





Awareness of Malaria Re-establishment in Sri Lanka
Awareness on malaria among healthcare providers and public during the prevention of re-establishment phase in Sri Lanka
Hamsananthy, J¹ and Wickremasinghe A R²
- Ministry of Health and Mass Media, Sri Lanka
- Department of Public Health, Faculty of Medicine, University of Kelaniya, Sri Lanka
OPEN ACCESS
PUBLISHED: 31 January 2025
CITATION: Hamsananthy, J., and Wickremasinghe, A.R., 2025. Awareness on malaria among healthcare providers and public during the prevention of re-establishment phase in Sri Lanka. Medical Research Archives, [online] 13(1). https://doi.org/10.18103/mra.v13i1.6213
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i1.6213
ISSN 2375-1924
ABSTRACT
Introduction
Prevention of re-establishment of malaria is a challenge for Sri Lanka due to the country’s high receptivity and importation risk. As imported malaria cases are being reported, awareness on malaria among both healthcare providers and the public is crucial to anticipate a resurgence and re-establishment of malaria in the country.
Objectives
The objective of this study was to assess the awareness on malaria among healthcare providers and the public during the prevention of re-establishment phase immediately after “malaria-free” certification by the World Health Organization (WHO).
Methodology
Two national surveys were conducted among 766 healthcare providers and 3454 households in 2016/17. Healthcare providers’ survey was conducted using stratified random sampling and administering a self-administered questionnaire. The household survey was conducted using multistage cluster sampling method. A marking scheme was developed and adjusted binary logistic regression analysis was used to assess the association between awareness and socio-demographic and economic factors, using IBM SPSS version 20 statistical software package.
Results
The mean score for awareness on malaria among healthcare providers was 54.7% (SD=10.6%) and the heads of households was 28.6 % (SD = 9.03%). Awareness among healthcare providers was significantly associated with the sector of the institution, type of institution, but not with ever seen a malaria case. For the heads of households, awareness was significantly associated with age group, family income/wealth quintile, sector of residency, ever heard about malaria, seen/heard messages about malaria in the past 6 month and had been overseas within the last 3 years.
Conclusions and recommendations
The awareness on malaria among healthcare providers and public in Sri Lanka is poor during the prevention of re-establishment phase. Awareness programmes should be conducted for both public and healthcare providers to keep malaria on the radar through television, mobile phones and newspapers. Updates about malaria should be regularly conducted for healthcare providers.
Key words: Awareness on malaria, Public, Healthcare providers, Prevention of Re-establishment of malaria, Sri Lanka
Introduction
Exactly 50 years after a missed opportunity to eliminate malaria, Sri Lanka reached a milestone in its malaria history. In September 2016, Sri Lanka was certified as a “malaria-free” country by the World Health Organization (WHO). The expansion of development projects, business, tourism, industry, and the influx of foreign labour and refugees from neighbouring malarious countries combined with the continued presence of malaria vectors in formerly endemic areas make the country receptive with a high importation risk threatening the prevention of re-establishment of malaria programme. As long as areas remain receptive, importation of parasites may lead to outbreaks. In addition, malaria has become a forgotten disease among health staff and the community resulting in delayed diagnosis which, in turn, increases the chance of the spread of the disease in the community. Therefore, even after elimination has been achieved, continued interventions are required to prevent re-establishment of malaria in the country¹.
The milestone achievement of malaria elimination in Sri Lanka is the result of a dedicated effort by health staff and the commitment of successive governments through adoption of favourable health policies and sustaining an effective public healthcare system free-of-charge. Improvement of living standards, housing, sanitation and road access have also contributed to this success. To sustain this achievement, there are threats in the form of receptivity and importation risk. The presence of the vector mosquitoes that can transmit malaria and the newly invaded mosquito vector species Anopheles stephensi is a major risk for re-establishment of malaria in the country². The influx of infected persons from malaria endemic countries increases importation risk³.
Many imported malaria cases have been reported since 2009, among both foreign and Sri Lankan nationals returning from malaria endemic countries. An introduced malaria case was reported December 2018, as a result of local transmission. With good surveillance and a rapid response, transmission was confined to a single case of malaria⁴. A case of transfusion-induced Plasmodium falciparum malaria was reported in April 2021. A 17-year-old splenectomized beta thalassaemia patient developed an infection following a blood transfusion 18 days earlier. The blood donor was armed-forces personnel who returned from South Sudan following a United Nations peace-keeping mission and both were successfully treated without further transmission⁵.
As there has been no indigenous malaria case reported since November 2012, the capacity to suspect malaria during a febrile illness has waned among healthcare providers. Even to suspect malaria after hospitalization in some instances has taken a long time. In a study performed during 2012 showed that clinician’s awareness of malaria was unacceptable, resulting in delayed diagnosis even up to one month after onset of fever. Evaluation of the malaria elimination programme in 2013 found that, referral by medical practitioners for a malaria diagnosis remain persistently low even though the diagnostic facilities were available¹.
A systematic review on knowledge, attitudes and beliefs about malaria among the South Asian population suggests the importance of increasing health awareness, mobilizing the local or community healthcare professionals for prevention as well as early detection, and effective treatment of malaria among people who are at risk⁶. Both public and healthcare professionals’ awareness is needed to prevent re-establishment of malaria so that events will not be allowed to repeat as happened in the past in Sri Lanka.
Every year, World Malaria Day is celebrated on 25ᵗʰ April to emphasize the collective energy and commitment of the global malaria community in uniting around the common goal of a world free-of-malaria⁷. The aim of this study was to assess the awareness on malaria among healthcare providers and the public during the prevention of re-establishment phase immediately after “malaria-free” certification by WHO.
Methods
STUDY SETTING
Sri Lanka is an island nation in the Indian Ocean, southeast of India, with a total land area of 65,610 km2. The population of Sri Lanka is approximately 22 million, a large proportion resident in rural areas⁸. Administratively, Sri Lanka is divided into 9 provinces, and the 9 provinces are further divided into 25 districts. The Medical Officer of Health (MOH) is responsible for preventive health services in a defined area. The MOH area is further divided into Public Health Inspector (PHI) and Public Health Midwife (PHM) areas⁹.
STUDY POPULATION, SAMPLE SIZE AND SAMPLING
Two cross sectional surveys were conducted among healthcare providers and heads of households, covering the whole country.
HEALTHCARE PROVIDERS’ SURVEY
The study population in the healthcare providers’ survey included all government sector medical officers, medical officers in leading private hospitals in the districts and general practitioners. The target population comprised medical officers working in all government healthcare institutions (curative and preventive care services) in 9 Provincial Director of Health Services (PDHS) offices, 25 Regional Director of Health Services (RDHS) offices, 22 Regional Malaria Offices (RMO) and Anti Malaria Campaign Headquarters (AMC HO), 621 medical institutions with in-patient facilities, 487 Primary Medical Care Units and 337 MOH offices. Medical officers include house officers, senior house officers and consultants in preventive, curative as well as administrative sectors.
The proportion of health care providers having good awareness on prevention of re-establishment of malaria was taken as 50% for the sample size calculation. The margin of error was taken as ranging from 47 to 53 % for a 95% confidence interval; the sample size was corrected for a 10% non-response rate (as it included independent medical practitioners as well). Hence, the required sample size was 1067.11*100/90≈1186. Healthcare providers were selected by stratified random sampling according to the type of institution. Two healthcare providers from each government institution were enrolled in the study. Two leading private hospitals were selected from each district and three medical officers were selected from the outpatient clinics on the day of visit. Ten general practitioners (GPs) were randomly selected from each district from the list that include the Independent Medical Practitioners Association (IMPA) registered healthcare providers and the list from the GP registers maintained at the regional offices of the Anti-Malaria Campaign and its headquarters.
HOUSEHOLD SURVEY
The study population consisted of heads of the households in all districts of Sri Lanka. One or more persons living together and who have a common arrangement for provision of food in a housing unit was included as a household¹⁰. Public places like home for elders, orphanages, and religious homes were excluded.
For the sample size calculation to assess awareness on malaria among the general public, the number of Sri Lankans travelling overseas was considered as the most important variable. In 2014, 1,311,258 Sri Lankans departed from the Bandaranaike International Airport, which was about 6% of the estimated population¹¹. Therefore, to estimate the proportion of Sri Lankans travelling overseas in a year as 6%, with a margin of error ranging from 4.5 to 7.5% for a 95% confidence interval, assuming a design effect of 3.2 for using cluster sampling (cluster size of 12), and a non-response rate of 10%, a sample of 3424 households had to be surveyed¹². Households were selected equally from among the 25 districts proportionate to population in urban, rural and estate sectors. Therefore, from each district 137 households had to be surveyed from 11.4 clusters per district. Hence, twelve clusters of 12 households from each cluster were randomly selected from each district (25 districts × 12 PHM clusters × 12 households) to give a total sample size of 3600 households.
A stratified multistage cluster sampling method was used with the primary sampling unit being MOH areas. 6–8 MOH areas were randomly selected from each district. 12 PHM area clusters were randomly selected from the selected MOH areas (on average 2 PHM clusters per MOH area). From each PHM area cluster, the starting point of the household survey was randomly selected by dropping a headed pin on the PHM area map and the house closest to the pointed edge was selected. After the first house was identified, every tenth house to the left of the selected house was chosen until 12 households for that PHM area were surveyed¹³.
DEVELOPMENT OF THE DATA COLLECTION TOOL
The healthcare providers’ questionnaire was a self-administered questionnaire, comprising information on the healthcare provider’s general profile and 21 questions related to awareness on possibility of re-establishment of malaria in Sri Lanka. The awareness questions covered different aspects of malaria, ranging from clinical case information, signs and symptoms, transmission, prophylaxis, investigation, diagnosis, treatment and notification as well as the measures for the prevention of re-establishment of malaria in the country.
The household survey questionnaire was an interviewer administered questionnaire, comprising identification of households including socio demographic characteristics of household members, and household characteristics to assess socio-economic status (SES). The assessment of SES was based on the Demographic Health Survey (DHS) format used worldwide¹⁴. Wealth index was used to classify the socio-economic status of participants. The source of water, toilet facilities, type of fuel used, material used for the floor of the house, mode of transport, access to mass media, electricity in the household, possession of some household items, and ownership of agricultural land and farm animals were included in the questionnaire. The migration history of household members within the last 3 years and history of fever prior to two weeks of survey were included. To assess awareness on malaria, eleven questions were included. The questions ranged from sources of malaria information, signs and symptoms of malaria, transmission, prevention as well as the current situation of malaria in the country.
VALIDATION OF TOOL
Questionnaires were distributed among malaria experts to assess judgmental validity (face and content) of the questionnaire. The questionnaires were translated using standard methods and pre-tested in the field; necessary changes were made accordingly. The reliability of the questionnaires was assessed by test-re-test reliability using the kappa statistics, and internal consistency using Cronbach’s alpha. The kappa statistics of 0.863 (P<0.001) for healthcare providers’ questionnaire and 0.736 (P<0.001) for household questionnaire indicated good and excellent agreement¹⁵. The Cronbach’s alpha values of 0.926 for the healthcare providers’ questionnaire and 0.888 for the household awareness questionnaire indicated good and excellent agreement¹⁶.
DATA COLLECTION
The validated tool was used in the household survey in all districts of the country. The public health field officers of the Anti-Malaria Campaign were trained on sampling technique and the importance of sampling during the training sessions; in the field they were supervised by malaria officers or the principal investigator. An interviewer manual and a Global Positioning System (GPS) data collection format were prepared based on the guidelines for conducting Malaria Indicator Surveys as given by the Roll Back Malaria Initiative; this was given to all data collectors for easy reference. Fieldwork was carried out from July 2016 to March 2017.
The PHM of the area informed the heads of selected households about the survey and the date of interview. On the assigned date, data collectors visited the households and interviewed the head of the household. If the head of the household could not be interviewed (e.g. household closed), the next
closest household was selected. If the head of the household had responded and was not available at the time of survey, the contact number was obtained; the household head was approached a second time, after confirmation of his/her presence, mainly during weekends. If the second attempt failed, the house was visited for a third time; if the head of the household could not be contacted a third time, it was considered a non-responder.
Data collection was supervised by regional malaria officers, medical officers attached to Anti Malaria Campaign/Headquarters and the principal investigator. Each healthcare provider was personally contacted by RMO/Medical officers. Questionnaires were given after brief explanation of the study. Most of the healthcare providers returned the filled questionnaire on the same day. For some healthcare providers, questionnaires were obtained after two/three visits. Another proportion did not return the questionnaire or had misplaced the questionnaire.
DATA ANALYSIS
Descriptive analyses were used to describe socio-demographic characteristics. Socio-economic status of the population was assessed by the wealth index using exploratory factor analysis. Principal components analysis (PCA) was used to generate a weighted score based on household assets. The wealth index for a household is the linear combination defined as the principal component variable across households or individuals with a mean of zero and a variance of one, corresponding to the “Eigenvalue” of the correlation matrix. The estimated wealth index was based on a population of 13,365 resident in 3,454 households located in all districts in Sri Lanka. The variables selected for derivation of the wealth index were based on the methodology used by the Department of Census and Statistics of Sri Lanka in their routine surveys (DHS)¹⁷ and in the guidelines to conduct a Malaria Indicator Survey¹⁸.
Descriptive analyses were used to describe variables, with proportions and 95% confidence interval. The awareness score for each healthcare provider and head of the household was marked according to the marking scheme. The questions were marked out of a maximum possible score of 100%. The total score for healthcare provider questionnaire was 60 and that for the head of the household was 30. The awareness score was converted to percentages and categorized into two using the median as the cutoff value for binary logistic regression analyses.
The association between awareness on malaria with wealth index, sector of residency and history of migration was analyzed using multivariable analyses. The binary logistic regression model was used with awareness (using the median score as the cutoff point) as the dependent variable to identify factors associated with awareness using age (categorized into 3 groups as <5 years, 6–35 years, 35–65 years, and >65 years), wealth index (categorized into three groups as wealth quintiles 1 and 2, wealth quintiles 3 and 4, and wealth quintile 5) and sector of residency.
Data analysis was done using IBM SPSS statistics version 20 software package.
ETHICS APPROVAL AND CONSENT TO PARTICIPATION
Ethics clearance (protocol number EC-16-089) was obtained from the Faculty of Medicine, University of Colombo. Written consent for voluntary participation was obtained before data collection. Permission to conduct the study was obtained from the Provincial Directors of Health Services and the Regional Directors of Health Services, local government authorities, Medical Officers of Health and heads of institutions.
Results
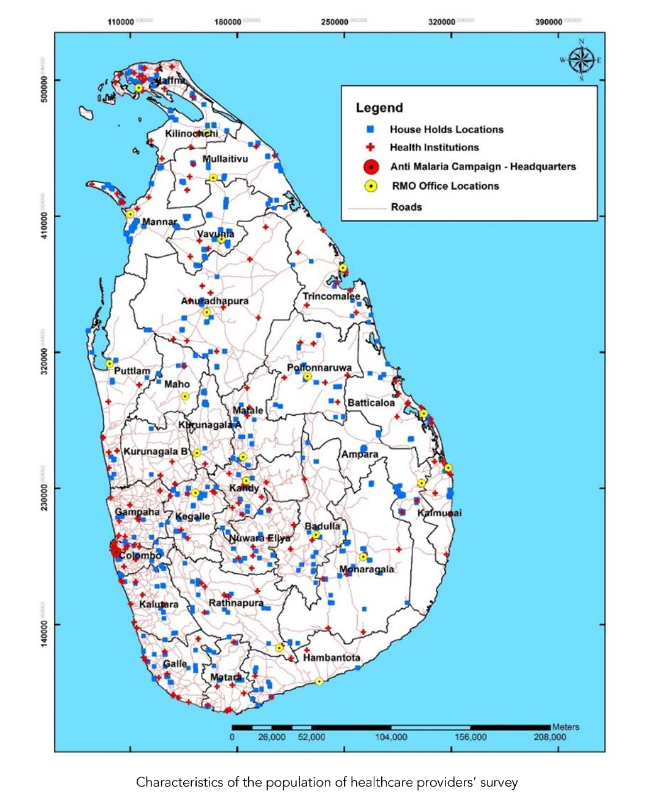
The response rate for the healthcare provider survey was 64.6%, (n=766) and for the household survey was 95.9% (n=3454) within two consecutive visits. Figure 1 shows the geographic distribution of surveyed households and institutions.
Characteristics of the population of healthcare providers’ survey
The median age of the healthcare providers was 40 years (range 23–77 years). The majority of healthcare providers were males (n=474, 61.9%) and Sinhalese (n=595, 77.7%). Around 53% (n=405) were working in urban areas and 71.9% (n=551) had served for more than 2 years. The median duration of services was 8 years (range from one month to 52 years) (Table 1).
The median age of the healthcare providers was 40 years (range 23-77 years). The majority of healthcare providers were males (574, 61.49%) and Sinhalese (n=595, 77.73%). Around 71.9% (n=551) had served for more than 8 years (range from one month to 52 years) (Table 1).
| Variable | Number (%) | 95% confidence interval of percentage |
|---|---|---|
| Age group | <30 years | 128 (16.7) 14.1-19.5 |
| 30-65 years | 474 (61.8) 57.8-65.3 | |
| ≥65 years | 62 (8.1) 5.7-11.4 | |
| Gender | Male | 292 (38.1) 34.3-41.9 |
| Ethnicity | Sinhalese | 494 (64.5) 61.0-68.0 |
| Tamil | 104 (13.8) 11.2-16.2 | |
| Muslim | 65 (8.49) 6.0-10.9 | |
| Other | 2 (0.26) 0.0-0.7 | |
| Institution area | Urban | 448 (58.9) 54.9-62.8 |
| Rural | 302 (39.4) 31.6-48.5 | |
| Type of institution | Curative sector Base Hospital and above | 79 (10.3) 7.1-13.6 |
| Curative sector below Base Hospital | 220 (28.7) 25.1-32.4 | |
| Hospital | 79 (10.3) 7.1-13.6 |
The mean awareness percentage score calculated according to the marking scheme was 54.7% (SD-10.6%, range 5.0% to 85.0%, median 55%). Around 17% (n=132) of healthcare providers had ever seen/diagnosed/treated malaria cases during the past 5 years. The majority (>65%) knew the symptoms of malaria; 99.1% stated that fever is a symptom of malaria. Table 2 shows the awareness on malaria among healthcare providers by question.
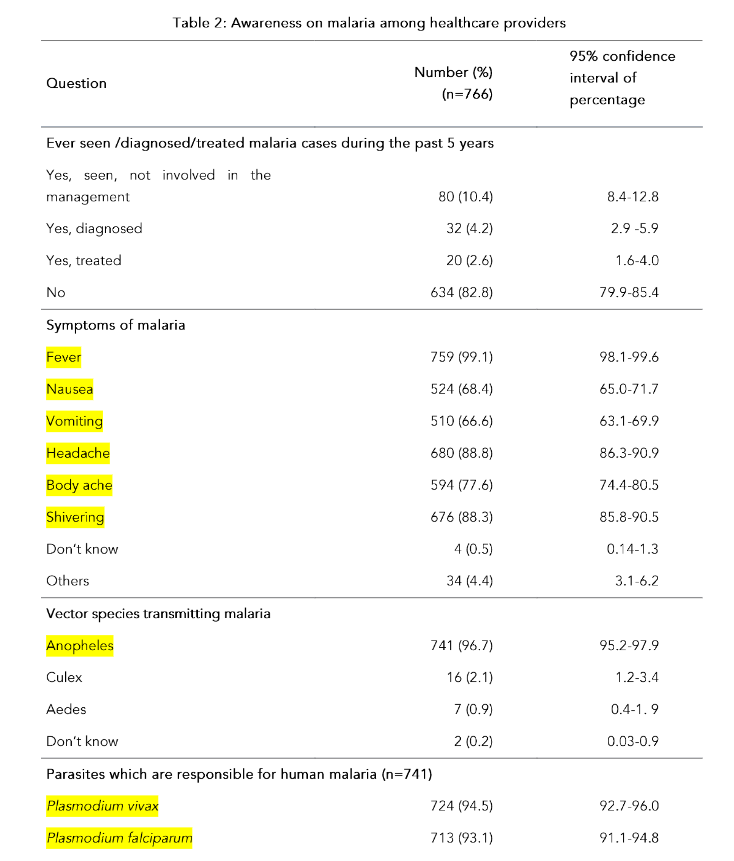
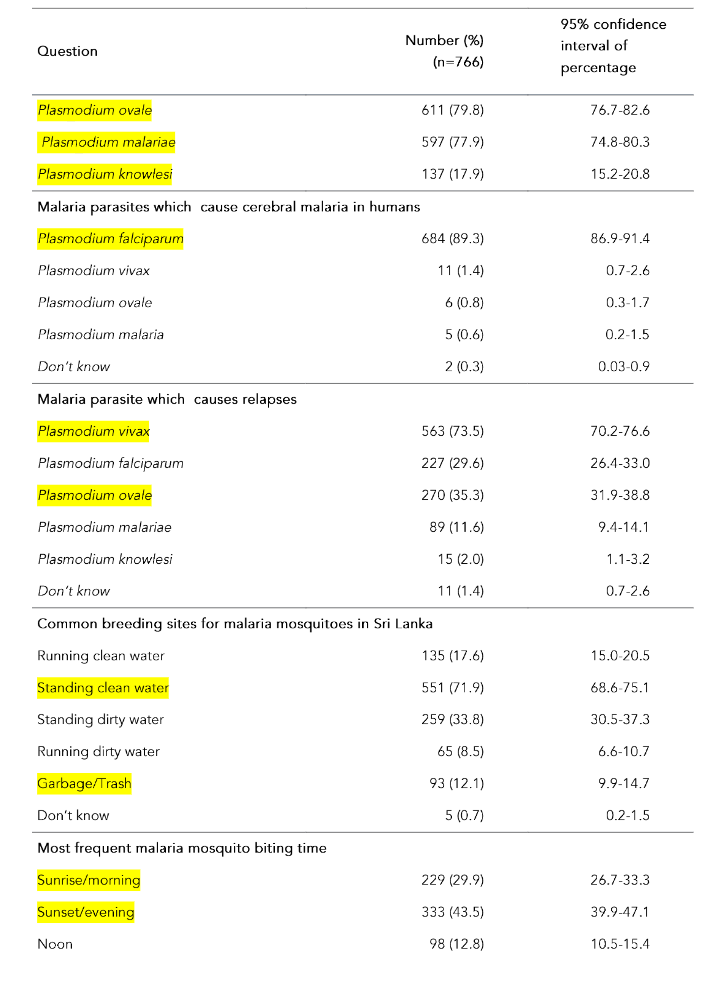
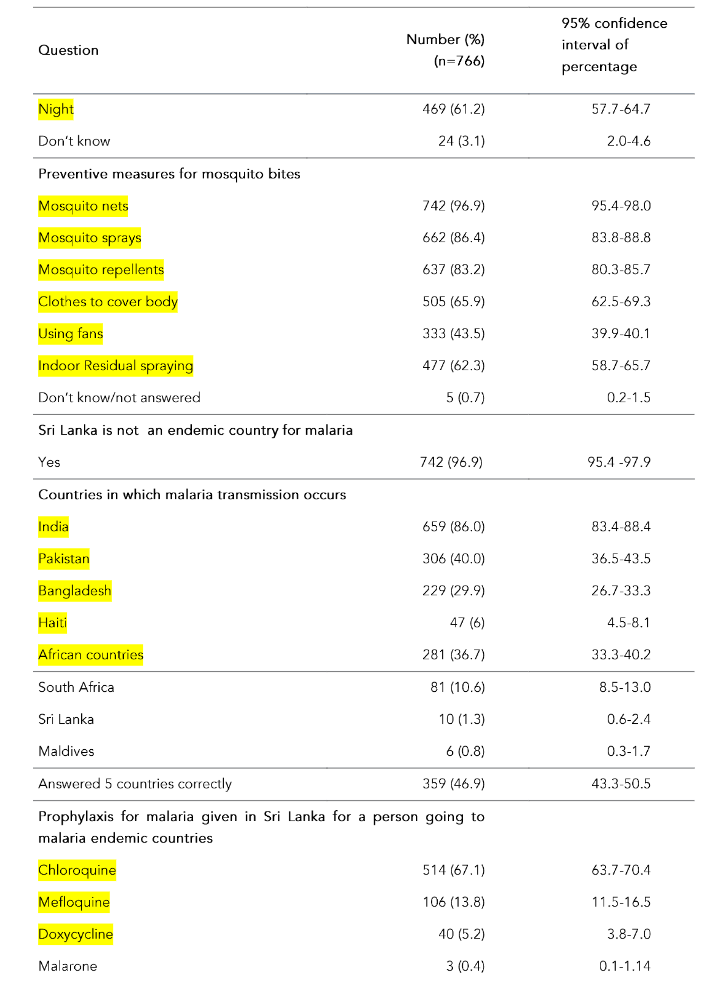
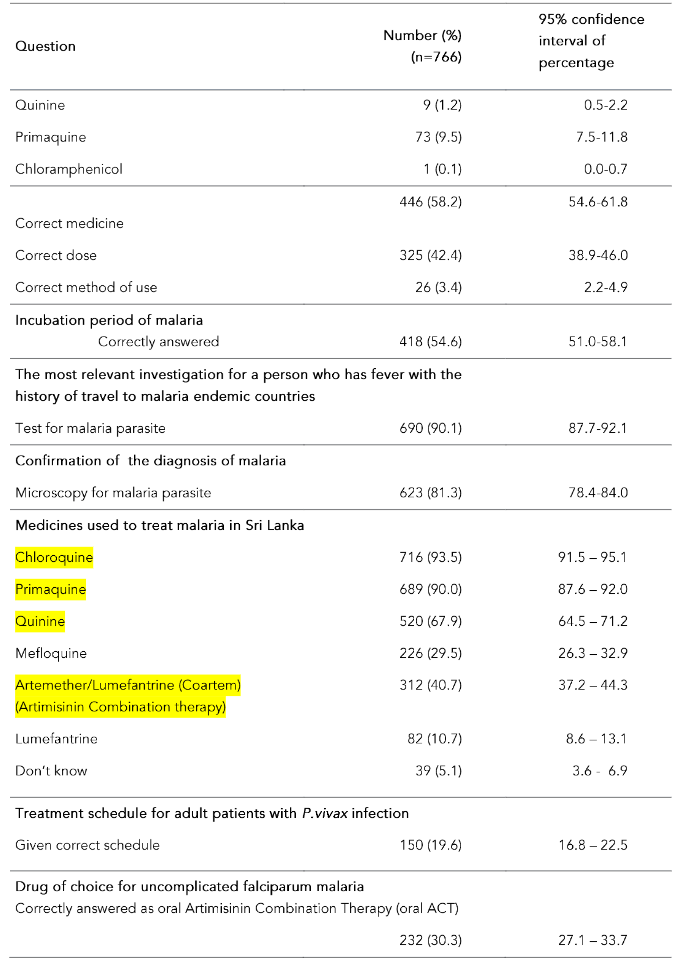
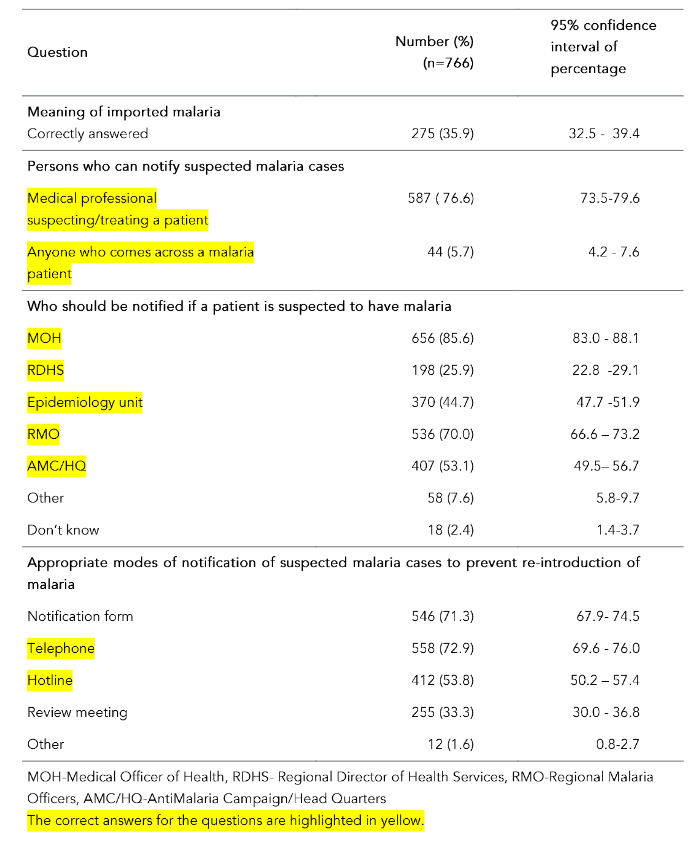
Table 2: Awareness on malaria among healthcare providers
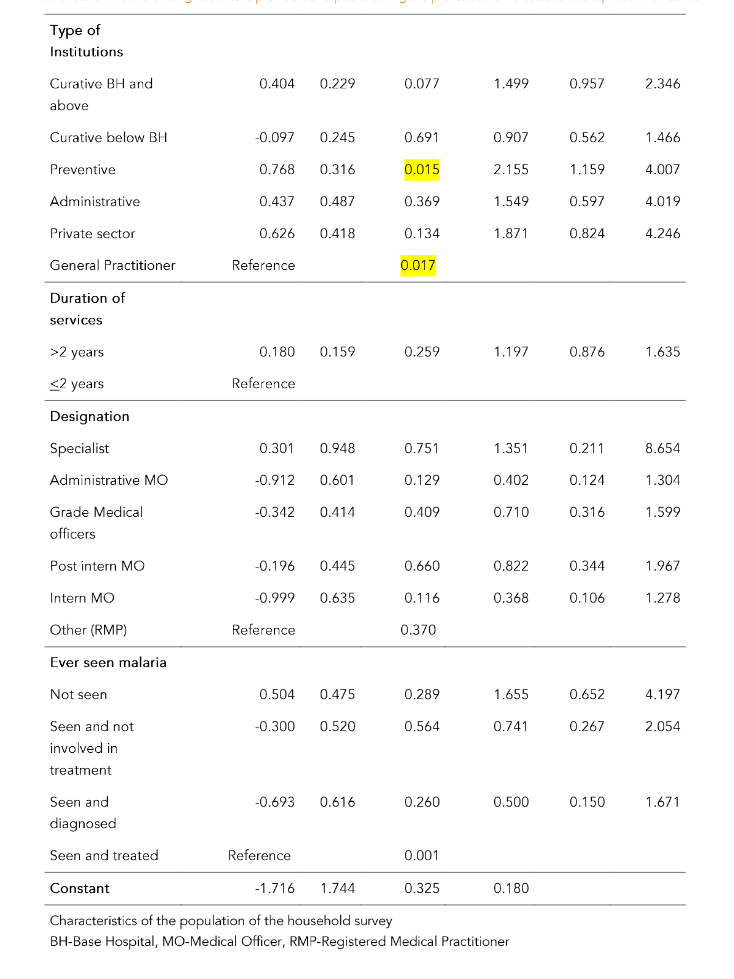
The association between the awareness and the socio demographic factors was assessed by binary logistic regression analysis, based on the awareness score more or less than the median, as the dependent variable adjusted for independent variables age, gender, ethnicity, institutional area, type of institution, duration of service, designation and ever seen a malaria case. Awareness was significantly associated with the area of the institution (urban/rural/estate) and the type of institution. Those who worked in urban and rural sector health care institutions were 3.5 times (OR=3.5, 95%CI: 1.1–11.6) and 4.4 times (OR=4.4: 95% CI; 1.3–14.2) more likely to have better awareness on malaria than estate sector healthcare providers after controlling for other variables. Those who worked in the preventive sector were 2.2 times (OR=2.2, 95% CI: 1.2–4.0) more likely to have better awareness on malaria than those working in other sectors adjusted for other variables. Ever seen a malaria case was not significantly associated with better awareness on malaria among healthcare professionals (Table 3).
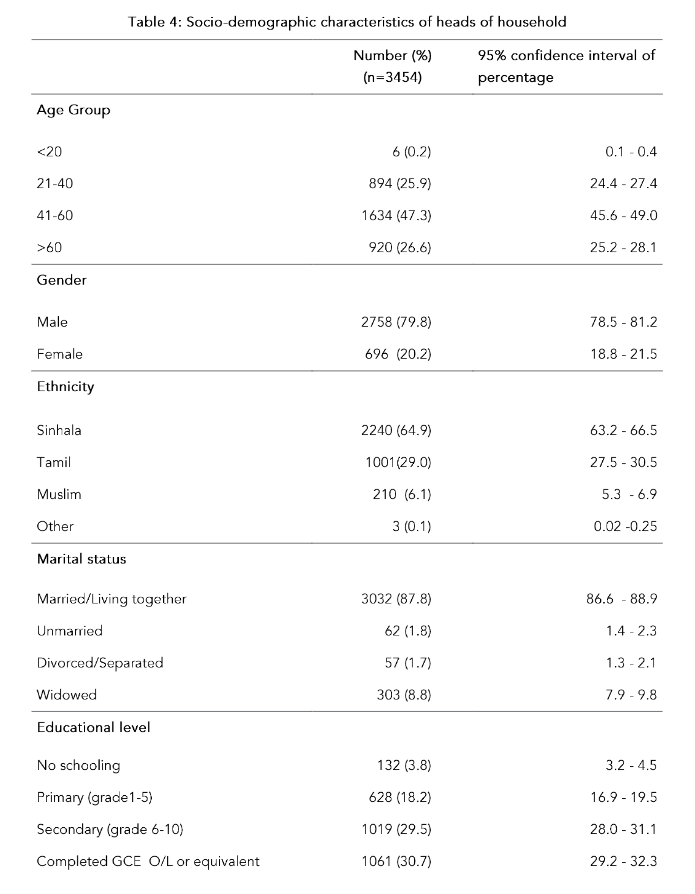
The mean age of the heads of household was 51 years (SD=13.9; range 19–92 years). The majority of the heads of households were males (n=2758, 79.8%) and Sinhalese (n=2240, 64.9%). The majority of households was from the rural sector (n=2,685, 77.7%) and had access to television (n=2714, 78.6%); almost 65% of household members had access to a mobile telephone (n=2242, 64.9%) (Table 4).
Table 4: Socio-demographic characteristics of heads of household
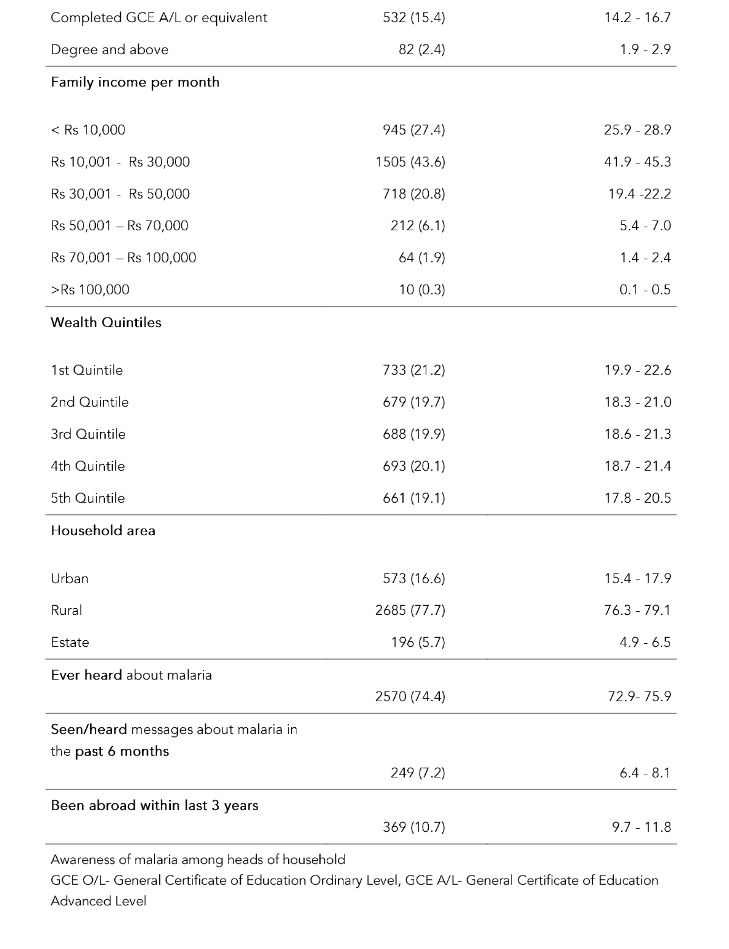
The mean awareness score calculated according to the marking scheme was 28.6% (SD = 9.03%; range 3.3% to 63.3%; median 26.7%). Table 5 shows the awareness on malaria among heads of the households according to each question. Although 74.4% (n=2570) of heads of households had ‘ever heard about malaria’ in the past, only 7.2% (n=249) had seen/heard messages about malaria in the past 6 months. The majority of them (n=149, 59.8%) had seen/heard messages about malaria through newspapers. Majority of heads of households (71.8%, n=2479) stated that fever is a symptom of malaria and 23.9% (n=824) stated that shivering is a symptom of malaria. The majority (92.7%, n=3202) knew that malaria is spread by a mosquito bite (Table 5).
Table 5: Awareness of malaria among heads of households
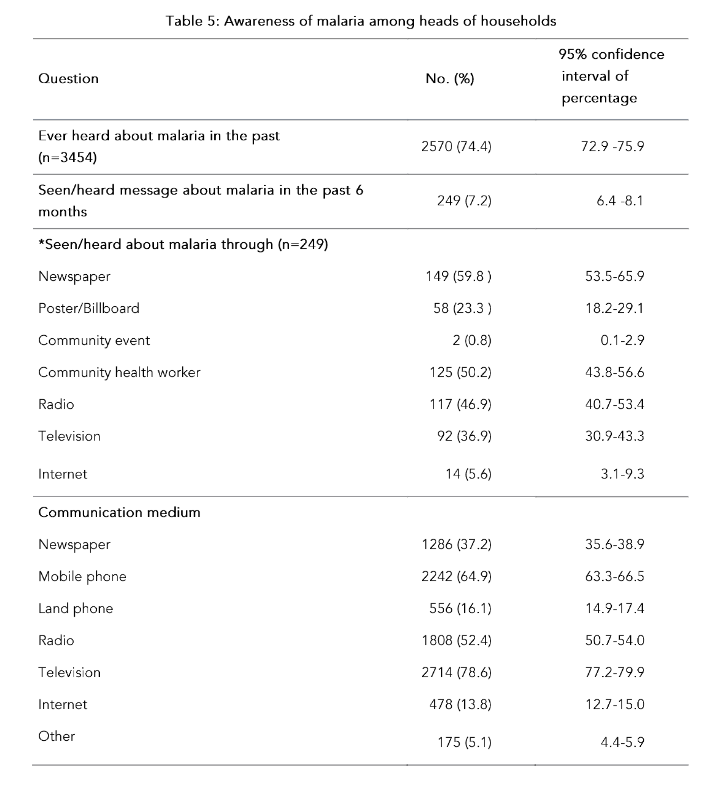
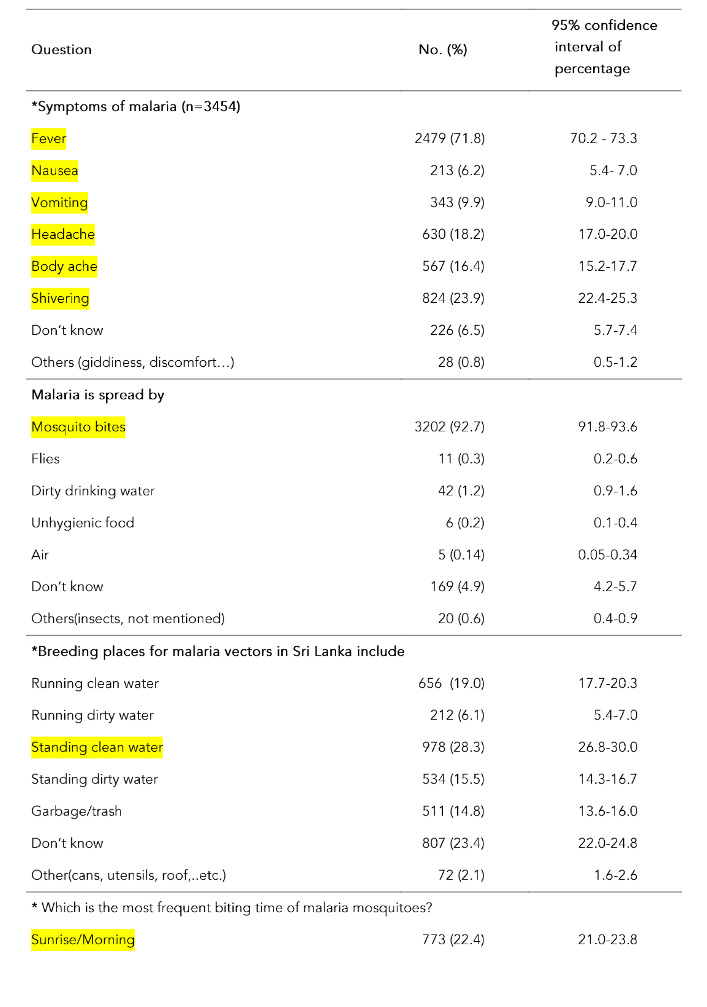
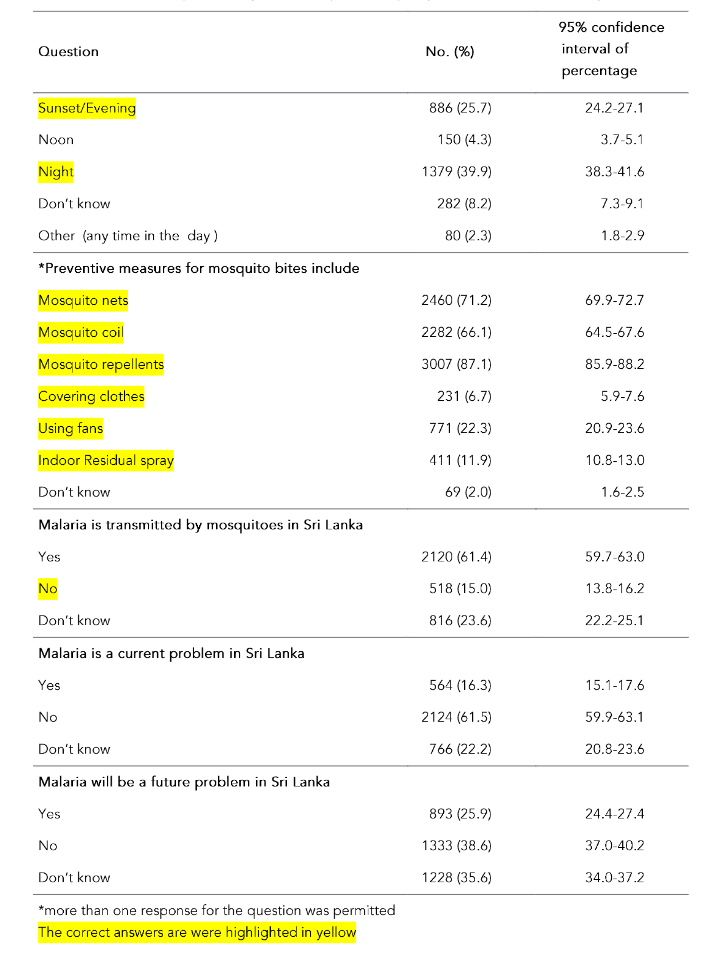
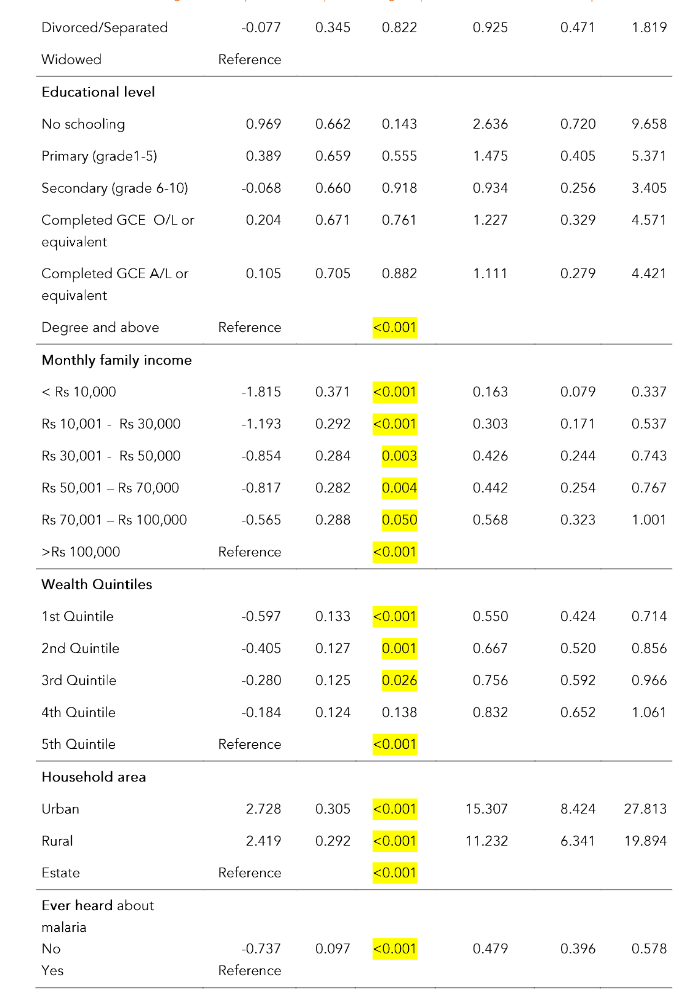
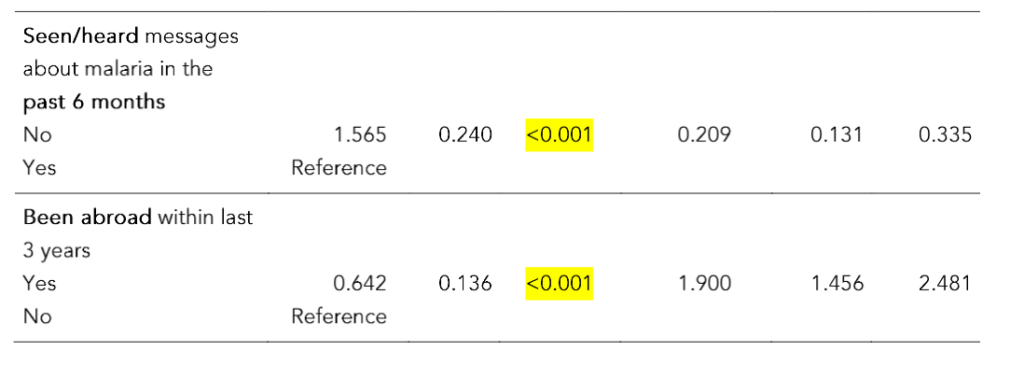
Table 6 shows the results of the binary logistic regression model using the awareness score categorized into two based on the median as the cutoff as the dependent variable adjusted for the independent variables age, sex, ethnicity, marital status, educational level, family income wealth quintile, household area, ever heard of a malaria case or message about malaria and been abroad within the last 3 years. Awareness was significantly associated with age group and family income/wealth quintile. Higher family income/wealth quintile population were more aware of malaria than the lower family income/wealth quintile populations.
Those who were in urban and rural sector had 15 times (OR=15.3; 95% CI of OR: 8.4–27.8) and 11 times (OR=11.2; 95% CI of OR: 6.3–19.9) more likelihood of having better awareness on malaria than those resident in the estate sector, respectively. Ever heard about malaria and seen/heard messages about malaria in the past 6 months was significantly associated with awareness on malaria among heads of households. Those who had been overseas within the last 3 years were 1.9 times (OR=1.9; 95% CI of OR: 1.5–2.5) more likely to have better awareness on malaria than the others.
Table 6: Results of logistic regression analysis using awareness on malaria of heads of households and their socio-demographic characteristics
| β | S.E. | Sig. | Adjusted OR (Adjusted Exp(β)) | 95% confidence interval of adjusted OR (adjusted(Exp(β))) Lower | Upper | |
|---|---|---|---|---|---|---|
| Age group | ||||||
| ≤20 | -0.637 | 1.107 | 0.565 | 0.529 | 0.060 | 4.628 |
| 21–40 | -0.279 | 0.121 | 0.022 | 0.757 | 0.596 | 0.960 |
| 41–60 | 0.041 | 0.096 | 0.671 | 1.042 | 0.863 | 1.256 |
| >60 | Reference | 0.015 | ||||
| Gender | ||||||
| male | 0.045 | 0.116 | 0.700 | 1.046 | 0.833 | 1.312 |
| Female | Reference | |||||
| Ethnicity | ||||||
| Sinhala | -0.247 | 0.742 | 0.739 | 0.781 | 0.182 | 3.345 |
| Tamil | -0.294 | 0.742 | 0.692 | 0.745 | 0.174 | 3.189 |
| Muslim | -0.520 | 0.761 | 0.494 | 0.594 | 0.134 | 2.642 |
| Other | Reference | 0.438 | ||||
| Marital status | 0.081 | |||||
| Married/Living together | 0.297 | 0.162 | 0.067 | 1.346 | 0.979 | 1.848 |
| Unmarried | -0.257 | 0.323 | 0.427 | 0.773 | 0.410 | 1.457 |
Discussion
Awareness on malaria is the level of understanding about the importance and implications of malaria prevention especially in the prevention of re-establishment phase. Raising awareness is not the same as telling them what to do. It is explaining issues and disseminating knowledge to persons so that they can make their own decisions. High public awareness occurs when a significant proportion of society agrees to certain decisions. When public awareness is low, a majority of people do not know or do not care about importation of malaria cases¹⁹. During the prevention of re-establishment phase of malaria in Sri Lanka, a national representative assessment is important to prevent even a single case of indigenous malaria leading to emergence of local transmission with rapid population movement within the country. This study is a national representative assessment on awareness both among the public and healthcare providers of malaria.
The present study shows that the overall awareness score (median 55%) is low among healthcare providers possibly due to the fact that nearly eighty percent of the healthcare providers had not seen, diagnosed or treated a malaria case during the last 5 years. Awareness on malaria is not significantly associated with the selected variables including ever seen malaria. It is only significantly associated with the area (urban/rural/estate) in which the institution is located and type of institution possibly reflecting better access to information in urban and rural sectors as compared to the estate sector. Thus, the suspicion of malaria in the differential diagnosis of fever by healthcare providers might be low even though the majority (>65%) knows the symptoms of malaria and 99.1% answered fever as one of the symptoms.
During the control phase, knowledge and attitudes of Public Health Midwives in the Anuradhapura district, a previously malaria endemic area, were very satisfactory and the responses of younger respondents with a 6–9 year service period were significantly better than those of respondents who were over 40 years with a service period of over 10 years²⁰. In a primary healthcare institution, clinicians’ suspicion of malaria in referring for blood smear examination was no better than patients’ self-diagnosis; the authors surmised that the decision for screening patients by microscopy need not be made by a clinician at the outpatient clinics thus saving clinicians time for more needed services²¹.
A study done during the pre-elimination phase in a resettled population after 30 years of displacement in the Mannar district, reported that the population had good knowledge and practices about malaria; 71% had sought treatment quickly and 67% had access to diagnostic facilities²². Another assessment on the existing knowledge and attitudes among pregnant women and service providers showed gaps in knowledge and attitudes regarding malaria. A health education intervention including focus group discussions was done and recommendations were given to employ the same on a larger scale to improve compliance to chemoprophylaxis²³. In 2008, findings of a study conducted to evaluate the effectiveness of