






Alcoholic Cardiomyopathy: Risks, Effects, and Treatments
Alcoholic Cardiomyopathy: Drinking to Excess
Patrick May1, Vincent M. Figueredo2
- Department of Medicine, St. Mary Medical Center, Langhorne, PA 19047, USA
- Department of Cardiology, St. Mary Medical Center, Langhorne, PA, 19047, USA
OPEN ACCESS
PUBLISHED: 30 September 2024
CITATION: May, P., and Figueredo, VM., 2024. Alcoholic Cardiomyopathy: Drinking to Excess. Medical Research Archives, [online] 12(9). https://doi.org/10.18103/mra.v12i9.5757
COPYRIGHT: © 2024 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v12i9.5757
ISSN 2375-1924
ABSTRACT
Alcohol is a commonly consumed and enjoyed commodity within the global population today. Despite a purported reduction in coronary artery disease with moderate alcohol use, chronic excessive alcohol consumption can lead to deleterious health effects. While mainly associated with liver disease, injury, and mental health, it can also have devastating effects on the cardiovascular system, such as heart failure, sudden cardiac death, and stroke. More than 280 million people worldwide are currently diagnosed with alcohol use disorder. Alcohol and its metabolites exert both direct and indirect toxic effects on myocardial tissues and can lead to myocardial cell damage, apoptosis, fibrosis, and progressive myocardial dysfunction, specifically dilated cardiomyopathy. We present the current epidemiology and incidence, outline the major toxic effects of alcohol and why they occur, discuss the current guideline-directed treatment strategies, and propose targets for possible therapies in the future based on pathophysiology.
Keywords
Dilated cardiomyopathy, alcohol use disorder, heart failure, ethanol
Introduction
Heart disease caused by alcohol is by no means a new phenomenon. It has been previously described and studied for more than a century. It was first mentioned as “alcoholic heart disease” in 1902 by William Mackenzie in his work Study of the Pulse. Even before that term was used, Otto Bollinger, a German pathologist, described “Munich Beer Heart” in 1884. He discovered that findings of dilated cardiomyopathy on autopsy were far greater in the population of Munich as compared to Berlin. At the time, Munich was known to have a higher alcohol consumption rate than other German cities, which led Bollinger to make this connection between increased average alcohol intake and the prevalence of dilated cardiomyopathy.
Alcohol is commonly consumed within the global population today. Despite the Framingham Heart Study suggesting a reduction in coronary artery disease events with moderate alcohol use, chronic excessive alcohol consumption can lead to deleterious health effects such as heart failure. Heart failure is most often caused by ischemic heart disease and hypertension. However, there are various diseases, insults, or toxins that can lead to heart disease and failure, labeled non-ischemic cardiomyopathies. Alcoholic cardiomyopathy (ACM) is a form of dilated cardiomyopathy caused by chronic and excessive alcohol consumption. In the 2021 American College of Cardiology (ACC)/American Heart Association (AHA) Guidelines, alcohol consumption was noted as a significant risk factor for the development of heart failure.
Today, ACM is recognized as one of the most common causes of non-ischemic dilated cardiomyopathy (DCM). While the most obvious treatment is abstinence first, medical therapies are being explored to reduce the morbidity and mortality associated with ACM. We discuss the epidemiology, pathophysiology, clinical features, and current management of ACM. Potential new therapies, based on the cellular pathophysiology of alcohol and its metabolites, are discussed.
Epidemiology
As of 2016, it was estimated that 2.3 billion persons were current drinkers, and 283 million persons worldwide age 15 or older had an alcohol use disorder. ACM represents a significant public health concern due to its association with high morbidity and mortality rates. It is the leading cause of non-ischemic dilated cardiomyopathy. According to the Center for Disease Control’s (CDC) Alcohol-Related Disease Impact (ARDI) tool, the total annual attributable deaths due to excessive alcohol use in the United States (as of 2020-2021) was 178,307 with the ratio of men to women slightly greater than 2:1. Additionally, the total annual attributable deaths to alcoholic cardiomyopathy in the United States was 665 with the ratio of men to women greater than 5:1. A study of 490,000 patients demonstrated increased all-cause mortality in those who were heavy drinkers under the age of 60. Even acute alcohol ingestion was shown to depress the preload, afterload, and systemic vascular resistance in healthy young adults. Heavy alcohol consumption (greater than 80g daily) for greater than 5 years places a person at risk for developing ACM.
The incidence of ACM in heavy alcohol drinkers is 1-2%. However, since there are so many heavy drinkers, ACM is one of the leading causes of non-ischemic dilated cardiomyopathy, given that 21-36% of all cases are attributed to heavy alcohol use. One study demonstrated that in patients with dilated DCM, there was a 40% prevalence of patients who drank more alcohol than the weekly recommendations as compared to non-DCM patients for whom prevalence was 24%. One large study (n > 49,000) demonstrated that patients who consumed greater than 60 g/day of alcohol had increased relative wall thickness, impaired left ventricular (LV) diastolic function, and the highest odds ratio for LV hypertrophy as compared to those who consumed less alcohol. An analysis of 83 prospective studies found that patients with alcohol consumption of greater than 100g per week were at higher risk of heart failure and had a higher all-cause mortality. Two additional studies both found that for patients with the same amount of alcohol intake, those who had been drinking longer were demonstrating more heart failure symptoms.
Pathophysiology
Acute large-volume consumption of alcohol can increase myocardial inflammation and can lead to cardiac arrhythmias and troponin elevation. Lang et al. demonstrated that in young, healthy adults, acute alcohol ingestion affected the cardiovascular system by decreasing systemic vascular resistance, afterload, and preload.
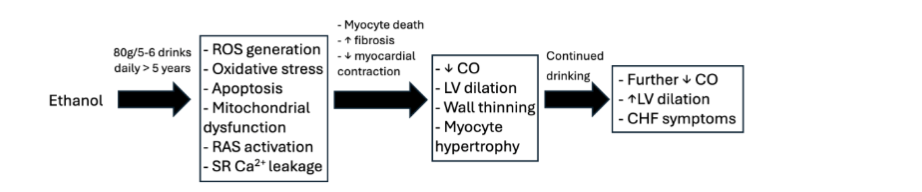
Chronic alcohol consumption exerts direct and indirect toxic effects on cardiac myocytes, leading to cellular damage and myocardial dysfunction. As delineated in Figure 1, mitochondrial dysfunction, oxidative stress from reactive oxygen species (ROS), renin-angiotensin system (RAS) activation, and increased apoptosis are pathophysiologic mechanisms contributing to the development of ACM.
Mitochondrial structure and function are both affected by alcohol and its metabolites. Structurally, alcohol can cause the degeneration of inner mitochondrial membrane folds and reduce the number of mitochondria present in the cardiac myocytes. Secondary to this structural alteration, the function of the mitochondria is hindered. One study showed that when rat cardiomyocytes were cultured with alcohol, the mitochondria were affected by having increased mitochondrial depolarization and decreased membrane potential. It has also been shown that alcohol contributes to the dysfunction of the electron transport chain (ETC) through the uncoupling of oxidative phosphorylation and decreases the activity of multiple enzymes within the tricarboxylic acid cycle.
Another mechanism of alcohol-induced myocardial damage is the generation of reactive oxygen species (ROS) which causes oxidative stress and can affect cardiac myocytes by inducing apoptosis and subsequent fibrosis. In male mice, after at least 6 weeks of alcohol feeding, superoxide production was increased, which represents an increase in ROS secondary to alcohol administration. Additionally, superoxide dismutase (SOD), an enzyme that degrades ROS, was shown to be decreased after longer durations of alcohol exposure in mice and rat populations. These effects were manifested as an over-expression of pro-apoptotic proteins Bax and caspase-3, cytosolic TUNEL-stained nuclei, and increased apoptotic bodies in heart cells from humans. By inhibiting the enzyme CYP2E1, which converts alcohol to acetaldehyde, these effects mentioned above were increased. In one study, alcohol was shown to increase p21 RNA and therefore p21 protein, which is part of the hypertrophic response. Another study demonstrated that ethanol could be promoting fibrosis secondary to decreased polarization of Th1 (T helper 1) cells and increased response of Th2 (T helper 2) cells.
Ethanol can also cause calcium to leak from the sarcoplasmic reticulum of cardiomyocytes, resulting in negative inotropy and arrhythmogenesis. This occurs by ROS causing oxidative activation of calmodulin-dependent protein kinase II (CaMKII). Additionally, alcohol was shown to activate the RAS and it was subsequently shown that an angiotensin receptor blocker could prevent the development of ACM when studied in dogs. NOX2 was identified as one of the main mediators of ROS generation by alcohol and its toxic metabolite acetaldehyde.
Clinical Features
No specific signs or symptoms distinguish ACM from other forms of dilated cardiomyopathy. The clinical features are the same as those of other diseases that lead to progressive heart dysfunction. These symptoms include dyspnea on exertion, orthopnea, paroxysmal nocturnal dyspnea, peripheral edema, third heart sound, elevated jugular venous distension, cardiomegaly, pulmonary edema, and rales. Patients may initially be asymptomatic as the depression of their cardiac function may be minimal at first, but they develop increasing manifestations as their myocardial function is further depressed.
Other serious ramifications of ACM are supraventricular tachycardias (SVTs), ventricular tachycardias (VTs), and sudden cardiac death (SCD). Atrial fibrillation is also an important comorbidity. SVTs are more closely associated with younger patients and binge alcohol use. VTs are more strongly linked to chronic alcohol use. The apoptosis and subsequent fibrosis of cardiomyocytes predisposes the patient to these arrhythmias. The risk of SCD and VT was shown to be decreased in those patients who permanently abstained from alcohol. One large study (n = 107,845) demonstrated that even drinking one standard alcoholic drink daily compared to abstinence can increase the patient’s risk of acquiring atrial fibrillation by 16%.
Diagnosis
Patients with ACM may be asymptomatic or present with the clinical features listed above. If heart failure secondary to dilated cardiomyopathy is diagnosed on imaging evidenced by biventricular dysfunction and dilatation, ACM should be on the list of potential causes. ACM remains a diagnosis of exclusion since the only distinguishing factor between ACM and idiopathic DCM is the history of significant chronic alcohol consumption in the absence of other causes. Thus, a detailed, thorough history is indispensable in the diagnosis of ACM. When taking this history, the provider must be sure to ask about other substances so as not to omit inquiring about other potential toxins, such as doxorubicin and cocaine, that could be contributing to the patient’s myocardial damage and dysfunction. Additionally, an important step in the diagnostic process of ACM is the exclusion of ischemic heart disease as a cause. Cirrhosis may complicate the diagnostic process since the process of cirrhosis could be secondary to alcohol, but the pathologic consequences of cirrhosis-induced portal hypertension can also impact the function of the heart and induce right-sided heart failure.
Management and Future Considerations
Once a patient is diagnosed with ACM, multiple issues need to be addressed. First and foremost, continued alcohol use must be addressed, and complete abstinence must be recommended. Haissaguerre et al. demonstrated that complete abstinence from ethanol had a statistically significant positive effect on prognosis in dilated cardiomyopathies. Fauchier et al. demonstrated that failure to maintain abstinence in ACM was a strong predictor of cardiac death. The mortality rate of ACM without abstinence is 40-50% at 3-6 years. According to the ACC/AHA, there is a recommendation for abstinence in ACM with a Level of Evidence C.
To help maintain abstinence there are a few options to help treat alcohol use disorder and help patients refrain from using alcohol. Cognitive behavioral therapy, naltrexone, acamprosate, and disulfiram are different options for aiding the patient with ACM to ensure abstinence from alcohol. Disulfiram is contraindicated in those with symptomatic heart failure secondary to the risk of an alcohol-disulfiram reaction which may lead to cardiovascular collapse and can be catastrophic in a patient with heart failure.
As per the 2022 ACC/AHA/HFSA Guideline for Management of Heart Failure, patients with heart failure with reduced ejection fraction (HFrEF) should be treated with the following medications:
- Angiotensin Receptor Blocker- Neprilysin inhibitor (ARNi), Angiotensin-Converting Enzyme inhibitor (ACEi), or Angiotensin Receptor Blocker (ARB)
- Beta Blockers (e.g. carvedilol, bisoprolol, or metoprolol succinate)
- Mineralocorticoid Receptor Antagonists (e.g. spironolactone or eplerenone)
- Sodium-Glucose Cotransporter 2 inhibitors (SGLT2i) (e.g. dapagliflozin or empagliflozin)
There is a Class I recommendation for patients with ischemic or non-ischemic HFrEF and a left ventricular ejection fraction (LVEF) less than 35%, who have an estimated lifespan greater than 1 year, to undergo implantation of an ICD to reduce mortality through the primary prevention of SCD. In the same patient population with symptomatic heart failure, if they are in sinus rhythm with left bundle branch block, and QRS duration > 150 ms, there is a Class I recommendation for Cardiac Resynchronization Therapy (CRT).
Additionally, patients who suffer from chronic alcoholism are predisposed to develop malnutrition and vitamin deficiency, so it is recommended to supplement these patients with thiamine and folate to prevent adverse outcomes.
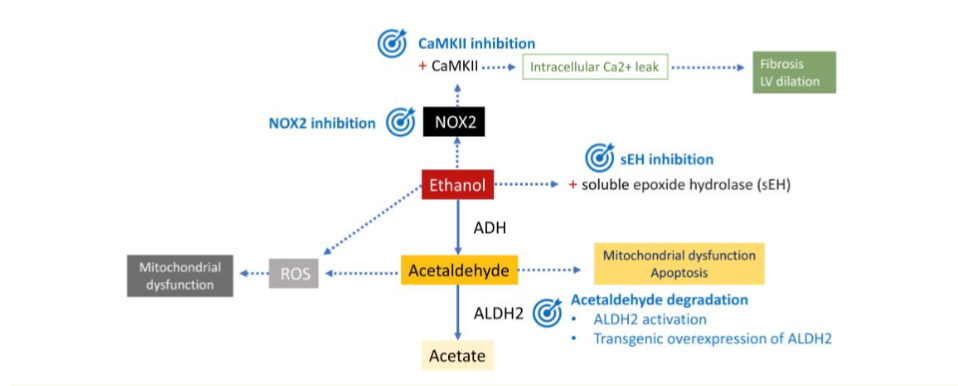
Based on pathophysiology, there are a few possible targets for future therapies in the treatment and/or prevention of ACM. For example, studies showed that extract from the Thespesia populnea plant, selenium, vitamin E, and sodium hydrosulfide all reduced the burden of ROS that was activated by ethanol and its metabolites; by affecting the activity of superoxide dismutase (SOD). This information could lead to the ability to blunt the harmful effect of alcohol-induced ROS. Additionally, aldehyde dehydrogenase 2 (ALDH2) helps to degrade the metabolite of ethanol, acetaldehyde, which on its own contributes to cardiomyocyte apoptosis. This could be another important target in the future to modulate the ability to clear toxic metabolites from ethanol ingestion. One more target that has been studied is the enzyme NOX2, which is a major part of the generation of ROS in the form of superoxide. When NOX2 was inhibited, there was a reduction in the amount of superoxide created by ethanol and acetaldehyde. This could also be a worthy target of further investigation to develop a potentially protective therapy against alcohol-mediated cell damage.
Conclusion
Alcoholic cardiomyopathy is a serious condition resulting from chronic excessive alcohol consumption. Understanding its pathophysiology, clinical features, and management strategies is essential for improving patient outcomes. Emphasis on early diagnosis, strict alcohol abstinence, and appropriate medical therapy can significantly alter the disease course and enhance the quality of life for affected individuals. Further research is needed to explore novel therapeutic targets and improve specific protective measures for this condition.
Disclosures
None
References:
- Mackenzie W. The study of the pulse, arterial, venous, and hepatic, and of the movements of the heart. Am J Med Sci. 1902;37(7):287
- Bollinger O. Ueber die haufigkeit und ursachen der idiopathischen herzhypertrophie in munchen. Deutsch Med Wchnschr. 1884:180e1.
- Walsh CR, Larson MG, Evans JC, et al. Alcohol consumption and risk for congestive heart failure in the Framingham Heart Study. Ann Intern Med. 2002;136(3):181-191. doi:10.7326/0003-4819-136-3-200202050-00005
- Kannel WB. Incidence and epidemiology of heart failure. Heart Fail Rev. 2000;5(2):167–173. doi: 10.1023/A:1009884820941.
- McKenna CJ, Codd MB, McCann HA, Sugrue DD. Alcohol consumption and idiopathic dilated cardiomyopathy: A case control study. Am Heart J. 1998;135(5 Pt 1):833–837. doi: 10.1016/s0002-8703(98)70042-0.
- Bozkurt B, Hershberger RE, Butler J, et al. 2021 ACC/AHA Key Data Elements and Definitions for Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Data Standards (Writing Committee to Develop Clinical Data Standards for Heart Failure). J Am Coll Cardiol. 2021;77(16):2053-2150. doi:10.1016/j.jacc.2020.11.012
- Glantz MD, Bharat C, Degenhardt L, et al. The epidemiology of alcohol use disorders cross-nationally: Findings from the world mental health surveys. Addict Behav. 2020;102:106128. doi: 10.1016/j.addbeh.2019.106128.
- Piano MR. Alcoholic cardiomyopathy: Incidence, clinical characteristics, and pathophysiology. Chest. 2002;121(5):1638–1650. doi: 10.1378/chest.121.5.1638.
- Center for disease control and prevention: Alcohol-related disease impact (ARDI) application. https://nccd.cdc.gov/DPH_ARDI/default/default.aspx. Updated 2024. Accessed 8, 2024.
- Thun MJ, Peto R, Lopez AD, et al. Alcohol consumption and mortality among middle-aged and elderly U.S. adults. N Engl J Med. 1997;337(24):1705-1714. doi:10.1056/NEJM199712113372401
- Lang RM, Borow KM, Neumann A, Feldman T. Adverse cardiac effects of acute alcohol ingestion in young adults. Ann Intern Med. 1985;102(6):742–747. doi: 10.7326/0003-4819-102-6-742.
- Regan TJ. Alcohol and the cardiovascular system. JAMA. 1990;264(3):377-381. doi:10.1001/jama.1990.03450030101041
- Park SK, Moon K, Ryoo JH, et al. The association between alcohol consumption and left ventricular diastolic function and geometry change in general Korean population. Eur Heart J Cardiovasc Imaging. 2018;19(3):271-278. doi:10.1093/ehjci/jex091
- Wood AM, Kaptoge S, Butterworth AS, et al. Risk thresholds for alcohol consumption: combined analysis of individual-participant data for 599 912 current drinkers in 83 prospective studies [published correction appears in Lancet. 2018 Jun 2;391(10136):2212. doi: 10.1016/S0140-6736(18)31168-1]. Lancet. 2018;391(10129):1513-1523. doi:10.1016/S0140-6736(18)30134-X
- Mathews EC Jr, Gardin JM, Henry WL, et al. Echocardiographic abnormalities in chronic alcoholics with and without overt congestive heart failure. Am J Cardiol. 1981;47(3):570-578. doi:10.1016/0002-9149(81)90540-3
- Urbano-Marquez A, Estruch R, Navarro-Lopez F, Grau JM, Mont L, Rubin E. The effects of alcoholism on skeletal and cardiac muscle. N Engl J Med. 1989;320(7):409-415. doi:10.1056/NEJM198902163200701
- Steiner JL, Lang CH. Etiology of alcoholic cardiomyopathy: Mitochondria, oxidative stress and apoptosis. The International Journal of Biochemistry & Cell Biology. 2018;89:125. doi: 10.1016/j.biocel.2017.06.009.
- Domínguez F, Adler E, García-Pavía P. Alcoholic cardiomyopathy: An update. European Heart Journal. 2024;45(26):2294. doi: 10.1093/eurheartj/ehae362.
- Laurent D, Mathew JE, Mitry M, Taft M, Force A, Edwards JG. Chronic ethanol consumption increases myocardial mitochondrial DNA mutations: a potential contribution by mitochondrial topoisomerases. Alcohol Alcohol. 2014;49(4):381-389. doi:10.1093/alcalc/agu029
- Piano MR, Phillips SA. Alcoholic cardiomyopathy: pathophysiologic insights. Cardiovasc Toxicol. 2014; 14(4):291–308. doi: 10.1007/s12012-014-9252-4
- Rajbanshi SL, Pandanaboina CS. Alcohol stress on cardiac tissue – ameliorative effects of Thespesia populnea leaf extract. J Cardiol. 2014; 63(6):449–59. doi: 10.1016/j.jjcc.2013.10.015
- Yao Z, Zhang Y, Li H, Deng Z, Zhang X. Synergistic effect of Se-methylselenocysteine and vitamin E in ameliorating the acute ethanol-induced oxidative damage in rat. J Trace Elem Med Biol. 2015; 29:182–7. doi: 10.1016/j.jtemb.2014.08.004
- Zhou X, Lu X, Xu W, Chen J. Protective effects of hydrogen sulfide against chronic alcohol intake-induced left ventricular remodeling in rats. Cardiovasc Drugs Ther. 2013;27(3):221-227. doi:10.1007/s10557-013-6441-5
- Chen DB, Wang L, Wang PH. Insulin-like growth factor I retards apoptotic signaling induced by ethanol in cardiomyocytes. Life Sci. 2000;67(14):1683-1693. doi:10.1016/s0024-3205(00)00759-1
- Zhang RH, Gao JY, Guo HT, et al. Inhibition of CYP2E1 attenuates chronic alcohol intake-induced myocardial contractile dysfunction and apoptosis [published correction appears in Biochim Biophys Acta. 2014 Dec;1842(12):2528]. Biochim Biophys Acta. 2013;1832(1):128-141. doi:10.1016/j.bbadis.2012.08.014
- Fernández-Solà J, Lluis M, Sacanella E, Estruch R, Antúnez E, Urbano-Márquez A. Increased myostatin activity and decreased myocyte proliferation in chronic alcoholic cardiomyopathy. Alcohol Clin Exp Res. 2011;35(7):1220-1229. doi:10.1111/j.1530-0277.2011.01456.x
- Guo R, Ren J. Alcohol dehydrogenase accentuates ethanol-induced myocardial dysfunction and mitochondrial damage in mice: role of mitochondrial death pathway. PLoS One. 2010;5(1):e8757. Published 2010 Jan 18. doi:10.1371/journal.pone.0008757
- Zhang B, Turdi S, Li Q, Lopez FL, Eason AR, Anversa P, et al. Cardiac overexpression of insulin-like growth factor 1 attenuates chronic alcohol intake-induced myocardial contractile dysfunction but not hypertrophy: Roles of Akt, mTOR, GSK3beta, and PTEN. Free Radic Biol Med. 2010; 49(7):1238–53. doi: 10.1016/j.freeradbiomed.2010.07.020
- Jänkälä H, Eklund KK, Kokkonen JO, et al. Ethanol infusion increases ANP and p21 gene expression in isolated perfused rat heart. Biochem Biophys Res Commun. 2001;281(2):328-333. doi:10.1006/bbrc.2001.4343
- Liu W, Li J, Tian W, Xu T, Zhang Z. Chronic alcohol consumption induces cardiac remodeling in mice from Th1 or Th2 background. Exp Mol Pathol. 2011;91(3):761-767. doi:10.1016/j.yexmp.2011.08.003
- Mustroph J, Wagemann O, Lebek S, et al. SR Ca2+-leak and disordered excitation-contraction coupling as the basis for arrhythmogenic and negative inotropic effects of acute ethanol exposure. J Mol Cell Cardiol. 2018;116:81-90. doi:10.1016/j.yjmcc.2018.02.002
- Wang S, Ren J. Role of autophagy and regulatory mechanisms in alcoholic cardiomyopathy. Biochim Biophys Acta Mol Basis Dis. 2018;1864(6 Pt A):2003-2009. doi:10.1016/j.bbadis.2018.03.016
- Cheng CP, Cheng HJ, Cunningham C, et al. Angiotensin II type 1 receptor blockade prevents alcoholic cardiomyopathy. Circulation. 2006;114(3):226-236. doi:10.1161/CIRCULATIONAHA.105.596494
- Brandt, M., Garlapati, V., Oelze, M. et al. NOX2 amplifies acetaldehyde-mediated cardiomyocyte mitochondrial dysfunction in alcoholic cardiomyopathy. Sci Rep 6, 32554 (2016). doi: 10.1038/srep32554.
- Guzzo-Merello G, Cobo-Marcos M, Gallego-Delgado M, Garcia-Pavia P. Alcoholic cardiomyopathy. World J Cardiol. 2014;6(8):771-781. doi:10.4330/wjc.v6.i8.771
- George A, Figueredo VM. Alcoholic cardiomyopathy: A review. Journal of Cardiac Failure. 2011;17(10):844. doi: 10.1016/j.cardfail.2011.05.008.
- Guzzo-Merello G, Segovia J, Dominguez F, et al. Natural history and prognostic factors in alcoholic cardiomyopathy. JACC Heart Fail. 2015;3(1):78-86. doi:10.1016/j.jchf.2014.07.014
- George A, Figueredo VM. Alcohol and arrhythmias: a comprehensive review. J Cardiovasc Med (Hagerstown). 2010;11(4):221-228. doi:10.2459/JCM.0b013e328334b42d
- Fauchier L. Alcoholic cardiomyopathy and ventricular arrhythmias. CHEST. 2003(123):1320. doi: 10.1378/chest.123.4.1320.
- Csengeri D, Sprünker N, Di Castelnuovo A, et al. Alcohol consumption, cardiac biomarkers, and risk of atrial fibrillation and adverse outcomes. Eur Heart J. 2021;42(12):1170–1177. Accessed 8/22/2024. doi: 10.1093/eurheartj/ehaa953.
- Bozkurt B, Colvin M, Cook J, et al. Current diagnostic and treatment strategies for specific dilated cardiomyopathies: A scientific statement from the american heart association. Circulation. 2024;134(23). doi: 10.1161/cir.0000000000000455.
- Haissaguerre M, Fleury B, Gueguen A, et al. Mortality of dilated myocardiopathies as a function of continuation of alcohol drinking. multivariate analysis concerning 236 patients. Presse Med. 1989;18(14):711–714.
- Fauchier L, Babuty D, Poret P, et al. Comparison of long-term outcome of alcoholic and idiopathic dilated cardiomyopathy. Eur Heart J. 2000;21(4):306-314. doi:10.1053/euhj.1999.1761
- Carroll KM, Kiluk BD. Cognitive behavioral interventions for alcohol and drug use disorders: Through the stage model and back again. Psychol Addict Behav. 2017;31(8):847-861. doi:10.1037/adb0000311
- Day E, Rudd JHF. Alcohol use disorders and the heart. Addiction. 2019;114(9):1670-1678. doi:10.1111/add.14703
- Heidenreich PA, Bozkurt B, Aguilar D, et al. 2022 AHA/ACC/HFSA guideline for the management of heart failure: A report of the american college of cardiology/american heart association joint committee on clinical practice guidelines. Circulation. 2022;145(18):e895–e1032. doi: 10.1161/CIR.0000000000001063.
- Wang Z, Song J, Zhang L, Huang S, Bao L, Chen F, et al. Increased expression of microRNA-378a-5p in acute ethanol exposure of rat cardiomyocytes. Cell Stress Chaperones. 2017; 22(2):245–52. Epub 2017/02/03. doi: 10.1007/s12192-016-0760-y.