

Adverse Outcomes of Cervical Spine Manipulation
A Case Report: Adverse Outcomes Following Cervical Spine Manipulation – A New Chronic Neck Patient?
Brun Kaalb, Tony McArthur, Manuel Contet, Kristoffer Kaalb
Published: 28 February 2025
Abstract: Cervical cord injury caused by spinal manipulation is a serious concern, and predictors of cervical spine manipulation has been emphasized to prevent adverse events. In October 2012, the International Federation of Orthopaedic Manipulative Physical Therapists developed and approved a framework for a safer clinical assessment of the cervical spine. This framework focused on evaluating the potential for Cervical Arterial and Neurological Dysfunction. Cervical spine injuries with Cervical Arterial and Neurological Dysfunction can be a serious condition, and it needs to be considered ahead of any intervention.
Keywords: cervical spine manipulation, adverse outcomes, cervical cord injury, clinical assessment, neurological dysfunction
Introduction
Cervical cord injury caused by spinal manipulation is a serious concern, and predictors of cervical spine manipulation has been emphasized to prevent adverse events. In October 2012, the International Federation of Orthopaedic Manipulative Physical Therapists developed and approved a framework for a safer clinical assessment of the cervical spine. This framework focused on evaluating the potential for Cervical Arterial and Neurological Dysfunction. Cervical spine injuries with Cervical Arterial and Neurological Dysfunction can be a serious condition, and it needs to be considered ahead of any intervention.

Case Report
This case report describes a patient with chronic neck pain following cervical spine manipulation techniques. The patient presented with significant neurological symptoms on both sides of the neck, caused by combined end-range cervical rotation and extension. We decided not to proceed with axial MRI in these cases. We followed up with an axial view, which showed…
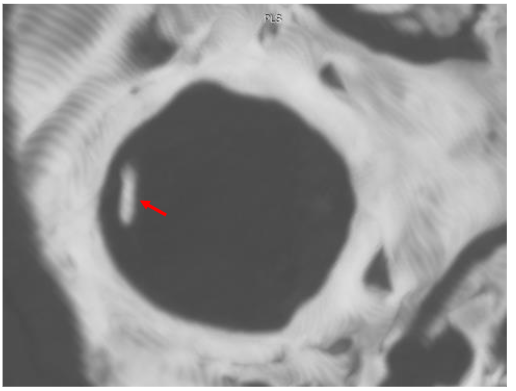
The MRI results illustrated non-existing R. Rectus Capitis Minor (RCM). This small, but vital muscle, normally goes from the atlas to the occipital bone. In this case, we located some loose connective tissue without the supporting muscular collagen fibers. See Figure 5.
The aim of this case report was to highlight the potential for significant spinal impairment and to explore the potential for clinical findings. The findings were correlated with the clinical findings presented.

Imaging Protocol Summarized
This study outlines a standardized protocol for magnetic resonance imaging (MRI) of the cervical spine using the 3T Siemens Skyra/Numaris4, Version Syngo MR E11. Utilizing a 20-channel Head and Neck coil, the imaging focuses on evaluating ligament integrity, particularly the atlas C1, through a combination of neutral and rotated positions.
Case Report Findings
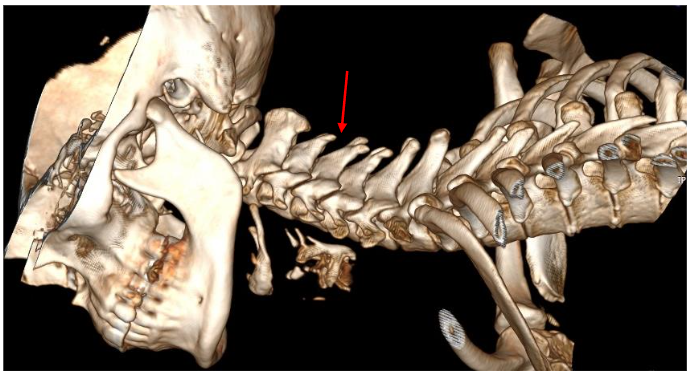
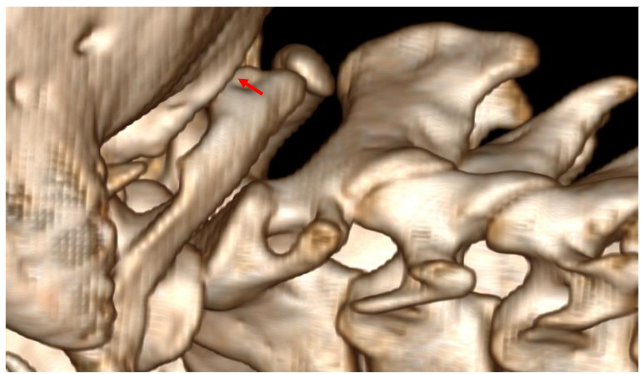
We positioned the cervical spine in a rotated position, and the findings showed that the C1-2 segment placed under tension. The MRI results indicated a cross-sectional lesion to the Anterior Longitudinal Ligament illustrated in Figure 10.
Discussion
This case report shows the very serious imbalance of the cervical spine manipulation techniques and simultaneously controlling the manipulative impact on the cervical morphology, biomechanics, vascular, and neurological system. The report lacks detailed documentation of clinical findings and a clear rationale for performing cervical manipulation. There are no documented findings that would justify the use of this treatment technique on her asymptomatic neck.
Conclusion
This case report highlights the significance of a clinical assessment combined with individualized pre-manipulative CT and MRI scanning before performing Cervical Spine Manipulation. Assessing the bone and soft tissue status in advance can help reduce the risk of creating a new chronic neck patient or exacerbating existing soft tissue lesions.
References
1. Kaalb BR, McArthur T, Kaalb K. A Case Report: Adverse Outcomes Following Cervical Spine Manipulation – A New Chronic Neck Patient? Medical Research Archives 2024;11:29-12(1):1 doi:10.18103/mra.v11i1.5940
2. Chung OJ. MRI confirmed cervical cord injury caused by spinal manipulation in a Chinese patient. Spinal Cord. Apr 2020;40(4):196-9. doi:10.1038/s41393-021-01724-3.
3. Murphy DR, Hurwitz EL, Gregory AA. Manipulation in the presence of cervical spinal cord compression: a case report. J Manipulative Physiol Ther. Mar-Apr 2006;29(2):236-44. doi:10.1016/j.jmpt.2006.01.001
4. Auerbach EJ, Marchi J, Anders J, et al. The role of physical therapists in managing patients with neck pain: a review of case reports and series. J Orthop Sports Phys Ther. May 2012;42(5):446-54. doi:10.2519/jospt.20.13890