





Arthroscopic Bankart Repair: All-Suture Anchor Outcomes
Arthroscopic Bankart Repair with All Suture Anchors as Treatment of Anterior Shoulder Instability
Juan Carlos Jaramillo. MD.1; Antonio Orrego. MD.2; Simón Uribe. MD.3; Daniela Galeano. MD.4; Manuel Vallejo. MD.5; Ana Maria Arcila. MD 6; Ana Milena Herrera. MD. Ph.D. *7
- Juan Carlos Jaramillo, MD Orthopedic surgeon. Shoulder and elbow orthopedics. Clínica del Campestre and Hospital Pablo Tobón Uribe. Medellín. Colombia. http://orcid.org/0009-0008-1910-6952
- Antonio Orrego, MD Orthopaedic surgery resident. CES University. Medellin, Colombia http://orcid.org/0000-0002-2119-9974
- Simón Uribe, MD Clinica del Campestre. Medellín, Colombia http://orcid.org/0000-0002-2949-293X
- Daniela Galeano, MD Orthopedic surgeon. Clinica del Campestre and Hospital Pablo Tobon Uribe. Medellín, Colombia http://orcid.org/0000-0003-0954-6352
- Manuel Vallejo, MD Orthopedic surgeon. Knee surgery fellow, Universidad El Bosque. Bogotá, Colombia http://orcid.org/0000-0001-6638-0710
- Ana Maria Arcila, MD Clinica del Campestre. Medellín, Colombia http://orcid.org/0009-0001-1438-1524
- Ana Milena Herrera, MD, PhD Epidemiology Unit, Clínica del Campestre. Medellin, Colombia http://orcid.org/0000-0002-7382-5631
OPEN ACCESS
PUBLISHED: 31 October 2025
CITATION: JARAMILLO, Juan Carlos et al. Arthroscopic Bankart Repair with All Suture Anchors as Treatment of Anterior Shoulder Instability. Medical Research Archives, [S.l.], v. 13, n. 10, oct. 2025. Available at: <https://esmed.org/MRA/mra/article/view/6999>. Date accessed: 07 nov. 2025. doi: https://doi.org/10.18103/mra.v13i10.6999.
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI: https://doi.org/10.18103/mra.v13i10.6999
ISSN 2375-1924
Abstract
Background: Arthroscopic Bankart repair is the preferred surgical treatment for recurrent anterior shoulder instability. The development of all-suture anchors aims to reduce invasiveness, preserve bone stock, and facilitate revision options.
Aims: To assess short- and mid-term clinical outcomes of arthroscopic Bankart repair using exclusively all-suture anchors, focusing on recurrence of instability, functional recovery, and safety.
Methods: We retrospectively reviewed 53 patients who underwent arthroscopic Bankart repair with all-suture anchors between 2010 and 2024. The primary outcome was recurrent instability (dislocation or subluxation). Secondary outcomes included pain assessed by visual analogue scale, range of motion, functional recovery using the Rowe score, and need for revision surgery. The use of adjunctive procedures (rotator interval closure, remplissage) was documented. Comparative analyses were performed using nonparametric tests, with significance set at p < 0.05.
Results: The median follow-up was 8 months (range, 4–94 months). Redislocation occurred in 4 patients (7.5%) and subluxation in 2 (3.8%); 3 patients (5.7%) required revision surgery. The median Rowe score improved from 30 preoperatively to 100 at final follow-up (p<0.01), with 88.6% of patients achieving excellent outcomes. Pain scores decreased significantly (median visual analogue scale from 7 to 0; p<0.01). Most patients recovered near-full range of motion, and return to sports was achieved at a median of 24 weeks. No anchor-related complications were observed.
Conclusion: Arthroscopic Bankart repair using all-suture anchors provides excellent functional outcomes, significant pain reduction, and low recurrence rates in short- and mid-term follow-up, confirming this technique as a safe and effective option for anterior shoulder instability.
Keywords: Bankart Lesion; Arthroscopy; Shoulder Dislocation; Suture Anchors; Shoulder Instability
Introduction
Anterior shoulder instability is a common and debilitating condition, particularly affecting young, active individuals and athletes. The risk of recurrence after a first-time traumatic anterior shoulder dislocation is strongly influenced by age and activity level, with reported rates as high as 70–90% in adolescents and young adults managed non-operatively 1–3. Beyond recurrent dislocation, patients often experience persistent pain, apprehension, and functional impairment that can negatively impact sports participation and quality of life 1,2. If not addressed, repeated instability episodes predispose to cartilage injury, progressive capsulolabral insufficiency, and ultimately glenohumeral osteoarthritis 1,2. The underlying pathology most frequently involves avulsion of the anteroinferior labrum from the glenoid rim (Bankart lesion), compromising both the labral bumper effect and the capsuloligamentous stabilizers 1,2,4. Surgical repair of the Bankart lesion remains the mainstay of treatment for patients with recurrent instability and for selected individuals at high risk of recurrence after first-time dislocation 2,3,5,6.
Historically, open Bankart repair was considered the gold standard due to its durability and low recurrence rates; however, with advances in arthroscopy, minimally invasive techniques have become increasingly favored. Arthroscopic Bankart repair (ABR) offers advantages such as smaller incisions, reduced morbidity, faster recovery, and the ability to manage concomitant intra-articular lesions 1,3,7,8. While early arthroscopic methods were associated with higher recurrence rates compared to open procedures, improvements in surgical technique, patient selection, and fixation devices have resulted in outcomes comparable to open repair 1,6–9. Consequently, ABR is now widely accepted as a reliable and reproducible method for anterior shoulder stabilization 3,8–11.
Implant technology has been central to these improvements. Traditional metallic and bioabsorbable anchors provide strong fixation but carry risks including implant migration, chondral injury, cyst formation, and imaging artifacts 8,12,13. All-suture anchors, introduced more recently, were designed to minimize these complications. Their smaller drill holes reduce bone loss, preserve glenoid stock for potential revision surgery, and avoid hardware-related morbidity 8,12–15.
Biomechanical studies demonstrate that all-suture anchors provide fixation strength comparable to metallic and bioabsorbable anchors 3,14,16,17, while clinical series have shown favorable functional outcomes, low complication rates, and satisfactory mid-term recurrence profiles 15,18–21. An additional advantage is the ability to maximize anchor density along the glenoid rim, which may enhance stability, particularly in patients with capsulolabral laxity 8,13,14.
Nevertheless, the use of all-suture anchors requires technical precision to achieve secure knot tying and appropriate capsulolabral tensioning 14,22. Furthermore, outcomes are influenced by patient-related variables such as age, activity level, and the presence of associated bone or soft-tissue lesions 10,23,24. Adjunctive techniques, such as remplissage for engaging Hill-Sachs lesions or rotator interval closure in cases of capsular redundancy, may further augment repair strength in carefully selected patients 25–31. Despite the growing adoption of all-suture anchors, questions remain regarding their long-term durability, optimal indications, and predictors of failure.
Given these knowledge gaps, robust clinical evidence is needed to inform surgical decision-making. The aim of this study was therefore to evaluate the short- and mid-term outcomes of arthroscopic Bankart repair performed exclusively with all-suture anchors in patients with anterior shoulder instability, with specific emphasis on recurrence, functional recovery, pain relief, and the need for revision surgery.
Methods
PATIENTS
Following approval by our institutional review board (IRB), we conducted a retrospective review of clinical data of consecutive patients who underwent outpatient arthroscopic Bankart repair using exclusively all-suture anchors for anterior shoulder instability between 2010 and 2024 at a medium-complexity specialized private practice. The senior author performed all procedures. Clinical records of patients of any age and sex were eligible for inclusion if they had undergone arthroscopic repair and completed at least one postoperative follow-up visit a minimum of 4 months after surgery. The diagnosis of primary anterior shoulder instability requiring repair was confirmed preoperatively using computed tomography (CT) or magnetic resonance imaging (MRI). Patients were not eligible for the procedure if they presented with circumferential (pan-labral) tears, had undergone revision procedures for recurrent instability. Incomplete clinical records were not considered for this analysis.
SURGICAL TECHNIQUE AND REHABILITATION PROTOCOL
With the patient in the lateral decubitus position, a standard posterior portal is established to perform diagnostic arthroscopy. Two additional portals are then created, mid-glenoid and anterosuperior, under needle localization. The mid-glenoid portal is positioned along the superior border of the subscapularis tendon with a 15–20° angle of attack, facilitating placement of the initial anchor at the 6 o’clock glenoid position. The anterosuperior portal is created anterior to the long head of the biceps, allowing placement of the cannula along the anterior glenoid margin and parallel to the articular surface.
Subsequently, the arthroscope is switched to the anterosuperior portal, and a cannula is placed posteriorly. When indicated, Hill-Sachs lesions are debrided through this portal, followed by insertion of a knotless Peek anchor (Quattro® Link Knotless Anchors, Zimmer Biomet) and completion of remplissage using a mattress suture tied at the end of the procedure. The anterior labrum is mobilized to the 6 o’clock position until the subscapularis belly is visualized. A guidewire is introduced through the anterior portal to the 6 o’clock glenoid position for placement of the first all-suture anchor. Capsular plication of the axillary recess is performed approximately 10 mm from the free capsule edge using Sixter forceps (TAG Medical Products Corporation Ltd. and Prof. Ofer Levy). Depending on the pathology, additional anchors are placed at the 7 o’clock (right shoulder) or 5 o’clock (left shoulder) positions, or a double-anchor construct is used at the 6 o’clock position. Anchors are further placed sequentially at the 5 o’clock and 4 o’clock positions with oblique mattress sutures. Additional fixation, when required, is performed with single-suture anchors, ensuring a “south-to-north” tensioning vector to reinforce the anterior band of the inferior glenohumeral ligament.
In patients with open rotator interval or signs of laxity, interval closure is performed percutaneously near the glenoid using the technique described by Stokes et al.26. All portals are closed conventionally with single sutures. Postoperative rehabilitation consists of sling immobilization for 4–5 weeks. At 8 days, sutures are removed and passive range of motion (ROM) initiated (flexion up to 90° and external rotation to neutral). At 4–5 weeks, the sling is discontinued, and active ROM is allowed with progressive stretching in flexion, external rotation, and internal rotation at 90° of abduction. At 12 weeks, supervised physiotherapy begins, focusing on strengthening and proprioception, while sport-specific training is permitted, excluding activities that involve throwing or contact. By 6 months, full return to sports is allowed if scapular mobility, strength, and stability are adequate and apprehension is absent.
OUTCOMES
Postoperatively, patients were followed according to the institutional protocol, and data were retrospectively extracted from clinical records using the last available follow-up for analysis. The primary outcome was recurrent instability, defined as any postoperative episode of dislocation or symptomatic subluxation, together with functional stability assessed using the Rowe Score 32. Secondary outcomes included recovery of shoulder range of motion, pain intensity measured with a visual analogue scale (VAS), clinical signs of instability, and the need for revision surgery.
STATISTICAL ANALYSIS
All analyses were performed using SPSS version 25.0 (IBM Corp., Chicago, IL, USA). Data distribution was assessed with the Kolmogorov–Smirnov test. Quantitative data are presented as medians with ranges (minimum–maximum), and categorical data as absolute frequencies and percentages. Pre- and postoperative comparisons at final follow-up were conducted using the Wilcoxon signed-rank test for continuous variables and chi-square test for categorical variables. The impact of adjunctive procedures (rotator interval closure and/or remplissage) on postoperative outcomes was analyzed using the Kruskal–Wallis test for continuous variables and Fisher’s exact test for categorical variables. A p-value <0.05 was considered statistically significant.
Results
This study included 53 patients with a mean age of 27 years (range, 15–63 years) at the time of surgery. In 51.9% of cases, the dominant shoulder was affected. Regarding occupational activity, 74.5% of patients worked in office-based jobs, whereas 20.7% reported manual or operative labor. Before surgery, 69.8% of patients experienced up to five dislocation episodes of the same shoulder, and 81.1% reported a traumatic mechanism of injury.
At baseline physical examination, the median anterior flexion was 170°, and external rotation in abduction was 70°. Posterior internal rotation reached the T12 spinal level in 90.5% of patients. Instability tests were frequently positive: apprehension in 94.3%, relocation in 75.5%, release in 67.9%, and sulcus in 20.8%. Shoulder pain of 7 or greater on the VAS was reported by 79.3% of patients. The median baseline Rowe score was 30, with 98.1% of patients classified in the poor category.
Imaging studies demonstrated a high prevalence of structural injuries, with Bankart lesions identified in 92.5% and Hill-Sachs lesions in 86.8% of patients. The median interval from first dislocation to surgery was 25 months. Intraoperatively, rotator interval closure was performed in 79.2% of patients and remplissage in 34%. The median number of all-suture anchors used was 4. No intraoperative complications were reported. Baseline clinical, imaging, and intraoperative variables are summarized in Table 1.
| Patients (n=53) | *Age (years) | £Sex | £Affected side | £Sports activity | £Mechanism of injury | £Number of previous dislocations | £Imaging findings | £Additional procedures | £Number of suture anchors | £Follow-up time (months) | *Time to return to sports activities (weeks) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| *Age (years) | 27 (15 – 63) | £Sex | Males 47 (79,2%) | Females 11 (20,8%) | £Affected side | Right 29 (54,7%) | Left 24 (45,3%) | £Sports activity | Contact sports 43 (81,1%) | £Mechanism of injury | Traumatic 43 (81,1%) | Atraumatic 10 (18,9%) | |||||||
| £Number of previous dislocations | 2 4 (2 – 22) | 3 5 (9,4%) | 11 (20,8%) | 14 (26,4%) | 7 (13,2%) | 10 (18,9%) | 6 (11,3%) | £Imaging findings | Classic Bankart-type labral lesion 49 (92,5%) | Bony Bankart-type labral lesion 13 (24,5%) | Labroligamentous periosteal avulsion 7 (13,2%) | Glenoid bone defect/bone loss 9 (17%) | Hill-Sachs lesion 46 (86,8%) | SLAP II lesion 3 (5,7%) | SLAP III lesion 0 | Rotator cuff injury 6 (11,3%) | £Additional procedures | Rotator interval closure 42 (79,2%) | Remplissage 18 (34%) |
| £Number of suture anchors | 2 1 (1,9%) | 3 7 (13,2%) | 4 27 (50,9%) | 5 9 (17%) | 6 6 (11,3%) | 7 3 (5,7%) | £Follow-up time (months) | < 6 8 (4 – 94) | 6 – 12 12 (22,6%) | 12 – 24 20 (37,7%) | 24 – 48 11 (20,8%) | > 48 6 (11,3%) | *Time to return to sports activities (weeks) 24 (24 – 28) |
During follow-up, recurrent anterior dislocation occurred in four patients (7.5%), including two atraumatic and two traumatic redislocations, while subluxation occurred in two patients (3.8%). Patients with redislocation had a median age of 28.5 years (range, 15–38), and those with subluxation had a median age of 19 years. Revision surgery was required in three cases (5.7%): one underwent open Bankart repair, and two underwent Latarjet procedures (Table 2).
| Outcomes and postoperative evolution | Preoperative (n=53) | Last follow-up in months (n=53) | < 6 (n=12) | p-value | 6 – 12 (n=20) | p-value | 12 – 24 (n=11) | p-value | 24 – 48 (n=6) | p-value | > 48 (n=4) | p-value | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| *Anterior flexion (°) | 170 (70 – 190) | 165 (160 – 180) | 0,660 | 170 (130 – 180) | 0,253 | 160 (140 – 180) | 0,518 | 170 (160 – 170) | 0,317 | 170 (120 – 180) | 0,655 | ||||||||||||
| *External rotation in aduction (°) | 70 (50 – 80) | 60 (30 – 70) | 0,027& | 65 (50 – 80) | 0,883 | 70 (50 – 80) | 0,257 | 60 (20 – 70) | 0,276 | 70 (30 – 70) | 1,000 | ||||||||||||
| £Posterior Internal rotation (vertebral level) | T5 1 (1,9%) | T6 1 (1,9%) | T10 2 (3,8%) | 48 (90,5%) | T12 1 (1,9%) | L1 1 (8,3%) | S1 4 (33,3%) | 6 (50%) | 1 (8,3%) | 0,130 | 7 (35%) | 13 (65%) | 0,263 | 4 (36,4%) | 1 (9,1%) | 6 (54,5%) | 0,210 | 1 (16,7%) | 5 (83,3%) | 0,219 | 1 (25%) | 3 (75%) | 0,625 |
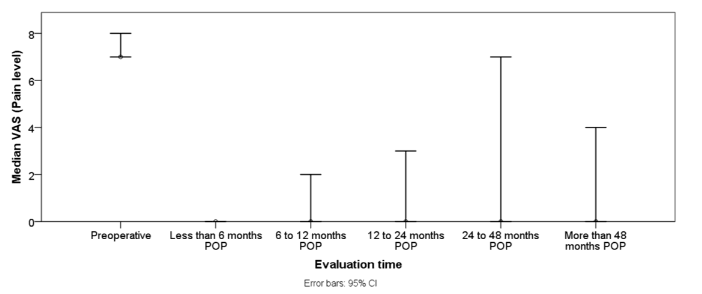
| *Pain level (VAS) | 7 (4 – 10) | 0 (0 – 6) | 0,002& | 0 (0 – 3) | 0,000& | 0 (0 – 8) | 0,004& | 0 (0 – 7) | 0,027& | 0 (0 – 4) | 0,066 | ||||||||||||
| *Rowe Score | 30 (20 – 65) | 100 (80 – 100) | 0,002& | 100 (50 – 100) | 0,000& | 100 (30 – 100) | 0,004& | 100 0,024& | 100 0,046& |
At the last follow-up, median anterior flexion was maintained at 170° (range, 120°–180°), and median abduction external rotation was 70° (range, 20°–80°). Posterior internal rotation improved, reaching T10 in 32.1% and T12 in 62.3% of patients. The apprehension sign was positive in only 9.4% of patients. Shoulder pain improved substantially: 92.5% reported VAS ≤3 at final follow-up (Figure 1).
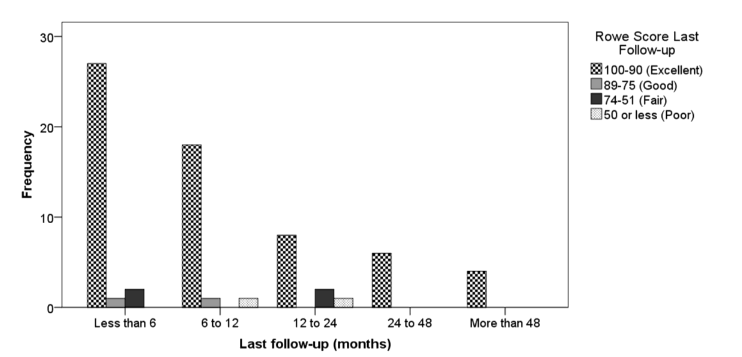
Median Rowe scores improved significantly to 100 (range, 30–100), with 88.6% of patients achieving excellent results (Table 2).
Comparative bivariate analysis confirmed significant improvement in median pain levels and Rowe scores across all follow-up intervals compared to preoperative values (Table 2).
External rotation in abduction only showed a significant difference in the subgroup with 4–6 months of follow-up (p = 0.027). For other parameters, changes in range of motion were not statistically different from baseline at later follow-up points. No significant relation was found between adjunctive procedures (rotator interval closure and/or remplissage) and the risk of recurrence (p=0.603), postoperative pain (p=0.383), Rowe score (p=0.920), or shoulder range of motion (p=0.761).
Discussion
This retrospective series demonstrated that arthroscopic Bankart repair using all-suture anchors achieves low recurrence rates (7.5%), significant pain reduction, and excellent functional outcomes (median Rowe 100) at short- to mid-term follow-up, with no anchor-related complications. These results highlight the reliability of all-suture anchors in managing anterior shoulder instability and align with contemporary evidence showing that advances in arthroscopic stabilization techniques provide results comparable to those of traditional open procedures.
Our recurrence rate (7.5%) is within the range reported in recent systematic reviews of ABR 7,10,11,33. Sugawara et al. 34 confirmed the long-term durability of ABR, with recurrence rates of 10% after 10 years of follow-up. Deshpande et al.27 recently compared ABR with the Latarjet procedure, showing that while Latarjet may reduce recurrence in high-risk patients, ABR provides similar functional outcomes and lower complication rates in the general population. In our study, nearly 90% of patients reached excellent Rowe scores, which is consistent with other reports of high postoperative satisfaction and functional recovery following ABR 8,11,18,21,34.
One of the central findings of our study was the absence of anchor-related complications. This corroborates reports from Ideler et al.35 and Wallace et al.36, who found that all-suture anchors are safe and radiologically stable at mid-term follow-up. These devices preserve glenoid bone stock, minimize cyst formation, and avoid migration risks associated with rigid anchors 2,37. Lee et al.14,22 further showed that anchor position and deployment angle significantly influence fixation strength, underscoring the importance of meticulous technique. These findings reinforce that all-suture anchors provide biomechanical stability equivalent to traditional anchors while avoiding revision procedures 3,15.
Despite favorable outcomes overall, recurrence remains a concern in specific populations 3. Young age, contact sports participation, and the presence of bipolar bone loss consistently emerge as risk factors 1,2,15,23. Recent meta-analyses by Bulleit et al.24 and Zhang et al.23 found that younger age (particularly <20 years), the presence of glenoid bone loss, Hill–Sachs lesions, and shoulder hyperlaxity are the most consistent predictors of recurrent instability following arthroscopic Bankart repair. Additional factors, such as participation in contact or competitive sports and male sex, have also been associated with higher recurrence risk 23,24. Likewise, our cases of redislocation and subluxation occurred predominantly in younger patients, consistent with these reports.
Bone loss assessment has shifted from absolute critical thresholds to a spectrum that includes subcritical loss and dynamic concepts such as the glenoid track 2,20. Lau et al.20 emphasized that defects as low as >7 % can compromise outcomes, while Asghar et al.38 questioned whether 13.5% should remain the defining cutoff. Recent reviews recommend that subcritical bone loss (10–15%) be carefully weighed when considering augmentation procedures 1,39. The glenoid track model, revisited by Itoi et al. 40 and Yamamoto et al.41, refines risk stratification by incorporating both glenoid and humeral head defects. In line with this, Moroder et al. 42 have recently proposed the global track concept, which integrates 3D evaluation of bipolar bone loss for a more precise prediction of engagement. While our study did not stratify by bone loss percentage, most failures occurred in patients with associated Hill-Sachs lesions, supporting the clinical importance of bipolar assessment.
Adjunctive remplissage has gained increasing attention 27,28,30. A recent meta-analysis by Davis et al.43 demonstrated that Bankart plus remplissage reduces recurrence and facilitates higher return-to-sport rates compared with Bankart repair alone, with outcomes similar or superior to Latarjet in selected patients 27,43. Our cohort included remplissage in 34% of cases, without anchor-related morbidity, supporting its role in treating engaging Hill-Sachs lesions 28,30,31,44. Similarly, rotator interval closure was performed in nearly 80% of cases. Although its benefit remains debated, closure has been advocated in cases of capsular laxity 29,45. Our analysis did not find a significant association between interval closure and recurrence, echoing recent reviews suggesting its effect may be patient-specific rather than universally beneficial 45.
The median time to sports resumption in our series aligns with the literature 1,27,46. Valk et al.47 reported that most athletes return between 5 and 7 months postoperatively, though psychological readiness may delay physical recovery 46,48. Utami et al.49 emphasized individualized, criteria-based progression to sport rather than rigid timelines. Our findings support this approach, as patients demonstrated a near-complete ROM and minimal pain before clearance.
The main limitations of our study are its retrospective design, variable follow-up, and lack of standardized imaging quantification of bone loss. These constraints may have limited our ability to fully stratify recurrence risk. Additionally, our sample was derived from a single surgeon’s practice, which enhances technique consistency but may limit generalizability. Longer prospective studies incorporating glenoid track measurements and patient-reported outcomes are warranted.
Overall, our findings add to the growing evidence that all-suture anchors are a safe, bone-preserving, and effective option for arthroscopic Bankart repair. Recurrence rates are low when the procedure is applied to appropriately selected patients, and functional outcomes are excellent. For high-risk populations, such as young athletes with bipolar bone loss, adjunctive procedures or alternative stabilizations like the Latarjet procedure should be considered.
Conclusion
Arthroscopic Bankart repair using all-suture anchors is a reliable option for treating anterior shoulder instability, providing low recurrence rates and excellent functional outcomes while preserving glenoid bone and minimizing implant-related complications.
Conflicts of Interest Statement:
The authors have no conflicts of interest to declare.
References
- Apostolakos JM, Wright-Chisem J, Gulotta LV, et al. Anterior glenohumeral instability: Current review with technical pearls and pitfalls of arthroscopic soft-tissue stabilization. World J Orthop. 2021;12(1):1-17. doi:10.5312/WJO.V12.I1.1
- Bauer S, Collin P, Zumstein MA, Neyton L, Blakeney WG. Current concepts in chronic traumatic anterior shoulder instability. EFORT Open Rev.British Editorial Society of Bone and Joint Surgery. 2023;8(6):468-481. doi:10.1530/EOR-22-0084
- DeFroda S, Bokshan S, Stern E, Sullivan K, Owens BD. Arthroscopic Bankart Repair for the Management of Anterior Shoulder Instability: Indications and Outcomes. Curr Rev Musculoskelet Med.Humana Press Inc. 2017;10(4):442-451. doi:10.1007/s12178-017-9435-2
- Pickett A, Svoboda S. Anterior Glenohumeral Instability. Sports Med Arthrosc Rev. 2017;25(3):156-162. doi:10.1097/JSA.0000000000000157
- Barlow JD, Grosel T, Higgins J, Everhart JS, Magnussen RA. Surgical treatment outcomes after primary vs recurrent anterior shoulder instability. J Clin Orthop Trauma.Elsevier B.V. 2019;10(2):222-230. doi:10.1016/j.jcot.2018.10.012
- Monk AP, Roberts PG, Logishetty K, et al. Evidence in managing traumatic anterior shoulder instability: A scoping review. Br J Sports Med.BMJ Publishing Group. 2015;49(5):307-311. doi:10.1136/bjsports-2013-092296
- Glazebrook H, Miller B, Wong I. Anterior Shoulder Instability: A Systematic Review of the Quality and Quantity of the Current Literature for Surgical Treatment. Orthop J Sports Med.SAGE Publications Ltd. 2018;6(11). doi:10.1177/2325967118805983
- Miura K, Tsuda E, Tohyama H, et al. Can arthroscopic Bankart repairs using suture anchors restore equivalent stability to open repairs in the management of traumatic anterior shoulder dislocation? A meta-analysis. Journal of Orthopaedic Science. 2018;23(6):935-941. doi:10.1016/j.jos.2018.06.016
- Gao B, DeFroda S, Bokshan S, et al. Arthroscopic Versus Open Bankart Repairs in Recurrent Anterior Shoulder Instability: A Systematic Review of the Association Between Publication Date and Postoperative Recurrent Instability in Systematic Reviews. Arthroscopy – Journal of Arthroscopic and Related Surgery.W.B. Saunders. 2020;36(3):862-871. doi:10.1016/j.arthro.2019.10.022
- Brown L, Rothermel S, Joshi R, Dhawan A. Recurrent Instability After Arthroscopic Bankart Reconstruction: A Systematic Review of Surgical Technical Factors. Arthroscopy – Journal of Arthroscopic and Related Surgery.W.B. Saunders. 2017;33(11):2081-2092. doi:10.1016/j.arthro.2017.06.038
- Asiri FAM, Alqhtani AA, Assiri AH, Alqahtani MH, Tedla JS, Awwadh BAA. Systematic Review of Arthroscopic Bankart Repair Outcomes for Anterior Shoulder Instability. Medical Science Monitor. 2024;30. doi:10.12659/MSM.945942
- Petrera M, Patella V, Patella S, Theodoropoulos J. A meta-analysis of open versus arthroscopic Bankart repair using suture anchors. Knee Surgery, Sports Traumatology, Arthroscopy. 2010;18(12):1742-1747. doi:10.1007/s00167-010-1093-5
- Marquardt B, Witt KA, Liem D, Steinbeck J, Pötzl W. Arthroscopic Bankart Repair in Traumatic Anterior Shoulder Instability Using a Suture Anchor Technique. Arthroscopy – Journal of Arthroscopic and Related Surgery. 2006;22(9):931-936. doi:10.1016/j.arthro.2006.04.105
- Lee JH, Itami Y, Hedayati B, et al. Biomechanical effects of position and angle of insertion for all-suture anchors in arthroscopic Bankart repair. Clinical Biomechanics. 2018;60:45-50. doi:10.1016/j.clinbiomech.2018.10.002
- Gül O, Okutan AE, Ayas MS. Arthroscopic glenoid labral lesion repair using all-suture anchor for traumatic anterior shoulder instability: short-term results. J Shoulder Elbow Surg. 2019;28(10):1991-1997. doi:10.1016/j.jse.2019.03.003
- Lee JH, Park I, Hyun HS, Kim SW, Shin SJ. Comparison of Clinical Outcomes and Computed Tomography Analysis for Tunnel Diameter After Arthroscopic Bankart Repair With the All-Suture Anchor and the Biodegradable Suture Anchor. Arthroscopy – Journal of Arthroscopic and Related Surgery. 2019;35(5):1351-1358. doi:10.1016/j.arthro.2018.12.011
- Uluyardımcı E, Öçgüder DA, Bozkurt ibrahim, Korkmazer S, Uğurlu M. All-suture anchors versus metal suture anchors in the arthroscopic treatment of traumatic anterior shoulder instability: A comparison of mid-term outcomes. Jt Dis Relat Surg. 2021;32(1):101-107. doi:10.5606/ehc.2021.75027
- Chalmers PN, Hillyard B, Kawakami J, et al. Double-loaded suture anchors in the treatment of anteroinferior glenohumeral instability. JSES Int. 2020;4(3):587-591. doi:10.1016/j.jseint.2020.03.015
- Jain V, Gupta H, Mehta N, Joshi D, Ajay, Kataria H. Retrospective Comparative Analysis of Clinical and Functional Outcome After Arthroscopic Bankart Repair using All-Suture Anchor and Metal Anchor. Malays Orthop J. 2024;18(1):11-18. doi:10.5704/MOJ.2403.002
- Lau LCM, Chau WW, Ng R, et al. Reconsidering “Critical” Bone Loss in Shoulder Instability: 17-Year Follow-Up Study following Arthroscopic Bankart Repair. Schwingel PA, ed. Adv Orthop. 2024;2024:1-11. doi:10.1155/2024/5598107
- Vermeulen AE, Landman EBM, Veen EJD, Nienhuis S, Koorevaar CT. Long-term clinical outcome of arthroscopic Bankart repair with suture anchors. J Shoulder Elbow Surg. 2019;28(5):e137-e143. doi:10.1016/j.jse.2018.09.027
- Lee JH, Shin SJ. All-Suture Anchor Deployment Configurations in Arthroscopic Bankart Repair: A Comparative Analysis of Clinical and Radiological Outcomes. Orthop J Sports Med. 2025;13(3). doi:10.1177/23259671251319533
- Zhang M, Liu J, Jia Y, et al. Risk factors for recurrence after Bankart repair: a systematic review and meta-analysis. J Orthop Surg Res. 2022;17(1):113. doi:10.1186/s13018-022-03011-w
- Bulleit CH, Hurley ET, Jing C, et al. Risk factors for recurrence following arthroscopic Bankart repair: a systematic review. J Shoulder Elbow Surg. 2024;33(11):2539-2549. doi:10.1016/j.jse.2024.04.017
- Shim SB, Jeong JY, Keum DH, Yoo JC. Does creating a trough on the anterior glenoid rim make a difference in Arthroscopic Bankart repair using suture anchors? A mid-term follow-up retrospective study. Journal of Orthopaedic Science. 2019;24(2):250-257. doi:10.1016/j.jos.2018.09.024
- Stokes DA, Savoie FH, Field LD, Ramsey JR. Arthroscopic repair of anterior glenohumeral instability and rotator interval lesions. Orthopedic Clinics of North America. 2003;34(4):529-538. doi:10.1016/S0030-5898(03)00091-9
- Deshpande V, Barnett I, Valk J, et al. Similar Outcomes, but Significantly Lower Complication Rate with Arthroscopic Bankart Repair with Remplissage Versus Open or Arthroscopic Latarjet for Shoulder Instability Across a Wide Range of Glenoid Bone Loss: A Systematic Review and Meta-Analysis. JSES Reviews, Reports, and Techniques. Published online August 2025. doi:10.1016/j.xrrt.2025.07.007
- Graden N, Ina J, Cabarcas B, et al. An Evidence-Based Approach to Indication for Remplissage. Curr Rev Musculoskelet Med. 2025;18(7):267-280. doi:10.1007/s12178-025-09969-4
- Karovalia SN, Collett DJ, Bokor D. Rotator interval closure: inconsistent techniques and its association with anterior instability. A literature review. Orthop Rev (Pavia). Published online June 26, 2019. doi:10.4081/or.2019.8136
- Liu JN, Gowd AK, Garcia GH, Cvetanovich GL, Cabarcas BC, Verma NN. Recurrence Rate of Instability After Remplissage for Treatment of Traumatic Anterior Shoulder Instability: A Systematic Review in Treatment of Subcritical Glenoid Bone Loss. Arthroscopy – Journal of Arthroscopic and Related Surgery.W.B. Saunders. 2018;34(10):2894-2907.e2. doi:10.1016/j.arthro.2018.05.031
- Lazarides AL, Duchman KR, Ledbetter L, Riboh JC, Garrigues GE. Arthroscopic Remplissage for Anterior Shoulder Instability: A Systematic Review of Clinical and Biomechanical Studies. Arthroscopy – Journal of Arthroscopic and Related Surgery.W.B. Saunders. 2019;35(2):617-628. doi:10.1016/j.arthro.2018.09.029
- Rowe CR, Patel D, Southmayd WW. The Bankart procedure: a long-term end-result study. J Bone Joint Surg Am. 1978;60(1):1-16.
- Manea H, Hafeez MH, Ahmad B, et al. Arthroscopic Bankart Repair Versus Open Latarjet Repair for Anterior Shoulder Instability: A Systematic Review and Meta-Analysis. Clin Med Insights Arthritis Musculoskelet Disord. 2025;18. doi:10.1177/11795441251360805
- Sugawara S, Yamamoto N, Koibuchi Y, et al. Long-Term Outcomes of Arthroscopic Bankart Repair: A 10-Year Follow-Up Study. JSES Int. Published online August 2025. doi:10.1016/j.jseint.2025.07.004
- Ideler N, De Mesel A, Vercruysse L, Declercq G, van Riet R, Verborgt O. Clinical and radiological outcome of all-suture anchors in shoulder and elbow surgery. Shoulder Elbow. 2023;15(5):544-553. doi:10.1177/17585732221127433
- Wallace AL, Calvo E, Ardèvol Cuesta J, et al. Safety and efficacy of second-generation all-suture anchors in labral tear arthroscopic repairs: prospective, multicenter, 1-year follow-up study. JSES Int. 2024;8(4):763-768. doi:10.1016/j.jseint.2024.04.008
- Ruiz Ibán MA, Vega Rodriguez R, Díaz Heredia J, Pérez Expósito R, Zarcos Paredes I, Ruiz Díaz R. Arthroscopic Bankart repair with all-suture anchors does not cause important glenoid bone osteolysis: a volumetric CT study of 143 anchors. Knee Surgery, Sports Traumatology, Arthroscopy. 2021;29(7):2152-2158. doi:10.1007/s00167-020-06192-1
- Asghar E, Burks R. Is 13.5% the Right Number for Critical Bone Loss? Arthroscopy: The Journal of Arthroscopic & Related Surgery. 2022;38(10):2773-2775. doi:10.1016/j.arthro.2022.08.001
- Cognetti DJ, DeFoor MT, Hartzler RU, Sheean AJ. Glenoid augmentation for subcritical bone loss: a narrative review. Ann Jt. 2024;9:15-15. doi:10.21037/aoj-23-36
- Itoi E, Yamamoto N, Di Giacomo G, Marcello G. Glenoid track revisited. J Shoulder Elbow Surg. 2024;33(12):2791-2799. doi:10.1016/j.jse.2024.03.044
- Yamamoto N, Aizawa T, Itoi E. Glenoid track and subcritical Hill-Sachs lesion. JSES Int. 2024;8(3):608-613. doi:10.1016/j.jseint.2023.11.016
- Moroder P, Provencher MT, Di Giacomo G. The global track concept for evaluation of bipolar bone loss in anterior shoulder instability: Current concepts. Journal of ISAKOS. 2025;12:100852. doi:10.1016/j.jisako.2025.100852
- Davis WH, DiPasquale JA, Patel RK, et al. Arthroscopic Remplissage Combined With Bankart Repair Results in a Higher Rate of Return to Sport in Athletes Compared With Bankart Repair Alone or the Latarjet Procedure: A Systematic Review and Meta-analysis. Am J Sports Med. 2023;51(12):3304-3312. doi:10.1177/03635465221138559
- Leroux T, Bhatti A, Khoshbin A, et al. Combined arthroscopic bankart repair and remplissage for recurrent shoulder instability. Arthroscopy – Journal of Arthroscopic and Related Surgery. 2013;29(10):1693-1701. doi:10.1016/j.arthro.2013.06.007
- Mirzayan R, Itoi E, Karpyshyn J, Wong IH, Di Giacomo G. Controversies in surgical management of anterior shoulder instability. State of the Art. Journal of ISAKOS. 2024;9(2):168-183. doi:10.1016/j.jisako.2023.10.008
- Fountzoulas K, Hassan S, Khoriati A achraf, Chiang CH, Little N, Patel V. Arthroscopic stabilisation for shoulder instability. J Clin Orthop Trauma.Elsevier B.V. 2020;11:S402-S411. doi:10.1016/j.jcot.2019.07.006
- Valk J, Deshpande V, Hitchens H, et al. Ranges of Return to Sport Outcomes Following Anterior Shoulder Instability Surgery Are Influenced by Procedure, Athletic Level, and Follow-Up Duration: A Systematic Review. Arthroscopy: The Journal of Arthroscopic & Related Surgery. Published online July 2025. doi:10.1016/j.arthro.2025.07.032
- Paul RW, Osman A, Windsor JT, Slavick C, Romeo AA, Erickson BJ. Psychological readiness of return to sport after arthroscopic Bankart repair: A systematic review. J Orthop. 2025;66:43-48. doi:10.1016/j.jor.2024.12.033
- Utami SW, Pratiwi SR, Mitchel, Gani KS, Kholinne E. Return to sports following arthroscopic Bankart repair: a narrative review. The Ewha Medical Journal. 2024;47(2). doi:10.12771/emj.2024.e21