





Anterior Scoliosis Correction in Early Onset Scoliosis
Anterior Scoliosis Correction with Intervertebral De-Tethering Releases for the Treatment of Patients 5 to 10 Years of Age with Early Onset Scoliosis
M. Darryl Antonacci, MD1, Janet Cerrone, PA-C1, Anthony Yung, MMSc2, Laury A. Cuddihy, MD3, Randal R. Betz, MD1,
OPEN ACCESS
PUBLISHED: 30 December 2024
CITATION: ANTONACCI, M. Darryl et al. Anterior Scoliosis Correction with Intervertebral De-Tethering Releases for the Treatment of Patients 5 to 10 Years of Age with Early Onset Scoliosis. Medical Research Archives, [S.l.], v. 12, n. 12, dec. 2024. Available at: <https://esmed.org/MRA/mra/article/view/5982>.
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI: https://doi.org/10.18103/mra.v12i12.5982
ISSN 2375-1924
ABSTRACT
Anterior Scoliosis Correction (ASC) with anterior longitudinal ligament and annular disc complex (intervertebral) de-tethering releases is the authors’ multi-year advancement of their original mini-open vertebral body tethering technique to include a dual screw-line construct and multi-level intervertebral de-tethering releases. The study included patients diagnosed with early onset scoliosis, aged 5-10 years of age, Sanders stage 2 or less, Risser sign of 0, open triradiate cartilages, and a minimum of 2 years of follow-up. Within a database encompassing 840 patients treated by ASC, 15 patients (17 curves) met the inclusion criteria. The average duration of follow-up for this cohort was 48.3 months (range 25 to 86 months). The mean age at the time of surgery was 8 years (range 5.7 to 10.1 years). Preoperative scoliosis curves averaged 81° (range 58° to 100°). At the most recent follow-up, the instrumented curves improved to an average of 22° (range -15° to 68°) and mean correction of 75%. Preoperative 3-D kyphosis, calculated as an average of -6° (range -23° to +20°), was improved to an average of + 28° (range ‑1° to +59°) at latest follow-up. As may be anticipated with early onset scoliosis, 11 of the 15 patients underwent a secondary surgical procedure an average of 43 months following the index procedure. Of these 11, lengthening was necessary for overcorrection in 3 patients (20%), revision or subsequent stage ASC was done for additional correction adjustment in 6 patients (40%), and spinal fusion was performed in 2 patients (13%). In conclusion, a cohort of 15 patients aged 5-10 years with early onset scoliosis treated by ASC with intervertebral de-tethering releases (initial average curve of 81°) demonstrated a substantial mean correction of 75% in the instrumented curve. Although 2/15 patients (13%) subsequently underwent posterior spinal fusion, these early outcomes suggest a potential alternative to traditional posterior growing rod system approaches and posterior spinal fusion for these young patients.
1.0 Introduction
The treatment paradigm for early onset scoliosis (EOS) is inherently complex due to the wide spectrum of underlying etiologies and the imperative to accommodate the growth potential of the pediatric spine. Progressive thoracic scoliosis, manifesting in early childhood, is linked to a trajectory of restrictive pulmonary disease, with a potential extension to cardiac dysfunction and increased early mortality risk. Traditional approaches, notably early posterior spinal fusion (PSF) in patients younger than 10 years of age, have been employed; nevertheless, their suitability for young patients with EOS is still a matter of debate. The rigid inhibition of normal spinal and thoracic growth trajectories posed by early fusion may elicit adverse cardiopulmonary outcomes and negatively impact the health-related quality of life (HRQoL). Furthermore, early spinal fusion, particularly of the lumbar spine, is associated with long-term consequences, including reduced spinal mobility, which can lead to later adjacent intervertebral disc degeneration, junctional failures, and chronic pain.
Recent advances in surgical practice have seen a pivot towards growth friendly (GF) technologies. Approaches such as distraction- and compression-based systems have been developed to provide alternative management strategies. These technologies aim to address the deformity while preserving some of the spine’s growth potential.
Distraction-based GF systems, encompassing technologies such as growing rods, Vertical Expandable Prosthetic Titanium Rib (VEPTR), and Magnetically Controlled Growing Rods (MCGR), are engineered to rectify spinal deformities through the application of mechanical distraction. This is achieved by anchoring the devices superiorly and inferiorly to the spine, ribs, or pelvis, thereby exerting a distractive force across the deformed spinal segment. These implants have been empirically validated to ameliorate the coronal curve angle and effect spinal elongation; however, their associated complications are well-chronicled. Transverse plane deformities, such as the crankshaft phenomenon, may be exacerbated under the application of distraction-based devices.
An analysis of 140 patients revealed a complication occurrence in 58%, with at least one adverse event being reported. Notably, 47 patients (34%) underwent unplanned surgical interventions. Further scrutiny of the data indicates a 24% increase in the risk of complications with each additional surgical procedure undertaken. In the broader context of existing literature, MCGRs have been associated with similar failure modes, including anchor pull-out and rod fracture. A systematic review encompassing 15 studies quantified the incidence of unplanned revision surgeries to be higher with MCGR systems, particularly those utilizing MAGEC technology, as compared to traditional growing rods. Despite this, MCGRs have demonstrated efficacy in correcting coronal deformity, a reduced number of lengthening procedures, and preservation of spinal growth, albeit with a 44.5% complication rate and a 33% frequency of unplanned revision surgeries.
In a comprehensive retrospective evaluation of prospective data extracted from a multicenter registry, 130 patients were analyzed to compare the outcomes of PSF, MCGR, and vertebral body tethering (VBT), a compression-based system, in patients aged 8 to 11 with idiopathic EOS. The study concluded that all treatment modalities were effective in managing the curve and enhancing thoracic and spinal height. However, it was observed that patients undergoing VBT and PSF experienced fewer complications, required fewer unplanned surgical revisions, and demonstrated an overall improvement in HRQoL when contrasted with patients treated with MCGR.
Compression-based GF modalities, notably Anterior Scoliosis Correction (ASC) and VBT, employ a compressive force to the convexity of spinal deformities. This force, congruent with the Hueter-Volkmann principle, hampers convex growth and may be engendered both mechanically during implantation and dynamically through inhibited longitudinal growth of vertebral endplates due to the presence of the implants. The utilization of VBT in patients 10 years of age or younger with EOS is currently not widespread, underscoring a significant void in clinical evidence. This paucity of data necessitates further research.
Since 2014, ASC with anterior longitudinal ligament and annular disc complex (intervertebral) de-tethering releases has been employed through a modified anterior trans-thoracic approach which provides both compression across the convexity and effective derotation. This technique of screws and pliable cords is designed to circumvent the limitations associated with VBT, such as limited curve correction, specific curve size requisites, and the inability to achieve significant thoracic derotation or restoration of thoracic kyphosis. ASC additionally conserves segmental arteries and incorporates multilevel intervertebral de-tethering releases. With the demonstrable success seen in patients with adolescent idiopathic scoliosis (AIS), ASC with intervertebral de-tethering releases is gradually being considered for a broader patient demographic (including children < 10 years of age) by the authors of this paper, thereby expanding the therapeutic scope of this approach.
Currently, there exists a paucity of research exploring the clinical outcomes for patients aged 5 to 10 years with EOS who have been treated using ASC. This study aims to elucidate the therapeutic effectiveness of ASC in an initial cohort of patients with EOS.
2.0 Materials and Methods
2.1 POPULATION COHORT
All 840 consecutive patients who underwent ASC at our institution from May 2014 through December 2021 were considered for this study. Only patients who were ≤ 10 years of age, skeletally immature (Risser 0, Sanders ≤ 2, open triradiate cartilages) and who underwent anterior screw/cord instrumentation were included. A minimum follow-up of 2 years with radiographs was required for inclusion. Exclusion criteria disqualified participants with a previous history of surgery for EOS. All surgeries were performed by the primary surgeon (MDA) as previously described.
2.2 SURGICAL TECHNIQUE
Anterior Scoliosis Correction (ASC) with intervertebral de-tethering releases is typically carried out with the patient in the lateral decubitus position, positioning the convexity of the curve in the superior or “up” orientation. A single longitudinal incision, averaging 10–12 cm in length, is implemented via anterior muscle-sparing thoracotomy to reach the thoracic, thoracolumbar, and/or lumbar curves. Additional small (2 cm) port incisions might be required for accessing T4–T6 or for managing extensive thoracic curves extending to L2 or L3; these may be either incisional or, much more commonly, subfascial within the same incision. Pre-incision fluoroscopic views are taken to identify and mark the vertebrae intended for instrumentation. Single-lung ventilation within the incision site is used to improve visual access into the thoracic cavity and facilitate the placement of the instruments. Hypoventilation is used for lumbar curves entering the chest cavity through ribs T11–T12. Careful dissection of the parietal pleura from the lateral aspect of the vertebral body, anterior to the rib heads, is undertaken, paying particular attention to leaving many of the segmental vessels intact.
With the aid of fluoroscopic imaging, the appropriate spinal levels are exposed for instrumentation. The segmental vessels’ mobility is preserved by dissecting them, enabling them to be shifted either cephalad or caudal. This allows for the insertion of one or two three-prong staples into each vertebra anterior to the rib head. A threaded tap with dynamic surgical guidance (DSG) technology (PediGuard [SpineGuard, Paris, France]) is then employed to establish the screw path through the vertebral body and to ascertain the screw’s length. This use of a tap minimizes fluoroscopy exposure and distinguishes between the conductivity of cancellous bone, cortical bone, and soft bone tissue. This enables the identification of bicortical purchase with minimal incursion into the contralateral thoracic cavity, reducing the risk of injuring the lung or great blood vessels. Screw length is verified using the threaded tap and confirmed with a ball tip probe. All screws, which come with a
Hydroxyapatite coating, are placed in this manner, with their final bicortical positioning confirmed with AP and lateral fluoroscopic images. Anterior longitudinal ligament and annular disc complex (intervertebral) de-tethering releases are performed where necessary to improve curve correction and increase curve derotation for correction of thoracic hypokyphosis. The intervertebral de-tethering releases are intended to preserve the disc complex; we do not remove the cartilaginous end plate nor do we extend from bone to bone as is done for anterior fusion. The release of the contracted anterior longitudinal ligament and the constricted, fibrotic annulus typical of the scoliotic disc complex allows for substantial segmental release and derotation during correction by “de-tethering” the rigid, fibrotic, and rotated scoliotic spine in the sagittal, axial, and coronal planes. Post-surgery, the intervertebral de-tethering releases heal with the spine in a corrected position and thereby help maintain the derotated correction, while additional bone remodeling may also occur.
A cord made of polyethylene terephthalate (PET) is then introduced from proximal to distal. Each vertebral segment undergoes correction starting with translation. The key correction involves applying translation and derotation to the next distal vertebral body segment, using the proximal vertebral body segments for counter torque. Once translated and derotated, tension is applied to compress the two vertebrae. When the construct is tensioned, the set screws are tightened to sustain the correction. This process is repeated for each instrumented level. If a dual line construct is used, depending on the vertebral body size, the posterior construct is tensioned first, followed by the anterior construct. This dual line construct as opposed to a single line construct aids in achieving and maintaining curve derotation. Previous biomechanical work indicates better stabilization than single line constructs, without significant loss of mobility.
In EOS, during surgery, after derotation, residual coronal curves of 15 to 30° are intentionally left to allow for growth modulation. Upon the acquisition of final radiographs, a chest tube is placed, the lung is reinflated, and the wound is closed in a layered manner. For patients with double curves, upon completion of the thoracic curve correction, the patient is repositioned to the opposite lateral decubitus position, and the procedure is repeated for the opposite lumbar curve.
2.3 DATA COLLECTION AND ANALYSIS
For this study, radiographic measurements were performed using the RadiAnt DICOM Viewer software and included preoperative posteroanterior (PA) and lateral films, preoperative bending films, a left-hand radiograph, and an assessment of either open or closed triradiate cartilages. Postoperative evaluations, utilizing PA and sagittal radiographs (applying a negative value to overcorrected curves), were conducted for the first erect postoperative films, at the end of the first and second years following the index procedure and at the most recent follow-up. Radiographic spinal flexibility is calculated for each curve using the following formula:
(Pre-op coronal curve – fulcrum bending coronal curve) / pre-op coronal curve × 100 = % flexibility.
Two-dimensional thoracic kyphosis measurements were taken from preoperative and most recent postoperative sagittal radiographs. The formula to estimate three-dimensional kyphosis is as follows:
3D T5–T12 kyphosis = 18.1 + (0.81 × 2D T5–T12 kyphosis) – (0.54 × 2D thoracic coronal curve) degrees, noting that this model has an average error of ± 7.0°.
Suspicion of construct breakage was defined as a change of > 5° in the angulation of two screws in adjacent levels in comparison with previous images. The rate among patients with single or dual line constructs and the number of intervertebral disc releases were analyzed.
3.0 Results
The cohort comprised 15 patients (2 with double curves) presenting with 17 curves classified as early-onset scoliosis (Table 1). Diagnoses in the 15 patients included idiopathic (n=8), syndromic (n=4), congenital (n=1), status post spinal tumor resection (n=1), and
status post right omphalocele major repair (n = 1). The syndromic cohort (4 patients) consisted of 2 patients with Prader–Willi syndrome, one with chromosome 16 deletion, and one with Noonan’s syndrome. The mean age at the time of surgery was 8.0 years (range 5.7 to 10.1 years). Follow-up averaged 48.3 months (range 25 to 86 months). In terms of the surgical construct, 9 patients (53%) received a single line construct, while the remaining 8 patients (47%) were treated with a dual line construct. The placement of one or two screws per vertebra was a subjective determination by surgeon MDA depending on size of the patients’ vertebrae. Intervertebral de-tethering releases were performed in 14/15 patients (93%), averaging 3.3 levels per patient (range 1 to 7).
3.1 CORONAL RADIOGRAPHIC ANALYSIS
Preoperative coronal curve measurements averaged 81° (range 58 to 100°), with an average preoperative flexibility of 51% (range 21 to 71%). The first erect postoperative assessment demonstrated an average curve reduction to 33° (range 16 to 66°), translating to an average correction of 58% (range 23 to 78%). Instrumented segments showed an average reduction to 27° (range 6 to 46°) with an average correction percentage of 66% (range 47 to 91%). The most recent postoperative measurements indicated further improvement, with coronal curve angles averaging 23° (range -15 to 68°) in the instrumented segments for an average correction of 75% (range 30 to 123%). Measurement of the maximum coronal curve angle is shown in Table 1 and averaged only about 8° less correction. A case example is seen in Figure 1.
3.2 CASE HISTORY FOR FIGURE 1
This is an example of a unilateral instrumented thoracic curve over a period of 60 months postoperative. Shown are preoperative PA (A) and lateral (B) radiographs of an 8-year-old boy with a 60° upper thoracic curve encompassing a T4 hemivertebra with a large, stiff compensatory thoracic curve measuring 92°. (C) The preoperative left lateral bend upper thoracic curve measures 48°. (D) The right fulcrum bend radiograph shows that the compensatory curve bends down to 65°. The patient underwent right T7 to L3 ASC with single line construct and 4 level intervertebral de-tethering releases (T8–T12). Next shown are erect PA (E) and lateral (F) radiographs at 6 weeks postoperative. The upper thoracic uninstrumented curve measures 41° and the instrumented compensatory curve is 40°. (G) Erect PA at one year. (H, I) Most recent PA (H) and lateral (I) radiographs at 60 months; the uninstrumented upper thoracic curve remains stable at 40° and the instrumented compensatory thoracic curve measures 23°, demonstrating growth modulation at 12 years of age (Risser 0, Sanders 3). Figures (J) and (K) are AP supine left and right lateral bend films done at 60 months showing 28° of motion. Figures (L) and (M) are lateral standing maximum flexion-extension radiographs also at 60 months showing maintained 13° of motion.
3.3 SAGITTAL RADIOGRAPHIC ANALYSIS
The 2D sagittal curve preoperative measurements averaged 25° (range 7 to 57°), with the most recent postoperative measurements averaging 35° (range 2 to 55°). In the 3D sagittal plane, the preoperative curve averaged -6° (range -23.2 to 19.7°), with the most recent postoperative curve averaging 28° (range -0.8 to 58.6°). This is an average correction of 34° towards a more normal thoracic kyphosis. See Table 1.
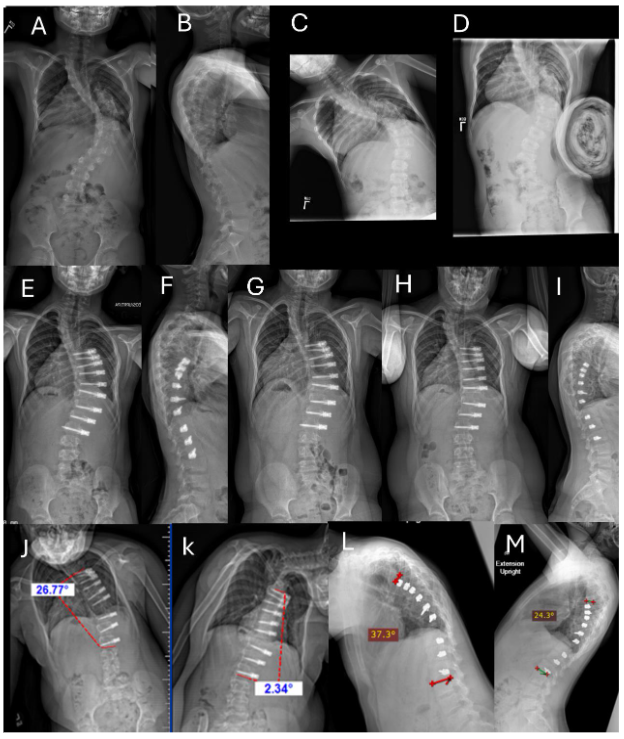
Fig. 1A-M. Example of unilateral instrumented thoracic curve over a period of 60 months postoperative. See Section 3.2 Case History for Figure 1.
Table 1. Data Summary: 15 Patients (17 Curves) with Early Onset Scoliosis
| Patients/% | Average (Range) | |
|---|---|---|
| Mean age at surgery (years) | 8.0 (5.7 to 10.1) | |
| Mean follow-up (months) | 48.3 (25 to 86) | |
| Construct of curves (n = 17) | ||
| • Single line construct | 9 (53) | |
| • Dual line construct | 8 (47) | |
| Intervertebral De-Tethering Releases | ||
| • # patients | 14/15 (93) | |
| • Avg # levels per patient | 3.3 (1 to 7) |
| Coronal Curve | Maximum | Instrumented |
|---|---|---|
| Pre-op (°) | 81.1 (58 to 100) | |
| Average flexibility (%) | 50.9 (21 to 71) | |
| First erect post-op (°) | 33.2 (16 to 66) | 26.9 (6 to 46) |
| Average correction (%) | 57.5 (23 to 78) | 65.9 (47 to 91) |
| Most recent post-op (°) | 30.6 (-38 to 73) | 22.5 (-15 to 68) |
| Average correction (%) | 63.5 (25 to 158) | 74.7 (30 to 123) |
| 2D Sagittal Curve | ||
|---|---|---|
| Pre-op (°) | 25.0 (7 to 57) | |
| Most recent (post-op) (°) | 35.1 (2 to 55) |
| 3D Sagittal Curve | ||
|---|---|---|
| Pre-op (°) | -5.6 (-23.2 to 19.7) | |
| Most recent (°) | 27.6 (-0.8 to 58.6) |
3.4 REVISION OR SUBSEQUENT STAGE SURGERY
Within the cohort, 11 of the 15 patients underwent a secondary surgical procedure at an average interval of 43 months (range 23 to 77 months) following the index procedure. Return to the operating room for lengthening due to overcorrection occurred in 3/15 patients (20%). See Figure 2.
3.5 CASE HISTORY FOR FIGURE 2
Example of a unilateral thoracic ASC with intervertebral de-tethering releases needing lengthening for overcorrection at 29 months postoperative. Preoperative PA (A) and lateral (B) radiographs of a 5½-year-old girl with an idiopathic thoracic curve measuring 80°. The patient underwent right T5 to L2 ASC with single screw-line, double cord construct and 5 level intervertebral de-tethering releases (T7–T12).
Erect PA (C) and lateral (D) radiographs at 6 weeks postoperative: the instrumented Cobb angle measures 36°. Erect PA (E) at 16 months showing 20° of distal overcorrection from T11 to L2. Right supine bending radiograph (F) at 16 months postoperative shows intra-construct flexibility from 35° to 20° (T5 to T11). Left supine bending radiograph (G) of the lumbar curve at 16 months postoperative shows intra-construct flexibility from -20° to -10° (T11 to L2). (F) and (G) demonstrate preserved mobility and the ability to delay surgical release the cord. (H) PA radiograph of the patient in a night brace to delay cord lengthening revision. She refused to wear the brace after 6 months. (I) At 29 months postoperative (pre-revision), the maximum curve measures 35° from T4 to T10 and minus 45° from T10–L12. (J) The left fulcrum bend Cobb angle measures 1° from T11 to L2, demonstrating continued flexibility. Revision involved removal of distal instrumentation in L1–L2 and the addition of all new cords from T4 to L2 and 9 intervertebral de-tethering releases. Specifically, the construct has slack between the screws to allow for growth and curve correction.
Most recent PA (K) and lateral (L) radiographs at 6 weeks post revision (30 months after index procedure) measure 27° instrumented curve and 45° maximum curve. The patient is now 8 years old. It is expected she will continue to grow and the curve will continue to correct. However, she still only has a single line construct, and it is possible that construct breakage and loss of correction could occur, requiring another stage of surgery.
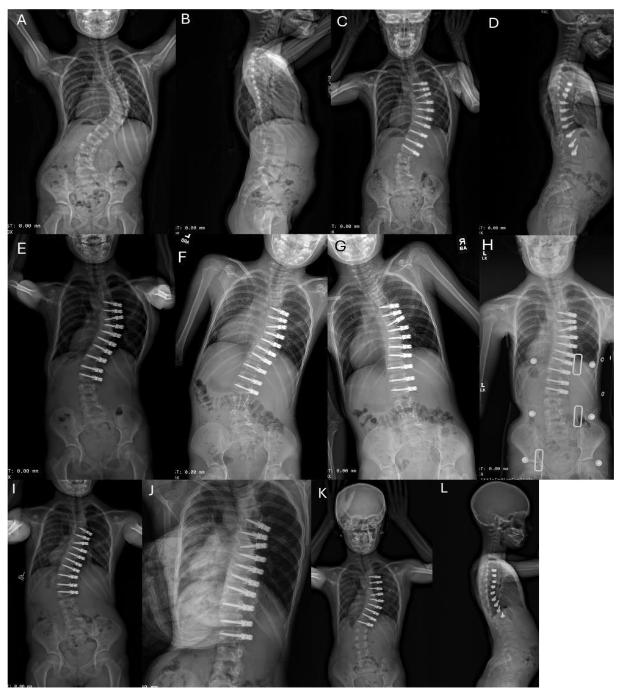
Fig. 2A-L. Example of a unilateral thoracic ASC with intervertebral de-tethering releases needing lengthening for overcorrection at 29 months postoperative. See Section 3.5 Case History for Figure 2.
Six of 15 patients (40%) required a subsequent stage ASC for additional curve correction. The other two patients (13%) required spinal fusion. One patient with a stiff curve measuring 106° had a fusion for persistent crankshaft. The instrumented curve corrected to 36°, but the curve crankshafted below the L2 instrumentation necessitating a fusion 3.5 years after initial ASC surgery. She had 3.5 years of growth before needing a fusion. The other patient with Prader-Willi syndrome needed a fusion for uncontrolled proximal kyphosis above the instrumented spine as is commonly seen in patients with this syndrome.
Interestingly, there is a trend that the 11 patients who required second surgeries initially had fewer intervertebral de-tethering releases, with an average of 2.5 per patient during the index procedure. In contrast, the 4 who did not require subsequent surgery underwent a higher number of intervertebral de-tethering releases, averaging 5.3 per patient. This trend requires further analysis after longer follow-up.
3.6 MEDICAL COMPLICATIONS
The study identified 3 medical complications in 3 separate patients. One patient with a known preoperative history of a minor temporary encephalopathy experienced a recurrence of encephalopathy postoperatively, which spontaneously resolved within 4 weeks. Another patient developed minor wound dehiscence that did not require surgery, and a third required extended intubation for secretion management. Notably, all patients who encountered these complications had pre-existing syndromes, suggesting a possible link between their underlying syndromic status and postoperative complication risk.
4.0 Discussion
4.1 COMPARATIVE ANALYSIS OF CORONAL RADIOGRAPHIC OUTCOMES AND CLINICAL SUCCESS AGAINST VERTEBRAL BODY TETHERING IN THE EXISTING LITERATURE
We found no other studies of similar aged patients undergoing VBT. The only potential study with which to compare was by Mackey et al.¹⁸ with patients with average age 11.3 years (range 10.9 to 11.8 years) at index surgery. In the Mackey study, VBT resulted in a 41.1% correction of the spinal curvature at final follow-up in a series of 37 patients. The median angle of the major preoperative curves in their cohort was only 50°, which is significantly less than the average preoperative curve angle of 81° found in our cohort. They noted an unplanned revision surgery rate of 16.2%, a figure that is comparatively lower than what was observed in our patients. It is critical to note that our cohort was not only characterized by a greater mean preoperative curve severity but also included much younger patients (by an average of 3 years) who were more skeletally immature (Sanders ≤ 2); both of these factors may contribute to an increased likelihood of a second surgery. Despite these challenges, our cohort of patients undergoing ASC with intervertebral de-tethering releases achieved a notable overall correction rate of 75%, which substantially surpasses the 41.1% correction rate observed by Mackey et al.
4.2 COMPARATIVE ANALYSIS OF CORONAL RADIOGRAPHIC OUTCOMES AND CLINICAL SUCCESS WITH GROWTH FRIENDLY DISTRACTION-BASED SYSTEM IN THE EXISTING LITERATURE
Historically, distraction-based growth-friendly systems have been the primary approach for managing EOS, yet they are often associated with a higher complication rate and suboptimal curve correction.³¹ ³⁴ Bess et al.¹⁵ reported an overall correction of 49% at an average follow-up of 59.6 months among 140 patients who underwent treatment with traditional growing rods. A recognized limitation of this intervention is the requirement for multiple planned surgeries. Notably, patients in this cohort experienced a 450% rate of return to the operating room (OR) for lengthenings every 4 to 6 months, a factor that is associated with an increased risk of complications. To mitigate this issue, magnetically controlled growing rods (MCGR) were developed to reduce the frequency of surgical lengthening interventions. Mackey et al.¹⁸ observed a significantly reduced
References
1. Pehrsson K, Larsson S, Oden A, Nachemson A. Long-term follow-up of patients with untreated scoliosis. A study of mortality, causes of death, and symptoms. Spine (Phila Pa 1976). 1992;17(9);1091-1096.
2. Jones RS, Kennedy JD, Hasham F, Owen R, Taylor JF. Mechanical inefficiency of the thoracic cage in scoliosis. Thorax. 1981;36 (6):456-461. DOI:10.1136/thx.36.6.456
3. Fernandes P, Weinstein SL. Natural history of early onset scoliosis. J Bone Joint Surg Am. 2007;89(Suppl 1):21-33. DOI: 10.2106/JBJS.F.00754
4. Winter RB, Moe JH. The results of spinal arthrodesis for congenital spinal deformity in patients younger than five years old. J Bone Joint Surg Am. 1982;64(3):419-432.
5. Campbell Jr RM, Hell-Vocke AK. Growth of the thoracic spine in congenital scoliosis after expansion thoracoplasty. J Bone Joint Surg Am 2003;85(3): 409-420. DOI: 10.2106/00004623-200303000-00002
6. Karol LA, Johnston C, Mladenov K, Schochet P, Walters P, Browne RH. Pulmonary function following early thoracic fusion in non-neuromuscular scoliosis. J Bone Joint Surg Am. 2008:90(6):1272-1281. DOI: 10.2106/JBJS.G.00184
7. Vitale MG, Matsumoto H, Bye MR, Gomez JA, Booker WA, Hyman JE, Roye Jr DP. A retrospective cohort study of pulmonary function, radiographic measures, and quality of life in children with congenital scoliosis: an evaluation of patient outcomes after early spinal fusion. Spine (Phila Pa 1976). 2008; 33(11):1242-1249.
DOI: 10.1097/BRS.0b013e3181714536
8. Danielsson AJ, Nachemson AL. Back pain and function 22 years after brace treatment for adolescent idiopathic scoliosis: a case-control study—part I. Spine (Phila Pa 1976). 2003;28(18):2078-2085. DOI: 10.1097/01.BRS.0000084268.77805.6F
9. Green DW, Lawhorne 3rd TW, Widmann RF, Kepler CK, Ahern C, Mintz DN, Rawlins BA, Burke SW, Boachie-Adjei O. Long-term magnetic resonance imaging follow-up demonstrates minimal transitional level lumbar disc degeneration after posterior spine fusion for adolescent idiopathic scoliosis. Spine (Phila Pa 1976). 2011;36(23):1948-1954. DOI: 10.1097/BRS.0b013e3181ff1ea9
10. Hsu PC, Feng CK, Huang SH. Chiu JW, Chou CL, Yang TF. Health-related quality of life in children and adolescent with different types of scoliosis: a cross-sectional study. J Chin Med Assoc. 2019;82(2):161-166.
DOI: 10.1097/JCMA.0000000000000020
11. Kepler CK, Meredith DS, Green DW, Widmann RF. Long-term outcomes after posterior spine fusion for adolescent idiopathic scoliosis. Curr Opin Pediatr. 2012;24(1):68-75. DOI: 10.1097/MOP.0b013e32834ec982
12. Lykissas MG, Jain VV, Nathan ST, Pawar V, Eismann EA, Sturm PF, Crawford AH. Mid- to long-term outcomes in adolescent idiopathic scoliosis after instrumented posterior spinal fusion: a meta-analysis. Spine (Phila Pa 1976). 2013;38(2):E113-119. DOI 10.1097/BRS.0b013e31827ae3d0
13. Motoyama EK, Yang CI, Deeney VF. Thoracic malformation with early-onset scoliosis: effect of serial VEPTR expansion thoracoplasty on lung growth and function in children. Paediatr Respir Rev. 2009;10(1):12-17.
DOI: 10.1016/j.prrv.2008.10.004
14. Skaggs DL, Akbarnia BA, Flynn JM, Myung KS, Sponseller PD, Vitale MG, Chest Wall and Spine Deformity Study Group, Growing Spine Study Group. A classification of growth friendly spine implants. J Pediatr Orthop. 2014;34(3):260-274. DOI: 10.1097/BPO.0000000000000073
15. Bess S, Akbarnia BA, Thompson GH, Sponseller PD, Shah SA, El Sebaie H, Boachie-Adjei O, Karlin LI, Canale S, Poe-Kochert C, Skaggs DL. Complications of growing-rod treatment for early-onset scoliosis: analysis of one hundred and forty patients. J Bone Joint Surg Am. 2010;92(15): 2533-2543. DOI 10.2106/jbjs.i.01471
16. Agarwal A, Kelkar A, Agarwal AG, Jayaswal D, Jayaswal A, Shendge V. Device-related complications associated with Magec Rod usage for distraction-based correction of scoliosis. Spine Surg Relat Res. 2019;4(2):148-151.
DOI: 10.22603/ssrr.2019-0041
17. Thakar C, Kieser DC, Mardare M, Haleem S, Fairbank J, Nnadi C. Systematic review of the complications associated with magnetically controlled growing rods for the treatment of early onset scoliosis. Eur Spine J. 2018;27(9):2062-2071. DOI:10.1007/s00586-018-5590-4
18. Mackey C, Hanstein R, Lo Y, Vaughan M, St. Hilaire T, Luhmann SJ, Vitale MG, Glotzbecker MP, Samdani A, Parent S, Gomez JA, Pediatric Spine Study Group. Magnetically controlled growing rods (MCGR) versus single posterior spinal fusion (PSF) versus vertebral body tether (VBT) in older early onset scoliosis (EOS) patients: how do early outcomes compare? Spine (Phila Pa 1976), 2022;47(4):295-302. DOI: 10.1097/BRS.0000000000004245
19. Stokes IA, Spence H, Aronsson DD, Kilmer N. Mechanical modulation of vertebral body growth. Implications for scoliosis progression. Spine (Phila Pa 1976), 1996;21(10):1162-1167.
DOI: 10.1097/00007632-199605150-00007
20. Mehlman CT, Araghi A, Roy DR. Hyphenated history: the Hueter-Volkmann law. Am J Orthop (Belle Mead NJ). 1997;26(11):798-800.
21. Baroncini A, Courvoisier A. The different applications of vertebral body tethering – narrative review and clinical experience. J Orthop. 2023; 37:86-92. DOI: 10.1016/j.jor.2023.02.012
22. Cuddihy L, Swiercz M, Antonacci C, Betz R, Antonacci M (2021) Predicting the major coronal curve angle on initial standing x-rays based on intraoperative correction during anterior scoliosis correction and vertebral body tethering: comparison of single vs. double cord/screw constructs. 28th International Meeting on Advanced Spine Techniques (virtual), April 23-25, 2021.
23. Cuddihy LA, Antonacci MD, Vig KS, Hussain AK, Levin D, Betz RR. Progressive double major scoliotic curve with concurrent lumbosacral spondylolisthesis in a skeletally immature patient with Marfan syndrome treated with anterior scoliosis correction. Spine Deform. 2020;8(1):139-146. DOI: 10.1007/s43390-020-00031-6
24. Cuddihy LA, Antonacci MD, Hussain AK, Vig KS, Mulcahey MJ, Betz RR. Progressive neuromuscular scoliosis secondary to spinal cord injury in a young patient treated with nonfusion anterior scoliosis correction. Top Spinal Cord Inj Rehabil. 2019;25(2):150-156. DOI: 10.1310/sci2502-150
25. Betz RR, Antonacci MD, Cuddihy LA. Alternatives to spinal fusion surgery in pediatric deformity. Curr Orthop Pract. 2018:29(5):430-435
26. Antonacci MD, Yung A, Kozicz A, Cerrone J, Antonacci CL, Verma Y, Sweeney M, Cuddihy LA, Betz RR. Double screw-line technique of anterior scoliosis correction with thoracic disc releases for thoracic curves > 65 degrees: surgical techniques and outcomes. Med Res Arch J. 2023;11(7.1). DOI: 10.18103/mra.v11i7.1.4095
27. Antonacci CL, Antonacci MD, Bassett WP, Cerrone JL, Haas AR, Haoson DS, Cuddihy LA, Betz RR. Treatment of patients with scoliosis using a unique anterior scoliosis correction technique. Med Res Arch J. 2021;9(7).
DOI: 10.18103/mra.v4i7.2463
28. Trobisch P, Mahoney JM, Eichenlaub EK, Antonacci CL, Cuddiny L, Amin DB, Razo-Castaneda D, Orbach MR, McGuckin JP, Bucklen BS, Antonacci MD, Betz RR. An investigation of range of motion preservation in fusionless anterior double screw and cord constructs for scoliosis correction. Eur Spine J. 2023;32(4):1173-1186. DOI: 10.1007/s00586-023-07608-5
29. Parvaresh KC, Osborn EJ, Reighard FG, Doan J, Bastrom TP, Newton PO. Predicting 3D thoracic kyphosis using traditional 2D radiographic measurements in adolescent idiopathic scoliosis. Spine Deform. 2017;5(3):159-165. DOI: 10.1016/j.jspd.2016.12.002
30. Newton PO, Bartley CE, Bastrom TP, Kluck DG, Saito W, Yaszay B. Anterior spinal growth modulation in skeletally immature patients with idiopathic scoliosis: a comparison with posterior spinal fusion at 2 to 5 years postoperatively. J Bone Joint Surg Am. 2020;102(9):769-777. DOI: 10.2106/JBJS.19.01176
31. Ellinger F, Tropp H, Gerdhem P, Hallgren HB, Ivars K. Magnetically controlled growing rod treatment for early-onset scoliosis: analysis of 52 consecutive cases demonstrates improvement of coronal deformity. J Spine Surg. 2023;9(3):259-268. DOI: 10.21037;jss-22-70
32. Urbański W, Tucker S, Ember T, Nadarajah R. Single vs dual rod constructs in early onset scoliosis treated with magnetically controlled growing rods. Adv Clin Exp Med. 2020;29(10):1169-1174. DOI: 10.17218/acem/126289
33. Acaroglu E, Yazici M, Alanay A, Surat A. Three-dimensional evolution of scoliotic curve during instrumentation without fusion in young children. J Pediatr Orthop. 2002;22(4):492-496
34. Klemme WR, Denis F, Winter RB, Lonstein JW, Koop SE. Spinal instrumentation without fusion for progressive scoliosis in young children. J Pediatr Orthop. 1997;17:734-742
35. Moe JH, Kharrat K, Winter RB, Cummine JL. Harrington instrumentation without fusion plus external orthotic support for the treatment of difficult curvature problems in young children. Clin Orthop Relat Res. 1984;185:35-45
36. Harrington PR. Treatment of scoliosis. Correction and internal fixation by spine instrumentation. J Bone Joint Surg Am. 1962;44: 591-610