

Acute Splenial Hemianopsia: Case Report and Insights
Acute Splenial Hemianopsia: A rare Case Report
Sofia Faria Camões 1, Nídia Pinheiro Oliveira 1, Beatriz Dias Silva 1, Hugo Sarabando Ventura 1, Ilídia Pereira Carmezim 1, Rui Santos André 2, Catarina Ramos Oliveira 1, Ana Isabel Gomes 1, Edite Marques Nascimento 1
- Internal Medicine, Unidade de Saúde Local Viseu Dão Lafões
- Neurology, Unidade de Saúde Local Viseu Dão Lafões
OPEN ACCESS
PUBLISHED 31 August 2025
CITATION Camões, SF., Oliveira, NP., et al., 2025. Acute Splenial Hemianopsia: A rare Case Report. Medical Research Archives, [online] 13(8). https://doi.org/10.18103/mra.v13i8.6884
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i8.6884
ISSN 2375-1924
ABSTRACT
We present the case of a 76-year-old woman admitted with acute-onset right parietal headache, left-sided visual field impairment, and gait imbalance, in the context of a hypertensive peak. Neurological examination revealed a left homonymous hemianopia. Cranial CT identified a recent ischemic lesion in the right splenium of the corpus callosum and right occipital cortex. MRI confirmed a subacute infarct in the right posterior cerebral artery (PCA) territory, with occlusion of the distal P2 segment. The patient remained hemodynamically and neurologically stable during a four-day hospitalization, with spontaneous improvement in visual symptoms and full return to baseline functional status (mRS 0). No arrhythmias were detected on 24-hour Holter monitoring. She was discharged on secondary prevention therapy with aspirin, atorvastatin, and ramipril. A repeat MRI performed 18 months later confirmed the chronic evolution of the infarct. This case highlights the variable clinical presentation of PCA strokes and the importance of comprehensive diagnostic work-up, even in patients with full clinical recovery.
Keywords:
- Posterior cerebral artery stroke
- splenium infarct
- homonymous hemianopia
- secondary prevention
- neuroimaging follow-up
Introduction
Cerebrovascular disease remains one of the most commonly diagnosed pathologies, particularly among the large number of patients seen daily. Fortunately, nowadays, with the improvement of neuroimaging, diagnosis is faster and patients are treated quickly, improving their prognosis. The corpus callosum (CC) is the primary commissural connection between the two neocortices of the cerebral hemispheres. Studies have shown that the CC plays a role in ocular movement and actively participates in this process. Information gathered by the eye muscles and retina is transmitted to the cerebral hemispheres, where stimuli are subsequently processed. Furthermore, this structure also contributes to the interpretation of sensory information, such as vision and touch. Infarction of the CC is relatively rare due to the rich blood supply from both the anterior and posterior circulations, accounting between 3-8% of all cerebral infarcts. The clinical manifestations of CC infarction are often non-specific, leading to frequent underrecognition or misdiagnosis. Anatomically, it is divided into rostrum, genu, body and splenium, with splenial infarction being the most common subtype, comprising 46-55% of CC infarcts.
The following report presents a rare case of splenial hemianopsia as the only clinical manifestation of a corpus callosum infarct.
Case presentation
A 76-year-old woman, with a baseline mRS (modified Rankin Scale) score of 0, presented to the Emergency Department with right parietal headache and associated paresthesias since the previous day. She subsequently reported difficulty seeing the bedroom door, describing “grayish vision” (sic) on the left side. At this time, she also reported gait imbalance. Also, she had taken ibuprofen (Brufen) with partial symptom relief. There was no associated nausea or vomiting and no history of similar episodes. Her medical history included a previous thrombosis in the right eye, and bilateral cataract surgery.
On physical examination, she was hypertensive (blood pressure: 202/81 mmHg). A left homonymous hemianopsia was observed, but no motor or sensory deficits were noted. Her gait was cautious, although no signs of ataxia were noted. In the Emergency department, was preformed non-contrast cranial CT scan followed by CT angiography (Figure 1) demonstrated a hypodense area in the right lateral aspect of the splenium of the corpus callosum, suggestive of mild expansion and compatible with recent ischemia.
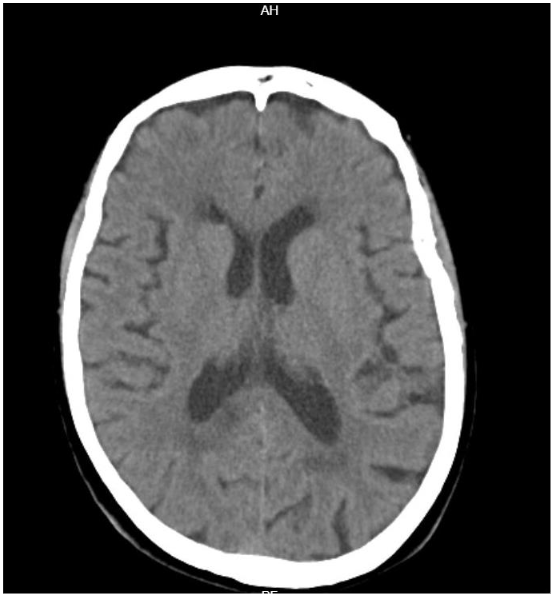
A probable 7 mm calcified meningioma with no mass effect was also identified. Blood tests were unremarkable, and electrocardiography showed no evidence of ischemia or arrhythmia.
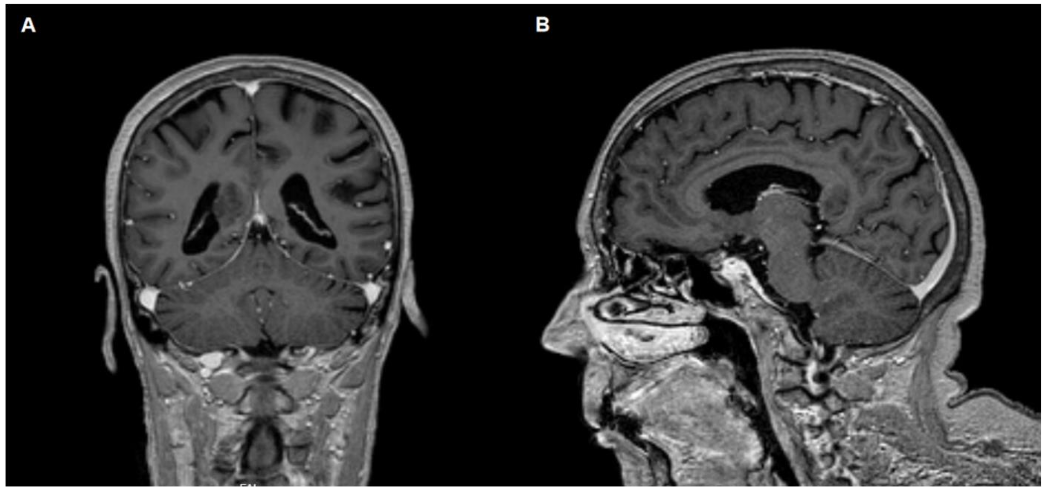
The patient was hospitalized for four days to the stroke unit, to continue the investigation of the ischemic cerebrovascular event in the vertebrobasilar circulation. Carotid and vertebral Doppler ultrasound showed bilateral atheromatous changes without hemodynamic significance and normal flow in vertebral arteries. A brain MRI (Figure 2A and B), including arterial MR angiography performed using the 3D-TOF technique, revealed a cortico-subcortical lesion in the right temporo-occipital region and in the splenium of the corpus callosum, with restricted diffusion of water molecules, consistent with a recent ischemic lesion in the territory of the right posterior cerebral artery. Angiography confirmed occlusion of distal right posterior cerebral artery (PCA) (P2 segment), likely by intraluminal thrombus.
During hospitalization, the patient remained hemodynamically stable, and there were no complications. At discharge, she had no visual complaints, although a persistent superior quadrant left visual field defect (quadrantanopia) was reported. No other neurological deficits were present. Her mRS score at discharge was 1.
As secondary prevention, the patient was prescribed with acetylsalicylic acid (Aspirin), 100mg (antiplatelet therapy), Atorvastatin, 20mg (lipid-lowering agent) and Ramipril, 10mg (antihypertensive, ACE inhibitor). A follow-up consultation was scheduled one month after discharge to monitor clinical evolution, reassess neurological status, review imaging and test results, and adjust secondary prevention strategies as needed. A 24-hour Holter monitor showed sinus rhythm with an average heart rate of 62 bpm, rare isolated polymorphic ventricular extrasystoles, and occasional supraventricular extrasystoles, with no arrhythmias detected. Follow-up blood tests revealed: LDL 70 mg/dL, HDL 42 mg/dL, total cholesterol 144 mg/dL and HbA1c glycated hemoglobin 5.4%. Thyroid function tests indicated suppressed TSH level with normal T3 and T4 values, compatible with subclinical hyperthyroidism.
The patient did not undergo rehabilitation, but experienced spontaneous improvement in her visual symptoms, returning to her previous functional status. Her mRS score was 0.
Regarding the meningioma, she was evaluated by Neurosurgery which recommended imaging follow-up. In this context, one and a half years after the ischemic event, she underwent a follow-up brain MRI. Compared with the previous exam, the right frontal meningioma remained stable, and the ischemic lesion in the right PCA territory showed evidence of chronicity. No new findings were observed.
Discussion
This case report highlights the pleomorphic clinical spectrum of posterior cerebral artery infarctions, which often present atypically and are under-recognized compared to anterior circulation strokes. The patient exhibited left homonymous hemianopia and subtle visual changes as the only focal deficits, consistent with infarcts affecting the occipital cortex and splenium of the corpus callosum.
PCA infarcts account for up to 10% of all ischemic strokes and are frequently associated with deficits such as hemianopsia, alexia without agraphia, memory disturbances, and visual agnosia depending on lesion localization. Lesions of the splenium, in particular, are associated with disconnection syndromes and may result in transient visual field deficits or higher-order processing impairment.
Our patient’s favorable recovery, marked by resolution of hemianopsia and return to baseline function, is consistent with reports of excellent outcomes in patients with isolated cortical infarcts in the PCA territory. The absence of significant motor, sensory, or speech deficits and the subtlety of symptoms emphasize the importance of clinical suspicion and detailed examination, particularly when patients report nonspecific complaints like visual grayness, imbalance, or headache. Given that the National Institutes of Health Stroke Scale (NIHSS) may underrepresent posterior circulation strokes, broader screening tools such as BE-FAST can provide enhanced diagnostic sensitivity in these cases.
Advanced imaging, including MRI and MR angiography, was essential in confirming the infarct in the right PCA territory and identifying the occlusion in the distal P2 segment. Importantly, the MRI also revealed an incidental, partially calcified right frontal meningioma, which required further neurosurgical evaluation. Given its small size and absence of mass effect, conservative management with imaging follow-up was appropriately advised, consistent with current guidelines on the management of asymptomatic meningiomas.
The etiologic investigation included 24-hour Holter monitoring and carotid/vertebral Doppler ultrasound. No arrhythmias were identified, and carotid Doppler revealed bilateral atheromatous changes without hemodynamic compromise. In the absence of cardioembolic sources or large-vessel occlusion, the stroke was classified as cryptogenic under TOAST criteria, a common finding in PCA infarctions.
Secondary prevention was initiated with aspirin, atorvastatin, and ramipril. Follow-up MR imaging confirmed the chronicity of the infarct and stability of the meningioma. Functional recovery remained complete (mRS 0), with no need for rehabilitation, underscoring the potential for full neurological restitution even in elderly patients.
This case exemplifies the diagnostic complexity and favorable prognosis of PCA strokes when recognized and managed appropriately. It also illustrates the need for a comprehensive stroke work-up to identify rare causes and incidental findings, as well as individualized care plans balancing stroke recurrence prevention and incidental pathology monitoring.
Conclusion
Splenial infarction is very uncommon and often presents with a wide range of non-specific symptoms, which can delay diagnosis. Our case highlights a rare and atypical presentation of splenial infarction manifesting solely as left-sided homonymous hemianopsia.
Conflicts of Interest Statement
The authors have no conflicts of interest to declare.
References
- Feigin VL, Brainin M, Norrving B, Martins SO, Pandian J. et al. World Stroke Organization: Global Stroke Fact Sheet 2025. Int J Stroke. 2025;20(2):132-144. doi:10.1177/17474930241308142
- Tzourio-Mazoyer N. Intra- and inter-hemispheric connectivity supporting hemispheric specialization. In: Kennedy H, Van Essen DC, Christen Y, eds. Micro-, Meso- and Macro-Connectomics of the Brain. Cham (CH): Springer. 2016 (2016):129-146. doi: 10.1007/978-3-319-27777-6_9
- Berlucchi G, Aglioti S, Marzi CA, Tassinari G. Corpus callosum and simple visuomotor integration. Neuropsychologia. 1995;33(8):923-936. doi:10.1016/0028-3932(95)00031-w
- Sanchez-Lopez J, Cardobi N, Parisi G, Savazzi S, Marzi CA. Role of corpus callosum in unconscious vision. Neuropsychologia. 2024;196(108839):1-11. doi:10.1016/j.neuropsychologia.2024.108839
- Pietrasanta M, Restani L, Caleo M. The corpus callosum and the visual cortex: plasticity is a game for two. Neural Plast. 2012;2012(838672):1-10. doi:10.1155/2012/838672
- Yang LL, Huang YN, Cui ZT. Clinical features of acute corpus callosum infarction patients. Int J Clin Exp Pathol. 2014;7(8):5160.
- Zhang Z, Meng X, Liu W, Liu Z. Clinical features, etiology, and 6-month prognosis of isolated corpus callosum infarction. Biomed Res Int. 2019;2019(9458039):1-9. doi:10.1155/2019/9458039
- Li S, Sun X, Bai YM, Qin H, Wu X. et al. Infarction of the corpus callosum: a retrospective clinical investigation. PLoS One. 2015;10(3):e0120409. doi:10.1371/journal.pone.0120409
- Salih N, Aljaberi K, Palat AN, Chirkkara SKP. Acute isolated corpus callosum infarction: a case report. Cureus. 2024;16(12):1-6. doi:10.7759/cureus.75984
- Chrysikopoulos H, Andreou J, Roussakis A, Pappas J. Infarction of the corpus callosum: computed tomography and magnetic resonance imaging. Eur J Radiol. 1997;25(1):2-8. doi:10.1016/s0720-048x(96)01155-2
- Blaauw J, Meiners LC. The splenium of the corpus callosum: embryology, anatomy, function and imaging with pathophysiological hypothesis. Neuroradiology. 2020;62(5):563-585. doi:10.1007/s00234-019-02357-z
- Arboix A, Arbe G, García-Eroles L, Oliveres M, Parra O, et al. Infarctions in the vascular territory of the posterior cerebral artery: clinical features in 232 patients. BMC Res Notes. 2011;4(329):1-7. Published 2011 Sep 7. doi:10.1186/1756-0500-4-329
- Kim JS. Delineation of posterior cerebral artery territory using MRI. Neurology. 1996;47(4):957–962.
- Cereda C, Carrera E. Posterior cerebral artery territory infarctions. Front Neurol Neurosci. 2012;30(1):128–131 doi: 10.1159/000333610
- Katsuki M, Kato H, Niizuma H, Nakagawa Y, Tsunoda M. Homonymous hemianopsia due to the infarction in the splenium of the corpus callosum. Cureus. 2021;13(11):e19574. doi:10.7759/cureus.19574
- Bogousslavsky J, Regli F. Posterior cerebral artery territory infarcts in the Lausanne Stroke Registry: clinical features, infarct topography, causes, and outcome. Arch Neurol. 1996;53(6):612–620.
- Carrera E, Michel P, Bogousslavsky J. Posterior circulation infarcts: risk factors, outcome, and evolution of infratentorial lesions. Stroke. 2007;38(3):824–830.
- Park KC, Yoon SS, Seo KH. Lesions in occipital lobe extending to splenium/parahippocampus and executive dysfunction after PCA infarction. J Clin Neurosci. 2009;16(7):914–917.
- Alemseged F, Rocco A, Arba F, Schwabova JP, Wu T. Posterior National Institutes of Health Stroke Scale improves prognostic accuracy in posterior circulation stroke. Stroke. 2022;53(4):1247–1255. doi:10.1161/STROKEAHA.120.034019
- Chen X, Zhao X, Xu F, Guo M, Yang Y. A systematic review and meta-analysis comparing FAST and BEFAST in acute stroke patients. Front Neurol. 2022;12(765069):1-15. doi:10.3389/fneur.2021.765069
- Kızılgöz V, Kantarci M, Kahraman Ş. Imaging findings of two patients with isolated infarction of the splenium during COVID-19. SAGE Open Med Case Rep. 2022;10(2050313X221135232):1-6 doi: 10.1177/2050313X221135232. eCollection 2022