






Advances in Lupus Nephritis Screening and Treatment
Lupus Nephritis: Current Advances and Future Options for Screening and Treatment
Reena Yaman¹, Krish Relan², Mandar Shah³, Archit Srivastava¹, Sehreen Mumtaz¹, Vikas Majithia¹
- Department of Rheumatology, Mayo Clinic Florida, Jacksonville, FL, 32224, USA
- Department of Neuroscience, University of Miami, Coral Gables, FL, 33146, USA
- Department of Internal Medicine, Albert Einstein College of Medicine, NY, 10461, USA
OPEN ACCESS
PUBLISHED: 31 January 2025
CITATION: Yaman, R., Relan, K., et al., 2025. Lupus Nephritis: Current Advances and Future Options for Screening and Treatment. Medical Research Archives, [online] 13(1).
https://doi.org/10.18103/mra.v13i1.6217
COPYRIGHT: © 2025 European Society of Medicine. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i1.6217
ISSN 2375-1924
ABSTRACT
Background: Lupus nephritis is one of the most common severe organ manifestations of systemic lupus erythematosus (SLE). Despite the continuing advancement in therapy, up to 30% of patients progress to end-stage renal disease. The clinical manifestations of lupus nephritis are variable and screening all SLE patients for lupus nephritis is imperative. There has been substantial advancement in availability of biomarkers and therapeutic options. This review focuses on epidemiology, early screening, advances in the biomarkers and management of lupus nephritis.
Content: Lupus nephritis is a devastating consequence of SLE and disproportionately affects the minorities. Inter-ethnic variation in the prevalence and severity of lupus nephritis as well as tolerance and clinical response to various therapeutic regimens for LN has led to variation in screening and treatment of lupus nephritis in SLE patients. Periodic screening of lupus nephritis in patients with SLE is imperative for early detection. Urinalysis and urine protein-to-creatinine ratio are useful screening tests. Quantification can be performed by 24-h urine sample collection for protein. Renal biopsy remains the gold standard for diagnosis of lupus nephritis. Traditional serum biomarkers used to monitor lupus nephritis disease activity and flares include anti-double-stranded DNA antibodies and complement components 3 and 4. New biomarkers for lupus nephritis include anti-C1q and type 1 interferon regulatory genes, urinary monocyte chemoattractant protein 1, neutrophil gelatinase-associated lipocalin, tumor necrosis factor-like inducer of apoptosis, and vascular cell adhesion molecule 1. Therapeutic options that better lead to remission of lupus nephritis, preserve kidney function and reduce the toxicities of concomitant glucocorticoids are unmet needs in lupus nephritis. There are newly approved treatments as well as investigational drugs in the pipeline, including the newer generation calcineurin inhibitors, biologic agents and cellular therapeutic options. The choice of therapy depends on a number of clinical considerations and should be tailored to individual patient circumstances. Molecular profiling, gene-signature fingerprints and urine proteomic panels might enhance the accuracy of patient stratification for treatment personalization in the future.
Summary: Promising advances have been made in screening and treatment of lupus nephritis. The use of traditional and alternative biomarkers has the potential to identify at risk patients and those having active flare-up but require validation in prospective studies. Renal remission rates in patients receiving standard of care therapy for induction and maintenance treatments have improved but remain low. Further research in newer therapeutic targets for lupus nephritis shows promising results.
Key points
- The development of biomarkers for early detection and novel therapeutics to improve the efficacy-to-toxicity balance for LN are current unmet needs.
- New serum and urinary biomarkers for LN can help screen and stratify the patients at risk and those having flare-up of LN.
- Biologic, belimumab and calcineurin inhibitor, voclosporin are recently approved drugs for the treatment of LN offering potential to provide early and sustained remission in LN.
- Options to better stratify patients and provide personalized treatment for patients with LN such as molecular profiling and urine proteomic panels are on the horizon.
- New-generation anti-CD20 biologic agents, type I interferon antagonists, combination of biologics and cellular therapies such as autologous anti-CD19 CAR-T cell show promise for the treatment of LN.
Introduction
The incidence and prevalence of lupus nephritis (LN) has been increasing over time with no significant improvement in mortality gap. Screening of all systemic lupus erythematosus (SLE) patients for LN is of the essence and ultimately “time is nephrons”-earlier diagnosis correlating with improved prognosis. There has been considerable advancement in the availability of biomarkers and therapeutic options over the past 5 years. Although there has been a pivotal shift in the management approach of LN, clinician education to improve utilization of novel therapeutics must be enhanced. This narrative review encompasses epidemiology, early screening, advances in biomarkers and management of LN.
Background/Classification
Systemic lupus erythematosus (SLE) is a complex autoimmune disease that affects multiple organ systems and impacts approximately 3.4 million individuals worldwide, out of which 90% are women. The kidney is the organ most frequently affected by this disease, significantly contributing to both morbidity and mortality. A significant proportion of patients with SLE develop lupus nephritis within the first five years after diagnosis, which has substantial implications for survival and quality of life. LN is a leading cause of death in SLE and places a significant socio-economic burden on society, primarily affecting those under the age of 50. The lifetime incidence of lupus nephritis ranges from 20% to 60%, with higher prevalence observed among African Americans and Hispanics compared to Caucasians. Although lupus occurs more frequently in women, LN has higher rates noted in men than in women. The survival rate for patients significantly decreases with the onset of lupus nephritis, making it a critical focus area in managing SLE.
Lupus nephritis is traditionally defined as a disease caused by immune complexes in patients with systemic lupus erythematosus (SLE). It presents a range of clinical symptoms, from asymptomatic proteinuria to nephrotic syndrome, and can potentially progress to end-stage renal disease (ESRD). This variability in the presentation underscores the complexity of LN and highlights the critical need for tailored management plans. Given the significant effects on kidney function, it is essential to prioritize intervention for both early stages and progressive forms of the disease to optimize patient outcomes.
The American College of Rheumatology and the 2012 Systemic Lupus International Collaborating Clinics (SLICC) criteria for diagnosing lupus nephritis emphasize the importance of urinary markers. These include proteinuria more significant than 0.5 grams per 24 hours or the presence of red blood cell casts. Urinalysis is a crucial screening tool for LN as all patients with clinical renal disease exhibit proteinuria, with about half of these cases showing nephrotic-range proteinuria. Abnormal results from urinalysis can be further evaluated by measuring proteinuria using a urine protein-to-creatinine ratio (PCR) or a 24-hour urine protein collection (24H-P). Although studies indicate that there are limitations to the accuracy of urinalysis and PCR in diagnosing and assessing the severity of LN, these methods continue to serve as valuable preliminary screening tools and can help reduce the number of unnecessary biopsies.
Clinical signs alone often do not fully capture the extent of kidney involvement in patients with SLE. Additionally, non-immune complex renal conditions can occur in these patients, some of which are directly related to lupus, such as lupus podocytopathy and thrombotic microangiopathy induced by lupus anticoagulant. Therefore, a renal biopsy remains essential for confirming diagnosis, assessing disease activity, and evaluating chronicity.
Over the past 40 years, the classification of lupus nephritis has evolved, beginning with the World Health Organization (WHO) system in 1974 and most recently updated in 2018. The classification now follows the International Society of Nephrology/Renal Pathology Society (ISN/RPS) system, which categorizes the disease into six classes (Class I-VI) and includes terms defining activity such as “acute,” “chronic,” and “acute on chronic.” This classification framework provides valuable insights for personalized treatment and prognosis, focusing on managing active, potentially reversible lesions while distinguishing them from chronic, often irreversible damage. Classes I and II are typically mild or asymptomatic, while Classes III and IV present with more severe renal manifestations and significant proteinuria. Class V has the highest incidence of nephrotic syndrome, and Class VI often leads to end-stage renal disease (ESRD) due to irreversible damage. A key strength of the current classification is its widespread acceptance, as it is incorporated into treatment guidelines for SLE by both the American College of Rheumatology and the European League Against Rheumatism.
Autoantibodies are a key feature of systemic lupus erythematosus (SLE), and traditional diagnostic and monitoring strategies for SLE and lupus nephritis (LN) often rely on markers such as anti-dsDNA and complement levels (C3, C4). However, these markers have limitations; for example, elevated anti-dsDNA titers do not consistently indicate the presence of nephritis, and fluctuations in complement levels are not always dependable predictors of disease flares or responses to treatment. Recent advances in our understanding of the pathophysiology of LN have led to the discovery of promising new biomarkers related to cellular and inflammatory pathways. These include anti-C1q antibodies, interferon regulatory genes, C-X-C motif chemokine ligand 10 (CXCL10), interleukin-18 (IL-18), and galectin-9. Additionally, urinary biomarkers have shown potential, with initial findings suggesting the usefulness of markers like monocyte chemoattractant protein 1 (MCP-1), TWEAK, B-cell activating factor (BAFF), vascular cell adhesion molecule 1 (VCAM-1), and matrix metalloproteinase 7 (MMP-7) in enhancing the diagnosis and monitoring of LN. Introducing these biomarkers paves the way for a more effective and nuanced approach to managing lupus nephritis.
In managing lupus nephritis (LN), the primary treatment goals are to preserve kidney function, decrease the risk of progression to end-stage renal disease, and minimize the side effects associated with medications. It is recommended that all patients with Systemic Lupus Erythematosus (SLE) and nephritis receive hydroxychloroquine (HCQ) treatment, unless contraindicated. The treatment approach for LN consists of an induction phase followed by maintenance therapy. Common agents used for induction include cyclophosphamide and mycophenolate mofetil, often in combination with high-dose corticosteroids. Recent studies have shown promising outcomes with alternative therapies, such as CD20-targeted monoclonal antibodies and recombinant human IgG-1λ monoclonal antibodies that target soluble B lymphocyte stimulators, which may provide additional management options. For maintenance therapy, mycophenolate mofetil or azathioprine is typically employed to prevent renal flares. However, the optimal duration of maintenance therapy and the effectiveness of combination treatments remain uncertain. Other innovative therapies, including the sequential use of two B-cell-targeting agents and a type I interferon receptor antibody, have also demonstrated encouraging results.
Lupus nephritis (LN) poses a significant risk of mortality in patients with systemic lupus erythematosus (SLE), driving intense research into innovative therapies and biomarkers to improve patient management. Achieving and maintaining remission in LN patients remains a significant challenge, with consistently high rates of flare-ups and low remission rates, even with optimized treatment. While several studies have shown promising results regarding potential therapies and biomarkers, validating these findings in prospective studies that include diverse patient populations before they can be integrated into standard clinical practice is essential. Our review captures the latest progress in the field, providing a clearer understanding of promising approaches to enhance disease management and improve patient outcomes.
Epidemiology/Scope of Issue/Current Literature
Systemic lupus erythematosus (SLE) is a chronic autoimmune disease that predominantly affects women of childbearing age, significantly impacting renal health. The women were 6 times more likely to have SLE compared to men, and prevalence in African Americans was twofold compared to their Caucasian counterparts. Approximately 90% of SLE patients are female, with a nearly 10:1 female-to-male ratio and six times more likely to have SLE compared to men. However, men with SLE face a higher risk of severe renal and cardiovascular complications. Renal impairment in SLE stems from glomerular, tubulointerstitial, and vascular lesions, which collectively contribute to lupus nephritis (LN) as a common complication. The 2019 EULAR/ACR classification criteria for SLE, though primarily used for classification rather than diagnosis, achieve 96.1% sensitivity and 93.4% specificity, assessing clinical symptoms like fever, cytopenia, rash, arthritis, and proteinuria, along with immunological markers such as autoantibodies and low complement levels.
The incidence of SLE varies from 0.3 to 31.5 cases per 100,000 people annually, with prevalence estimates now exceeding 50–100 cases per 100,000 adults. LN occurs in 40-50% of individuals with SLE, usually within the first five years post-diagnosis. Progression to end-stage renal disease (ESRD) affects 4.3–10.1% of these patients after ten years, with LN patients facing a 1.5 times higher mortality risk compared to those without LN. The progression risk is highest within the initial five years, with studies indicating that 50-74% of LN cases develop within a year or five years after an SLE diagnosis. Major risk factors for ESRD include high serum creatinine, class III, IV, or VI LN, elevated blood pressure, male sex, and Black race, with the cumulative ten-year ESRD incidence around 4% for SLE and 6–16% for SLE with LN.
The presence of two genotypes (G1/G2) of the APOL1 gene, and elevated levels of anti-Ro/SS-A, anti-Sm, and anti-nRNP antibodies likely contribute to the disparities making LN more frequent and severe in patients of African American, Hispanic, or Asian descent than in White patients. In terms of socio economics, whites with higher socioeconomic status tend to do develop LN at a lower rate as compared with Blacks and Hispanics, although prevalence was still high in Blacks irrespective of financial status. Children and adolescents with LN experience more severe disease, higher relapse rates, and greater organ damage than adults, with poor treatment adherence further elevating risks in younger populations. Males also tend to fare worse with LN than women, suffering more renal dysfunction. Patients with childhood-onset SLE also experienced higher rates of LN than adult-onset SLE.
Histological transformation occurs in up to 76% of LN cases, often from non-proliferative to proliferative forms. Predictors of renal disease progression include a high chronicity index, glomerular sclerosis, and tubulointerstitial injury seen at biopsy. LN is classified into six histological classes, with classes III (focal proliferative), IV (diffuse proliferative), and combined III/IV plus V being the most severe. Class IV LN has a poorer prognosis, especially the IV-G (global) subtype, which is more frequent and severe than IV-S (segmental) subtype. LN can manifest subtly, with normal urinalysis and renal function tests, or present acutely with hematuria, leukocyturia, proteinuria, or nephritic and nephrotic syndromes, underscoring the need for regular assessment of renal function, proteinuria, and urinary sediment in SLE patients. Among rare forms, vascular lesions in LN may arise from coexisting antiphospholipid syndrome (APS) or thrombotic microangiopathy (TMA), characterized by endothelial swelling and thrombus formation, especially in patients with antiphospholipid antibodies. While TMA occurs in less than 10% of cases, its presence increases the risk of acute or chronic kidney injury.
A timely diagnosis and effective treatment are the primary objective in managing SLE and LN is achieving remission or disease quiescence, characterized by low symptom severity and limited use of glucocorticoids. Long-term management includes immunosuppressive agents such as azathioprine, mycophenolate mofetil, and cyclophosphamide. Hydroxychloroquine, widely regarded as the standard SLE treatment, is associated with lower mortality rates. Recently, the FDA approved belimumab, voclosporin, and anifrolumab as additional treatment options for SLE and LN, expanding the therapeutic arsenal for these conditions. Despite treatment advances, LN patients still face a mortality risk six times higher than the general population. Kidney failure remains a leading cause of death in SLE, particularly among young women, African American, and Hispanic populations. Between 10% and 30% of patients with proliferative LN (class III, IV, or III/IV + V) require kidney replacement therapy (KRT), with complete responders exhibiting a 92% kidney survival rate at ten years. Since 2000, the incidence of LN requiring KRT has plateaued, though rates may be rising among Black populations.
Clinical Presentation, Evaluation, Biomarkers
CLINICAL PRESENTATION
Lupus nephritis is a heterogeneous disease manifestation ranging from silent subclinical renal involvement without associated symptoms, serum, or urine abnormalities to overt acute renal failure and severe nephritic or nephrotic syndromes. Most commonly, early disease presents with urine abnormalities with presence of WBC, RBC, and/or casts. LN, and other SLE-related kidney involvement, can lead to varied levels of proteinuria with even small amounts potentially being indicative of pathology.
The 2012 American College of Rheumatology (ACR) guidelines define LN as persistent proteinuria (≥0.5g/day or 3+ by dipstick or creatinine-to-protein ratio >0.5) and/or active urinary sediment (cellular casts or >5 RBC or WBC per high power field. Biopsy is recommended at baseline and if significant suspicious urine abnormalities (proteinuria ≥1g/day or ≥0.5/day plus hematuria or cellular casts) or worsening eGFR present unexplained by other potential causes. Current Kidney Disease: Improving Global Outcomes (KDIGO) guidelines recommend creatinine, eGFR, urinalysis, spot urine protein-creatinine ratio, dsDNA, and complement level testing at time of SLE diagnosis, for surveillance, and during suspected flares. Kidney biopsy is also able to evaluate for podocyte and vascular pathology and can diagnose concurrent pathology such as thrombotic microangiopathy. Biopsies can be graded on both disease activity measures such as cellularity, necrosis, crescent formation, and hyaline deposits, as well as markers of chronicity glomerulosclerosis, fibrosis, and atrophy. The particular microscopic findings are crucial for accurate disease classification and treatment recommendations. KDIGO guidelines recommend kidney biopsy interpretation by nephropathologists.
Similarly, the European Alliance of Associations for Rheumatology (EULAR) guidelines recommend kidney biopsy for evaluation of urine abnormalities or decline in eGFR. They also include anti-C1q, anti-ds-DNA, C3, C4, urinalysis, urine protein-to-creatinine ratio biomarkers and monitoring labs. Unfortunately, discordance between clinical and histological response has been documented and residual histological activity despite apparent clinical response has been associated with increased flare risk. Kidney biopsy is recommended for unexplained GFR decrease, hematuria or casts, proteinuria defined as >0.5g in 24 hours or urine protein-to-creatinine ratio >500mg/g.
In addition to defining the class of LN and evaluating for comorbid conditions, renal biopsy is beneficial in identification of subclinical disease. Repeat kidney biopsy is recommended in the setting of persistently elevated serological biomarkers although the ideal timing is debated. Benefits provided by renal biopsy need to be weighed with the invasive nature of this procedure with special consideration for bleeding risk. Timing and need for repeat biopsy remains case-dependent without available guidelines to inform this decision.
DISEASE ACTIVITY ASSESSMENT
Several disease activity measures have been developed and are currently in use for both the management and study of SLE. SLEDAI 2000 (SLEDAI-2K) was developed in 2002 via validated modifications to the initial SLEDAI developed in 1985 via expansion to include persistent disease activity to capture clinical disease manifestations. It includes neurological, vasculitic, myopathic, arthritic, mucocutaneous, serosal measures in addition to fever and hematologic abnormalities, hypocomplementemia, and ds-DNA serologies. This has been shown to be predictive of mortality. The BILAG 2004 modified the original 1988 BILAG to better capture ophthalmic and gastrointestinal disease manifestations and removal of manifestations more consistent with damage rather than activity. Additionally, this includes scoring of 9 organ systems with the goal of providing a systems-based activity assessment rather than global measure. Physician’s Global Assessment (PGA) is a simple and less granular measure that uses a visual analog scale to measure physicians’ assessment of disease activity. Though comprehensive and simple to use, it is prone to both inter-and intra-rater variability.
A renal activity score composed of weighted scores for proteinuria, as well as urine RBC and WBC counts was developed by consensus methodology with the goal of identifying variables that were considered most strongly in making a clinical diagnosis of lupus nephritis. This appears to be less commonly used. System components of SLEDAI and BILAG can be used to estimate organ-specific disease involvement. Urine biomarker testing showed superior assessment of histological disease activity by kidney biopsy than SLEDAI renal domain score in children with LN.
Composite measures based on changes or combinations of component BILAG, SLEDAI, PGA, or other scores such as BICLA (BILAG-based Composite Lupus Assessment) and SRI (SLE Responder Index) have also been used although mainly useful as clinical trial outcome measures. Thanou and Merrill (2013) and Ohmura (2021) summarized several disease activity indices, including composite scoring modalities, and outlined the implications of their specific designs in both clinical practice and trials. A recent systematic review aimed at summarizing current definitions of low, or minimal, disease activity in SLE based on SLEDAI-2K scores. Minimal disease activity defined as SLEDAI-2K ≤1 in the setting of therapies considered to be low-risk for long-time morbidity and mortality (antimalarial agents, standard dosing of immunosuppressive agents, ≤5 mg prednisone equivalent daily). Low disease activity was defined as SLEDAI-2K ≤2 in the setting of antimalarial therapy. These definitions exclude positive serologies from scoring. Lupus low activity state was developed and defined via expert consensus and required fulfillment of 5 clinical criteria including physician global assessment, clinical presentation, SLEDAI-2K, and medication regimen.
Current measures appear to be helpful in assessing current disease activity, albeit imperfectly, rather than predicting flares.
LUPUS NEPHRITIS BIOMARKERS
Biomarkers help to uncover the complex pathological processes contributing to the development of LN but also reflect nonpathogenic changes that result from disease-related damage. These include autoantibodies, serum markers of kidney function, complement levels, lymphocyte counts, both elevated and decreased serum cytokine levels, serum and urine chemokines, serum and urine cell adhesion molecules (CAMs), serum and urine proteins, micro-RNAs (miRNAs), microparticles, kidney biopsy histologic findings, kidney biopsy proteins/cytokines. Traditional biomarkers based on clinically available and utilized tests include elevated urine RBC, WBC, protein levels, presence of casts, as well as elevated BUN, creatinine, decreased C3 and C4 complement levels, and elevated anti-dsDNA antibody. Additionally, lymphocyte count has been shown to increase in response to therapy and hyperuricemia is considered a serologic marker of kidney function.
Markers of activation of specific pathogenic pathways including DNAase activity and CH50 in addition to traditional C3 and C4 levels, anti-interferon antibodies, and blood interferon (α, gamma, type I, type II) signatures have also shown biomarker capabilities. Anti-CL/β2 GPI Abs have emerged as a predictor of TMA. Although anti-SSB antibodies are associated with SLE, these do not predict histological LN nor ESRD. Anti-dsDNA and anti-α actinin antibodies have been associated with LN while anti-Smith has some suspected predictive characteristics (such as ESRD) despite lack of correlation with histologic LN. Many types of urinary biomarkers have been identified and studied including serum uric acid, urinary galectin-3 binding protein (uGAL3BP), kidney injury molecule-1 (KIM-1), and several additional urinary micro-RNAs. Various combinations of baseline histologic findings of interstitial fibrosis and tubular atrophy, presence of TMA, and presence of proliferative LN, as well as complement fractions of C1q and C3 have associations with different outcomes including prediction of disease activity, flares, and progression to ESRD.
Novel and nontraditional biomarkers investigated in more than one original study include serum autoantibodies anti-C1q, anti-C1q, anti-ENO-1, anti-neutrophil cytoplasmic antibodies. Such urine biomarkers include Tumor necrosis factor-like weak inducer of apoptosis (TWEAK), interleukin 10, interleukin 17, A proliferation-inducing ligand (APRIL), B-cell activating factor (BAFF or BLySS), monocyte chemoattractant protein 1 (MCP-1 or CCL2), activated leukocyte cell adhesion molecule (ALCAM), vascular cell adhesion molecule 1 (VCAM-1), interferon gamma-induced protein 10 (IP-10 also known as CXCL10), angiostatin, neutrophil gelatinase-associated lipocalin (NGAL), transferrin, beta-2 microglobulin (β2-MG), serum angiopoietin-like protein 4 (Angptl4), CD163. Additional serum markers include TWEAK, transforming growth factor-beta 1 (TGF-β1), Axl, HE4, soluble tumor necrosis factor receptor II (sTNFRII), miRNA-21.
A systematic review my Palazzo and colleagues in 2022 provided a summary of biomarkers clustered by purpose of biomarker including diagnosis, clinical and histological disease activity, therapeutic response, organ damage, and prognosis including progression to ESRD and mortality. Authors also included test characteristics (sensitivity, specificity, and AUC). Biomarkers highlighted for perceived clinical utility include urinary MCP-1 and NGAL based on their clinical correlation and urinary VCAM-1, CD163, and ALCAM based on their clinical correlation and validation. They note heterogeneity in outcome measures, populations, study design, and laboratory techniques that may hinder generalizability of findings and subsequent translation into clinical practice.
Comprehensive and detailed summaries of current biomarkers have been summarized in recent reviews. Unfortunately, feasibility of application of multiple novel biomarkers remains limited due to lack of validation, heterogeneity of patient populations and SLE clinical presentation. Furthermore, development of standardized scalable assays would be further required. Munroe and colleagues in 2023 developed a flare risk index on the evaluation of 37 plasma biomarkers with resulting 12-17 biomarker combinations identified capable of differentiating patients who experienced subsequent SLE flare compared to those who did not. This was further narrowed to an 11-analyte panel to optimize technical feasibility and cost. Unfortunately, this study included few patients with flare involving LN. Immunoassays that utilize algorithm-based calculators to determine disease activity indices based on plasma levels of IFN-y, IL-4, IL-7, IL-10, IL-15, BLyS/BAFF, CXCL10/IP-10, IFN-a2, osteopontin (OPN), tumor necrosis factor-related apoptosis-inducing ligand (TRAIL) are commercially available but require integration with other clinical measures. Improved biomarker capabilities that can better reflect renal pathological processes and reduce reliance on renal biopsy for definitive diagnosis are imperative.
Management
Early diagnosis and subsequent management of lupus nephritis (LN) which may be clinically silent can have vast implications for improving prognosis and reducing dialysis dependence and morbidity long term. First LN episode can lead to loss of 1/3rd of the nephrons while remaining nephrons may hypertrophy, potentially overestimating residual renal function. Add to that progression of loss of podocytes with normal aging-delay in management comes with significant consequences.
Screening for LN should be undertaken in all patients with presentation of systemic lupus erythematosus, suspicion of systemic lupus erythematosus flare and there on every 3 months for active disease and annually for inactive disease. Although anti double stranded DNA (ds DNA) and low complements can indicate active LN, utility of serological assessment is variable. Urine sediment should be characterized and GFR and spot urine protein/creatinine ratio (UPCR) measured. ACR 2024 LN guidelines recommend screening for proteinuria every 6 to 12 months. The ACR/EULAR 2019 guidelines use threshold of UPCR > 0.5 with Class 3/4 glomerulonephritis scoring the highest. Class 3 and 4 are focused on compared to other classes of LN because active immunosuppressive is used for most of the time in their treatment.
Kidney biopsy is indicated in patients with suspected flare after initial response, non-responders or in SLE with UPCR >0.5 g/g. EULAR/ERA-EDTA 2019 principles recommend considering kidney biopsy for proteinuria ≥ 0.5 g/24 h (UPCR ≥0.5g/g first void urine) or an unexplained drop in GFR. KDIGO 2021 practice guideline added positive acanthocyte sediment and presence of red blood cells or white blood cells. Kidney biopsy however is indispensable and consideration for early biopsy can lead to best outcomes. KDIGO 2024 update further outlined considering renal biopsy when proteinuria > 500 mg/g, active urine sediment and decreased eGFR.
It is important to distinguish between activity and chronicity in LN. Modified NIH activity and chronicity indices are helpful for this determination. Patients who have more chronicity reported in the biopsy have poorer outcomes. However, not all kidney diseases in LN need aggressive immunosuppression, for example class 2 LN or chronic changes with minimal active inflammation. ACR 2024, EULAR 2023 and KDIGO 2024 recommendations include Hydroxychloroquine recommendation for all patients with LN unless contraindicated at a target dose of 5 mg/kg actual body weight.
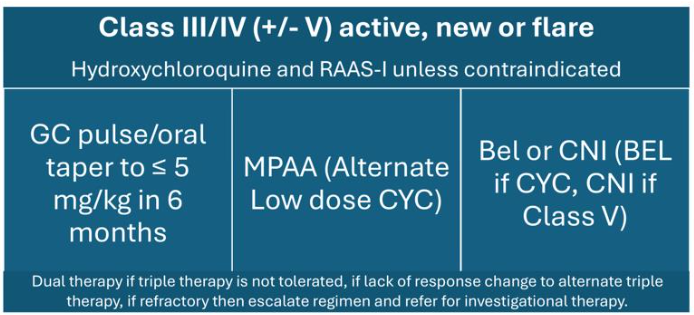
ACR 2024 conditionally recommended pulse intravenous methylprednisolone 250-1000 mg for 1-3 days followed by oral glucocorticoid <0.5 mg/kg/day with taper to ≤ 5 mg by 6 months. This induction regimen has a lower cumulative dose of glucocorticoids compared to the EULAR/ERA-EDTA 2019 guidelines which outline induction with IV methylprednisolone 500-2500 mg total with taper to oral prednisone <7.5 mg/day by 3-6 months. Induction is recommended with mycophenolic acid analog (MPAA) and belimumab, MPAA and calcineurin inhibitor (CNI) or low dose IV cyclophosphamide (EURO LUPUS dosing 500 mg every 2 weeks for 6 months) and belimumab.
Mycophenolate (2-3g/day) regimen was conditionally recommended over cyclophosphamide based regimen in 2024 ACR LN guidelines. Belimumab addition should be considered for extrarenal manifestations, significant hypertension or CrCl <45. It would also be beneficial to consider belimumab especially if the patient desires less pill burden and if using cyclophosphamide induction. If proteinuria is ≥ 3 g/g a triple immunosuppressive regimen consisting of MPAA and CNI is recommended. Hence, calcineurin inhibitors would be appropriate for nephrotic range proteinuria and combined class 3/3 or 4/5 histopathology. Neither belimumab or CNI have been studied as monotherapy for LN yet.
For maintenance minimal prednisone is recommend 2.5-5 mg/day and mycophenolate 1-2 g/day or azathioprine 2 mg/kg/day (reproductive consideration). EULAR 2023 update includes combination of belimumab with either cyclophosphamide or mycophenolate or calcineurin inhibitor for induction followed by mycophenolate alone or in combination with belimumab or calcineurin inhibitor for maintenance therapy. KGIDO 2024 update added patients with Class 3/4 LN be treated with glucocorticoids and either one of mycophenolate, low-dose cyclophosphamide, belimumab with mycophenolate or low-dose cyclophosphamide, mycophenolate and calcineurin inhibitor if GFR is not severely impaired. These updates are similar to recommendations as per EULAR 2023 update.
Fertility preservation for both males and females must be addressed if cyclophosphamide is used, and EURO lupus regimen is preferred due to low cumulative dose. Encourage patient centered discussions on Lupron shots, oocyte and sperm cryopreservation, and embryo preservation. It is also important to optimize cardiovascular risk with blood pressure control, consideration of Renin-angiotensin-aldosterone system inhibitors (RAAS-I), sodium-glucose cotransporter-2 (SGLT2) inhibitors, and treating dyslipidemia. ACR 2024 LN guideline has emphasized further by conditionally recommending RAAS-I for all patients with elevated proteinuria. Patients should be educated on high-risk medication monitoring, malignancy risk, minimizing UV light exposure and maintaining bone health especially if on chronic prednisone.
Assessment of bone density by dual energy X-ray absorptiometry (DEXA) and fracture risk assessment tool (FRAX) is imperative. Ensuring up-to-date vaccinations to minimize risk of infections must also be visited. Definitions of clinical response as per KDIGO 2024 clinical practice guidelines include primary efficacy renal response, partial response, complete response, and no kidney response. Primary efficacy renal response is UPCR <0.7 g/g and GFR not worse than 20% below baseline or ≥ 60 ml/min. Partial response includes reduction in proteinuria by at least 50% with stabilization and improving kidney function within 6-12 months of starting therapy while complete response is defined as reduction in proteinuria <0.5 g/g with stabilization or improvement in kidney function within 6-12 months of starting therapy but may be longer. Inability to achieve partial or complete response within 6-12 months is defined as no kidney response.
Labs to target include urine protein to creatinine ratio, serum creatinine and EGFR. Target reduction in proteinuria by at least 25% with stable GFR +/- 10% baseline at 3 months, reduction in proteinuria by at least 50% at 6 months. Target proteinuria <0.5-0.7 g/24 hours at 12-24 months. Nephrotic range of proteinuria at baseline may require an additional 6-12 months to reach complete clinical response, however if proteinuria is progressively improving it is reassuring. If clinical response has not reached 3-12 months switching to an alternate triple therapy is recommended and escalating to triple therapy if initial dual therapy used. If refractory disease it is crucial to check for medication adherence, considering anti-CD 20 and repeating biopsy.
Optimal duration is at least 3 to 5 years of treatment with 1 year of complete clinical remission with follow up withdrawing immunosuppression. Withdrawal of immunosuppression comes with its own risk of disease activity and flares, worsening kidney outcomes contributing to morbidity and mortality. It was noted that at least 30% of complete responders may have ongoing serological activity which may correlate with subsequent kidney flare at time of withdrawal of immunosuppression.
Belimumab, BAFF (Blys) monoclonal antibody was first approved in 2011 for non-renal lupus but approved in 2020 for LN in intravenous and subcutaneous formulations (BLISS-LN trial). 448 patients were followed for two years and received induction with high dose steroids and induction per EUROLUPUS cyclophosphamide or mycophenolate and maintenance with low-dose steroids and azathioprine or lower dose mycophenolate. At 6 months prednisone dose was ≤10 mg/day and patients who had received belimumab had 55% greater odds of achieving primary end point with greater mean eGFR values compared with placebo.
Voclosporin, a novel structurally modified calcineurin inhibitor, approved in January 2021 as a combination immunosuppressive therapy which inhibits T-cell activation, cytokine production but also promote podocyte stability which is incredibly significant for patients who have proteinuria. Unique features include consistent dose response as well as no need for drug level monitoring. AURORA Phase 3 study consisted of a regimen of mycophenolate 2 g per day, voclosporin 23.7 mg BID and a rapid taper of oral corticosteroids to 2.5 mg/day at week 16. More patients achieved complete renal response, greater renal response versus control as early as 24 weeks, and reduction in proteinuria twice faster. AURORA 2 study confirmed sustained reduction in proteinuria and eGFR stability at 3 years.
Consideration for faster prednisone taper and less overall steroid has been advocated since the rapid prednisone tapers used in the AURORA trials. EULAR 2023 recommendations emphasized reduction of maintenance corticosteroids to ≤ 5 mg/day and withdrawing steroids when possible. KDIGO 2024 outlined tapering corticosteroids to < 5 mg by week 25 in moderate and high-dose schemes and < 2.5 mg in reduced dose scheme. BLISS-LN and AURORA 1 showed improved outcomes with triple compared to dual therapies.
Table 1. Selected serum and urine lupus nephritis biomarkers by sample and type (adapted from Ref 38-40)
| Sample | Biomarker type | Biomarker |
|---|---|---|
| Serum | Markers of kidney function | Creatinine/eGFR, urea, uric acid |
| Serum | Antibodies | Anti-dsDNA, ANCA, anti-C1q, anti-CRP, anti-ENO-1 |
| Serum | Complements | C3, C4 |
| Serum | Cytokines and chemokines | TWEAK, IL-10, IL-17 |
| Serum | Proteins | Axl, HE4, sTNFRII |
| Serum | Micro-ribonucleic acids | MiRNA-21 |
| Urine | Markers of kidney function | Protein, WBC, RBC, casts |
| Urine | Cytokines and chemokines | TWEAK, TGF-β1, APRIL, BAFF, MCP-1, ALCAM, VCAM-1, IP-10 |
| Urine | Specific proteins | Angiostatin, NGAL, transferrin, β2-MG, Angptl4, CD163 |
There are many emerging therapies on the horizon with promising evidence. One of those includes Obinutuzmab (anti-CD20 monoclonal antibody) with promising results in the Phase 2 NOBILITY trial where improve renal responses through week 104 were observed in LN patients who received combination of obinutuzumab with standard therapy. REGENCY trial is the phase 3 trial investigating Obinutuzumab, ORCHID-LN is a phase 2 trial evaluating guselkumab and SELUNE trial is a phase 3 trial evaluating Secukinumab for LN.
Raviluzumab (complement 5 inhibitor), iptacopan (factor B inhibitor), anifrolumab are other potential treatment targets.
Discussion and Future Direction
Despite the immense progress made in diagnosis and management of LN over the last few decades, it remains an important cause of morbidity and mortality in SLE. Around 70% of patients do not achieve CR after a 6-month standard induction treatment and 10–30% of them still progress to ESRD within 10 years of diagnosis, with an associated burden of increased cardiovascular and infectious risk. The biggest challenges in management of LN remains prevention of relapses and preservation of renal function and minimization of drug toxicity, primarily due to long-term GC therapy.
Recent advancement in treatment of LN includes success with addition of Voclosporin and Belimumab as induction agents along with standard therapy leading to improved outcome as well as a reduction in the cumulative dose of glucocorticoids. However, these agents may also have their own limitations due to adverse events. VOC can worsen hypertension and reduce GFR, limiting its use in CKD, and long-term histological data on nephrotoxicity are lacking. Other biologic agents such as new generation anti-CD20 (obinutuzumab), IFN-I antagonists (anifrolumab), and RTX-BEL sequential therapy or combination hold promise in improving the efficacy-to-toxicity balance in LN treatment and in offering new tools to manage refractory and relapsing disease.
In addition to these drugs, several exciting new developments particularly using cellular therapy for treatment of LN are on the horizon. These include CD19 CAR T-cell therapy, natural killer cells (NK) cells that target similar cytotoxic cellular mechanisms and BCMA CAR T-cell. Similarly engineered T cells which express chimeric auto-antibody receptors (DNA-CAART) and can selectively target B cells expressing anti-dsDNA autoantibodies. Another expanding area of research is that of therapeutic manipulation of different ncRNAs, which could inhibit the expression of crucial genes involved in LN. This intervention could modulate multiple pathways and interfere with key immunological and inflammatory mechanisms of kidney damage. Additionally, as highlighted above, there remains an unmet need for biomarkers to identify high-risk patients who require a stronger induction therapy with a triple-drug regimen to achieve CR and distinguish them those who do not need more aggressive therapy.
Another exciting development is the potential for the “Omic” approach in evaluation of LN. Rapid ongoing progress in molecular diagnosis of LN based on genetic fingerprints and specific pathway activation, integrated with artificial intelligence and machine learning tools, has the potential for the discovery of many new non-invasive biomarkers, which may replace the need for renal biopsy in diagnosis and treatment of LN.
Conclusion
The last 2 decades have seen a substantial advancement in screening and management of lupus nephritis. Additionally, promising advances have been made in availability of biomarkers and therapeutic options. Despite these advances, there continue to exist unmet needs for early detection of patients at risk and those having active flare-up. Using new protocols incorporating recently approved therapeutic agents to treat has led to improved renal remission rates in patients with LN but there still are a significant percentage of patients who do not achieve renal remission despite receiving standard of care therapy for induction and maintenance treatment. However, additional studies with newer therapeutic agents and cellular therapies show promising potential in treatment of lupus nephritis.
References
2. Fiehn, C.; Hajjar, Y.; Mueller, K.; Waldherr, R.; Ho, A.D.; Andrassy, K. Improved clinical outcome of lupus nephritis during the past decade: Importance of early diagnosis and treatment. Ann. Rheum. Dis. 2003, 62, 435–439.
3. Desai SB, Ahdoot R, Malik F, Obert M, Hanna R. New guidelines and therapeutic updates for the management of lupus nephritis. Curr Opin Nephrol Hypertens. 2024;33(3):344-353. doi:10.1097/MNH.0000000000000969.
4. Smith CD, Cyr M. The History of Lupus Erythematosus. Rheum Dis Clin N Am. 1988;14(1):1-14. doi:10.1016/S0889-857X(21)00942-X.
5. Hahn BH, McMahon MA, Wilkinson A, et al. American College of Rheumatology guidelines for screening, treatment, and management of lupus nephritis. Arthritis Care Res. 2012;64(6):797-808. doi:10.1002/acr.21664.
6. Alarcon GS, McGwin G Jr, Petri M, et al. Baseline characteristics of a multiethnic lupus cohort: PROFILE. Lupus. 2002;11:95–101.
7. Feldman CH, Hiraki LT, Liu J, Fischer MA, Solomon DH, Alarcón GS, Winkelmayer WC, Costenbader KH. Epidemiology and sociodemographics of systemic lupus erythematosus and lupus nephritis among US adults with Medicaid coverage, 2000-2004. Arthritis Rheum. 2013 Mar;65(3):753-63. doi: 10.1002/art.37795. PMID: 23203603; PMCID: PMC3733212.
8. Mok CC, Kwok RC, Yip PS. Effect of renal disease on the standardized mortality ratio and life expectancy of patients with systemic lupus erythematosus. Arthritis Rheum. 2013;65:2154–2160.
9. Anders HJ, Rovin B. A pathophysiology-based approach to the diagnosis and treatment of lupus nephritis. Kidney Int 2016; 90:493–501.
10. Rovin BH, Adler SG, Barratt J, Bridoux F, Burdge KA, Chan TM, Cook HT, Fervenza FC, Gibson KL, Glassock RJ, Jayne DRW, Jha V, Liew A, Liu ZH, Mejía-Vilet JM, Nester CM, Radhakrishnan J, Rave EM, Reich HN, Ronco P, Sanders JF, Sethi S, Suzuki Y, Tang SCW, Tesar V, Vivarelli M, Wetzels JFM, Lytvyn L, Craig JC, Tunnicliffe DJ, Howell M, Tonelli MA, Cheung M, Earley A, Floege J. Executive summary of the KDIGO 2021 Guideline for the Management of Glomerular Diseases. Kidney Int. 2021 Oct;100(4):753-779. doi: 10.1016/j.kint.2021.05.015.
11. Petri M, Orbai A-M, Alarcón GS, Gordon C, Merrill JT, Fortin PR, Bruce IN, Isenberg D, Wallace DJ, Nived O, Sturfelt G, Ramsey-Goldman R, Bae SC, Hanly JG, Sanchez-Guerrero J, Clarke A, Aranow C, Manzi S, Urowitz MB, Gladman DD, Kalunian K, Costner M, Werth V, Zoma A, Bernatsky S, Ruiz-Irastorza G, Khamashta M, Jacobsen S, Buyon JP, Maddison P, Dooley MA, Van Vollenhoven R, Ginzler E, Stoll T, Peschken C, Jorizzo JL, Callen JP, Lim S, Fessler BJ, Inanc M, Kamen DL, Rahman A, Steinsson K, Franks Jr. AG , Sigler L, Hameed S, Fang H, Pham N, Brey R, Weisman MH, McGwin Jr. G, Magder LS. Derivation and validation of Systemic Lupus International Collaborating Clinics (SLICC) classification criteria for systemic lupus erythematosus. Arthritis Rheum 2012; 64:2677-2686.
12. Fanouriakis A, Kostopoulou M, Cheema K, Anders HJ, Aringer M, Bajema I, Boletis J, Frangou E, Houssiau FA, Hollis J, Karras A, Marchiori F, Marks SD, Moroni G, Mosca M, Parodis I, Praga M, Schneider M, Smolen JS, Tesar V, Trachana M, van Vollenhoven RF, Voskuyl AE, Teng YKO, van Leew B, Bertsias G, Jayne D, Boumpas DT. 2019 Update of the Joint European League Against Rheumatism and European Renal Association-European Dialysis and Transplant Association (EULAR/ERA-EDTA) recommendations for the management of lupus nephritis. Ann Rheum Dis. 2020 Jun;79(6):713-723. doi:10.1136/annrheumdis-2020-216924.
13. Almaani S, Meara A, Rovin BH. Update on Lupus Nephritis. Clin J Am Soc Nephrol. 2017 May 8;12(5):825-835. doi: 10.2215/CJN.05780616. Epub 2016 Nov 7. PMID: 27821390; PMCID: PMC5477208.
14. Malvar A, Pirruccio P, Alberton V, et al. Histologic versus clinical remission in proliferative lupus nephritis. Nephrol Dial Transplant. 2017;32:1338–1344.
15. Zickert A, Sundelin B, Svenungsson E, et al. Role of early repeated renal biopsies in lupus nephritis. Lupus Sci Med. 2014;1:e000018.
16. Stokes MB, D’Agati VD. Classification of Lupus Nephritis; Time for a Change? Adv Chronic Kidney Dis. 2019;26(5):323-329. doi:10.1053/j.ackd.2019.06.002.
17. Danchenko N, Satia J, Anthony M. Epidemiology of systemic lupus erythematosus: a comparison of worldwide disease burden. Lupus 2006;15:308–18.
18. Moroni G, Radice A, Giammarresi G, Quaglini S, Gallelli B, Leoni A, et al. Are laboratory tests useful for monitoring the activity of lupus nephritis? A 6-year prospective study in a cohort of 228 patients with lupus nephritis. Ann Rheum Dis 2009;68:234–7.
19. Ho A, Barr SG, Magder LS, Petri M. A decrease in complement is associated with increased renal and hematologic activity in patients with systemic lupus erythematosus. Arthritis Rheum 2001;44:2350–7.
20. Alforaih N, Whittall-Garcia L, Touma Z. A Review of Lupus Nephritis. J Appl Lab Med. 2022;7(6):1450-1467. doi:10.1093/jalm/jfac036.
21. Pons-Estel GJ, Alarcon GS, McGwin G, Danila MI, Zhang J, Bastian HM, et al. Protective effect of hydroxychloroquine on renal damage in patients with lupus nephritis: LXV. Data From a multiethnic US cohort. Arthritis Rheum 2009;61:830–9.
22. Fanouriakis A, Tziolos N, Bertsias G, et al. Update οn the diagnosis and management of systemic lupus erythematosus Annals of the Rheumatic Diseases 2021;80:14-25.
23. Siegel CH, Sammaritano LR. Systemic Lupus Erythematosus: A Review. JAMA. 2024;331(17):1480–1491. doi:10.1001/jama.2024.2315.
24. Gasparotto M, Gatto M, Binda V, Doria A, Moroni G. Lupus nephritis: clinical presentations and outcomes in the 21st century. Rheumatology (Oxford). 2020 Dec 5;59(Suppl5):v39-v51. doi: 10.1093/rheumatology/keaa381. PMID: 33280015; PMCID: PMC7751166.
25. Mahajan A, Amelio J, Gairy K, Kaur G, Levy RA, Roth D, Bass D. Systemic lupus erythematosus, lupus nephritis and end-stage renal disease: a pragmatic review mapping disease severity and progression. Lupus. 2020 Aug;29(9):1011-1020. doi: 10.1177/0961203320932219. Epub 2020 Jun 22. PMID: 32571142; PMCID: PMC7425376.
26. Hasan B, Fike A, Hasni S. Health disparities in systemic lupus erythematosus-a narrative review. Clin Rheumatol. 2022 Nov;41(11):3299-3311. doi: 10.1007/s10067-022-06268-y. Epub 2022 Jul 31. PMID: 35907971; PMCID: PMC9340727.
27. Suchun Li, Qimei Luo, Yuting Fan, Chen Zhao, Fengxian Huang, Xi Xia, Wei Chen; Clinicopathological Characteristics and Prognosis of Lupus Nephritis Patients with Acute Kidney Injury. Am J Nephrol 12 December 2023; 54 (11-12): 536–545. https://doi.org/10.1159/000533847.
28. Anders HJ, Saxena R, Zhao MH, Parodis I, Salmon JE, Mohan C. Lupus nephritis. Nat Rev Dis Primers. 2020 Jan 23;6(1):7. doi: 10.1038/s41572-019-0141-9. PMID: 31974366.
29. Rovin BH, Ayoub IM, Chan TM, Liu ZH, Mejía-Vilet JM, Floege J. KDIGO 2024 Clinical Practice Guideline for the management of LUPUS NEPHRITIS. Kidney Int. 2024;105(1):S1-S69. doi:10.1016/j.kint.2023.09.002
30. Lupus Clinical Practice Guideline (Accessed October 20, 2024). https://rheumatology.org/lupus-guideline.
31. Gladman DD, Ibañez D, Urowitz MB. Systemic lupus erythematosus disease activity index 2000. J Rheumatol. 2002 Feb;29(2):288-91. PMID: 11838846.
32. Isenberg, D.A., Rahman, A., Allen, E.B.I.L.A.G., Farewell, V., Akil, M., Bruce, I.N., D’cruz, D., Griffiths, B., Khamashta, M., Maddison, P. and McHugh, N., 2005. BILAG 2004. Development and initial validation of an updated version of the British Isles Lupus Assessment Group’s disease activity index for patients with systemic lupus erythematosus. Rheumatology, 44(7), pp.902-906.
33. Thanou A, Jupe E, Purushothaman M, Niewold TB, Munroe ME. Clinical disease activity and flare in SLE: Current concepts and novel biomarkers. J Autoimmun. 2021;119:102615.
34. Koichiro Ohmura, Which is the best SLE activity index for clinical trials?, Modern Rheumatology, Volume 31, Issue 1, 2 January 2021, Pages 20–28, https://doi.org/10.1080/14397595.2020.1775928.
35. Petri, M., Kasitanon, N., Lee, S.S., Link, K., Magder, L., Bae, S.C., Hanly, J.G., Isenberg, D.A., Nived, O., Sturfelt, G. and Van Vollenhoven, R., 2008. Systemic lupus international collaborating clinics renal activity/response exercise: development of a renal activity score and renal response index. Arthritis & Rheumatism: Official Journal of the American College of Rheumatology, 58(6), pp.1784-1788.
36. Aljaberi N, Wenderfer SE, Mathur A, Qiu T, Jose S, Merritt A, Rose J, Devarajan P, Huang B, Brunner H. Clinical measurement of lupus nephritis activity is inferior to biomarker-based activity assessment using the renal activity index for lupus nephritis in childhood-onset systemic lupus erythematosus. Lupus Sci Med. 2022 May;9(1):e000631. doi: 10.1136/lupus-2021-000631. PMID: 35568436; PMCID: PMC9109101.
37. Thanou A, Merrill JT. Treatment of systemic lupus erythematosus: new therapeutic avenues and blind alleys. Nat Rev Rheumatol. 2014;10(1):23-34. doi:10.1038/nrrheum.2013.145
38. Tselios K, Gladman DD, Urowitz MB. How can we define low disease activity in systemic lupus erythematosus? Semin Arthritis Rheum. 2019 Jun;48(6):1035-1040. doi: 10.1016/j.semarthrit.2018.10.013. Epub 2018 Oct 16. PMID: 30415943.
39. Alduraibi, F.K. and Tsokos, G.C., 2024. Lupus nephritis biomarkers: a critical review. International Journal of Molecular Sciences, 25(2), p.805.
40. Renaudineau, Y., Brooks, W. and Belliere, J., 2023. Lupus nephritis risk factors and biomarkers: An update. International Journal of Molecular Sciences, 24(19), p.14526.
41. Palazzo, L., Lindblom, J., Mohan, C. and Parodis, I., 2022. Current insights on biomarkers in lupus nephritis: a systematic review of the literature. Journal of Clinical Medicine, 11(19), p.5759.
42. Munroe, M.E., Blankenship, D., DeFreese, D., Purushothaman, M., DeJager, W., Macwana, S., Guthridge, J.M., Kamp, S., Redinger, N., Aberle, T. and Chakravarty, E.F., 2023. A flare risk index informed by select immune mediators in systemic lupus erythematosus. Arthritis & rheumatology, 75(5), pp.723-735.
43. Banos A, Bertsias G. Flares in Lupus Nephritis: Risk Factors and Strategies for Their Prevention. Curr Rheumatol Rep. 2023 Oct;25(10):183-191. doi: 10.1007/s11926-023-01109-6. Epub 2023 Jul 15.
44. Sakhi H, Moktefi A, Bouachi K, Audard V, Hénique C, Remy P, Ollero M, El Karoui K. Podocyte Injury in Lupus Nephritis. J Clin Med. 2019 Aug 29;8(9):1340. doi: 10.3390/jcm8091340.
45. Bruschi M, Angeletti A, Prunotto M, Meroni PL, Ghiggeri GM; Zeus consortium; Moroni G, Sinico RA, Franceschini F, Fredi M, Vaglio A, Cavalli A, Scapozza L, Patel JJ, Tan JC, Lo KC, Cavagna L, Petretto A, Pratesi F, Migliorini P, Locatelli F, Pazzola G, Pesce G, Giannese D, Manfredi A, Ramirez GA, Esposito P, Murdaca G, Negrini S, Bui F, Trezzi B, Emmi G, Cavazzana I, Binda V, Fenaroli P, Pisan I, Montecucco C, Santoro D, Scolari F, Mescia F, Volpi S, Mosca M, Tincani A, Ravelli A, Murtas C, Candiano G, Caridi G, La Porta E, Verrina E. A critical view on autoantibodies in lupus nephritis: Concrete knowledge based on evidence. Autoimmun Rev. 2024 May;23(5):103535. doi: 10.1016/j.autrev.2024.103535.
46. 2024 American College of Rheumatology (ACR) Guideline for the Screening, Treatment, and Management of Lupus Nephritis. 2024 Nov 18 (Pending publication).
47. Naomi, I, Maria., Anne, Davidson. (2020). Protecting the kidney in systemic lupus erythematosus: from diagnosis to therapy. Nature Reviews Rheumatology, 16(5):255-267. doi: 10.1038/S41584-020-0401-9.
48. Bajema IM, Wilhelmus S, Alpers CE, Bruijn JA, Colvin RB, Cook HT, D’Agati VD, Ferrario F, Haas M, Jennette JC, Joh K, Nast CC, Noël LH, Rijnink EC, Roberts ISD, Seshan SV, Sethi S, Fogo AB. Revision of the International Society of Nephrology/Renal Pathology Society classification for lupus nephritis: clarification of definitions, and modified National Institutes of Health activity and chronicity indices. Kidney Int. 2018 Apr;93(4):789-796. doi: 10.1016/j.kint.2017.11.023.
49. Aringer M, Costenbader K, Daikh D, Brinks R, Mosca M, Ramsey-Goldman R, Smolen JS, Wofsy D, Boumpas DT, Kamen DL, Jayne D, Cervera R, Costedoat-Chalumeau N, Diamond B, Gladman DD, Hahn B, Hiepe F, Jacobsen S, Khanna D, Lerstrøm K, Massarotti E, McCune J, Ruiz-Irastorza G, Sanchez-Guerrero J, Schneider M, Urowitz M, Bertsias G, Hoyer BF, Leuchten N, Tani C, Tedeschi SK, Touma Z, Schmajuk G, Anic B, Assan F, Chan TM, Clarke AE, Crow MK, Czirják L, Doria A, Graninger W, Halda-Kiss B, Hasni S, Izmirly PM, Jung M, Kumánovics G, Mariette X, Padjen I, Pego-Reigosa JM, Romero-Diaz J, Rúa-Figueroa Fernández Í, Seror R, Stummvoll GH, Tanaka Y, Tektonidou MG, Vasconcelos C, Vital EM, Wallace DJ, Yavuz S, Meroni PL, Fritzler MJ, Naden R, Dörner T, Johnson SR. 2019 European League Against Rheumatism/American College of Rheumatology Classification Criteria for Systemic Lupus Erythematosus. Arthritis Rheumatol. 2019 Sep;71(9):1400-1412. doi: 10.1002/art.40930.
50. Fanouriakis A, Kostopoulou M, Andersen J, Aringer M, Arnaud L, Bae SC, Boletis J, Bruce IN, Cervera R, Doria A, Dörner T, Furie RA, Gladman DD, Houssiau FA, Inês LS, Jayne D, Kouloumas M, Kovács L, Mok CC, Morand EF, Moroni G, Mosca M, Mucke J, Mukhtyar CB, Nagy G, Navarra S, Parodis I, Pego-Reigosa JM, Petri M, Pons-Estel BA, Schneider M, Smolen JS, Svenungsson E, Tanaka Y, Tektonidou MG, Teng YO, Tincani A, Vital EM, van Vollenhoven RF, Wincup C, Bertsias G, Boumpas DT. EULAR recommendations for the management of systemic lupus erythematosus: 2023 update. Ann Rheum Dis. 2024 Jan 2;83(1):15-29. doi: 10.1136/ard-2023-224762.
51. Sammaritano LR, Bermas BL, Chakravarty EE, Chambers C, Clowse MEB, Lockshin MD, Marder W, Guyatt G, Branch DW, Buyon J, Christopher-Stine L, Crow-Hercher R, Cush J, Druzin M, Kavanaugh A, Laskin CA, Plante L, Salmon J, Simard J, Somers EC, Steen V, Tedeschi SK, Vinet E, White CW, Yazdany J, Barbhaiya M, Bettendorf B, Eudy A, Jayatilleke A, Shah AA, Sullivan N, Tarter LL, Birru Talabi M, Turgunbaev M, Turner A, D’Anci KE. 2020 American College of Rheumatology Guideline for the Management of Reproductive Health in Rheumatic and Musculoskeletal Diseases. Arthritis Care Res (Hoboken). 2020 Apr;72(4):461-488. doi: 10.1002/acr.24130.
52. Frangou E, Anders HJ, Bajema IM, Teng YKO, Malvar A, Rovin BH, Kronbichler A. Immunosuppression Withdrawal in Patients with Lupus Nephritis: When, How, and for Whom Will It Be Safe? J Am Soc Nephrol. 2024 Jul 1;35(7):955-958. doi: 10.1681/ASN.0000000000000365. Epub 2024 Apr 9.
53. Furie R, Petri M, Zamani O. A phase III, randomized, placebo-controlled study of belimumab, a monoclonal antibody that inhibits B lymphocyte stimulator, in patients with systemic lupus erythematosus. Arthritis Rheum. 2011;63(12):3918–3930. doi: 10.1002/art.30613.
54. Rovin BH, Teng YKO, Ginzler EM, Arriens C, Caster DJ, Romero-Diaz J, Gibson K, Kaplan J, Lisk L, Navarra S, Parikh SV, Randhawa S, Solomons N, Huizinga RB. Efficacy and safety of voclosporin versus placebo for lupus nephritis (AURORA 1): a double-blind, randomised, multicentre, placebo-controlled, phase 3 trial. Lancet. 2021 May 29;397(10289):2070-2080. doi: 10.1016/S0140-6736(21)00578-X.
55. Saxena A, Ginzler EM, Gibson K, Satirapoj B, Santillán AEZ, Levchenko O, Navarra S, Atsumi T, Yasuda S, Chavez-Perez NN, Arriens C, Parikh SV, Caster DJ, Birardi V, Randhawa S, Lisk L, Huizinga RB, Teng YKO. Safety and Efficacy of Long-Term Voclosporin Treatment for Lupus Nephritis in the Phase 3 AURORA 2 Clinical Trial. Arthritis Rheumatol. 2024 Jan;76(1):59-67. doi: 10.1002/art.42657.
56. Furie RA, Aroca G, Cascino MD, Garg JP, Rovin BH, Alvarez A, Fragoso-Loyo H, Zuta-Santillan E, Schindler T, Brunetta P, Looney CM, Hassan I, Malvar A. B-cell depletion with obinutuzumab for the treatment of proliferative lupus nephritis: a randomised, double-blind, placebo-controlled trial. Ann Rheum Dis. 2022 Jan;81(1):100-107. doi: 10.1136/annrheumdis-2021-220920.
57. Avasare R, Drexler Y, Caster DJ, Mitrofanova A, Jefferson JA. Management of Lupus Nephritis: New Treatments and Updated Guidelines. Kidney360. 2023 Oct 1;4(10):1503-1511. doi: 10.34067/KID.0000000000000230.
58. Schett G, Mackensen A, Mougiakakos D. CAR T-cell therapy in autoimmune diseases. Lancet 2023; 402: 2034–44.
59. Mackensen A, Müller F, Mougiakakos D, Böltz S, Wilhelm A, Aigner M, Völkl S, Simon D, Kleyer A, Munoz L, Kretschmann S, Kharboutli S, Gary R, Reimann H, Rösler W, Uderhardt S, Bang H, Herrmann M, Ekici AB, Buettner C, Habenicht KM, Winkler TH, Krönke G, Schett G. Anti-CD19 CAR T cell therapy for refractory systemic lupus erythematosus. Nat Med. 2022 Oct;28(10):2124-2132. doi: 10.1038/s41591-022-02017-5.
60. Müller F, Taubmann J, Bucci L, Wilhelm A, Bergmann C, Völkl S, Aigner M, Rothe T, Minopoulou I, Tur C, Knitza J, Kharboutli S, Kretschmann S, Vasova I, Spoerl S, Reimann H, Munoz L, Gerlach RG, Schäfer S, Grieshaber-Bouyer R, Korganow AS, Farge-Bancel D, Mougiakakos D, Bozec A, Winkler T, Krönke G, Mackensen A, Schett G. CD19 CAR T-Cell Therapy in Autoimmune Disease – A Case Series with Follow-up. N Engl J Med. 2024 Feb 22;390(8):687-700. doi: 10.1056/NEJMoa2308917.
61. Figueroa‐Parra G, Cuéllar‐Gutiérrez MC, González‐Treviño M, et al. Impact of Glucocorticoid Dose on Complete Response, Serious Infections, and Mortality During the Initial Therapy of Lupus Nephritis: A Systematic Review and Meta‐Analysis of the Control Arms of Randomized Controlled Trials. Arthritis Rheumatol. 2024;76(9):1408-1418. doi:10.1002/art.42920
62. Sobhy N, Ezzat Y, Gamal SM, et al. Cumulative pulse methylprednisolone and its relation to disease activity, damage and mortality in systemic lupus erythematosus patients: A post hoc analysis of COMOSLE-EGYPT study. Clin Rheumatol. 2024;43(3):985-992. doi:10.1007/s10067-023-06858-4
63. Solé C, Royo M, Sandoval S, Moliné T, Gabaldón A, Cortés-Hernández J. Precise Targeting of Autoantigen-Specific B Cells in Lupus Nephritis with Chimeric Autoantibody Receptor T Cells. Int J Mol Sci. 2024;25(8):4226. doi:10.3390/ijms25084226
64. So BYF, Yap DYH, Chan TM. MicroRNAs in Lupus Nephritis–Role in Disease Pathogenesis and Clinical Applications. Int J Mol Sci. 2021;22(19):10737. doi:10.3390/ijms221910737