snack replacement medical nutrition therapy) from Signutra Inc. Proximate composition, available carbohydrates (estimated by a direct method, Megazyme Kit, Ireland), and total dietary fiber (Megazyme Kit, Ireland) were estimated at the Food Quality Analysis Lab of the Institution. Snack composition was maintained meeting caloric requirements with less amount of carbohydrate. The test dose was 53 g carbohydrate/100 gm given as 47.1 g of ONS mixed in 100 ml water to make up 390 ml). The reference food for the GI study was Glucose Monohydrate (27.5 g of glucose monohydrate dissolved in 125 ml of water).
Study Procedures
A recall questionnaire was circulated among the subjects before the start of the study. The questionnaire asked the subjects about their previous day’s meals (24-hour recall), physical activity, smoking, alcohol, and caffeine-containing drinks to ensure that they followed the same diet daily and performed the same level of physical activity on pre-test dates. The subjects were asked to avoid alcohol and tobacco during the study period. The subjects visited the GI testing centre (study site) each test day in the morning after 10-12 hours of overnight fasting.
Before administration of the test product, the subjects were first administered the reference food for three days. Blood samples were collected at 15, 30, 45, 60, 90, and 120 minutes after consuming glucose solution. After collecting blood glucose samples analysis was done within 30 minutes. This was followed by a washout period of 2-3 days to cancel out any possible carryover effects. The same 24-hour recall questionnaire was administered again. After this, the subjects were administered the test food for one day in random order. 31 subjects received 53 g of carbohydrates from 100 gm of nutritional product. A CGM device was attached (all participants received the same CGM device BeatO). FBG was measured at -5 minutes and 0 minutes by the CGM device before consumption of the food. The baseline values were taken as the mean of these two values. Within 12-15 minutes, the participants consumed Vidavance®. The first sip in the mouth was timed as 0 minutes and the first CGM reading was taken conventionally exactly 15 minutes after. CGM data was obtained at 15, 30, 45, 60, 90, and 120 minutes after the start of the test meal.
Data Analysis
The sample size was determined randomly based on the primary investigator’s considerations. The participants’ data were recorded in Microsoft Excel and the R version 4.2.2 was used to analyse the data. Data were represented as percentages, mean ± standard deviation, or median. To measure the Glycemic index of Vidavance®, an incremental area under the blood glucose response curve (IAUC) was plotted. The geometrical method using the trapezoidal rule was used to calculate the IAUC while the area below the fasting baseline level was ignored. GI value was calculated by expressing each participant’s AUC for the test food as a percentage of the same participant’s mean reference IAUC. The mean of the resultant was the GI of the test food.
GI value of test food (%) = Blood glucose (IAUC value for the test food) / IAUC value of the reference food × 100
The GI values were further tested to see the influence of age (years), sex, and previous days’ (of the reference and test food feeding) dietary intake [energy (kcal), protein (g), fat (g), carbohydrates (g), dietary fiber (g)] and physical activity level (PAL -sedentary, moderate, and vigorous levels) using a generalized linear model (GLM). The Glycemic load (GL) of the test food was calculated too.
The GL of the test food = GI of the test food x carbohydrate/100
Ethical Considerations
The evaluation process employed in the study was as per the international standards put forth for regulating ethical research with humans and was approved by the institutional ethics committee of The Good Society of Ethical Research, India on 13th July 2022 and all participants gave informed consent. The study has been registered with the clinical trial registry of India as CTRI/2022/07/056471.
Results
Thirty-one subjects were included in the analysis; 21 females and 10 males; the mean age of the participants was 55.2 ± 13.0 years. The participants had multiple symptoms of diabetes, its complications, and comorbid conditions as shown in Table 1.
| Symptoms of diabetes, its complications, and comorbid conditions | No of participants |
|---|---|
| Weakness | 27 |
| Lethargy | 28 |
| Nocturia | 22 |
| Polyuria | 19 |
| Constipation | 11 |
| Gastritis | 20 |
| Blurring vision | 11 |
| Tingling/burning sensation in legs | 16 |
| Hypoglycemia | 26 |
| Breathlessness | 9 |
| Cardiovascular disease | 5 |
| Chronic kidney disease | 1 |
| Hypertension | 1 |
| Dyslipidemia | 3 |
| Neuropathy | 1 |
CGM showed that postprandial blood glucose concentration (mg/dL) at 15, 30, 45, 60, 90, and 120 min after ingestion of test food (Vidavance®) was lower than the reference food (Glucose monohydrate). The blood glucose excursions (mg/dl) for 2 hours following the intake of test food were minimal, uniform, and sustained while following reference food consumption; the blood glucose levels exhibited a spike at around 15 minutes and then decreased gradually at 2 hours.
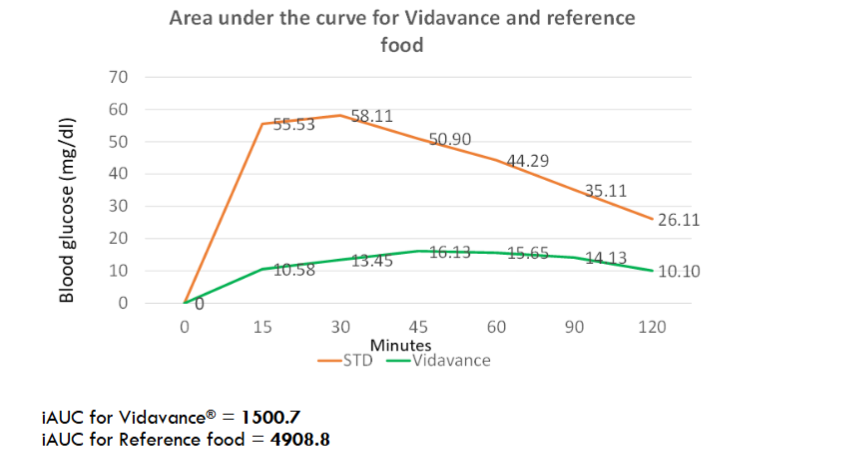
iAUC for Vidavance® = 1500.7
iAUC for Reference food = 4908.8
The GI of the test food was 30.57 (low GI). No hyperglycemic events were observed during the study. The GI value was not influenced by age (years), sex, and the previous day’s dietary intake [energy (kcal)]. The GL of the test food (Vidavance®) was 3.85 (low GL).
Discussion
Diet and exercise are important lifestyle management strategies for people with diabetes (PD). However, often this is the most neglected part of the diabetes management program, often due to a lack of time to prepare low GI and low GL meals. Thus, according to the ICMR-INDIAB-13 study, almost three-fourths of the PD need something apart from medications to control their blood sugar levels.
Low GI (GI<55) and low GL (<75) foods are considered ideal for patients with diabetes (PD). GI is a strong predictor of Glycemic variations and therefore it is important to determine the GI of food to understand the food’s impact on glycemia. GL is related to the carbohydrate content of the food. Low-carbohydrate and low-GI meals have a significantly lower PPG than low-GI high-carbohydrate meals.
High postprandial glucose is associated with DR-NCD. In this study, participants also had DR-NCDs like CVDs, CKD, and neuropathy. The study also showed that the participants had several symptoms of diabetes such as polyuria, nocturia, lethargy, weakness, tingling/burning sensation in legs, and blurring vision. These are indicative of poor PPG control.
Hence, lowering PPG is considered an important diabetes management strategy and is recommended by the International Diabetes Federation (IDF). Low GI/GL dietary interventions help in improving Glycemic control including lowering PPG. The PRIDE study (Partial meal Replacement on Glycemic level and Body weight in Indian Patients with T2DM) showed that partial meal replacement with ONS can positively impact FBG, PPG, and HbA1c, and can be an option to manage diabetes. Our study showed that the ONS Vidavance® has a low GI of 30.57 and low GL of 3.85, and is thus an ideal snack replacement for PD. We also show minimal Glycemic variation with Vidavance® and a decrease in PPG as compared to reference food.
The scientific and judicious blend of proteins, fibers, carbohydrates, and other nutrients in Vidavance® are likely to be responsible for the low GI/GL benefit and the PPG lowering effect. The key ingredients of interest in Vidavance® include soy protein isolate, calcium caseinate, soy Fiber, Polydextrose, modified maltodextrin, chromium, zinc, antioxidants, and vitamins.
The ingredients of Vidavance® also play an important role in decreasing the risk of diabetes. A high fiber, low GI, low GL nutrition blend with proteins and low-calorie carbohydrate significantly decreases the risk of diabetes as compared to a high GI, high GL and low fiber diet.
The maltodextrin component of Vidavance® is a low-palatable, viscous, fiber with ample evidence showing that it reduces the Glycemic response to food. There is a reduction in PPG as well.
Polydextrose is a low-calorie (only 1 kcal/g), sugar-free, low-GI (4–7) carbohydrate, that also improves satiety, and thus is ideally suited for a diabetic diet. Polydextrose reduces glucose absorption and thereby reduces its GI by 11%. When given in combination with soy protein or maltodextrin, as in Vidavance®, there is a reduction in energy intake, gastric emptying rate, appetite, and Glycemic response. Decreased food and energy intake helps in losing weight and thereby obesity-related diabetes.
Asian Indians are more susceptible to metabolic diseases owing to their protein deficit staple diet and relatively greater body fat than Caucasians. Vidavance® contains a high-quality blend of protein (soy protein isolate, calcium caseinate) with Protein Digestibility Corrected Amino Acid Score (PDCAAS) 1. A diet rich in high-quality protein can help induce satiety and reduce fat mass.
The micronutrient components present in Vidavance® are also beneficial for diabetes. E.g. Chromium enhances insulin activity, improves blood sugar metabolism, and decreases diabetes-associated oxidative stress. Zinc has a protective effect on vision and prevents diabetic retinopathy. High blood sugar increases the risk of retinopathy. 11 patients in this study complained of blurring vision before the test.
Judicious macronutrient and fiber composition of a diet can help change a high GI meal to a low GI meal with a significant reduction in PPG. Vidavance® is a low GI/GL option with high protein and soluble Fiber and other micronutrients conferring health benefits in diabetes. Hence, Vidavance® can be a healthy ONS and Medical Nutrition Therapy (MNT) of choice both for the prevention and control of diabetes.
Strengths And Limitations
The study shows that Vidavance® demonstrated a low GI/GL and reduction in PPG in a real-world setting, where participants ate their normal diet. We only standardized the same diet that they ate on the test day as taken on the previous day. The study, however, had some limitations. The study assessed the effect of a single meal replacement with Vidavance® for one day only. Physical activity can also affect the energy and blood glucose level. Hence, further trials are required to study the effect of Vidavance® when people go about their normal daily routine. The components of Vidavance® can also help in weight loss and this effect too can be studied in a real-world setting.
Conclusion
The Glycemic index of the Vidavance® is 30.57, which is below 55 and hence is classified as a low GI food product/ONS. The Glycemic load is 3.85 which is low GL. The GI value of Vidavance® was not influenced by age, sex, and dietary calories. Based on our study results, the ONS and MNT Vidavance® could be a suitable healthy supplement for diabetes. Future large-scale clinical trials are required to study the long-term effect of Vidavance® on diabetes and weight management.
Ethics Compliance
The study was approved by the Good Society Ethical Research-Independent Ethics Committee.
Conflict of interest: None
Funding: None
Acknowledgements: The authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this manuscript, take responsibility for the integrity of the work, and have given final approval for the version to be published. The authors thanks Pramod Pillai, Sanjay Singh of Signutra Inc and Mediception Science Pvt. Ltd. for providing medical writing support in the preparation of this manuscript.
References
- International Diabetes Federation P. Factsheets | IDF Diabetes Atlas; Tenth Edition. International Diabetes Federation; 2022. Accessed January 1, 2023. https://diabetesatlas.org/idfawp/resource-files/2021/11/IDF-Atlas-Factsheet-2021_SEA.pdf
- Singer ME, Dorrance KA, Oxenreiter MM, Yan KR, Close KL. The type 2 diabetes ‘modern preventable pandemic’ and replicable lessons from the COVID-19 crisis. Preventive Medicine Reports. 2022;25:101636. doi:10.1016/j.pmedr.2021.101636
- Pradeepa R, Mohan V. Epidemiology of type 2 diabetes in India. Indian Journal of Ophthalmology. 2021;69(11):2932-2938. doi:10.4103/ijo.IJO_1627_21
- Mohan V. Why are Indians more prone to diabetes? J Assoc Physicians India. 2004;52:468-474.
- Kapoor N, Sahay R, Kalra S, et al. Consensus on Medical Nutrition Therapy for Diabesity (CoMeND) in Adults: A South Asian Perspective. Diabetes Metab Syndr Obes. 2021;14:1703-1728. doi:10.2147/DMSO.S278928
- Anjana RM, Unnikrishnan R, Deepa M, et al. Achievement of guideline recommended diabetes treatment targets and health habits in people with self-reported diabetes in India (ICMR-INDIAB-13): a national cross-sectional study. The Lancet Diabetes & Endocrinology. 2022;10(6):430-441. doi:10.1016/S2213-8587(22)00072-9
- Thomas D, Elliott EJ. Low glycaemic index, or low glycaemic load, diets for diabetes mellitus. Cochrane Database Syst Rev. 2009;2009(1):CD006296. doi:10.1002/14651858.CD006296.pub2
- Wolever TMS, Gibbs AL, Chiasson JL, et al. Altering source or amount of dietary carbohydrate has acute and chronic effects on postprandial glucose and triglycerides in type 2 diabetes: Canadian trial of Carbohydrates in Diabetes (CCD). Nutr Metab Cardiovasc Dis. 2013;23(3):227-234. doi:10.1016/j.numecd.2011.12.011
- Misra A, Singhal N, Sivakumar B, Bhagat N, Jaiswal A, Khurana L. Nutrition transition in India: Secular trends in dietary intake and their relationship to diet-related non-communicable diseases. Journal of Diabetes. 2011;3(4):278-292. doi:10.1111/j.1753-0407.2011.00139.x
- Veena N, Surendranath B, Arora S. Polydextrose as a Functional Ingredient and its Food Applications: A Review. IJDS. 2016;69(3):239-251. doi:10.5146/IJDS.V69I3.51101.G24364
- Olli K, Salli K, Alhoniemi E, et al. Postprandial effects of polydextrose on satiety hormone responses and subjective feelings of appetite in obese participants. Nutrition Journal. 2015;14(1):2. doi:10.1186/1475-2891-14-2
- Soong YY, Lim WX, Leow MKS, Siow PC, Teh AL, Henry CJ. Combination of soya protein and polydextrose reduces energy intake and glycaemic response via modulation of gastric emptying rate, ghrelin and glucagon-like peptide-1 in Chinese. Br J Nutr. 2016;115(12):2130-2137. doi:10.1017/S0007114516001689
- Alptekin İM, Erdoğan E, İşler A, Yanalak EC, Çakiroğlu FP, Aras S. Short-term effects of milkshake containing polydextrose and maltodextrin on subjective feelings of appetite, energy intake and blood glucose in healthy females. Nutrition & Food Science. 2021;52(1):151-162. doi:10.1108/NFS-02-2021-0082
- Pesta DH, Samuel VT. A high-protein diet for reducing body fat: mechanisms and possible caveats. Nutrition & Metabolism. 2014;11. doi:10.1186/1743-7075-11-53
- Havel PJ. A scientific review: the role of chromium in insulin resistance. Diabetes Educ. 2004;Suppl:2-14.
- Rajendran K, Manikandan S, Nair LD, et al. Serum Chromium Levels in Type 2 Diabetic Patients and Its Association with Glycaemic Control. J Clin Diagn Res. 2015;9(11):OC05-OC08. doi:10.7860/JCDR/2015/16062.6753
- Miao X, Sun W, Miao L, et al. Zinc and Diabetic Retinopathy. J Diabetes Res. 2013;2013:425854. doi:10.1155/2013/425854
- Brouns F, Bjorck I, Frayn KN, et al. Glycaemic index methodology. Nutr Res Rev. 2005;18(1):145-171. doi:10.1079/NRR2005100
- Ceriello A. Postprandial hyperglycemia and diabetes complications: is it time to treat? Diabetes. 2005;54(1):1-7. doi:10.2337/diabetes.54.1.1
- International Standards Organization. ISO 26642-2010 Food Products Determination of the Glycemic Index (GI) and Recommendation for Food Classification. International Standards Organization; 2010. Accessed March 16, 2022. https://www.iso.org/cms/render/live/en/sites/isoorg/contents/data/standard/04/36/43633.html
- FAO/WHO. Carbohydrates in human nutrition. Report of a Joint FAO/WHO Expert Consultation. FAO Food Nutr Pap. 1998;66:1-140.
- Atkinson FS, Foster-Powell K, Brand-Miller JC. International Tables of Glycemic Index and Glycemic Load Values: 2008. Diabetes Care. 2008;31(12):2281-2283. doi:10.2337/dc08-1239
- Schwingshackl L, Hoffmann G. Long-term effects of low glycemic index/load vs. high glycemic index/load diets on parameters of obesity and obesity-associated risks: A systematic review and meta-analysis. Nutrition, Metabolism and Cardiovascular Diseases. 2013;23(8):699-706. doi:10.1016/j.numecd.2013.04.008
- Ceriello A, Colagiuri S. International Diabetes Federation guideline for management of postmeal glucose: a review of recommendations. Diabet Med. 2008;25(10):1151-1156. doi:10.1111/j.1464-5491.2008.02565.x
- Misra A, Sharma R, Gulati S, et al. Consensus Dietary Guidelines for Healthy Living and Prevention of Obesity, the Metabolic Syndrome, Diabetes, and Related Disorders in Asian Indians. Diabetes technology & therapeutics. 2011;13:683-694. doi:10.1089/dia.2010.0198
- American Diabetes Association. Postprandial Blood Glucose. Diabetes Care. 2001;24(4):775-778. doi:10.2337/diacare.24.4.775
- International Diabetes Federation. IDF Diabetes Atlas. Seventh edition. International Diabetes Federation; 2015. https://www.idf.org/component/attachments/attachments.html?id=728&task=download
- Dharmalingam M, Das R, Jain S, et al. Impact of Partial Meal Replacement on Glycemic Levels and Body Weight in Indian Patients with Type 2 Diabetes (PRIDE): A Randomized Controlled Study. Diabetes Ther. 2022;13(9):1599-1619. doi:10.1007/s13300-022-01294-0
- Bhupathiraju SN, Tobias DK, Malik VS, et al. Glycemic index, glycemic load, and risk of type 2 diabetes: results from 3 large US cohorts and an updated meta-analysis. Am J Clin Nutr. 2014;100(1):218-232. doi:10.3945/ajcn.113.079533
- Yeomans MR, Gray RW, Conyers TH. Maltodextrin preloads reduce food intake without altering the appetiser effect. Physiol Behav. 1998;64(4):501-506. doi:10.1016/s0031-9384(98)00086-9
- Livesey G, Tagami H. Interventions to lower the glycemic response to carbohydrate foods with a low-viscosity fiber (resistant maltodextrin): meta-analysis of randomized controlled trials. Am J Clin Nutr. 2009;89(1):114-125. doi:10.3945/ajcn.26842
- Sadakiyo T, Ishida Y, Inoue S ichiro, et al. Attenuation of postprandial blood glucose in humans consuming isomaltodextrin: carbohydrate loading studies. Food Nutr Res. 2017;61(1):1325306. doi:10.1080/16546628.2017.1325306
- Jie Z, Bang-Yao L, Ming-Jie X, et al. Studies on the effects of polydextrose intake on physiologic functions in Chinese people. Am J Clin Nutr. 2000;72(6):1503-1509. doi:10.1093/ajcn/72.6.1503
- Wilding JPH. The importance of weight management in type 2 diabetes mellitus. Int J Clin Pract. 2014;68(6):682-691. doi:10.1111/ijcp.12384
- Meena PC, Kumar S, Srinivas K, et al. Great Indian Food Paradox: Trends and Patterns. Agri Econ Rese Revi. 2016;29(conf):31. doi:10.5958/0974-0279.2016.00031.8
- Raji A, Seely EW, Arky RA, Simonson DC. Body fat distribution and insulin resistance in healthy Asian Indians and Caucasians. J Clin Endocrinol Metab. 2001;86(11):5366-5371. doi:10.1210/jcem.86.11.7992
- Right to Protein, Madan J. Indias-Protein-Paradox-Study.pdf. Accessed November 10, 2022. https://righttoprotein.com/assets/pdf/Indias-Protein-Paradox-Study.pdf
- Hoffman JR, Falvo MJ. Protein – Which is Best? J Sports Sci Med. 2004;3(3):118-130.
- Nisak MB, Ruzita AT, Norimah AK, Azmi KN, Fatimah A. Acute Effect of Low and High Glycemic Index Meals on Post-prandial Glycemia and Insulin Responses with Type 2 Diabetes Mellitus. Malaysian Journal of Medicine and Health Sciences. 2009;5(1):11-20. Accessed March 17, 2022. http://wprim.whocc.org.cn/admin/article/articleDetail?WPRIMID=628073&articleId=628073
- Vlachos D, Malisova S, Lindberg FA, Karaniki G. Glycemic Index (GI) or Glycemic Load (GL) and Dietary Interventions for Optimizing Postprandial Hyperglycemia in Patients with T2 Diabetes: A Review. Nutrients. 2020;12(6). doi:10.3390/nu12061561