





Assessing Iron Status: Hb and Ferritin in Anaemia Treatment
Use of haemoglobin and ferritin to assess the need for and impact of use of iron fortified iodised salt
Prema Ramachandran1, K. Kalaivani2
- Prema Ramachandran Director
 http://orcid.org/0000-0003-1974-8281
http://orcid.org/0000-0003-1974-8281 - K. Kalaivani Deputy Director http://orcid.org/0000-0002-9582-4488
OPEN ACCESS
PUBLISHED: 31 May 2025
CITATION: Ramachandran, P., and Kalaivani, K., 2025. Use of haemoglobin and ferritin to assess the need for and impact of use of iron fortified iodised salt. Medical Research Archives, [online] 13(5). https://doi.org/10.18103/mra.v13i5.6431
COPYRIGHT © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i5.6431
ISSN 2375-1924
Abstract
Diagnosis of anaemia is by Haemoglobin (Hb) estimation. The World Health Organisation (WHO) has recommended ferritin estimation for assessment of iron deficiency because of concordance between ferritin levels in blood and stainable iron in bone marrow cells. In view of the wide variations in ferritin levels between individuals, communities, in presence of inflammation and in response to interventions, WHO recommended that population based longitudinal studies should be taken up to assess usefulness of ferritin for assessing the need for and for monitoring the impact of interventions to improve iron status.
Data from a 12-month longitudinal community-based open randomised trial to assess the impact of use of iron fortified iodised salt (DFS) were re-analysed to assess:
- usefulness of Hb and ferritin assays in assessing:
- need for use of iron fortified iodised salt (DFS) to improve Hb, and
- impact of 12-month use of DFS,
- usefulness of C Reactive Protein (CRP) assay in defining iron deficiency in presence of inflammation.
Haemoglobin (Hb) is the stable final circulating product which reflects the impact of nutrient deficiencies and interventions to correct them. Hb is the optimal parameter for:
- diagnosis of anaemia and severity of anaemia in individuals,
- assessing prevalence of anaemia in communities and the need for public health intervention to improve Hb and
- assessing the impact of intervention to improve Hb status both at the individual level and in population groups.
Both in men and women there was a progressive reduction in the mean ferritin with decreasing Hb level. Cut off of ferritin <15 ng/ml was useful for assessing prevalence of iron deficiency in women but not in men. Mean ferritin in women is useful for monitoring the impact of DFS in groups. Iron deficiency in women with inflammation could not be identified using CRP because most women with CRP ≥ 5 mg/L, had ferritin <70 ng/ml. Persistent inflammation (high CRP both at 0 and at 12 months) was not associated with lower mean Hb, as compared to those women who had no inflammation (CRP < 5 mg/L both at 0 and at 12 months).
Keywords
- anaemia
- haemoglobin
- ferritin
- iron fortified iodised salt
- C Reactive Protein
Introduction
Anaemia due to micro-nutrient deficiencies is the most common nutritional deficiency disease in the world. India is among the countries with a very high prevalence of anaemia. Anaemia is associated with increased risk of morbidity; severe anaemia during pregnancy is associated with higher maternal morbidity and mortality. Diagnosis of anaemia and assessing impact of interventions to correct anaemia at individual and in groups is by haemoglobin (Hb) estimation. The World Health Organisation (WHO) had reviewed global data and made recommendations for cut-off Hb levels to define anaemia and for grading the severity of anaemia in different age, sex and physiological groups. Taking into account the high prevalence and adverse health impact of anaemia, the Sustainable Development Goals (SDG) has set the target that by 2030 prevalence of anaemia in women in reproductive age (WRA) should be reduced by 50%. The mid-term assessment of progress towards SDG indicates that the progress towards the target is tardy; by 2030 there may in fact be some increase in the prevalence of anaemic women in reproductive age.
Currently, Hb is the most widely used parameter for assessing prevalence and severity of anaemia to decide on the need for public health interventions to improve Hb status both at community and at the individual level. Haemoglobin does not provide any information about the cause of anaemia. However, once the cause is identified and appropriate intervention had been initiated, Hb is the optimal parameter to assess the impact of intervention.
In developing countries about 3/4th of the anaemia is due to nutritional deficiencies (iron, folic acid and vitamin B12); acute blood loss, chronic blood loss due to infections such as malaria, haemoglobinopathies account for the remaining one fourth. Global data indicate that iron deficiency defined as inadequate body iron stores, accounts for about 2/3rd of the anaemia. The gold standard test for iron deficiency is absence of stainable iron in bone marrow aspirate. Bone marrow aspiration is an invasive procedure, done in clinical settings for diagnosis and management of patients. It is neither feasible nor ethical to undertake this procedure for the purpose of detecting iron deficiency in anaemic persons or defining prevalence of iron deficiency in communities. Ferritin is the primary iron-storage protein. Small amounts of ferritin are secreted into the circulation and can be readily measured. There was good concordance between ferritin levels in blood and stainable iron in bone marrow cells. The WHO reviewed the global data, recommended use of ferritin to assess iron deficiency in individuals and populations. Currently ferritin is the most widely used parameter for assessing iron deficiency.
Global data indicate that there are substantial variations in ferritin levels in apparently healthy men and women, between communities and countries. Ferritin is an inflammatory protein; infections and chronic inflammation are associated with elevated ferritin levels and mask the existence of iron deficiency. Taking all these into account, WHO also recommended that evidence base for use of ferritin for public health programmes should be improved through:
- well-designed, population-based longitudinal studies to define ferritin response to iron interventions which can be used to monitor the impact of public health programmes;
- studies to clarify cut-off points for ferritin, to define iron deficiency in presence of chronic, low-grade inflammation.
In India prevalence of anaemia, iron deficiency and chronic inflammation are high. Large scale national surveys to assess changes in nutritional status including anaemia and iron deficiency of the population are under way in India. Given the known variation in Hb, ferritin and C reactive protein (CRP) between countries, there is a need to explore the relationship between Hb, ferritin and CRP in Indian context. Our institution had undertaken a community based open randomised longitudinal study to assess impact of use of iodised salt (IS) and iron fortified iodised salt (double fortified salt DFS) in urban low middle-income families. The data from this longitudinal study were analysed to assess the usefulness of:
- Hb and ferritin in the population for assessing the need for public health intervention;
- Hb and ferritin in assessing the impact of intervention to reduce anaemia;
- concurrent ferritin and CRP assays for defining iron deficiency in presence of inflammation.
This analysis may be help in using Hb, ferritin and CRP for assessing the magnitude and severity of anaemia and iron deficiency in similar communities in India.
Material and Methods
Our institution had undertaken a community based longitudinal study in which the families were randomly allocated to IS or DFS groups. Allocated salt was given every month and families were followed up for 12 months. Estimation of Hb, ferritin and CRP were done in samples collected prior to the initiation (0 month), after 6 months and 12 months of salt use. The study design, inclusion-exclusion criteria, socio-demographic and nutritional profile of the families have been described in our earlier publication. Prior to initiation of the salt use there were no differences in Hb, ferritin and CRP profile, prevalence of anaemia, or iron deficiency of the men and women from the families who were randomly allocated to IS or DFS.
The primary objective of the current data analysis of the raw data without identifiers from an earlier community-based longitudinal study was to document usefulness of:
- Hb and ferritin at 0 months to assess the need for use DFS; and
- Hb and ferritin at 0 and 12 months for assessing the impact of DFS.
The secondary objective was to document how far concurrent ferritin and CRP assays help in defining iron deficiency in presence of inflammation.
The Study Design
Study design 1 was used assessing the need for use of DFS in the community. Based on the Hb levels at 0-month, prevalence of anaemia in men, women and children were computed. Prevalence of iron deficiency in men and women were computed using the cut-off of 15 ng/ml of ferritin for defining iron deficiency. In addition, mean ferritin levels were calculated in anaemic and non-anaemic women and men to assess the relationship between Hb and ferritin in women and men. Prevalence of anaemia in women, men and children and iron deficiency in women were used to assess whether the families required public health interventions to improve Hb and iron status.
Study design 2 was used for assessing impact of use of DFS for 12 months on Hb and ferritin. Usefulness of Hb in assessing the impact of DFS use for 12 months was ascertained by:
- Comparing the mean Hb at 0 and 12 months in men and women
- Comparing the mean Hb at 0 and 12 months in women and men who were grouped as anaemic or not anaemic based on Hb at 0 month
Usefulness of ferritin in assessing the impact of use of DFS for 12 months was ascertained by:
- Comparing the mean ferritin at 0 and 12 months in men and women
- Comparing the mean ferritin 0 and 12 months in women and men who were grouped as iron deficient (ferritin <15 ng/ml) and not iron deficient (ferritin ≥ 15 ng/ml) on the basis of ferritin at 0 month.
The secondary objective of the re-analysis was to document whether:
- concurrent ferritin and CRP assays help in defining iron deficiency in presence of inflammation and
- persistent inflammation (as assessed by CRP ≥ 5mg/L both at 0 and at 12 months) was associated with lower mean Hb at 12 months.
Results
Mean Hb was higher in men as compared to women and children (10.8±1.52 in 208 children). At the time of enrolment to the study, over 3/4th of the women, 62% of the children and nearly 40% of men were anaemic. By the WHO criteria, (prevalence of anaemia ≥ 40%) anaemia was a severe public health problem in these families.
More than one-third of women had ferritin level below 15 ng/ml; by WHO criteria, iron deficiency was a moderate public health problem in women. Mean ferritin level in men was three times the mean ferritin level in women. Prevalence of iron deficiency as assessed by ferritin level <15 ng/ml in men was very low. The low prevalence of iron deficiency as assessed by ferritin level <15 ng/ml might be due to the high levels of ferritin in men rather than absence of iron deficiency in men.
At the time of initial sample collection all women and men were apparently healthy and did not have any overt infection. Despite this one fifth of the women and one sixth of the men had CRP levels ≥ 5mg/L. In the study families 50.3% of women and 44% of men were over-nourished (BMI ≥25). Inflammation associated with adiposity may at least in part account for the high prevalence of CRP levels ≥ 5mg/L.
| 0 month | Women | Men |
|---|---|---|
| Hb (g/dL) | 10.8±1.52 (914) | 13.2±1.34 (323) |
| % anaemic | 77.8 | 39.0 |
| Ferritin (ng/ml) | 34.5±35.86 (871) | 101.8±60.66 (288) |
| %<12 | 28.8% | 2.8% |
| %<15 | 35.3% | 3.5% |
| CRP (mg/L) | 3.1±3.65 (870) | 2.8±3.36 (289) |
| % ≥ 5 mg CRP | 20.5 | 17.4 |
Differences in Hb and ferritin between men and women t test p< 0.001 & chi square p<0.001
Across all Hb levels, mean ferritin level in men was substantially higher as compared to the mean ferritin level in women; less than 5% of men had ferritin levels <15 ng/ml. There was a gradient in mean ferritin levels in relation to Hb levels both in men and women. Women who had lower Hb also had lower mean ferritin and higher prevalence of iron deficiency.
Table 2: Relationship between Hb and ferritin in women and men at 0 month
| Women | Men | ||||
|---|---|---|---|---|---|
| Hb (g/dL) | Ferritin (ng/ml) | % ferritin<15 | Hb (g/dL) | Ferritin (ng/ml) | % ferritin <15 |
| ≥12 | 45.9±40.96 (191) | 14.7 | ≥13 | 108.11±60.22 (177) | 2.3 |
| 10-11.9 | 34.8±33.26 (456) | 30.5 | 11-12.9 | 97.87±60.86 (96) | 3.1 |
| 8-9.9 | 24.9±32.94 (190) | 60.0 | 8-10.9 | 55.79±37.88 (14) | 14.3 |
| <8 | 19.5±35.43 (34) | 76.5 | <8 | 5.83±0.00 (1) | 100.0 |
| Total | 34.5±35.86 (871) | 35.3 | Total | 101.80±60.66 (288) | 3.5 |
T test ferritin level in women Hb≥12 vs 10-11.9, 8-9.9, and <8 all <0.001; men Hb≥13 vs 8-10.9 g/dL 0.002 Chi square ferritin <15 in women Hb ≥12 vs 10-11.9, 8-9.9, and <8 all <0.001 Chi square ferritin < 15 in men Hb ≥13 vs 8-10.9 <0.01
Anaemic men had lower mean ferritin, but prevalence of iron deficiency was low even in those with Hb <10g/dL. Relationship between Hb and ferritin in men and women is shown in the scatter-plot.
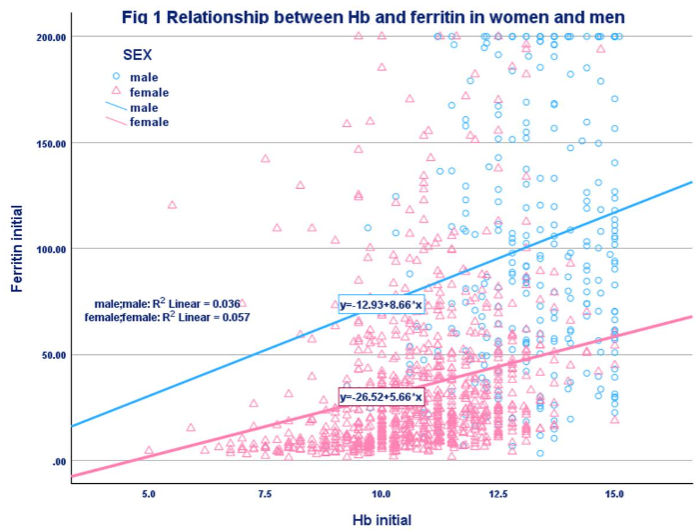
The differences in Hb levels between men and women were relatively small but differences in the ferritin levels between men and women were very large. Because of the high ferritin levels in men, prevalence of ferritin < 15 mg/ml was <5%.
RELATIONSHIP BETWEEN CRP AND FERRITIN
Mean ferritin levels were significantly higher in men and women who had CRP ≥ 5 mg/L as compared to those who had CRP <5 mg/L. Irrespective of the CRP levels over a third of women had ferritin levels <15 ng/ml. These data indicate that iron deficiency was a public health problem in women. Less than 5% of men had ferritin <15 ng/ml.
| CRP mg/l | Mean ferritin ng/ml | Ferritin < 12ng/ml | Ferritin < 15 ng/ml | |
|---|---|---|---|---|
| Women | CRP< 5 | 30.3±31.96 (692) | 31.8 | 39.9 |
| Men | CRP< 5 | 100.1±60.28 (238) | 2.9 | 3.8 |
| Women | CRP≥ 5 | 50.6±44.73 (178) | 16.3 | 35.4 |
| Men | CRP≥ 5 | 110.1±62.36 (50) | 2.0 | 3.5 |
T test women CRP <5 mg/l vs ≥ 5 mg/l <0.001 Chi square all salts women CRP <5 mg/l vs ≥ 5 mg/l <0.001
IMPACT OF USE OF DFS
There was a statistically significant increase in mean Hb (0.5 g/dL), a reduction in prevalence of anaemia, increase in mean ferritin (5 ng/ml) and reduction in the prevalence of low ferritin at 12 months as compared to 0 month in women who had used DFS for 12 months. The increase in Hb and ferritin levels in men after 12 months of use of DFS was small and not significant. The changes in mean CRP as well as CRP ≥5 mg/L in women and men using DFS for 12 months were small and not significant.
| Women | Men | ||
|---|---|---|---|
| DFS 0 month | Hb g/dL | 10.8±1.49 (595) | 13.3±1.30 (201) |
| % anaemic | 76.8 | 38.8 | |
| Ferritin ng/ml | 35.3±37.47 (571) | 105.8±57.79 (182) | |
| % <12 | 28.6 | 1.1 | |
| % <15 | 35.6 | 1.6 | |
| CRP mg/L | 3.2±3.66 (570) | 3.0±3.58 (182) | |
| % CRP ≥ 5 | 20.5 | 18.4 |
T test 0 vs 12-month women p value Hb <12 <0.001; ferritin <15 0.02 chi square test 0 vs 12-month women p value Hb <12 <0.001; ferritin <15 0.02
Women and men were classified as anaemic and non-anaemic on the basis of Hb at enrolment and the impact of DFS use for 12 months on Hb in anaemic and non-anaemic women and men were computed.
| Hb g/dL | 0 month | 12months |
|---|---|---|
| Women Anaemic <12 | 10.2±1.16 (457) | 10.9±1.10 (154) |
| Not anaemic ≥12 | 12.7±0.68 (138) | 12.7±0.88 (60) |
| Men Anaemic <13 | 11.9±0.82 (78) | 12.9±0.80 (14) |
| Not anaemic ≥13 | 14.1±0.69 (123) | 14.5±0.58 (31) |
T Test Hb in anaemic women and men <0.001; not anaemic men 0.003
Mean ferritin levels were computed in relation to Hb levels in women who had used DFS or IS for 12 months. For any given Hb category the mean ferritin levels were higher and prevalence of iron deficiency (ferritin <15 ng/ml) was lower in women who had used DFS for 12 months as compared to those who had used IS for 12 months. The differences in the mean ferritin and iron deficiency in men who had used IS or DFS were small. These data indicate that as compared to IS users, DFS use improves mean ferritin levels both in anaemic and non-anaemic women but not in men.
Women were classified as having low ferritin (<15 ng/ml) and normal ferritin at enrolment and the impact of use of DFS for 12 months on the mean ferritin levels were computed in paired values. Improvement in the mean ferritin level after 12 months of use of DFS was higher in the group of women who initially had ferritin <15 ng/ml as compared with the group who had normal ferritin values.
Table 6: Relationship between Hb & ferritin in women & men after 12 months of use of DFS or IS
| Salt used | Women | Men | ||||
|---|---|---|---|---|---|---|
| Hb g/dL | Ferritin (ng/ml) | % ferritin <15 ng/ml | Hb g/dL | Ferritin (ng/ml) | % ferritin <15 ng/ml | |
| IS | ≥12 | 42.3±23.51 (20) | 10.0 | ≥13 | 108.7±56.64 (35) | 2.9 |
| IS | 10-11.9 | 32.0±33.48 (71) | 40.8 | 11-12.9 | 95.4±70.08 (11) | 18.2 |
| IS | 8-9.9 | 23.1±34.92 (15) | 66.7 | 8-10.9 | 98.2±103.27 (2) | 0.0 |
| IS | <8 | 47.4±0.00 (1) | 0.0 | <8 | 0 | 0 |
| Total | 32.8±32.14 (107) | 38.3 | Total | 105.2±60.22 (48) | 6.3 |
T test DFS W ≥12.0 vs 10-11.9 <0.001; Chi square W IS≥12.0 vs 10-11.9 0.01; ≥12.0 vs 8-9.9 <0.001; DFS W ≥12.0 vs 8-9.9 <0.001
Impact of 12 months use of DFS in women with low and normal ferritin levels at enrolment (paired values)
| Ferritin groups | Ferritin (ng/ml) | T test | 0 month | 12 months |
|---|---|---|---|---|
| <15 ng/ml | <15 | 7.1±2.78 (39) | 8.5±3.15 (39) | 0.04 |
| ≥15 | 10.0±2.62 (37) | 32.7±21.33 (37) | <0.001 | |
| Total | 8.5±3.07 (76) | 20.3±19.28 (76) | <0.001 | |
| ≥15 ng/ml | <15 | 26.1±14.19 (10) | 10.9±3.85 (10) | 0.004 |
| ≥15 | 44.9±32.10 (94) | 54.9±34.56 (94) | 0.04 | |
| Total | 43.1±31.29 (104) | 50.7±35.35 (104) | <0.001 |
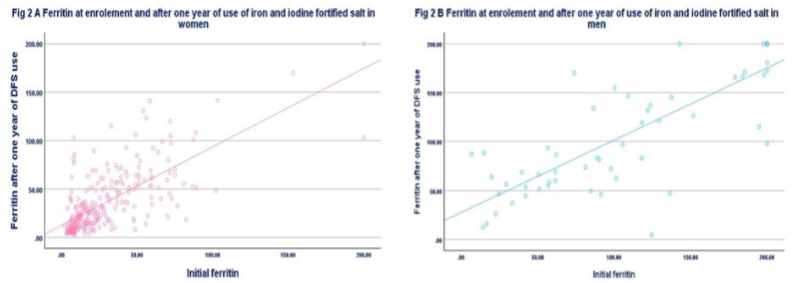
Scatter plot of ferritin in women and men at enrolment and after 12 months of use of DFS is given in the figure. Most of the ferritin values are clustered below 30 ng/ml in women; in men ferritin values were distributed between 30 and 200 ng/ml. If the cut-off of ferritin <15 ng/ml is used to define iron deficiency in men, very few will be classified as iron deficient either at enrolment or after use of DFS for 12 months.
In recent years there had been reports about association between anaemia and inflammation as assessed by CRP levels. Iron can also provoke inflammatory response. Paired data from the longitudinal study was analysed to find out whether there was any relationship between anaemia and persistent inflammation as assessed by CRP ≥ 5mg/L at enrolment and after 12 months of use of either IS or DFS. On the basis of CRP at 0- and 12-months women using DFS or IS were classified into four groups: those who had CRP <5 mg/L at both periods (no inflammation at both time points), those who had CRP ≥ 5 mg/L at 0 and 12 months (persistent inflammation) and those who had CRP ≥ 5 mg/L either at initial or at 12 months. The mean Hb and prevalence of anaemia was calculated in each of the four groups both in IS and DFS users.
| Salt | CRP mg/L | Hb g/dL 0 month | Hb g/dL 12 months | Number | 0 month | 12 month | Mean Hb <12 | Mean Hb <12 |
|---|---|---|---|---|---|---|---|---|
| IS | <5 mg/L | 10.5±1.48 | 11.0±1.30 | 78.9 | 71 | |||
| IS | ≥5 mg/L | 11.7±1.43 | 11.8±1.38 | 100.0 | 12 | |||
| IS | ≥5 mg/L | 10.7±0.98 | 10.5±1.23 | 66.7 | 8 | |||
| IS | ≥5 mg/L | 11.0±0.95 | 11.1±1.02 | 90.0 | 10 | |||
| DFS | <5 mg/L | 10.9±1.39 | 11.3±1.24 | 71.6 | 134 | |||
| DFS | ≥5 mg/L | 11.5±1.47 | 11.9±1.64 | 71.4 | 18 | |||
| DFS | ≥5 mg/L | 11.2±1.62 | 11.3±1.64 | 61.1 | 14 | |||
| DFS | ≥5 mg/L | 10.8±1.77 | 11.4±1.57 | 65.2 | 23 |
Ferritin is an inflammatory protein and ferritin levels are higher in presence of inflammation as assessed by CRP. In women mean CRP and ferritin were computed in paired samples collected at 0 and 12 months of IS and DFS users. Mean ferritin levels were higher and ferritin levels below 15 ng/ml were lower in women who had CRP ≥ 5mg/L irrespective of the salt used and period of sample collection (0 and 12 months). Irrespective of the CRP levels over a third of women had ferritin levels <15 ng/ml both at 0 and at 12 months.
| Salt used | CRP 0 month | CRP 12 months | Ferritin (ng/ml) 0 month | Ferritin (ng/ml) 12 months | Number | % <15 ng/ml | % <15 ng/ml |
|---|---|---|---|---|---|---|---|
| IS | <5 mg/L | <5 mg/l | 21.3±18.58 (69) | 25.3±22.05 (69) | 48.6 | 69 | |
| IS | ≥ 5 mg/l | 47.8±28.76 (10) | 12.5 | 49.5±29.08 (10) | 12.5 | 10 | |
| IS | ≥ 5 mg/l | 39.3±28.40 (8) | 10.0 | 43.4±43.43 (8) | 10.0 | 8 | |
| IS | ≥ 5 mg/l | 37.9±30.19 (10) | 30.0 | 39.9±30.43 (10) | 30.0 | 10 | |
| DFS | <5 mg/L | <5 mg/l | 24.5±25.75 (129) | 33.5±31.53 (129) | 33.3 | 129 | |
| DFS | ≥ 5 mg/l | 27.6±18.16 (16) | 14.3 | 59.8±37.75 (16) | 7.1 | 16 | |
| DFS | ≥ 5 mg/l | 43.8±21.34 (14) | 25.0 | 36.6±19.48 (14) | 6.3 | 14 | |
| DFS | ≥ 5 mg/l | 42.0±47.27 (23) | 26.1 | 45.6±38.83 (23) | 22.7 | 23 |
Paired data on prevalence of ferritin levels ≥70 ng/ml in men and women using IS or DFS (at 0 and 12 months) is given in the table. Majority of men and about 10% of women had ferritin levels ≥70ng/ml; therefore, cut-off of 70 ng/ml of ferritin (WHO recommended cut-off for iron deficiency when CRP level was ≥5 mg/L) may not be useful to define iron deficiency in women who had CRP ≥ 5 mg/L.
| Period | Salt | % Ferritin ≥70ng/ml | |
|---|---|---|---|
| 0 month | IS | 11.7 | 57.5 |
| DFS | 13.3 | 66.5 | |
| 12 months | IS | 8.4 | 62.5 |
| DFS | 15.2 | 70.7 |
Discussion
Anaemia due to micro-nutrient deficiencies is the most common nutritional deficiency disease in the world. Taking into account the high prevalence and adverse health impact of anaemia, the Sustainable Development Goals (SDG) has set the target that by 2030 prevalence of anaemia in WRA should be reduced by 50%. The mid-term assessment of progress towards SDG indicates that the progress towards the target is tardy; by 2030 there may in fact be some increase in the prevalence of anaemic WRA.
India is among the countries with a very high prevalence of anaemia. Five decades ago, India initiated the national programme of iron-folic acid supplementation to pregnant women and pre-school children. Coverage under the programme and continued use of IFA supplementation was low because of minor but troublesome side effects. Studies using newer, more expensive oral iron preparations have not been able to substantially reduce the side effects but increase the cost. Therefore, the national programme continues to use ferrous sulphate tablets. Surveys undertaken a decade ago using the accurate cyanmethaemoglobin method for estimating Hb showed that there has been some reduction in the prevalence of anaemia in women and children but anaemia remained a major public health problem.
Since 2018, the country has been implementing Intensive Iron Plus Initiative (I-NIPI) for combating anaemia by:
- improving dietary intake of micro-nutrients (long term strategy),
- use of iron fortified food stuffs to improve iron intake (medium-term strategy),
- ‘test, treat and track’ anaemia in pregnant women (short term strategy), and
- iron-folic acid supplementation to WRA and children (short term strategy).
India a vast and varied country and had been investing in research studies and surveys to obtain state/district specific data on:
- the need for initiating public health interventions such as iron fortified salt, IFA supplementation to WRA and
- assessing the impact of such interventions.
Given the known variation in Hb, ferritin and CRP between countries, there is a need to explore the relationship between Hb, ferritin and CRP in Indian context. The present study aims at ascertaining information on usefulness of Hb, ferritin and CRP in assessing the need as well as impact of public health interventions to combat anaemia and iron deficiency in India.
HB: THE PIVOTAL PARAMETER
Hb estimation is the most reliable method of assessment of current prevalence, need for public health intervention as well as impact of interventions on anaemia. At the time of enrolment to the study, nearly 3/4th of the women, nearly 2/3rd of the children (62%) and nearly 40% of men were anaemic. By the WHO criteria anaemia is a major public health problem in all age and sex groups, suggesting the urgent need for a sustainable public health intervention such as DFS to improve Hb status of the entire family.
Available data on iron intake in these families indicate that the gap between estimated average requirement (EAR) for iron and average iron intake in these families was between 5-10 mg/day/Consumption Unit. The DFS formulations contain 1 mg iron/gram of salt. The average salt consumption in these families was about 10 g/day. DFS provided about 10 mg of iron/day and bridged the existing gap in iron intake/day. Use of DFS for 12 months resulted in a small but significant improvement of the mean Hb in men, women and children. These data suggest that mean Hb is the appropriate parameter for assessing the impact of public health interventions such as DFS on all family members.
The reduction in prevalence of anaemia following 12-month use of DFS was relatively small. This is to be expected because, a rise in Hb of 0.3-0.5 g/dL will change the status only of those anaemic persons whose Hb values were < 0.5g/dl from cut-off for anaemia. Therefore, changes in prevalence of anaemia in any group is not a suitable parameter for assessing the impact of public health intervention such as DFS.
It is reassuring to note that following use of DFS for 12 months the improvement in mean Hb was higher in anaemic women and men. This is likely to be due to the fact that absorption and utilization of the iron from DFS might be higher in anaemic and/or iron deficient persons. There was no change in the mean Hb in non-anaemic persons, indicating that the iron metabolism in humans is so regulated that a small increase in iron intake improves the Hb in anaemic persons, but does not alter Hb levels in the non-anaemic person. Continued use of DFS beyond one year resulted in further improvement in Hb levels. These data suggest that in India, DFS use might be the feasible affordable and sustainable strategy for improving Hb levels and reaching the SDG targets of achieving 50% reduction in the anaemia in WRA.
In recent years there had been concerns that persons with adequate iron intake consuming one or more iron fortified foodstuff may incur risk of iron overload and its potential adverse impact on health status. The gap between EAR and Tolerable Upper Limit (TUL) in iron is quite narrow and excretory path for iron has not been defined. It is therefore, essential that multiple food stuffs fortified with iron do not reach the consumer. To prevent the possibility of excess iron intake from multiple iron fortified food stuffs, it is essential to ensure that no other food stuff is fortified with iron if DFS becomes universally available and used.
ANAEMIA AND INFLAMMATION
Research studies based on the data from a recent national survey in India in which Hb, ferritin and CRP were measured, have reported an association between anaemia and inflammation as assessed by CRP levels in children and adolescents. Persistent inflammation can have adverse impact on iron absorption but is likely to be associated with gastrointestinal symptoms. Anaemia, high ferritin and high CRP levels have been reported in adults with obesity, diabetes and chronic ill health. Most of these data were from cross-sectional studies; therefore, it was not possible to assess whether the association was causal or casual.
In our study both at 0 and at 12 months prevalence of anaemia and over-nutrition was high; inflammation as assessed by CRP was seen in about 1/5th of the women. Data from our longitudinal study showed that persistent inflammation (defined as CRP ≥ 5mg/L both at 0 and at 12 months in women) was not associated with lower mean Hb or higher prevalence of anaemia in women. These data suggest that in the group of women studied there was no association between anaemia and persistent inflammation (CRP ≥ 5mg/L).
FERRITIN FOR ASSESSMENT OF IRON STATUS
Available global data indicate that in nutritional anaemia, iron deficiency is the most common nutritional deficiency. Assessment of dimensions, distribution and severity of iron deficiency is useful in deciding the need for public health intervention to reduce iron deficiency and monitor the impact of the intervention. After reviewing the global data, WHO recommended that ferritin, the primary iron-storage protein secreted in small amounts into the blood circulation is a good marker of iron stores and should be used to diagnose iron deficiency in otherwise apparently healthy individuals (strong recommendation, low certainty of evidence). The WHO provided age specific cut-off values of ferritin for diagnosis of iron deficiency in different age groups. The WHO has recommended that prevalence of anaemia and iron deficiency in communities should be used for assessing the need for public health interventions to improve Hb and iron status of the population.
Data from the present study showed that prior to the initiation of the intervention:
- mean ferritin level in women was 34.5 ng/ml and in men 101 ng/ml;
- the differences in Hb levels between men and women was small but the differences in mean ferritin levels between men and women was large; and
- prevalence of iron deficiency (ferritin <15 ng/ml) was 30% in women but <5% in men.
It is well documented that iron deficiency may precede anaemia and prevalence of iron deficiency increases with decrease in Hb. It was surprising to note that in our study iron deficiency (ferritin level <15 ng/ml) was seen only in one-third of women. There was a gradient in the mean ferritin level in relation to Hb level; there was a progressive reduction in mean ferritin in men and women with reduction in Hb, and increase in prevalence of iron deficiency in women with decrease in Hb. These data suggest that there was a relationship between anaemia and low ferritin levels both in men and women and prevalence of iron deficiency is higher in anaemic women.
The low prevalence of iron deficiency in men might be because WHO cut-off for ferritin (<15 ng/ml) to define iron deficiency is the same for men and women despite the large differences in ferritin levels between men and women. There is a need to undertake studies to assess optimal cut-off point for ferritin to define iron deficiency in men in countries with high prevalence of anaemia and iron deficiency in men.
Available limited data from under-five children indicate that ferritin cut-off of <12 ng/ml for defining iron deficiency, works well in under-five children. There is a need to investigate and document age related changes in ferritin levels in 5-19-year girls and boys, assess the age from which the difference in ferritin levels between sexes begin; such a database is needed to provide age and sex specific cut-off points to define iron deficiency in children especially for the vulnerable adolescent girls.
IMPACT OF INTERVENTION ON FERRITIN
Use of DFS for 12 months resulted in a small but significant increase in the mean ferritin both in women and men; the reduction in prevalence of ferritin <15 ng/ml was statistically significant in women. Mean ferritin provides some information on iron status in groups of women at any given time and improvement in iron status following specific interventions as assessed by mean ferritin prior to and after intervention. The improvement in mean ferritin was higher in women who had ferritin <15 ng/ml prior to use of DFS, suggesting that anaemic and iron deficient women respond with greater increase in Hb and ferritin after 12-month use of DFS. These findings are similar to the finding that improvement in Hb is higher in anaemic women. Mean ferritin level prior to and after intervention is a good indicator to assess the impact of the intervention. Data from the present study showed that paired data on ferritin levels in individuals at enrolment and after 12 months use did not show any consistent trend and therefore cannot be used to assess improvement in iron status over time in the individual. This is because ferritin levels are determined by dynamics between absorption, transport, storage and utilisation of iron at the time of blood collection; the dynamics may be different at enrolment and at 12 months of use of DFS.
EFFECT OF INFLAMMATION ON FERRITIN
In normal healthy persons without any inflammation, the concentration of ferritin is positively correlated with the size of the total body of iron stores. Ferritin levels are high during inflammation in children with or without infection, obesity and chronic ill health. High ferritin levels due to inflammation should not be mistaken for iron sufficiency. To prevent this WHO recommended that CRP should be concurrently measured along with ferritin; if CRP is ≥5 mg/L ferritin concentration below 30 ng/ml in children and 70 ng/ml in adults may be considered to indicate iron deficiency (conditional recommendation, low certainty of evidence).
Men and women who participated in this study were apparently healthy and did not have any overt infection at the time of blood drawing. However, prevalence of over-nutrition was high both in women (50.3%) and in men (44%); this might be related to the reported high CRP levels. Further studies are needed to assess the inter-relationship between over-nutrition and high CRP levels in communities with high prevalence of anaemia, iron deficiency and over-nutrition.
Irrespective of the CRP levels over a third of women had ferritin levels <15 ng/ml. In men ferritin <15 ng/ml is rare irrespective of the CRP levels. These data suggest that ferritin with or without CRP assay cannot be used for assessing iron deficiency in men. Use of cut-off point of 70 ng/ml for ferritin for defining iron deficiency in women with CRP ≥ 5mg/L in women was not useful in our community settings because very few women with CRP ≥ 5mg/L had ferritin levels of ≥ 70 ng/ml.
WAY FORWARD
Data from the present study indicate that valuable information about usefulness of Hb, ferritin and CRP in assessing the need for and impact of interventions to improve Hb and iron status can be obtained by re-analysis of data from research studies and surveys. India is undertaking large scale national surveys in representative samples of population in which Hb, ferritin, CRP, folic acid and Vit B12 estimations are being done. Data from these surveys can be analysed to find out the concordance between the findings reported in the present study and findings at regional, urban-rural, income category levels. Numerous research studies on management of anaemia in different groups report on impact of intervention using Hb, ferritin, CRP, folic acid and Vit B12 estimations. These data can be analysed to assess usefulness of Hb and other parameters to assess impact of intervention at individual and group level. With such an effort it may be possible to build up India specific evidence base required for assessing micronutrient deficiencies rapidly.
Five decades ago, clinicians and haematologists based their assessment of predominant micro-nutrient deficiency responsible for anaemia and the response to treatment on the number and morphological changes in RBCs. There has been a revival of interest in using these RBC based indices for assessment of micro-nutrient deficiencies in anaemic individuals. It may be worthwhile to assess, feasibility, availability, accuracy and cost of bio-markers-based assessment of micro-nutrient status and RBC number and morphology-based assessment of micro-nutrient status in prevention and management of anaemia in different settings in India.
Conclusion
In the urban low middle income families investigated, anaemia was a severe public health problem in women, men and children.
There was substantial difference in ferritin levels between men and women. Both in men and women, there was a progressive reduction in the mean ferritin with decreasing Hb level suggestive of increase in iron deficiency with reduction in Hb. Iron deficiency (ferritin < 15 ng/ml was a moderate public health problem in women but not in men. There is a need to reassess the cut-off level of ferritin for assessing iron deficiency in men in countries where anaemia and iron deficiency are common.
In view of the high prevalence of anaemia both in men and women and iron deficiency in women, DFS use as a public health intervention for improving iron intake of the entire family was warranted.
Hb was the best parameter for:
- detection of anaemia in an individual,
- assessment of the prevalence and severity of anaemia in women, men and children,
- assessment of impact of DFS use on Hb in anaemic and non-anaemic persons.
Data from our longitudinal study failed to show any association between anaemia and persistent inflammation (as assessed by CRP ≥ 5 mg/L both at 0 and at 12 months). Ferritin <15 ng/ml was useful for detection of iron deficiency prior to salt use, and impact of DFS in women but not in men. Mean ferritin levels in groups of women provide information on impact of intervention on iron status.
Irrespective of the CRP levels over a third of women had ferritin levels <15 ng/ml both at 0 and at 12 months. Majority of women with CRP of ≥ 5mg/L had ferritin level <70 ng/ml. Irrespective of CRP levels majority of men had ferritin level beyond 70 ng/ml and prevalence of ferritin <15ng/ml was less than 5%. These data indicate that concurrent CRP estimation with ferritin was not useful in detection of iron deficiency in women or men.
Conflict of interest: None
Funding statement: The analysis of data and preparation of the manuscript was funded by Nutrition Foundation of India.
Acknowledgement: The authors gratefully acknowledge permission given by Nutrition Foundation of India to undertake this analysis.
References
- World Health Organisation. Anaemia. www.who.int. Published 2021. https://www.who.int/data/nutrition/nlis/info/anaemia
- World Health Organization. Anaemia. World Health Organization. Published February 10, 2025. https://www.who.int/news-room/fact-sheets/detail/anaemia
- GBD 2021 Anaemia Collaborators. Prevalence, years lived with disability, and trends in anaemia burden by severity and cause, 1990-2021: findings from the Global Burden of Disease Study 2021 [published correction appears in Lancet Haematol. 2023 Oct;10(10):e796. doi: 10.1016/S2352-3026(23)00283-1.] [published correction appears in Lancet Haematol. 2024 Jan;11(1):e10. doi: 10.1016/S2352-3026(23)00373-3.]. Lancet Haematol. 2023;10(9):e713-e734. doi:10.1016/S2352-3026(23)00160-6
- Anemia – Level 1 impairment | Institute for Health Metrics and Evaluation. www.healthdata.org. https://www.healthdata.org/research-analysis/diseases-injuries-risks/factsheets/2021-anemia-level-1-impairment
- Ramachandran P. Prevention and management of Anaemia in Pregnancy in India: Challenges and Opportunities. Kalaivani K, ed. Medical Research Archives. 2023;11(9):1-14. doi:https://doi.org/10.18103/mra.v%2011i9.4404
- Organization WH. Haemoglobin concentrations for the diagnosis of anaemia and assessment of severity. iriswhoint. Published online 2011. https://iris.who.int/handle/10665/85839 accessed on 23.3.2025
- Guideline on haemoglobin cutoffs to define anaemia in individuals and populations. www.who.int . Published March 5, 2024. https://www.who.int/publications/i/item/9789240088542 accessed on 23.3.2025
- United Nations. The 17 Sustainable Development Goals. United Nations. Published 2015. https://sdgs.un.org/goals
- SDG midterm review: what have we learned from implementation to date? How can we fast-track progress? | High-Level Political Forum 2022. Un.org. Published 2022. Accessed April 4, 2025. https://hlpf.un.org/2022/programme/sdg-midterm-review-what-have-we-learned-from-implementation-to-date-how-can-we-fast
- WHO guideline on use of ferritin concentrations to assess iron status in individuals and populations. www.who.int. https://www.who.int/publications/i/item/9789240000124
- Serum and red blood cell folate concentrations for assessing folate status in populations. www.who.int. https://www.who.int/publications/i/item/WHO-NMH-NHD-EPG-15.01
- Garcia-Casal MN, Pasricha SR, Martinez RX, Lopez-Perez L, Peña-Rosas JP. Serum or plasma ferritin concentration as an index of iron deficiency and overload. Cochrane Database of Systematic Reviews. 2021;5(5). doi:https://doi.org/10.1002/14651858.cd011817.pub2
- Ramachandran P, Prabhakar K, Kumari H, Kalaivani K. Impact of the use of iron-fortified iodized salt on haemoglobin levels: a community based open randomized trial. Published online June 2023:2197-2207. doi: https://dx.doi.org/10.18203/2394-6040.ijcmph20231703
- Weiss G, Ganz T, Goodnough L. Anaemia of inflammation. Blood. 2019;133(1):40-50.
- MoHFW. Prophylaxis against nutritional anaemia among mothers and children 1970 Technical Information, MCH No. 1 New Delhi
- K Ramachandran Prevention & management of anaemia in pregnancy: Multi-pronged integrated interventions may pay rich dividends Indian J Med Res 2021:154 (1) 12-15
- Kalaivani K Ramachandran P Hb estimation at point of care using cyanmethaemoglobin method Int J Community Med Public Health. 2021 8(9):4498-4505
- Prema Ramachandran and K Kalaivani Prevalence of Anaemia in India and Strategies for Achieving Sustainable Development Goals (SDG) Target Proc Indian Natn Sci Acad 2018 84 (4) 899-912
- MOHFW. Anaemia Mukht Bharat Intensified National Iron Plus (I-NIPI) initiative and POSHAN Abhiyaan. Ministry of Health and Family Welfare, Government of India. April, 2018. accessed on 23.3.2025 https://resources.anemiamuktbharat.info/Awareness_Generation/Anemia-Mukt-Bharat-brochure
- Pramanik A, Kalaivani K, Ramachandran P. Food security and dietary intake in pregnant women from urban low income group. The Indian Journal of Nutrition and dietetics. 2021;58(2):161-173. doi:https://doi.org/10.21048/IJND.2021.58.2.27088
- Ramachandran P, Prabhakar K, Kumari H, Kalaivani K. Impact of use of iron fortified iodised salt beyond 12 months on haemoglobin level. International Journal of Community Medicine and Public Health. 2024;11(2):835-840. doi:https://dx.doi.org/10.18203/2394-6040.ijcmph20240274
- Ramachandran P. Food Fortification: A Public Health Approach to Bridge the Gap Between Requirement and Intake of Micro-nutrients. Proceedings of the Indian National Science Academy. 2018;84(4):913-922.
- Kurpad A, Ghosh S, Thomas T, Bandhyopadhyay S. When the cure might become the malady: the layering of multiple interventions with mandatory micronutrient fortification of foods in India. American Journal of clinical Nutrition. 2021;00:1-6.
- Sarna A, Porwal A, Ramesh S, Agarwal PK. et al Characterisation of the types of anaemia prevalent among children and adolescents aged 1-19 years in India: a population-based study. Lancet. 2020;4(7):515-525.
- MOHFW, UNICEF, Population Council Comprehensive National Nutrition Survey National Report New Delhi 2019
- Chandra et al J. Diagnosis, Treatment and Prevention of Nutritional Anemia in Children: Recommendations of the Joint Committee of Pediatric Hematology Oncology Chapter and Pediatric and Adolescent Nutrition Society of the Indian Academy of Pediatrics. Indian Pediatrics. 2022;59(10):782-801.