

Autogenous Tooth-Derived Grafts in Bone Regeneration
Autogenous Tooth-Derived Graft Material in Alveolar Bone Regeneration: A Clinical and Histological Assessment
Lanka Mahesh, BDS, MBA, PhD ¹, Gregori M. Kurtzman, DDS ² and Nikita Gulati, MDS ³
¹ Private practice New Delhi, India
[email protected]
² Private practice Silver Spring, Maryland, USA
[email protected]
³ ITS Dental College, Department of Oral Pathology, Ghaziabad, UP, India
[email protected]
OPEN ACCESS
PUBLISHED: 31 August 2025
CITATION Mahesh, L., et al., 2025. Autogenous Tooth-Derived Graft Material in Alveolar Bone Regeneration: A Clinical and Histological Assessment Medical Research Archives, [online] 13(8). https://doi.org/10.18103/mra.v13i8.6785
COPYRIGHT © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI: https://doi.org/10.18103/mra.v13i8.6785
ISSN: 2375-1924
Abstract
Autogenous tooth-derived graft materials have recently emerged as a novel option in alveolar bone regeneration due to their biocompatibility, osteoconductive and osteoinductive properties. This study evaluates the clinical and histological outcomes of using processed extracted teeth as bone graft material during immediate implant placement. The results support that tooth-derived grafts are effective in socket preservation and promote bone regeneration comparable to traditional graft materials.
Keywords
autogenous graft, tooth-derived graft, alveolar bone regeneration, histological assessment, implant placement
Introduction
Bone grafting is a critical component of maxillofacial, periodontal, and dental implant surgery. Conventional grafting materials, including autografts, allografts, xenografts, and synthetic alternatives.[1,2] These offer good osteoinductive and osteoconductive capacities but suffer some risk of negative host response. Synthetic materials are an alternative graft material which offers osteoconductive capacities and can be supplied in unlimited quantities. Alternative graft materials including allografts, xenografts, and alloplastic bone grafts are clinically used, but they have disadvantages such as they lack osteoproliferation and have high material cost and limited osteoinductivity. Development of an alternative graft material that surpasses those limitations is desired. Extracted human teeth, often discarded as clinical waste, possess a mineral and organic composition similar to alveolar bone, making them a promising alternative for autogenous grafting[3,4]. Utilization of the patients own extracted tooth eliminates the potential for immunological reactions that may occur when utilizing other grafting materials whether allograft, xenograft or synthetic. Recent advancements have enabled the processing of extracted teeth into sterile, particulate graft material using devices such as the Smart Dentin GrinderTM (KometaBio, Tenafly, NJ, USA). This approach eliminates immunogenic reactions and capitalizes on the inherent bioactivity of dentin, rich in collagen and non-collagenous proteins[5-7].
Methodology
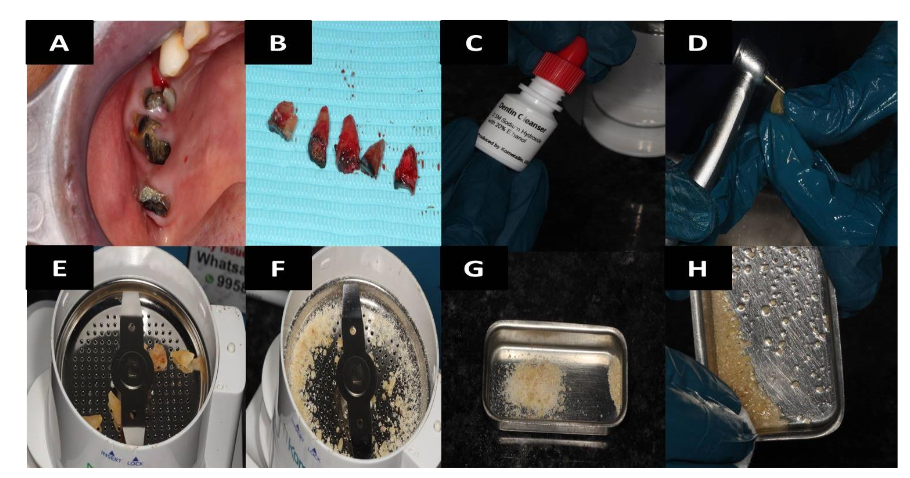
Freshly extracted teeth were processed using a Smart Dentin Grinder (KometaBio, NJ, USA) to produce sterile particulate dentin. Teeth with root canal fillings were excluded due to contamination risk. Also, teeth with restorative materials should not used for grinding. After being cleaned with an air syringe, the teeth are put in a sterile grinding chamber of the Smart Dentin GrinderTM. The tooth was ground into particles using the dentin grinder machine. The particles were then saturated for 10 minutes in a dentin cleanser solution (sodium hydroxide solution mixed in 20% ethanol); this was followed by a phosphate buffered saline wash, resulting in a bacteria-free, autogenous graft material ready for implantation. In addition to grinding the roots in 3 seconds, this device can produce particles smaller than 1200 µm in 20 seconds by shaking the grinding chamber. After passing through a sieve to a lower chamber, particles that are 300 1200 µm in size and appropriate for regeneration are submerged in basic alcohol for ten minutes in a sterile glass container. 30% alcohol (v/v) and 0.5M NaOH make up a basic alcohol cleaning, which is used to defatten and dissolve all organic debris, bacteria, from dentin particles. Alveolar bone deficiencies can be grafted with this wet particulate dentin. The dentin graft material was hydrated and immediately used in sockets post-extraction followed by Rapiplug collagen plug. Soft tissue closure was achieved, and patient was recalled at 2 weeks for suture removal. Further, he was recalled at 3 months for clinical and histological evaluation. Core biopsies were taken using a trephine bur (3.2mm Koine Italy) and sent for histological analysis, Osteotomies were created at the sites and MIS implants of 4.2mm x10mm (Dentsply, Sirona, Charlotte, NC, USA) were inserted.
Histological Analysis
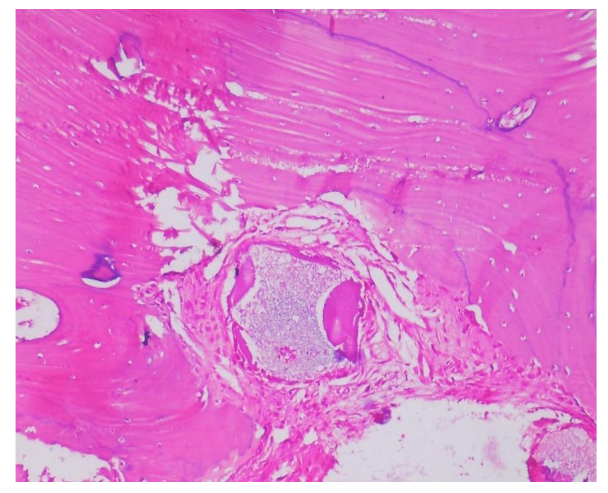
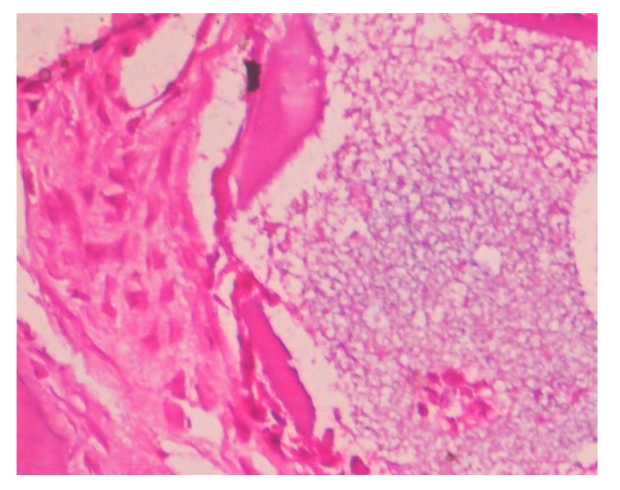
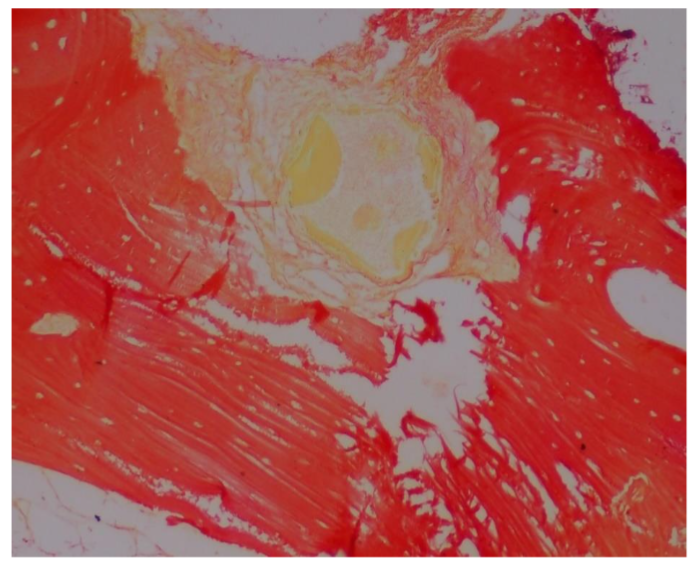
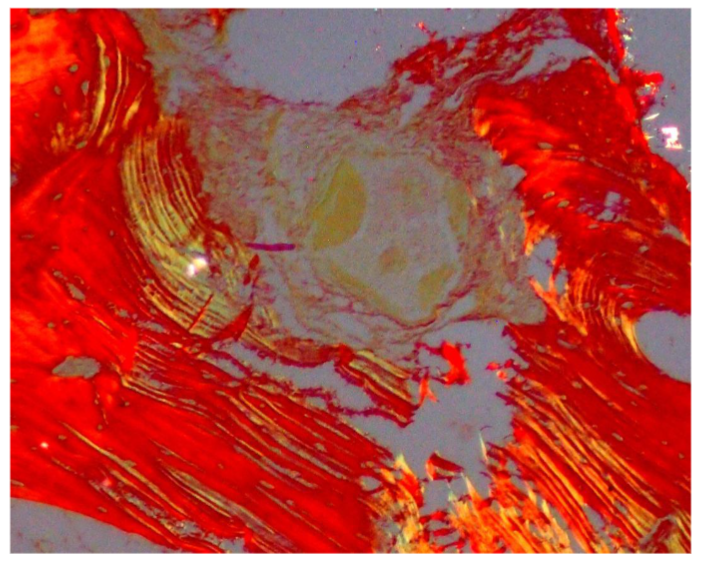
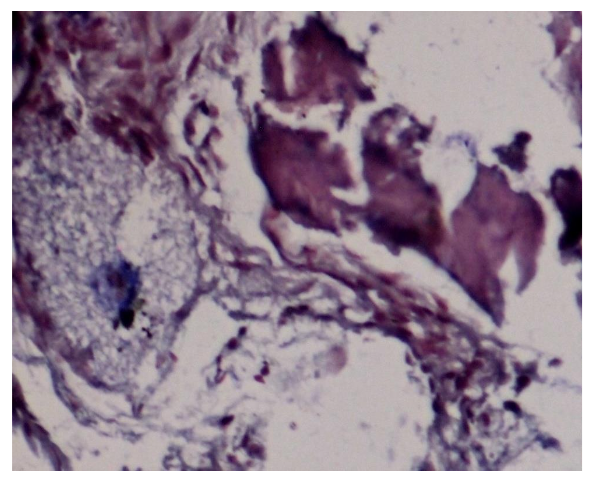
Biopsies were fixed in 10% formalin, decalcified with 0.5M EDTA, and sectioned. Hematoxylin and eosin (HE), Van Geison, Mason trichrome and Picrosirius Red were used. Microscopic analysis revealed remnants of dentin particles integrated with new lamellar bone. Plump osteoblasts, entrapped osteocytes, and fibrovascular stroma with minimal chronic inflammation were evident, confirming osteoconductive and osteoinductive potential. Mature bone trabeculae along with residul graft material were confirmed with various special stains.
Discussion
Dentin and bone share similar composition: collagen (20%), hydroxyapatite (70%), and fluid (10%)[8]. The dentin matrix contains proteins like dentin phosphoprotein (DPP) and dentin sialoprotein (DSP) crucial in mineralization[6,7]. Demineralized dentin matrix (DDM) has demonstrated enhanced biocompatibility and osteoinductivity akin to demineralized bone matrix[9,10]. In comparative studies, human dentin grafts matched autogenous bone grafts in resorption and bone regeneration capabilities[11]. Tooth-derived grafts have shown higher crystallinity than bone but require time-consuming demineralization. Despite this, fresh demineralized tooth (FDT) has exhibited promising regeneration outcomes. In a study by Kim et al., autogenous tooth grafts showed progressive resorption with replacement by trabecular bone at 6 months[13]. Autogenous dentin grafting is a viable option for use in the treatment of osseous defects, eliminating potential immunological reactions that may present with osseous graft materials that are commercially available.[14,15] Additionally, histological analysis has demonstrated in multiple studies that autogenous dentin converts to host bone during the healing process.
For osteoconduction, the presence of differentiated mesenchymal cells is essential, which requires an adequate blood supply. Histologically, large bone particles show less vascularity compared to small graft particles. Smaller particles provide more surface area, promoting the release of growth factors, encouraging angiogenesis, and accelerating the differentiation of mesenchymal cells into osteoblasts. It is important to note that studies referenced have used various graft materials at different anatomical sites, indicating that the regenerative potential is both particle-type and site-dependent. However, there is no large case series assessing a single graft type across multiple sites to determine the most suitable particle size for each indication.
Inter-particle spacing is another critical factor. Research suggests that a minimum space of 100 µm between particles is necessary, with optimal bone formation observed at 300 500 µm spacing. This is influenced by the porous structure of the graft, which significantly affects osteoconduction and synostosis. Studies have shown that materials with high porosity positively influence bone formation. Two types of pore sizes have been studied: <5 µm (micropores) and >100 µm (macropores). Micropores increase the surface area, while macropores facilitate material resorption, osteogenesis, and vascular infiltration. Interconnected macropores are particularly important for vascularization, cell migration, and the diffusion of pro-osteogenic factors.
Rapiplug collagen (Dalim Tissen Inc., Seoul, Korea) is a resorbable, type I collagen-based wound dressing commonly used in dental and oral surgical procedures, especially in guided tissue regeneration (GTR) and guided bone regeneration (GBR). It is typically derived from bovine or porcine sources and is available in plug or sheet forms, designed for easy placement into extraction sockets or bone defects. Rapiplug naturally resorbs over time, usually within 4 to 6 weeks, which eliminates the need for a second surgical intervention for removal. Clinically, Rapiplug is used in various procedures including socket preservation after tooth extractions, where it helps stabilize the blood clot and maintain soft tissue architecture. It also serves as an effective barrier in GTR/GBR procedures by preventing epithelial migration and allowing bone-forming cells to repopulate the defect. Additionally, it is frequently used to cover bone grafts, helping to stabilize the graft material and protect the site from contamination. One of the key advantages of Rapiplug is its haemostatic property, as collagen promotes platelet aggregation, aiding in early bleeding control. It is highly biocompatible, integrating well with host tissues and inducing minimal immune response. Its soft, pliable texture makes it easy to trim and adapt to different anatomical sites, and it supports healing by providing a scaffold for cellular ingrowth and angiogenesis.
Conclusion
Tooth-derived autogenous grafts offer a safe, cost-effective, and biologically favourable alternative to traditional grafting materials. They leverage the osteoconductive and osteoinductive potential of dentin, with excellent clinical and histological outcomes. Further longitudinal and large-scale studies are required to validate their use in routine clinical practice.
References:
- Aghaloo TL, Moy PK. Which hard tissue augmentation techniques are the most successful in furnishing bony support for implant placement? Int J Oral Maxillofac Implants. 2007;22(Suppl):49-70.
- Sheikh Z, et al. Bone replacement materials and techniques used for achieving vertical alveolar bone augmentation. Materials. 2015;8(6):2953-2993.
- Kim YK, et al. Tooth-derived bone graft material. J Korean Assoc Oral Maxillofac Surg. 2013;39(3):103-111.
- Murata M. Autogenous demineralized dentin matrix for maxillary sinus augmentation in humans: the first clinical report. J Dent Res. 2013;92(12):1138-1143.
- Kim YK, et al. Histological study of demineralized tooth and bone matrix grafts. Implant Dent. 2014;23(3):331-336.
- Nampo T, et al. A new method for alveolar bone repair using extracted teeth. J Periodontol. 2010;81(9):1264-1272.
- Bessho K, et al. Human dentin matrix as a scaffold for bone morphogenetic protein-induced bone formation. J Biomed Mater Res. 1991;25(10):1303-1311.
- Tziafas D, et al. Odontoblast-like cell differentiation in dog pulp cultures by allogenic dentin matrix. Arch Oral Biol. 1995;40(10):941-950.
- Bang G. Histopathological studies of the pulpal response to calcium hydroxide-containing cements. J Dent Res. 1967;46(5):1034-1042.
- Gomes MF, et al. Dentin matrix for alveolar bone tissue engineering: a systematic review. J Appl Oral Sci. 2017;25(5):551-558.
- Al-Asfour A, et al. Comparison of demineralized dentin graft and autogenous bone graft for onlay bone grafting in a rabbit model. Int J Oral Maxillofac Implants. 2013;28(5):e236-e243.
- Zitzmann NU, et al. The volume stability of autogenous bone grafts. Clin Oral Implants Res. 2001;12(6):559-565.
- Kim YK, et al. Evaluation of autogenous tooth bone graft material for socket preservation. J Korean Assoc Oral Maxillofac Surg. 2013;39(3):103-111.
- Kuperschlag A, Kerytė G, Kurtzman GM, Horowitz RA. Autogenous Dentin Grafting of Osseous Defects Distal to Mandibular Second Molars After Extraction of Impacted Third Molars. Compend Contin Educ Dent. 2020 Feb;41(2):76-82; quiz 83. PMID: 32017585.
- Horowitz RA, Kurtzman GM. Improving the Prognosis of Periodontally Involved Teeth at the Time of Extraction of Adjacent Teeth With an Amnion-Chorion Barrier and Bioactive Dentin Graft. Compend Contin Educ Dent. 2024 Jul-Aug;45(7):e1-e4. PMID: 39029967.