






Alburnin Levels and Fracture Risk in Older Adults
THE ASSOCIATION OF ALBUMINURIA WITH FRACTURE RISK
Joshua I Barzilay MD¹, Petra Buzkova PhD², Jane A Cauley PhD³, Howard A. Fink MD, MPH⁴, Laura Carbone MD, MPH⁵, John A Robbins MD⁶, Rachel Elam MD⁷, Elizabeth Lisa Samelson PhD
- Kaiser Permanente of Georgia, Atlanta, GA
- University of Washington School of Public Health, Seattle, WA
- University of Pittsburgh School of Public Health, Pittsburgh, PA
- Veterans Affairs Health Care System, Minneapolis, MN
- Medical College of Georgia at Augusta University
- University of California at Davis, Sacramento, CA
- Medical College of Georgia at Augusta University, Augusta, GA
- Marcus Institute for Aging, Research at Hebrew Senior Life, Boston, MA
OPEN ACCESS
PUBLISHED: 30 April 2025
CITATION: Barzilay, J. I., et al., 2025. THE ASSOCIATION OF ALBUMINURIA WITH FRACTURE RISK. Medical Research Archives, [online] 13(4).
https://doi.org/10.18103/mra.v13i4.6473
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI
https://doi.org/10.18103/mra.v13i4.6473
ISSN2375-1924
ABSTRACT
Background: The loss of bone density (osteoporosis) and the consequent increased risk of fracture are strongly related to aging. In women, the loss of estrogen production in the menopause also contributes to bone loss. Other factors associated with hip fracture risk in older individuals that we have described include: (1) increased circulating levels of advanced glycation end products (AGEs); (2) increased levels of trans fats in the diet; (3) cardiolipin subclinical vascular disease in the absence of clinical cardiovascular disease; and (4) reduced cardiac parasympathetic tone as derived from 24-hour Holter monitoring. All these factors are age-related and may help to explain the high mortality associated with hip fracture risk.
Keywords: albuminuria, fracture risk, osteoporosis, microvascular disease.
Introduction
The loss of bone density (osteoporosis) and the consequent increase in fracture risk are strongly related to aging. In women, the loss of estrogen production in the menopause also contributes to bone loss. Other factors associated with hip fracture risk in older individuals that we have described include: (1) increased circulating levels of advanced glycation end products (AGEs); (2) increased levels of trans fats in the diet²; (3) carotid artery subclinical vascular disease in the absence of clinical cardiovascular disease³; and (4) reduced cardiac parasympathetic tone as derived from 24-hour Holter monitoring⁴. All these factors are age-related and may help to explain the high mortality associated with hip fractures in the elderly.
In this review article, we highlight yet another risk factor that we have identified for hip fracture: albuminuria. Aside from this being a “novel” risk factor, knowledge of its effect on bone broadens our understanding of the association of vascular disease with fracture risk. It is well known that coronary artery disease, stroke and heart failure are related to hip fracture risk⁵˒⁶. What is not well appreciated is that microvascular disease – as represented by albuminuria – is also independently associated with hip fracture risk.
We divide this review into four sections:
-
A review of the osseous microcirculation and its association with bone loss.
-
Examination of albuminuria as a marker of extra-osseous microvascular dysfunction and its independent relationship with hip (and other osteoporotic) fracture risk.
-
A discussion of endothelial dysfunction which underlies albuminuria and microvascular disease.
-
Finally, a review of trabecular bone volume and markers of endothelial function as possible mechanisms explaining fracture risk in association with albuminuria.
I. Osseous Microcirculation and the Association of Disturbances of the Intra-Osseous Microcirculation with Bone Density
Bone is a highly vascularized tissue, receiving up to 10% of resting cardiac output²⁸. In long bones, blood enters through three routes: (1) a central nutrient artery; (2) metaphyseal–epiphyseal arteries near the ends of the bones; and (3) periosteal arteries. The entry of an artery into the bone, where it divides into smaller arterioles, is the beginning of the osseous microcirculation. These arterioles provide vascular resistance which controls blood flow to meet tissue needs. Once inside the bone, blood flows through a dense capillary network of Haversian (longitudinal) and Volkmann’s (transverse) canals, delivering nutrients, hormones, oxygen, and metabolic signals to bone tissue. Ultimately, blood egresses through periosteal, epiphyseal/metaphyseal, and central venous sinusoids, removing waste products.
The vascularization of flat bones resembles that of long bones but includes a large periosteal vascular network that provides the majority of perfusion.
Two clinical studies indicate that disturbances of the intraosseous microcirculation are associated with osteoporosis. A pathology study of femoral head fracture specimens revealed a reduction in the number of arterioles and arterial capillaries compared to femoral heads removed for arthritis¹⁰. In another study of 120 post-menopausal, healthy female subjects (mean age, 74 years; age range, 67–89 years), perfusion indices in the femoral head [maximum enhancement, defined as the maximum percentage increase in signal intensity from baseline], and enhancement slope [the rate of enhancement between 10% and 90% of the signal intensity difference between baseline and maximum signal intensity] were significantly lower in subjects with osteoporosis compared to subjects with osteopenia or normal bone mineral density¹¹. Together these studies show that disturbances in the number and function of the intraosseous circulation are associated
with osteoporosis. They do not indicate, however, if they are causally associated with osteoporosis or are epiphenomena of low bone density.
Rodent studies suggest a causal association of microvascular disease/dysfunction with bone loss. Nitric oxide knockout rodents, which exhibit reduced arterial and capillary vasomotor control, demonstrate decreased bone mineral density and cortical thickness¹². Another study found that a reduction in a specific bone marrow capillary subtype (type H micro-vessels) declined with age with subsequent bone loss¹³.
II. Albuminuria and Bone Health
In addition to disturbances of the intra-osseous microcirculation, abnormalities of the extra-osseous microcirculation are associated with bone disease and fractures. One such disorder is albuminuria — the excess excretion of protein in urine. This marker of extra-osseous microvascular disease is easily assessed in most clinical laboratories and is the focus of many cohort and population studies. It is associated with microvascular disorders elsewhere in the body. These include the brain¹⁴, lungs¹⁵˒¹⁶, skin¹⁷, eyes¹⁸˒¹⁹, and myocardium²⁰. Albuminuria is likely a manifestation of a systemic disorder affecting parts or the entirety of the microvascular system, making it a valid marker for assessing the association between extra-osseous microvascular disease and bone health and fracture risk.
In one of our early studies²¹, done in a cohort of 3110 elderly participants with albuminuria testing, there were 313 hip fractures during follow-up (7.7 % of men; 11.7 % of women). The incidence rate for men, with and without albuminuria, was 1.43 and 0.93/100 person-years of follow-up (p = 0.02); for women, 1.84 and 1.33 (p = 0.04) (FIGURE). After adjustment for osteoporosis-related factors, frailty and falling, a doubling of albuminuria was significantly associated with hip fracture risk in women (hazard ratio, 1.12, 95 % CI, 1.001-1.25).
In a large blood pressure study (n=28,602)²² participants with baseline albuminuria had a significantly increased risk of hip fracture compared with participants without albuminuria (unadjusted hazard ratio=1.62 [1.22, 2.15], P<0.001; adjusted hazard ratio=1.36 [1.01, 1.84], P=0.05). Participants with macroalbuminuria had a particularly high fracture risk (unadjusted hazard ratio=2.01 [1.21, 3.35], P=0.007; adjusted hazard ratio=1.71 [1.007, 2.91], P=0.05). In this cohort, estimated glomerular filtration rate was not a risk factor for hip fracture.
In a prospective cohort study of 352,624 Korean adults²³, the adjusted hazard ratios (HRs) for hip fracture were 1.30 (95% CI 1.02-1.65) for moderate albuminuria (albumin creatinine ratio [ACR] 30-299 mg/gram) and 1.58 (95% CI 1.07-2.35) for severe albuminuria (ACR >300) compared to no albuminuria (< 30 mg/gram ACR). This increased risk of hip fracture was independent of the estimated glomerular filtration rate and kidney function; that is, it was albuminuria, not kidney function, which was responsible for the increased fracture risk.
Finally, a study involving 2.7 million residents of Alberta, Canada²⁴, found that participants with albuminuria (ACR >300, had a significantly increased odds of hip fracture (adjusted odds ratio [OR] = 1.37; 95% confidence interval [CI] 1.28, 1.47), vertebral fracture (OR = 1.31; 95% CI 1.21, 1.41), and any-type fracture (OR = 1.22; 95% CI 1.17, 1.28) compared to individuals with no or mild albuminuria (ACR <300).
In support of the notion that albuminuria is a marker of a systemic disorder of the microvasculature, we reported that increasing amounts of abnormal white matter disease (AWMD) on brain MRI were associated with hip fracture risk. AWMD is a marker of cerebral small blood vessel disease²⁵. Adjustment for albuminuria attenuated the association of AWMD with hip fracture, suggesting that AWMD and albuminuria are part of the same microvascular disorder that is linked to bone disease. Diabetic retinopathy, another microvascular complication, is also associated with hip fracture risk²⁶˒²⁷.
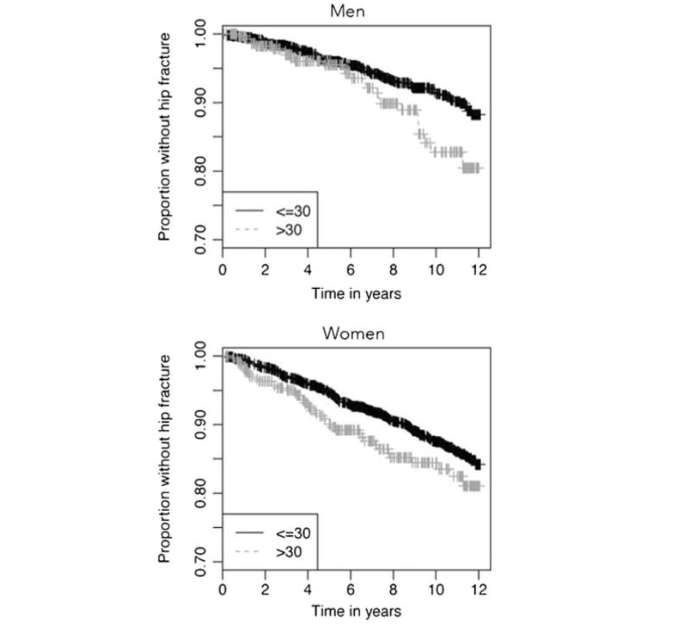
FIGURE: Kaplan-Meier plots for time without hip fracture categorized by the presence or absence of albuminuria (>30 mg / g creatinine) in men and women from the Cardiovascular Health Study. Reproduced with permission. Taken from Barzilay JI, Bůžková P, Chen Z, et al. Albuminuria is associated with hip fracture risk in older adults: the cardiovascular health study. Osteoporos Int. 2013;24(12):2993-3000. Reprinted with permission.
Albuminuria is commonly considered a complication of diabetes. However, in older individuals it is more often associated with hypertension, which is highly prevalent in the age group experiencing bone loss²⁸. Based on a cross-sectional analysis of the Third National Health and Nutrition Examination Survey (NHANES III) from the United States, albuminuria is present in 30% of adults over the age of 70 years and in 40% of similarly aged adults with diabetes²⁹. Thus, it is highly prevalent in the demographic group in which osteoporotic fractures occur.
III. Endothelial Dysfunction
Endothelial dysfunction (EndDys) underlies albuminuria. It is characterized by disturbances of vascular tone due to imbalanced release of endothelium-derived relaxing and contracting factors. EndDys also encompasses compromised endothelial cell functions that support an impermeable barrier between the circulation and the tissues it perfuses³⁰. Abnormally increased permeability, excessive coagulation, fibrinolysis, cell proliferation, and immune activation in the blood vessel wall characterize this aspect of EndDys.
cell proliferation, and immune activation in the blood vessel wall characterize this aspect of EndDys.
Studies of bone physiology support the role of EndDys as a mechanism for bone loss. There is a crosstalk between bone cells and endothelial cells. Bone cells release factors that modulate blood vessel function (e.g., endothelin and TGF-β), while blood vessels release factors that stimulate bone cellular activity (e.g., insulin-like growth factor-1, nitric oxide). The impairment of this symbiotic relationship disrupts the arterial microcirculation, which regulates vascular resistance to control tissue blood flow, which in turn regulates bone cellular activities (e.g., recruitment, proliferation, differentiation). A discussion of these interactions is beyond the scope of this paper. The reader is referred to two recent reviews on these subjects³¹˒³².
A clinical example of how EndDys is associated with bone loss comes from a study of coronary vascular reactivity. A cohort of 194 postmenopausal women over 50 years of age with non-obstructive coronary arteries was administered intracoronary acetylcholine during diagnostic angiography³³. Impaired reactivity was defined as a ≤50% increase in coronary blood flow from baseline. After a mean follow-up of 8.4±4.7 years, women with impaired response were more than twice as likely to report having osteoporosis compared to those without evidence of EndDys (relative risk, 2.4; 95% confidence interval [CI], 1.1, 5.6, P=0.02).
IV. Markers of Endothelial Dysfunction and Bone Density
Given that low bone mineral density and fracture risk are associated with intra- and extra-osseous microcirculatory disorders and EndDys, it is logical to deduce that metabolically active trabecular bone density — the site of vertebral and hip fractures — would be associated with microvascular disease. A study of ours does not support such a conclusion³⁴. Among 6,814 participants in the Multi-Ethnic Study of Atherosclerosis (MESA), we opportunistically derived volumetric thoracic vertebral trabecular bone mineral density (BMD) from computer tomography scans of the chest and heart. We measured urine albumin to creatinine ratios (UACR), retinal arteriolar and venular widths, flow-mediated dilation (FMD) of the brachial artery after 5 minutes of ischemia, and levels of five soluble endothelial adhesion markers (ICAM-1, VCAM-1, L-selectin, P-selectin, and E-selectin). Linear regression models were used to examine the association of trabecular BMD with the markers of microvascular disease and endothelial dysfunction. We found no significant associations between UACR, retinal arteriolar or venular widths, or FMD with BMD. Additionally, we observed no statistically significant association of spine trabecular BMD with levels of endothelial adhesion markers. Men and women exhibited similar results.
This finding can be interpreted in several ways. First, we could conclude that extra-osseous microvascular disease and EndDys are not associated with fracture because reduced trabecular BMD. In an analysis from the Cardiovascular Health Study, increased urine albumin levels were not associated with decreased total hip BMD in women, despite women having a high risk of hip fracture³⁵. In a Scandinavian study³⁶, DEXA-based BMD was also not associated with albuminuria, even though albuminuria was linked to fracture risk. Second, the markers of EndDys that we chose are not comprehensive and other markers may have a relationship with bone health. Last, markers of extra-osseous microvascular disease may be associated with loss of cortical bone density or decreased cortical bone quality. A study of diabetic individuals using high-resolution peripheral quantitative tomography (HR-pQCT) found that participants with diabetic microvascular disease (retinopathy, nephropathy, nerve disease) had lower cortical volumetric BMD in the radius and greater cortical porosity than participants without DM³⁷. There were no differences in trabecular bone density or quality. Such findings suggest—but do not prove—that extra-osseous microvascular disease may have a pronounced impact on the periosteal microvasculature which is related to cortical bone health.
V. Conclusions
What are the implications of these findings? We believe there are several lessons to be learned.
-
Both intra- and extra-osseous microcirculations are associated with the risk of hip fractures. How they interact with one another requires further investigation.
-
Extra-osseous microvascular disease, as represented by albuminuria, is independently associated with hip fracture risk. The risk is 20–50% higher compared to the absence of albuminuria. This risk is lower than that associated with macrovascular disease, e.g., coronary artery disease, which can be associated with a two to five-fold increased risk⁵. Nonetheless the ubiquity of microvascular disease makes population attributable risk for fracture high.
-
How extra-osseous microvascular disease leads to fracture risk requires further investigation, given that albuminuria and measures of endothelial dysfunction are not related to trabecular bone density. Future studies with newer technologies³⁸ will further delineate the role of the vascular system with bone health.
Last, it should be remembered that albuminuria reflects many disease processes, e.g., inflammation and endothelial dysfunction. These basic cellular disturbances likely lie at the root of the association of microvascular disease and fracture risk.
Declaration:
The authors do not have a financial or intellectual conflict of interest regarding the contents of this paper.
References:
References
1. Barzilay JI, Bůžková P, Zieman SJ, Kizer JR, Djoussé L, Ix JH, Tracy RP, Siscovick DS, Cauley JA, Mukamal KJ. Circulating levels of carboxy-methyl-lysine (CML) are associated with hip fracture risk: The Cardiovascular Health Study. J Bone Miner Res 2014; 29: 1061-1066. doi: 10.1002/jbmr.2123
2. Barzilay JI, Buzkova P, Djoussé L, Ix J Kizer J, Cauley J, Matthan N, Lichtenstein AH, Mukamal KJ. Serum Non-Esterified Fatty Acid Levels and Hip Fracture Risk in Older Adults: The Cardiovascular Health Study. Osteoporos Int 2021; 32(9):1745-1751. doi: 10.1007/s00198-021-05897-4
3. Barzilay J, Buzkova P, Cauley JA, Robbins JA, Fink HA, Mukamal KJ. The associations of subclinical atherosclerotic cardiovascular disease with hip fracture risk and bone mineral density in elderly adults; the Cardiovascular Health Study. Osteoporos Int 2018; 29(10): 2219-2230. doi: 10.100 7/s00198-018-4611-9
4. Stein PK, Buzkova P, Fink HA, Robbins JA, Mukamal KJ, Cauley JA, Carbone L, Elam R, McMillan DW, Valderrabano R, Barzilay JI. Cardiovascular Autonomic Nervous System Function and Hip Fracture Risk: The Cardiovascular Health Study. Arch Osteoporos 2021 Oct 31; 16(1):163. doi: 10.1007/s1 1657-021-01028-y
5. Robbins JA, Buzkova P, Barzilay JI, Cauley JA, Fink HA, Carbone LD, Chen Z, Stein PK, Elam R, Sheets K, Mukamal KJ. Mortality following hip fracture in older adults with and without coronary heart disease: The Cardiovascular Health Study Am J Med 2023: 136 (8): 789-795. doi: 10.1016/j.amjm ed.2023.03.036
6. Carbone L, Buzkova P, Fink HA, Lee JS, Chen Z, Ahmed A, Parashar S, Robbins JA. Hip fractures and heart failure: findings from the Cardiovascular Health Study. Eur Heart J 2010; 3 (1): 77-84. doi.org/10.1093/eurheartj/ehp345
7. Gross PM, Heistad DD, Marcus ML. Neurohumoral regulation of blood flow to bones and marrow. Am J Physiol. 1979;237:H440–H448. doi: 10.1152/ajpheart.1979.237.4.H440.
8. McCarthy I. The physiology of bone blood flow: a review. Bone Joint Surg Am 2006; 88 Suppl 3: 4-9. doi: 10.2106/JBJS.F.00890.
9. Prisby RD. Bone marrow microvasculature. Compr Physiol 2020; 10 (3): 1009- 1046. doi: 10.100 2/cphy.c190009.
10. Laroche M, Ludot I, Thiechart M. Study of the intraosseous vessels of the femoral head in patients with fractures of the femoral neck or osteoarthritis of the hip. Osteoporos Int 1995; 5: 213-217. doi: 10.1007/BF01774009
11. Griffith JF, Yeung DKW, Tsang PH. Compromised bone marrow perfusion in osteoporosis. J Bone Miner Res. 2008; 23(7): 1068-75. doi: 10.1359/jbmr.080233.
12. Aguirre J, Buttery L, O’Shaughnessy M, et al. Endothelial nitric oxide synthase gene-deficient mice demonstrate marked retardation in postnatal bone formation, reduced bone volume, and defects in osteoblast maturation and activity. Am J Pathol. 2001;158(1):247-57. doi: 10.1016/S0002-9440(10)63963-6.
13. Ramasamy SK, Kusumbe AP, Schiller M, et al. Blood flow controls bone vascular function and osteogenesis Nat Commun. 2016 Dec 6:7:13601. doi: 10.1038/ncomms13601.
14. Sheets KM, Buzkova P, Chen Z, et al. Association of covert brain infarcts and white matter hyperintensities with risk of hip fracture in older adults: the Cardiovascular Health Study. Osteoporos Int. 2023;34(1):91-99. doi: 10.1007/s0 0198-022-06565-x
15. Pallister I, Gosling P, Alpar K, Bradley S. Prediction of posttraumatic adult respiratory distress syndrome by albumin excretion rate eight hours after admission. J Trauma. 1997;42(6):1056-61. doi: 10.1097/00005373-199706000-00012.
16. Kopf S, Groener JB, Kender Z, et al. Breathlessness and Restrictive Lung Disease: An Important Diabetes-Related Feature in Patients with Type 2 Diabetes. Respiration. 2018;96(1):29-40. doi: 10.1159/000488909.
17. Steegh FMEG, Keijbeck AA, de Hoogt PA, et al. Capillary rarefaction: a missing link in renal and cardiovascular disease? Angiogenesis. 2024; 27(1):23-35. doi: 10.1007/s10456-023-09883-8.
18. Martens RJH, Houben AJHM, Kooman JP, et al. Microvascular endothelial dysfunction is associated with albuminuria: the Maastricht Study. J Hypertens. 2018;36(5):1178-1187. doi: 10.1097/H JH.0000000000001674
19. Li J, Zhang W, Zhao L, et al. Positive correlation between hypertensive retinopathy and albuminuria in hypertensive adults. BMC Ophthalmol. 2023;23 (1):66. doi: 10.1186/s12886-023-02807-6.
20. von Scholten BJ, Hasbak P, Christensen TE. Cardiac (82)Rb PET/CT for fast and non-invasive assessment of microvascular function and structure in asymptomatic patients with type 2 diabetes. Diabetologia 2016; 59(2):371-8. doi: 10.1007/s00125-015-3799-x.
21. Barzilay JI, Bůžková,P, Chen Z, et al. Albuminuria is associated with hip fracture risk in older adults: the cardiovascular health study. Osteoporos Int. 2013;24(12):2993-3000. doi: 10.100 7/s00198-013-2389-3.
22. Barzilay JI, Gao P, Clase CM, et al. Albuminuria and rapid loss of GFR and risk of new hip and pelvic fractures. Clin J Am Soc Nephrol. 2013;8(2):233-240. doi: 10.2215/CJN.06640712
23. Kim SH, Yi SW, Yi JJ, Kim YM, Won YJ. Chronic Kidney Disease Increases the Risk of Hip Fracture: A Prospective Cohort Study in Korean Adults. J Bone Miner Res. 2020;35(7):1313-1321. doi: 10.1002/jbmr.3997.
24. Cooke-Hubley SM, Senior P, Bello AK, Wiebe N, Klarenbach S. Degree of Albuminuria is Associated with Increased Risk of Fragility Fractures Independent of Estimated GFR. Kidney Int Rep. 2023;8(11):2315-2325. doi: 10.1016/j.ekir.2023.08.016.
25. Bůžková P, Barzilay JI, Fink HA, Robbins JA, Cauley JA, Fitzpatrick AL. Ratio of urine albumin to creatinine attenuates the association of dementia with hip fracture risk. J Clin Endocrinol Metab. 2014;99(11):4116-4123. doi: 10.1210/jc.2014-2409.
26. Johannesdottir F, Tedtsen T, Cooke LM, et al. Microvascular disease and early diabetes onset are associated with deficits in femoral neck bone density and structure among older adults with longstanding type 1 diabetes. J Bone Miner Res. 2024 Sep 26;39(10):1454-1463. doi: 10.1093/jbm r/zjae134.
27. Goldshtein I, Nguyen AM, dePapp AE, et al. Epidemiology and correlates of osteoporotic fractures among type 2 diabetic patients. Arch Osteopor 2018 Mar 3; 13 (1): 15. Doi: 10.1007/116 57-018-0432-x.
28. Barzilay JI, Peterson D, Cushman M, et al. The relationship of cardiovascular risk factors to microalbuminuria in older adults with or without diabetes mellitus or hypertension: The Cardiovascular Health Study. Am J Kid Dis 2004; 44: 25 – 34. doi: 10.1053/j.ajkd.2004.03.022.
29. Garg AX, Kiberd BA, Clark WF, Haynes RB, Clase CM. Albuminuria and renal insufficiency prevalence guides population screening: results from the NHANES III. Kidney Int. 2002; 61(6):2165-75. doi: 10.1046/j.1523-1755.2002.00356.x.
30. Gimbrone MA Jr, García-Cardeña G (2016) Endothelial cell dysfunction and the pathobiology of atherosclerosis. Circ Res 2016: 118(4):620–636. doi.org/10.1161/CIRCRESAHA.115.306301
31. Prisby RD. Mechanical, hormonal and metabolic influences on blood vessels, blood flow and bone. J Endocrinol. 2017;235(3): R77-R100. doi: 10.1530/JOE-16-0666.
32. Watson EC, Adams RH. Biology of bone: the vasculature of the skeletal system. Cold Spring Harb Perspect Med. 2018; 8(7):a031559. doi: 10.110 1/cshperspect.a031559.
33. Prasad M, Reriani M, Khosla S, et al. Coronary microvascular endothelial dysfunction is an independent predictor of development of osteoporosis in postmenopausal women. Vasc Health Risk Manag 2014:10:533-8. doi: 10.2147/VH RM.S63580. eCollection 2014.
34. Barzilay JI, Buzkova P, Bielinski SJ, et al. The association of microvascular disease and endothelial dysfunction with vertebral trabecular bone mineral density: The MESA study. Osteoporos Int. 2024;35 (9):1595-1604. doi: 10.1007/s00198-024-07152-y.
35. Barzilay JI, Buzkova P, Fink HA, et al. Systemic markers of microvascular disease and bone mineral density older in adults: The cardiovascular health study. Osteoporos Int. 2016;27(11):3217-3225. doi: 10.1007/s00198-016-3649-9.
36. Jørgensen L, Jenssen T, Ahmed L, Bjornerem A, Joakimsen R, Jacobsen BK. Albuminuria and risk of nonvertebral fractures. Arch Intern Med. 2007; 167:1379–1385. doi: 10.1001/archinte.167.13.1379.
37. Shanbhogue VV, Hansen S, Frost M, et al. Compromised cortical bone compartment in type 2 diabetes mellitus patients with microvascular disease. Eur J Endocrinol. 2016; 174(2):115-24. doi: 10.1530/EJE-15-0860.
38. Samelson EJ, Broe KE, Xu H, et al. Cortical and trabecular bone microarchitecture as an independent predictor of incident fracture risk in older women and men in the Bone Microarchitecture International Consortium (BoMIC): a prospective study. Lancet Diabetes Endocrinol. 2019;7(1):34-43. doi: 10.1016/S2213-8587(18)30308-5