

Abecedarian Lifespan Model: Enhancing Functional Intelligence
The Abecedarian Lifespan Approach to Learning and Functional Intelligence
Craig T. Ramey1 and Sharon L. Ramey1
- Fralin Biomedical Research Institute at VTC, Virginia Tech
OPEN ACCESS
PUBLISHED: 30 September 2025
CITATION: Ramey, CT. and Ramey, SL., 2025. The Abecedarian Lifespan Approach to Learning and Functional Intelligence. Medical Research Archives, [online] 13(9). https://doi.org/10.18103/mra.v13i9.6859
COPYRIGHT © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i9.6859
ISSN 2375-1924
ABSTRACT
In this summation of the Abecedarian Project (1971-2025) we present our lifespan biosocial model of learning that emphasizes the development of Functional Intelligence. Functional Intelligence is what an individual, at each age period and in dominant environmental contexts, accomplishes in socially-valued domains of living through thinking and behavior. The Abecedarian Project is a randomized controlled trial (RCT) to prevent intellectual and social subnormality in children born into extremely high-risk social and economic circumstances. A full-day, year-round early education program for the first 5 years of life was the core of the early intervention. The control group received nutritional supplements, pediatric care, and family social work services, as did the intervention group, but not the early education intervention. Teacher-child transactions were construed as Developmental Priming Mechanisms. The model specifies 5 cumulative learning and cognitive processes. Central features include recognizing culturally powerful ecological contexts and relevant domains of knowledge within those contexts. The initial goal of the early educational program was to promote cognitive and language development and ensure high levels of school preparedness at kindergarten entry. Evidence is provided that supports the conclusion that the Abecedarian Early Education Program positively affected assessed intelligence and developmental competence from 18 months through school entry, followed by consistently higher achievement in academic areas of reading and mathematics at all tested ages through early adulthood. Rates of retention in grade and placement in special education also were markedly reduced. Longer-term outcomes in adulthood, from their early 20s through middle age in their 30s and 40s, demonstrated significant benefits related to health, especially cardiovascular biomarkers, and increased functional intelligence (i.e., effective real-world thinking and acting) including attaining more years of education and degrees post-high school, having higher rates of full-time employment, greater self-sufficiency, closer positive relationships with both their mothers and fathers, displaying longer future planning horizons, adopting better decision-making strategies, and having evidence of structural brain differences in both overall cortex size and in 4 of 5 hypothesized brain regions theoretically linked to the early education intervention and active learning and language processes. We conclude that future early education interventions might usefully focus on understanding changes in developmental trajectories during and after the intervention and the forces that regulate both individual stability and change. Characterizations of impact might also seek to capture more fully the multiple experiential contexts where study participants spend time, both during and after the planned educational intervention, and identifying the types of functional intelligence skills that optimize success in those contexts. A joint focus on changes in developmental trajectories and the specification of important and facilitative (versus thwarting) contexts is consistent with a dynamic biosocial systems and its probabilistic, multi-domain perspective on human development. This conceptual framework puts the focus of scientific efforts relating to learning, health, educational achievement, personal life satisfaction, and becoming an engaged and contributory adult citizen on further specifying the effective (and sometimes alternative or compensatory) components to support developmental advances within and across the various functional domains as well as periods in the lifespan.
Keywords
Abecedarian Project, Functional Intelligence, Early Education, Lifespan Development, Cognitive Development
Introduction
Early experience is increasingly recognized as powerful in shaping developmental trajectories. Many scientific, educational, and therapeutic disciplines now feature special interest groups for infancy and early childhood. These specialty areas have been intensified due to increasing evidence that early childhood experiences significantly impact later functioning. The driving questions have been: Can systematic interventions improve developmental outcomes in vulnerable populations? If so, how? To what degree? The history of children with Down Syndrome is a good example. Until the 1970s, medical textbooks portrayed children with Down Syndrome as having very limited intellectual capability and self-help skills, accompanied by an expected short lifespan. Parents were frequently advised to place their children in institutions for the overall good of the family. Unfortunately, many institutions were merely custodial and the dismal professional predictions for low levels of achievement and poor health proved true. Some parents rejected this pessimistic prognosis and developed their own sets of supports and early education and learning opportunities for their children. Through research and case studies, evidence showed that increased early learning activities and living in supportive communities and a family context, attending local schools (outlawed for many in the U.S. until the 1970s), and engaging in a wide range of social and recreational activities, individuals with Down Syndrome now live and work in society as adults who, on average, realize far healthier, personally rewarding, and much longer and healthier lives. Concerted parent advocacy add immense support to the realization that early intervention and individualized learning opportunities are critical for all children diagnosed with developmental disabilities/delays to realize their full learning potential. This remarkable change within one or two generations refuted the idea that chromosomal and other biological differences were the primary factor for non-optimal outcomes for many clinical groups, and pointed to the profound influence of societal marginalization and exclusion from receiving high and appropriated levels of educational and health supports needed for all children to acquire Functional Intelligence skills and strategies and to live healthy adult lives, often independently. We propose that the dramatically improved outcomes from providing early universal education and evidence-based pediatric rehabilitation is a powerful harbinger of the potential for early intervention to improve the quality of life for all infants at elevated risk. This is a significant political issue in the United States and around the world; far too many people, groups, and nations still harbor the view that individual differences are a drain or burden on societal resources, rather than welcoming these as an integral, vibrant, and natural reality.
In 2019, the US Census Bureau projected that more than 3 million or over 4.3% of the under-18 population had a recognized disability. Worldwide, the estimates are even greater largely due to extremely low and unstable resources, chaotic environments, damaging discrimination, and wars. By what means and to what extent can early interventions alter the odds and costs of a developmental disability or a set of risk conditions? This disability/relative risk issue is vital to a society that cares for all its citizens. This topic involves everyone and warrants high priority; the potential rewards for all citizens have never been fully documented, and likely are notably high and enduring.
Two factors are germane to guide future activities to optimize early human development and reduce the incidence of childhood-onset and lifelong disabilities. First, is the need for a clear and widely shared understanding of how learning and the seeds of functional intelligence develop starting in infancy. Learning affects all aspects of functioning, including the domains of neuromotor, sensory, perceptual, language, cognitive, social, and emotional development. A shared understanding of the learning processes necessitates identifying the key individuals who guide children’s early lives, including parents, and extended kinship networks, health care and education providers, community recreational and arts programs, and spiritual and other value-based organizations. Second, is the need for a common conceptual framework to facilitate identifying and enhancing environmental affordances, while minimizing constraints and harm to developmental trajectories within major Developmental Contexts.
During the past 50+ years, we have been honored to lead and collaborate with multidisciplinary teams of scientists, interventionists/clinicians/educators, and families dedicated to finding effective interventions to improve developmental outcomes for highly vulnerable children. We have witnessed how practically useful a conceptual framework can be to improve communication and understanding so that they can transcend the unnecessarily complex worlds of disciplinary jargon and divisiveness about who or what is the most important in determining a life course. Our Framework is inductive and continues to develop as new discoveries are made.
The Abecedarian Conceptual Framework for the Development of Intellectual Competence
We have organized key influences on early human intellectual development into a Biosocial Contextual Systems Developmental Framework. Figure 1 provides an abbreviated schematic summary. We posit that an individual’s course of development is influenced by conditions that begin even before conception, shown as contextual forces in the top row of Figure 1. Examples include genetics, prenatal care and conditions, as well as family and community norms and practices within the larger society. If a therapy or educational practice begins at or near birth these influential contextual factors need to be considered and documented when evaluating results from particular interventions. These background and contemporaneous contextual factors, taken together, help shape the behavioral and neurobiological status of children and their family members. Some of these influences are recorded on US standard birth certificates and helped identify differential risks and needs for individualized learning opportunities in the Abecedarian Approach.
The center feature of Figure 1 is the box labeled Transactions with Others and the Environment. These dynamic transactions, influenced by many factors, comprise the major causal activities in the development of Functional Intelligence a term representing more than intelligence scores measured by currently available tools. Although intelligence tests can be informative, the Abecedarian Project focused more broadly on intelligence as lived. We developed a curriculum of progressively more advanced learning and language activities and provided ongoing professional development for all the center-based adults (see Ramey, Sparling, and Ramey, 2012). Embedded within this curriculum are experiences that we labelled as Developmental Priming Mechanisms that is, learning activities that adult teachers/caregivers incorporated into the planned and spontaneous transactions designed to encourage, shape, and advance cognitive development, communication skills, and social-emotional competence. Arrows in the schematic diagram highlight feedback loops representing reciprocal influences among participating individuals. Table 1 lists these specific Developmental Priming Mechanisms.
These priming mechanisms have been a focus of our work on family/child and teacher/child transactions since the project was being conceptualized in the late 1960s.
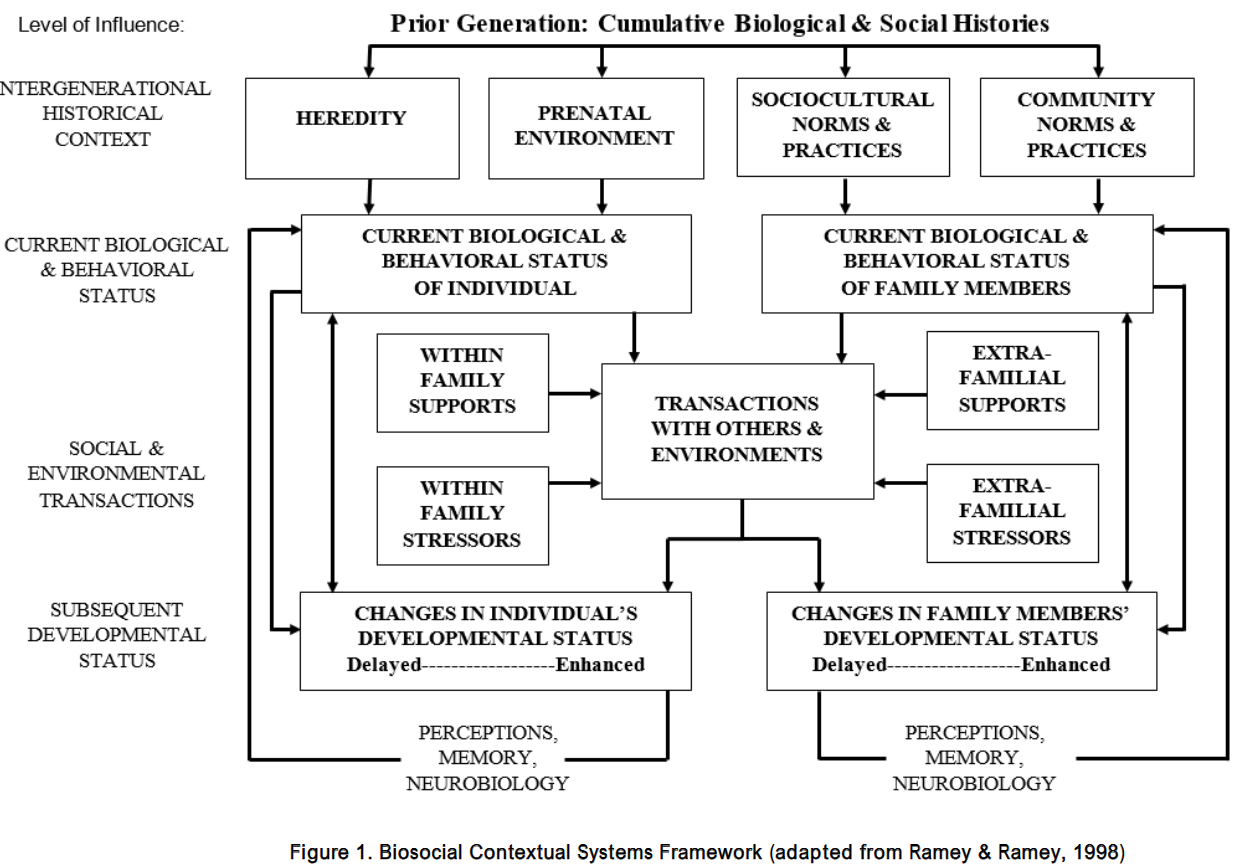
Table 1. Essential Transactions for Learning and Cognitive Development
| Encourage exploration with all the senses, in familiar and new places, with others and alone, safely and with joy. |
| Mentor in basic skills, showing the whats and whens, the ins and outs of how things and people work. |
| Celebrate developmental advances, for learning new skills, little and big, and for becoming a unique individual. |
| Rehearse and extend new skills, showing how to practice, in the same and different ways, with new people and new things. |
| Protect from inappropriate punishment. |
| Communicate richly and responsively with sounds, songs, gestures, and words. |
| Guide and limit behavior to keep children safe and to teach what’s acceptable, and what’s not—the rules of being a cooperative, responsive, and caring person. |
Positive behavioral transactions are causally linked to a child’s developmental advances. Key areas emphasized include: 1) specific learning activities to broaden knowledge and readiness for school at kindergarten entry; 2) language for both concept representation and social relationships; 3) conversational reading as an enjoyable activity promoting pre-literacy and storytelling; and 4) enriched positive caregiving to establish practical learning sets toward daily activities and trust in caring adults. We hypothesized that these enriched experiences would positively impact early brain development and better preparedness and functioning in K-12 schooling. Greater K-12 achievement was hypothesized to create greater self-sufficiency and accomplishment in adulthood, all other things being equal which they rarely are.
Abecedarian Types of Early Learning Leading to Functional Intelligence
Human learning is a process of adaptation to current and changing contexts or circumstances. These impinge on the child from the outside sources and internal processes, biological and cumulative memories, and reflections and new insights as they emerge. At its best, Functional Intelligence guides reasoning and strategizing about important issues, as well as acting responsibly and effectively, rather than reflexively or rigidly many of the processes now often grouped under terms such as metacognition and prefrontal cortex or Executive Functions.
Within our perspective we have come to differentiate five levels of learning, which begin in early childhood given appropriate social interactions and experiences propelled by mentors. For us, functional intelligence is incremental and cumulative. These processes can continue to be elaborated and refined throughout the lifespan. These learning processes are developed in conjunction with experience and self-appraisal or reflection and are often guided by more knowledgeable partners which include both adults and peers for young children. Our model of Functional Intelligence is depicted in Figure 2 and is a modification of an earlier conceptualization and schematic from Ramey and Blair (1996). These five levels of learning are each potentially applied, in sequence, to every domain of knowledge including academic, artistic, practical, athletic and so forth.
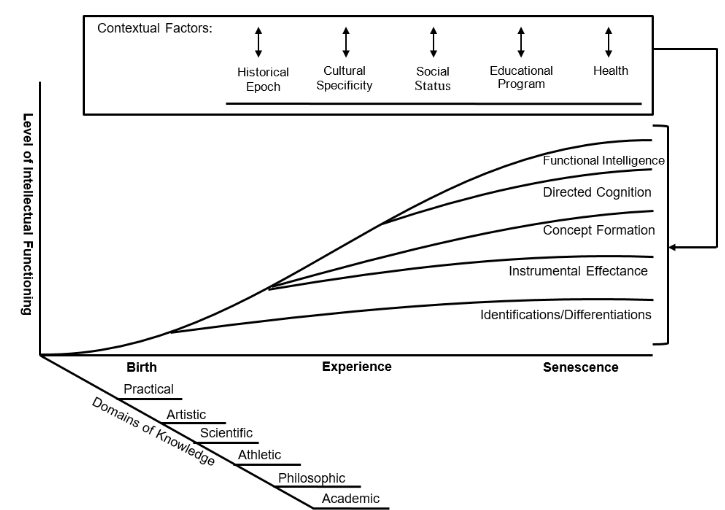
Levels of learning become established in an orderly manner in and across Domains of Knowledge.
As best as we can determine, these 5 levels of learning occur in all cultures. The magnitude of increases in intellectual and social competence from infancy to early and then middle childhood is simply breathtaking! This early learning occurs so rapidly because everything worth knowing has to be learned and practiced including: danger, sights, sounds, smells, tastes, textures, time, people, rules, strategies everything. All young children are potentially powerful biosocial learning machines with high potential. Accordingly, it is in the child’s and society’s best interest to ensure that each individual reaches increasingly higher stages/levels of Functional Intelligence. Worldwide this issue of maximizing Functional Intelligence is immense. We submit that outdated paradigms of societies that fix the levels of intellectual competence across subgroups create harmful consequences for individuals and the whole of society. For example, The World Health Organization now projects between 130 and 140 million annual births. Each child’s future will be created within a biosocial context with varying degrees of risk. Assuming at least a 3% likelihood of disabilities in the general world population, this will represent over 4.2 million new cases per year that may be amenable to successful treatment or prevention.
We regard advancing knowledge about Functional Intelligence as inherently a topic that necessitates longitudinal observations and analysis quite opposite from just storytelling or fact-free debate filtered through ideology and only personal experiences/memories. Cross-sectional analyses which measure separate groups of individuals at different ages are simply unable to address this issue adequately since change itself is not directly measured, and quite distinctive environmental and biological circumstances can influence different cohorts or ages sampled in cross-sectional datasets. The resulting curves generated from cross-sectional data may not accurately represent the course of individuals or even groups, and this may produce misleading or wrong impressions about the patterns that depict lives over time or the benefits from treatments and interventions provided.
Some communities, societies, and countries, for example, may want to reward innovation and risk-taking while others may encourage custom-oriented conformity and stability. Often, multiple groups within a context may diverge in their goals and strategies. This divergence can be the basis for constructive dialog and information exchange; alternatively, political, social, and economic factors can result in challenging, or even harmful disruptions to families and communities seeking to optimize opportunities for helping all young children to learn and thrive. We have applied our Conceptual Framework to multiple groups of children at high risk for or diagnosed with disabilities in more than a dozen countries. Some of our studies have been small-scale while others have involved thousands of participants. In total, over 78,000 children and their families have participated in our longitudinal research on interventions regarding developmental disabilities and functional intelligence. Some have begun prior to birth or early in infancy while others have begun later in early childhood. All of our research has dealt with the fundamental question of human potential for enhanced development beginning at various points in the lifespan that is, what does positive human malleability look like?
Human Malleability as a Controversy
Human malleability that is, the potential for individuals to change — has a long and controversial history in philosophy, literature, science, and politics. In the United States, racial and social class assumptions about malleability became cornerstones of national, state, and local public policies concerning civil liberties, education, housing, health care, employment, and marriage/partnerships. Scientists have contributed to the frequently heated debate with some individuals taking strongly predetermined and overly simplistic genetic views such as Galton (1883), Jensen (1969), and Herrnstein and Murray 1994) while others have favored an experiential or multifaceted point of view (e.g. Hunt, 1961; Bijou & Baer, 1961; Ceci, 1996; Blair & Raver, 2012; Ramey & Ramey, 2023); particularly with respect to learning and intelligence.
What became clear to many of us in the 1960s and 1970s was that this basic controversy needed a truly experimental and longitudinal approach (see, for example, Lazar et al…Ramey, 1982 for a detailed argument). The malleability controversy simply could not be adequately addressed via correlational analyses of naturalistic observations or cross-sectional epidemiological research due to the co-occurrence of many plausible causal factors.
The most basic practical and policy question concerning human malleability in the United States in the 1960s became whether individuals likely to have low tested Intelligence Quotients (IQs) or to experience inter-generational subnormal lives could benefit significantly if they were given access to more adequate and better organized resources. Chief among these hypothesized important resources were high-quality and responsive early care and education, as well as good health care, nutrition, and family support social services.
The Abecedarian Approach (summarized in Table 2) is a set of standards, resources, and practices derived from our biosocial conceptual framework that guided the first three RCT interventions: the Abecedarian Project, Project CARE, and The Infant Health and Development Program (IHDP). (see Ramey, Sparling & Ramey, 2012 for a detailed description of these and other directly relevant projects plus an extensive bibliography with over 350 publications). We will now use the Abecedarian Project’s findings to illustrate our conceptual approach in research practice. We chose to use it because it is our longest running and most comprehensive endeavor to understand human malleability.
Table 2. Major Features of the Abecedarian Approach
| An education program that began in early infancy. |
| A structured curriculum grounded in developmental theory and research findings. |
| A highly trained and actively monitored teaching staff committed to implementing the curriculum and documenting each child’s progress with biweekly summaries. |
| Provision of high quality health and safety practices. |
| Low adult to child ratios (1:3 until babies were walking, 1:4 for toddlers and twos; 1:6 for ages 3 and 4). |
| Ongoing professional development with weekly meetings and frequent monitoring and in-classroom supports for teachers. |
| Individualization of pace in the curriculum and attention to special needs of the child and family. |
| Provision of transportation to children and families as needed. |
| Full-day, year round program (center open from 7:30 am to 5:30 pm, operating 5 days a week, 50 weeks per year). |
| Parent engagement including group meetings and special topic sessions as well as teacher meetings with parents about their own children’s progress. |
| Referral of children to specialists when any problems were detected or suspected based on systematic and frequent assessments. |
| Provision of a well-supplied book and toy lending library for families, including many of the same materials available to children during their center experiences. |
| Stable and stimulating adult-child interactions with a central commitment to ensuring that each child engaged daily in many rich and varied language and learning activities. |
| A planned transition program in the summer before kindergarten that was a preview to what the public kindergarten classrooms were like. |
Discovering the Extent of Early Infant Learning
The research that initially drove the creation of the Abecedarian Project came from our basic laboratory research on infant learning, memory, generalization, and transfer. In that research we were the first to show experimentally in randomized controlled trials that young infants were capable of learning, remembering, and generalizing from experiences that were created to be especially responsive to their emerging behaviors (see Ramey & Ourth, 1971; Watson & Ramey, 1972; Finkelstein and Ramey, 1977; and Ramey & Finkelstein, 1978 for in-depth presentations of that work and emerging insights that were used in the Abecedarian Project). We discovered that quick feedback to an infant that was contingent on the infant’s displayed behavior produced significant changes (increases) in attentional deployment in new contexts and increased Instrumental Effectance. Thus, infants who had more of these response-contingent learning experiences showed more rapid and more generalized learning, which supported increases in their early Directed Cognition in problem-solving situations. The Abecedarian Project sought to determine whether the long-term provision of a conceptually-guided set of increasingly complex response-contingent (responsive) learning experiences could produce significant benefits in learning and language for children from highly impoverished, multi-risk families who, from observational studies, were determined to be less likely to engage in social response-contingent parent/child transactions.
The control group children in the Abecedarian Project were not untreated (as has been typical in other early intervention research). Rather, the control condition children received extra support for health care, nutrition, and family social work services, as well as timely referrals when any developmental problems of clinical concern were detected. Because the control group received these effective multiple supports, the research findings provide a strong basis for concluding that it was the educational features of the Abecedarian Approach that produced the differences between the children in the treatment and control groups rather than some important extra-educational component including health care, nutrition and family support services.
The overall Abecedarian program with specific educational practices and curricula were designed to be highly engaging, fun, active, and responsive with learning occurring throughout the day in various activities including caregiving, play and exploration, as well as more structured adult/child learning and activities. The systematic educational curriculum was based on the types of learning processes described earlier and was paced to be appropriate for a child’s developmental level and to continuously provide opportunities individualized for each child. The Abecedarian Approach strongly acknowledged the centrality of communication to the development of intelligence. Thus, the planned curricular activities included many ways to use signs, symbols, sounds, words, sentences, stories, and interactive conversations starting early in the first year of life. Conversational reading and associated play began in infancy with specially written picture/word books. Adults used varied, complex, and informative language throughout the day as a model for effective communication.
The Commitment to High Quality, Consistently Positive, and Varied Learning Opportunities in the Abecedarian Approach
Program evaluation requires consistent attention to how well the intended intervention is implemented often called fidelity of implementation. Otherwise, one is left with understanding the effects of an unspecified black box not a scientific strong point with respect to issues of causality and replication. In the Abecedarian Approach, the following four broad areas of daily activity were considered operationally important to help young children thrive within our Child Development Center.
- Health and Safety Practices: behaviors that seek to prevent accidents and promote physical and mental health and safety
- Adult-Child Interactions: frequent, warm, and responsive to the individual child.
- Language and Learning Activities: adapted for the child’s age and developmental level.
- Caregiver-Family Relationships: responsive, respectful, supportive, and informative.
Activity in each of these four areas was monitored, recorded, and periodically analyzed and used as substantive information to inform ongoing staff development and continuous program quality assurance.
Recruitment of participants
The Abecedarian Project was a randomized controlled trial (RCT) to test the efficacy of a program of early educational intervention to prevent intellectual disabilities in children born to low-income, undereducated, multirisk families. An RCT refers to a process of randomization to minimize initial bias in the group assignments followed by exerting control over the intervention to ensure it was carried out at sufficient levels to accurately be able to estimate its effects. Local prenatal clinics and the department of social services partnered in screening for eligible participants using the 13-factor High-Risk Index in Table 3. Families who expressed interest (99%) were then visited at home by study personnel to conduct an initial assessment of the family’s eligibility for inclusion in the project. The condition of random assignment to early childhood treatment or control groups was explained in advance to mothers before they granted written consent to enroll in the study. Four successive cohorts of 28 infants each, born between 1972 and 1977, were enrolled and randomized into the study’s treatment groups. Clinical interviews and IQ assessments of family members and scoring of the High-Risk Index completed the intake process. Newborns had to be healthy and judged clinically to be free from biological conditions associated with developmental disabilities.
Table 3. High-Risk Index for Eligibility into the Abecedarian Study
| Factor | Weight |
| Mother’s Educational Level (last grade completed) | 6 8 |
| 7 | 7 |
| 8 | 6 |
| 9 | 3 |
| 10 | 2 |
| 11 | 1 |
| 12 | 0 |
| Father’s Educational Level (last grade completed) | 6 8 |
| 7 | 7 |
| 8 | 6 |
| 9 | 3 |
| 10 | 2 |
| 11 | 1 |
| 12 | 0 |
| Family Income ($ per year) | 1,000 8 |
| 1,001-2,000 | 7 |
| 2,001-3,000 | 6 |
| 3,001-4,000 | 5 |
| 4,001-5,000 | 4 |
| 5,001-6,000 | 0 |
| Father absent for reason other than health or death | 3 |
| Absence of maternal relatives in local area | 3 |
| Siblings of school age one or more grades behind age-appropriate level or with equivalently low scores on school-administered achievement tests | 3 |
| Payments received from welfare agencies within past 3 years | 3 |
| Records of father’s work indicates unstable or unskilled labor | 3 |
| Records of mother’s or father’s IQ indicate score of 90 or below | 3 |
| Records of sibling’s IQ indicates scores of 90 or below | 3 |
| Relevant social agencies in the community indicate the family is in need of assistance | 3 |
| One or more members of the family has sought counseling or professional help in the past 3 years | 1 |
| Special circumstances not included in any of the above that are likely contributors to cultural or social disadvantage | 1 |
Note: Criterion for inclusion in high-risk sample was a score of more than 11 prior to being invited to provide consent and participate.
Table 4. Entry level demographic data for Abecedarian experimental and control families
| Group | Variable | Experimental n = 55 | Control n = 54 | Total N = 109 |
| 1. Mean High Risk Index | 20.08 (5.72) | 21.41 (5.88) | 20.75 (5.81) | |
| 2. Mean maternal age (years) | 19.62 (3.87) | 20.28 (5.77) | 19.94 (4.89) | |
| 3. Mean maternal Education (years) | 10.46 (1.75) | 10.00 (1.89) | 10.23 (1.83) | |
| 4. Mean maternal IQ (WAIS Full Scale) | 85.49 (12.43) | 84.18 (10.78) | 84.84 (11.61) | |
| 5. Percent female-headed family | 78% | 65% | 72% | |
| 6. Percent African American/Black families | 96% | 100% | 98% |
Numbers in parentheses are standard deviations.
The recruited families were predominately African American (98%) although race was not an item in the risk index. The racial composition of the sample is an indicator of historical policies in the Southeastern part of the United States. At birth, 76% of the children lived in single parent or multigenerational households. Mothers ages ranged from 13 to 44 years, with an average age of slightly less than 20 years. Mean maternal education when the study child was born was approximately 10th grade in both groups—the age for legally withdrawing from the educational system. Average maternal IQ as assessed by clinical examination was approximately 85 or one standard deviation below the national average. Stated another way, the typical mother participant scored at about the 15th percentile rank compared to the expected IQ distribution in the general population. Table 4 presents family demographics in more detail.
Program Goal
The primary goal of the prekindergarten phase of the Abecedarian Project was to enhance school readiness by preventing intellectual disabilities and thus establish a stronger cognitive basis for a successful transition into kindergarten in a high performing local education system in a small university town (Chapel Hill, NC). The Abecedarian Project was located in a generally affluent community where the majority of parents were highly educated, employed full-time at well-paying and stable jobs, and the economy was robust (unemployment was consistently under 3%). Relatively few families in the local population would be considered socioeconomically at high risk. Those who did fit this category were disproportionately of African American/Black descent. The city and county political leaders had a generally progressive stance toward disadvantaged families and therefore provided policies and funds for many public and private services for those in need. In 1971-1972, when the project began, there were 33 separate agencies in the town and county devoted to meeting the needs of low-income and multi-risk families. This level of support remained in force throughout the project and was dramatically exemplified by extensive development of new low-cost housing options beginning in the early 1970s. Free or low cost high-quality prekindergarten programs became available for control group participants particularly after they were 2 years of age (see Burchinal, Lee & Ramey, 1989 for evidence of these community child care centers on the performance of control group participants IQ scores, mostly between 3 to 5 years of age). Those collective services are presumed to have improved the performance of the control group children over what would have occurred in a poorer, less resourceful community context. Moreover, the Abecedarian Project provided additional services to both treated and control group participants, including referrals of control children for follow-up treatment in cases where study assessments indicated poor cognitive performance of clinical significance. It is thus reasonable to view the research design as a rigorous test of the power of daily (high dose) systematic, early educational intervention to alter the life course of children from intergenerationally poor multi-risk families. The lifespan approach in the Abecedarian Project looks at trajectories within and across the developmental periods (Birth-Kindergarten; Kindergarten-Grade12; Early and Middle Adulthood). Multiple repeated measures were conducted within each period to characterize the developmental trajectories in age-specific Developmentally Dominant Contexts. We used IQ test along with a variety of other cognitive and academic achievement assessments, school and agency records, interviews, naturalistic observations of home and school behavior and at later ages, self-reports from the children/adults and brain imaging. We focused on major societal benchmarks for primary outcomes within each of the periods.
Lifespan Results of Abecedarian Project
PREKINDERGARTEN INTERVENTION EFFECTS
Three main points are particularly relevant to cognitive development and assessed intelligence during the first 5 years:
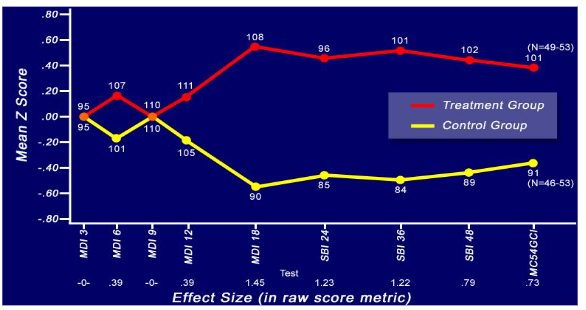
- Intervention reduced the incidence and prevalence of low cognitive development during the preschool years. Developmental delay on standardized tests of intelligence appeared reliably in the control group in the 2nd year of life and persisted throughout the preschool years. Figure 3 shows these scores from 3 to 54 months after amalgamating the IQ or Developmental Quotient (DQ) data of treated and control participants at each age, standardizing the combined distribution and then calculating the mean z scores for the treatment and control groups separately. The graph depicts data from the Bayley Mental Development Index, the Stanford Binet IQ, and the McCarthy Scales of General Cognitive Development at appropriate age points in months. We use these scores as the best available PreK index of overall general knowledge during this age period because there is no other culturally agreed upon real life criteria within this period. The number at each z score is the treatment or control group mean IQ score or equivalent. (M = 100, SD = 15 points) in the standardization samples of these tests. Below each age point on the X axis is the effect size estimates based on standardized scores using the following formula: M treatment group M control group SD of control group. Effect sizes greater than 0.25 are generally considered by educators to have practical significance. Effect sizes of greater than .80 are considered large. Our calculations reveal that no effect size difference existed at the first infant measurement occasion thus supporting the inference of initial group equivalence in cognitive functioning. Over the first 18 months of age, however, the differences became progressively larger and consistently favored the performance of the educationally treated group over the control group. The average effect size estimate of preschool treatment between 18 months and 4½ years was 1.08, a remarkably large and consistent effect size difference in the early education intervention literature. Practical Significance. To learn the extent to which the High-Risk Index successfully identified children at risk for developmental delay during the preschool period, Ramey and Campbell (1984) reported the percentages of children who obtained a Stanford Binet IQ of 85 or less at various occasions during the preschool years. For example, at 48 months, approximately 40% of control group children scored in this range compared to less than 5% of the preschool intervention group. In the general population about 15% of children score this low or lower. This eightfold relative risk reduction is consistent with the hypothesized positive cognitive impact of the Abecedarian Approach.
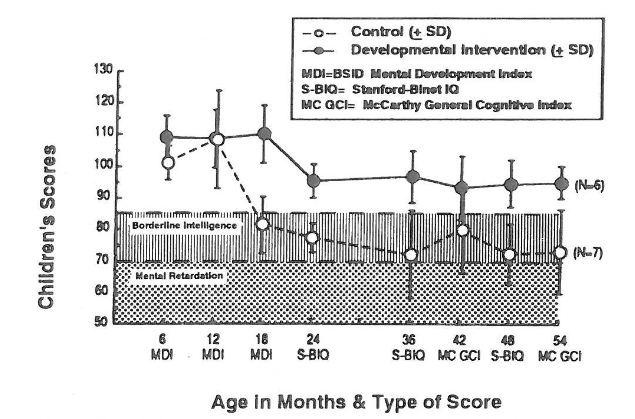
- The most vulnerable children benefitted the most from the Abecedarian Educational Program. We estimated the effects of the prekindergarten treatment on intellectual development through 54 months of age. The average IQs of treatment group children ranged from 8 to over 20 IQ points higher than those of control children when maternal IQ and home environment, both important factors in the occurrence of developmental delay, were statistically accounted for via multiple-regression analyses. Among the subgroups of children who benefitted the most were those whose birth mothers had tested IQs below 70 (clinically considered mentally retarded then, and now classified as intellectually disabled). Figure 4 shows the trajectory of IQ performance for the relatively small number of children in both groups who had mothers with IQ < 70. Beginning at the 18-month assessment, these children in the two treatment groups differed consistently by more than 20 IQ points. Stated another way, the children at greatest risk for intellectual disability benefitted at even higher levels than the overall group. That is, within the educationally-treated group, the early Abecedarian educational intervention helped all children on average but had a notably larger positive effect on the most vulnerable.
- The Abecedarian early education intervention increased children’s cognitive resilience to nonoptimal biological and behavioral initial conditions. The Abecedarian educational intervention significantly ameliorated the effects of relatively mild biological and behavioral risk factors including low neonatal Apgar scores, difficult initial temperament, and fetal undernourishment. These factors took an additional developmental toll in the control group but were eliminated as significant negative factors in the treatment group. As a behavioral consequence mothers interacted with their infants in ways that responded to their child’s presenting behaviors, learned during treatment interacting more when the children had been treated and less when they were in the control group. We discovered that the treatment children were the ones who were initiating engagement with their mothers, bidding for more play time by reaching out to and talking to their mothers more frequently. Mothers in both the treatment and control groups responded well to their children bids for attention and social engagement, but the higher child initiation rates of the early intervention group resulted in them receiving more stimulation and higher response-contingent transactions in total. This finding underscores the reciprocity or bidirectionality of influence of social experiences. The primary mechanism for this increased resilience was by enhancing the social initiative and responsiveness (social competence) of the treated children.
Kindergarten to Grade 12 Results
We have reported that the Abecedarian Approach resulted in consistently superior performance in both assessed IQ throughout the school years as well as better performance in key subject areas including language, reading, and mathematics at 8, 12, 15, and 21 years of age. We also reported significant large reductions in grade retention (30% versus 55%) and special education placement (12 versus 48%). Thus, the Abecedarian Approach strongly supported the study’s leading hypothesis that a high-quality early education program could prepare children for greater success even in a high-performing, high-resource school system, where there was only a small percentage of seriously at-risk children. A trajectory analysis of the K-12 school years and adult outcomes data by Burchinal et al Ramey (2024) discovered that post-intervention contexts may also have had differential effects on males and females, since on some measures females showed better cognitive/IQ test performance in later adulthood. This finding begs for more information on contexts in examining how program effects contribute to very long-term outcome differences. The Abecedarian Project results have exerted some measurable influence on decisions and investments by many local and statewide governments and educational agencies. The reader is referred, for example, to a recent publication by Ramey, Stokes et al Ramey (2025) for a report of a successful application of the Abecedarian Approach beginning at 4 years of age to a statewide program. In the statewide Louisiana program, only a one year program, the pre-K children outperformed comparison group children with better statewide test scores at third grade in all subject areas assessed including language, math, science, and social studies. Treated children consistently performed better than the statewide average in each of the 4 areas assessed. Treated children also had significant reductions in grade retention and special education placement.
Adult Functional Intelligence among the Abecedarian participants
The follow-up of former Abecedarian participants afforded the opportunity to examine prospectively documented life histories and environmental contexts with respect to performance within adulthood. We have conducted adult follow-up studies at ages 21, 30, 35, 40, and 45 years of age. At most ages, we obtained some measures of academically-oriented cognitive performance and attainment of higher education/earned degrees, but we also wanted to take a broader view about quality of life issues consistent with our concept of Functional Intelligence. We chose to focus on: 1) formal educational attainment 2) employment and economic self-sufficiency, 3) social decision-making, 4) family cohesiveness, 5) civic and social engagement, and 6) adult brain structure and functioning. These findings and those about health are reviewed in more detail in a recent article by C. Ramey and Ramey (2023).
In summary, a composite measure of midlife strengths and assets was significantly higher for those in the early education compared to control group. Adult findings include higher levels of positive relationships to parents (both mother/mother figures and fathers/father figures), longer planning horizons and more social equitable or fair decision-making demonstrated in standardized game-playing economic protocols, better overall health and cardiovascular and weight biomarkers, brain structural differences suggestive of positive association with the early education objectives, and more productive mainstream lifestyles as indicated by adult residential zip codes showing residence in greater income and better educated neighborhoods with less crime and welfare dependence and higher rates of voting in recent national elections. We interpret these findings within our Biosocial Contextual Framework as demonstrating how there is a linked chain or flow from positive early experiences and outcomes to greater success in new and varied age-appropriate settings, throughout childhood and into adulthood years of further education and training, work, and family life and maintaining positive lifestyles. These findings indicate that the Abecedarian Education participants used their Functional Intelligence well to benefit from schooling and meet to the multiple and often complex realities of adult life and community participation. We further note that many of the control group study participants are leading healthy and productive lives, and during a series of interviews with all study participants, both the controls and early education participants spontaneously mentioned how much their parents and they valued their participation in this 50-year longitudinal study.
Looking to the Future
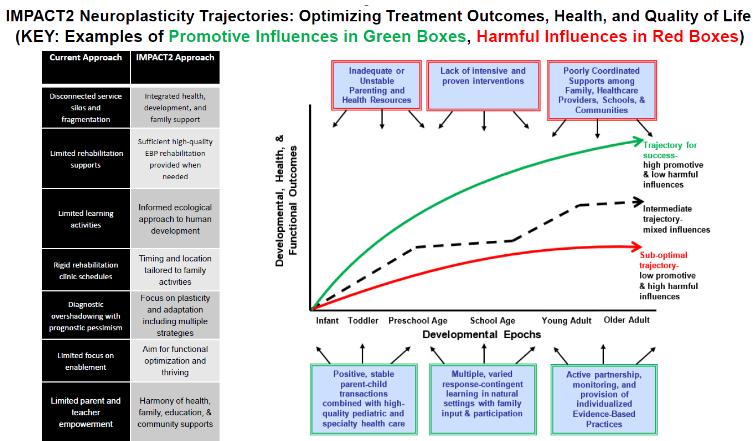
We summarize our lifespan research perspective on the prevention and treatment of disabilities in Figure 5. On the left side of the figure, we compare the current (conventional) approach to a new dynamic approach that we and our colleague, Michael Msall, have named IMPACT. Applying the recommended changes in approach that are noted in Figure 5, we propose to track neuroplasticity trajectories of individuals while documenting both restraining forces (noted in red) and promotive forces (noted in green). We also identify contextual areas for regular monitoring and analysis. Within this agenda for research and program development, we advocate conducting vigorous testing of novel and combination forms of therapy and natural supports through interdisciplinary teams that include people with lived experiences. This incorporation of lived experiences may be used to improve program attractiveness and effectiveness. Ineffective conventional practices need to be replaced with a new focus on continuously improving the developmental trajectories of individuals at risk for disabilities whatever their ages. We must figure out how to provide opportunities for effective treatment to those who need it while we simultaneously look at differential response-to-treatment analyses to maximize effectiveness and efficiency in program operation. Routine trajectory analyses and public reports about related factors could help in getting to responsible and effective public policies.
Conclusion We are optimistic that our trajectory-oriented biosocial and ecological systems approach with its emphasis on learning processes, social transactions, and important life periods and contexts has major implications across the lifespan with respect to minimizing negative effects of risk conditions and the occurrence of disabilities. The identification of the mechanisms undergirding individual stability and change would be ideal for both conceptual advancement and therapeutic guidance. From our perspective, human development, developmental science, and public policy are inextricably intertwined. Each can serve as the context for the others, with many dynamic and potentially reciprocal influences. Systematic research is one of the powerful mechanisms for generating new and stronger knowledge about how to improve quality of life for individuals affected by non-optimal biological, economic, environmental, and family challenges. But we also have witnessed how socially inspired movements to improved conditions of children born into extremely impoverished life circumstances can benefit more than just the at risk children; greater community stability, establishing trustworthy and positive family supports, improving the quality and accessibility of health and many other community services are examples that benefit everyone. Finally, to our knowledge, the joy and the affirmation associated with taking altruistic actions that improve the lives of all young children and all families in a community or a larger entity (e.g., region, nation) are dimensions rarely considered in scientific basic research on human development. We consider them worthy of greater attention.
Acknowledgements:
We gratefully acknowledge the long-term supports from the U.S. National Institutes of Health, especially the Eunice Kennedy Shriver National Institute of Child Health and Human Development; the U.S. Department of Education; the Administration for Children, Youth and Families; and the Maternal and Child Health Bureau of the Public Health Service. Additional substantial financial and practical support has been provided by the Robert Wood Johnson Foundation, the Rockwell Foundation, the Fralin Biomedical Research Institute, the Civitan International Research Center, and the state of North Carolina. We extend deep gratitude to the families and children who have participated in the Abecedarian Project. We are deeply grateful to Laura Bateman for her help in preparing this manuscript.
References:
- Ramey CT, Ramey SL. Early intervention and early experience. Am Psychol. 1998;53(2):109-120. doi:10.1037//0003-066x.53.2.109.
- Ramey CT, Ramey SL. Early childhood education that promotes lifelong learning, health, and social well-being: The Abecedarian Project and its replications. Med Res Arch. 2023;11(11):1-17. doi:10.18103/mra.v11i11.4590.
- Ramey CT, Sparling J, Ramey SL. Abecedarian: The Ideas, the Approach, and the Findings. Los Altos, CA: Sociometrics Corporation; 2012.
- Ramey CT, Blair C. Intellectual development and the role of early experience. In: Detterman DK, ed. Current Topics in Human Intelligence Norwood, NJ: Ablex Publishing; 1996:59-67.
- Galton F. Inquiries into Human Faculty and its Development. Macmillan; 1883.
- Jenson AR. How much can we boost IQ and scholastic achievement? Harvard Educ Rev. 1969; 39:1-123.
- Herrnstein RJ, Murray CA. The Bell Curve: Intelligence and Class Structure in American Life. Free Press; 1994.
- Hunt JM. Intelligence and Experience. Ronald; 1961.
- Bijou S, Baer D. Child Development: A Systematic and Empirical Theory. New York: Appleton-Century-Crofts; 1961.
- Ceci, SJ. On Intelligence: A Biological Treatise on Intellectual Development, 2nd Edition. Cambridge, MA: Harvard University Press; 1996.
- Blair C, Raver CC. Individual development and evolution: Experiential canalization of self-regulation. Dev Psychol. 2012;48(3):647-657. doi:10.1037/a0026472.
- Lazar I, Darlington RB. Lasting effects of early education: A report from the Consortium for Longitudinal Studies. Monographs of the Society for Research in Child Dev. 1982;47(2-3):1-151. doi:10.2307/1165938.
- Ramey CT, Ourth LL. Delayed reinforcement and vocalization rates of infants. Child Dev. 1971; 42(1):291-297.
- Watson JS, Ramey CT. Reactions to response-contingent stimulation in early infancy. Merrill-Palmer Quarterly. 1972;18(3):219-227.
- Finkelstein NW, Ramey CT. Learning to control the environment in infancy. Child Dev. 1977;48:806-819. doi:10.2307/1128329.
- Ramey CT, Finkelstein NW. Contingent Stimulation and Infant Competence. J Pediatr Psychol. 1978; 3(2):89-96. doi:10.1093/jpepsy/3.2.89.
- Burchinal M, Lee M, Ramey C. Type of day-care and preschool intellectual development in disadvantaged children. Child Dev. 1989;60(1):128-137. doi:10.1111/j.1467-8624.1989.tb02702.x.
- Ramey CT, Campbell FA, Burchinal M, Skinner ML, Gardner DM, Ramey SL. Persistent effects of early childhood education on high-risk children and their mothers. Appl Dev Sci. 2000;4(1):2-14. doi:10.1207/S1532480XADS0401_1.
- Ramey CT, Campbell FA. Preventive education for high-risk children: Cognitive consequences of the Carolina Abecedarian Project. Am J Ment Defic. 1984;88(5):515-523.
- Martin SL, Ramey CT, Ramey S. The prevention of intellectual impairment in children of impoverished families: Findings of a randomized trial of educational day care. Am J Public Health. 1990;80(7):844-847. doi:10.2105/ajph.80.7.844.
- Ramey CT. A rejoinder to Spitz’s critique of the Abecedarian experiment. Intelligence. 1993;17:25-30.
- Breitmayer BJ, Ramey CT. Biological nonoptimality and quality of postnatal environment as codeterminants of intellectual development. Child Dev. 1986;57(5):1151-1165. doi:10.1111/j.1467-8624.1986.tb00444.x.
- Ramey CT, Sparling JJ, Bryant D, Wasik B. Primary prevention of developmental retardation during infancy. J Prev Human Services. 1982;1:61-83.
- Zeskind PS, Ramey CT. Fetal malnutrition: An experimental study of its consequences on infant development in two caregiving environments. Child Dev. 1978;49(4):1155-1162.
- Zeskind PS, Ramey CT. Preventing intellectual and interactional sequelae of fetal malnutrition: A longitudinal, transactional, and synergistic approach to development. Child Dev. 1981;52(1):213-218.
- Burchinal MR, Campbell FA, Bryant DM, Wasik BH, Ramey CT. Early intervention and mediating processes in cognitive performance of children of low-income African American families. Child Dev. 1997; 68(5):935-954. doi:10.1111/j.1467-8624.1997.tb01972.x.
- Burchinal M, Foster T, Garber K, et al…Ramey. Sex differences in early childhood education intervention impacts on cognitive outcomes. J Appl Dev Psychol. 2024;95:101712. doi:https://doi.org/10.1016/j.appdev.2024.101712.
- Ramey CT, Stokes BR, Asmus GJ, Hankey MS, Ramey SL. Large-scale, well-implemented public pre-kindergarten linked to better academic performance and school health. Med Res Arch. 2025;13(5). doi:10.18103/mra.v13i5.6534.
- Luo Y, Hétu S, Lohrenz T, et al…Ramey. Early childhood investment impacts social decision-making four decades later. Nature Communications. 2018; 9(1):4705. doi:10.1038/s41467-018-07138-5.
- Campbell F, Conti G, Heckman JJ, et al. Early childhood investments substantially boost adult health. Science. 2014;343(6178):1478-1485. doi:10.1126/science.1248429.
- Farah MJ, Sternberg S, Nichols TA, et al…Ramey. Randomized manipulation of early cognitive experience impacts adult brain structure. J Cog Neurosci. 2021;33(6):1197-1209. doi:10.1162/jocn_a_01709.
- Ramey SL, Msall ME, Ramey CT. Paradoxes in pediatric rehabilitation: Building an interdisciplinary, total-child framework to promote effective interventions and life course well-being. Front Pediatr. 2025;13. doi:10.3389/fped.2025.1540479.