





B-cell Maturation in AITL: DLBCL Development Insights
B-cell maturation in angioimmunoblastic T cell lymphoma (AITL): Development of secondary diffuse large B cell lymphoma (DLBCL) is likely associated with Attygalle patterns II and III
Yukiko Shishido-Hara¹, Aya Miyagawa-Hayashino², and Junya Kuroda³
- Department of Pathology and Applied Neurobiology, Kyoto Prefectural University of Medicine.
- Department of Surgical Pathology, Kyoto Prefectural University of Medicine.
- Division of Hematology and Oncology, Kyoto Prefectural University of Medicine.
OPEN ACCESS
PUBLISHED: 30 September 2024
CITATION: Shishido-Hara, Y., Miyagawa-Hayashino, A., et al., 2024. B-cell maturation in angioimmunoblastic T cell lymphoma (AITL): Development of secondary diffuse large B cell lymphoma (DLBCL) is likely associated with Attygalle patterns I and III. Medical Research Archives, [online] 12(9).
https://doi.org/10.18103/mra.v12i9.5720
COPYRIGHT: © 2024 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v12i9.5720
ISSN 2375-1924
Abstract
The pathology of an inguinal lymph node, diagnosed as angioimmunoblastic T cell lymphoma (AITL) with secondary development of EB virus (EBV)-related diffuse large B cell lymphoma (DLBCL), is analyzed in detail. The AITL lymph node was divided into three pathological areas, A, B, and C, corresponding to Attygalle Patterns I, II, and III. Development of DLBCL was observed at the areas B-C boundaries, corresponding to Patterns II and III. This likely indicated excessive B-cell maturation by neoplastic follicular helper T (TFH) cells. Although the mechanisms of DLBCL development in AITL are unclear, B-cell maturation is likely enhanced by neoplastic TFH, leading to germinal center disruption. Attygalle’s patterns are important in evaluating both T-cell and B-cell activities.
Keywords
- Angioimmunoblastic T cell lymphoma
- Diffuse large B cell lymphoma
- EB virus
- Follicular helper T cells
Introduction
Angioimmunoblastic T-cell lymphoma (AITL) is a distinctive subtype of peripheral T-cell lymphoma, primarily characterized by the proliferation of neoplastic follicular helper T (TFH) cells within lymph node. The pathological hallmark of AITL involves small to medium-sized neoplastic TFH cells with pale cytoplasm surrounding high endothelial venules (HEVs). The presence of irregular follicular dendritic cell meshwork (FDC-MW) is also a characteristic feature. Its histopathology is relatively divergent, but AITL is often associated with B-cell or plasma cell expansion. The B cells may be atypical and infected with Epstein-Barr virus (EBV).
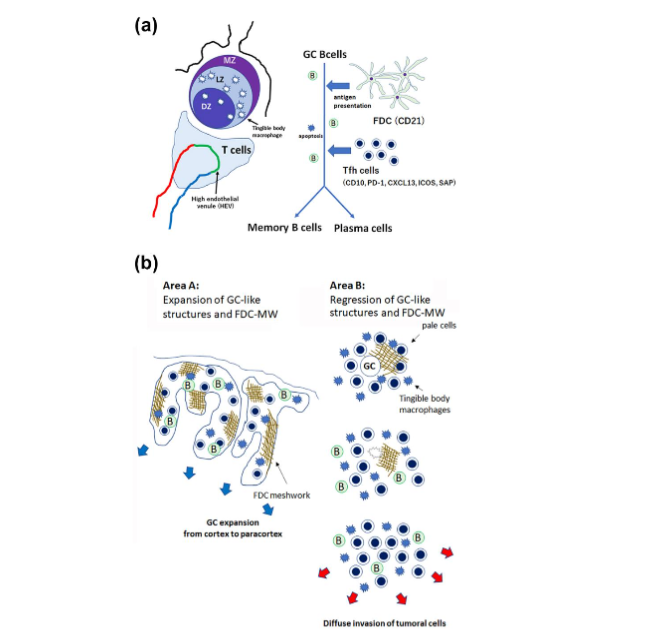
Recent advancements in immunology have elucidated the critical role of heterogeneous TFH cells in facilitating B-cell maturation within germinal centers (GCs). In normal lymph nodes, the TFH cells, through interactions with antigen-presenting follicular dendritic cells (FDCs), are essential in promoting the selection and survival of high-affinity B cells, ultimately leading to their differentiation into memory B cells or plasma cells. In AITL lymph nodes, neoplastic TFH cells may also contribute to B-cell maturation, but their potential functions remain unclarified.
A rare composite B- and T-cell lymphoma exists, and the risks of bidirectional risk of malignancy are poorly understood. DLBCL may occur following AITL, and vice versa. Attygalle et al. previously classified the AITL pathology into three distinct patterns, I, II, and III, each correlating with different disease activities. Pattern I, characterized by an intrafollicular T-zone pattern, is considered indolent. Meanwhile, Patterns II and III, marked by atrophic lymph follicles and almost complete follicular disappearance, are associated with more aggressive disease and poorer prognoses. These pathological AITL patterns may relate to the risks of secondary development of B cell lymphoma, but this is not yet elucidated due to the rarity of composite AITL and DLBCL.
In this report, we examined the expression patterns of B-cell markers in an AITL lymph node that developed secondary EBV-related DLBCL. The study aims to elucidate the influence of neoplastic TFH cells on B-cell maturation, particularly in the context of the histological patterns proposed by Attygalle et al. Understanding the pathological processes may help to elucidate the mechanisms of the development for composite AITL and DLBCL.
Clinical summary
A 57-year-old man was diagnosed as EBV-positive DLBCL after a biopsy of an inguinal lymph node. Chemotherapy of R-CHOP and CHASER 2 was performed, but the disease progressed. The inguinal lymph node was re-examined, and the revised pathological diagnosis was AITL with secondary development of EBV-positive DLBCL. A year after the first diagnosis, he received an allogeneic peripheral blood stem cell transplantation (PBSCT) using a reduced-intensity conditioning regimen with fludarabine/melphalan 140 mg/m2 (Flu/Mel140). However, he passed away on day 114 post-PBSCT due to posttransplant lymphoproliferative disorder (PTLD). In the present report, we focus on the pathology of the inguinal lymph node obtained by biopsy, AITL with secondary DLBCL.
Pathological findings
A biopsy of an inguinal lymph node was performed, but the diagnosis of AITL was not readily reported due to the presence of a relatively large number of EBV-positive atypical B cells. However, when the same lymph node was re-examined, T cell proliferation was evident. Immunohistochemistry (IHC) was performed in use of various antibodies; T cells (CD3, CD4, CD8), B cells (Pax5, CD10, CD20, CD79a, MUM-1), and follicular dendritic cells (CD21) were examined. The lymph node was also evaluated for cell cycle activation with MIB-1 immunostaining, and for EBV infection with EBV-encoded small RNA in situ hybridization (EBER-ISH). Representative six figures (HE, Pax 5, CD20, MUM-1, CD21, EBER-ISH,) are presented in Figure 1. For clearer understanding, the lymph node was roughly divided into three areas, A, B, and C, and the levels of B cell maturation were distinct between the areas. For example, area A displayed distinct expression of Pax 5, CD20, and CD79a, but MUM-1 expression was markedly low. In contrast, in area B, the expression of Pax 5 is low, and the expression of CD20 and CD79a is distinct. MUM-1 expression was also apparent at the marginal region of area B. These observations indicate that B cell maturation is more advanced in area B than in area A.
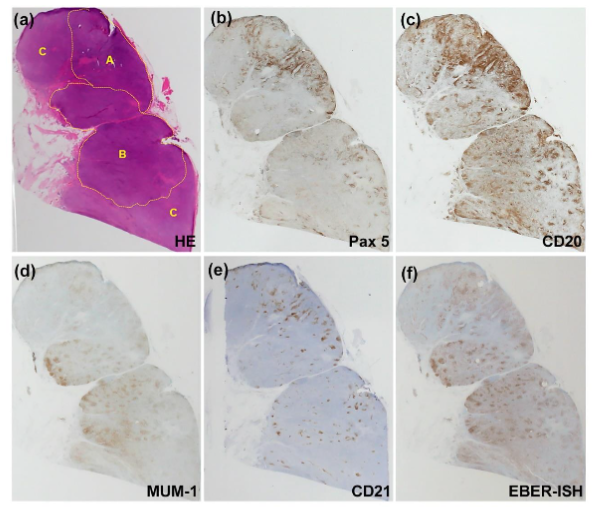
Patterns of follicular dendritic cell meshwork (FDC-MW) were also investigated with CD21 immunostaining. The FDC-MW patterns were distinct between areas A and B. In area A, CD21-positive FDC-MW was expansive, and neoplastic TFH cells coexisted with FDC, surrounding the increased HEVs. In contrast, in area B, FDC-MW was diminished or disappeared, and only atrophic FDC-MW remained at the margin of the lymph node. Area A (with expansive FDC-MW) and area B (with atrophic FDC-MW), respectively, corresponded to AITL patterns I and II-III proposed by Attygalle et al. Previous studies suggested that pattern I (area A) is an indolent lesion, while patterns II-III (area B) is an active AITL lesion. In good agreement, the MIB-1 labeling index was higher in area B, as well as positivity with EBER-ISH. Area C was contiguously located next to area B, but the number of B cells were smaller.
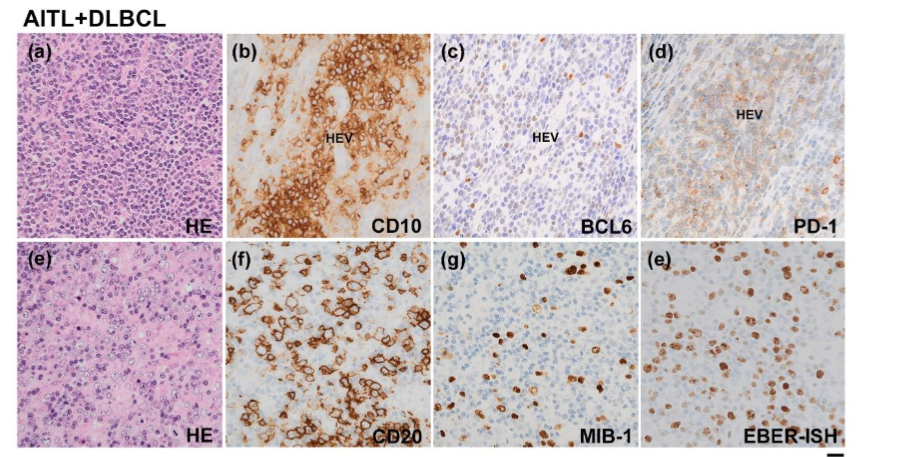
Microscopically, AITL cells were distributed in the entire lymph node. Generally, TFH cells are immunohistochemically defined with positivity of at least two, ideally three, of the following molecules: CD10, BCL6, PD-l, CXCL13, ICOS, and SAP. In the present case, the pale cells clustered around HEVs showed distinctive positivity with CD10 and PD-l and mild to moderate positivity for BCL6. Thus, the pathological diagnosis of AITL was confirmed. At the boundary of areas B-C, a relatively large number of atypical CD20-positive cells were seen. The cells were positive with EBER-ISH and also labeled with MIB-1. Their sheet-like distribution suggested the diagnosis of secondary DLBC. Although DLBCL-like pathology was apparent in the boundary of areas B-C, area A was not involved.
Discussion
This study underscores the relevance of the Attygalle classification in understanding B-cell maturation within AITL lymph nodes, particularly in light of recent advances in molecular pathology and targeted therapies. As noted by Du et al., AITL falls under the broader category of nodal T-follicular helper cell lymphoma (T-FHCL), a subtype of peripheral T-cell lymphomas (PTCLs). The histopathological classification proposed by Attygalle et al. offers a framework for assessing unique features of AITL and may distinguish it from PTCLs. The Attygalle’s Patterns, reflecting the degrees of lymph node destruction, are also important in evaluating the prognosis.
In the present case, the inguinal lymph node was divided into three areas labelled A, B, and C, corresponding to Attygalle’s Patterns I, II, and III, respectively. Histopathological examination revealed that B-cell maturation was more advanced in area B, which exhibited characteristics of Pattern II, compared to area A, which was consistent with Pattern I. Furthermore, the transition from Pattern II to Pattern III was marked by the emergence of DLBCL-like pathology at the interface between areas B and C. This finding highlights the dynamic nature of AITL, where different regions within the same lymph node can represent varying stages of disease evolution, reflecting the underlying heterogeneity in the tumor microenvironment.
These histological observations are consistent with the findings reported by Du et al., who emphasized the importance of molecular markers and genetic mutations in diagnosing and understanding T-FHCL. Specifically, the presence of mutations in genes such as TET2, DNMT3A, and RHOA, commonly seen in AITL, can drive the pathological changes observed in the lymph nodes, including the enhancement of B-cell maturation and the potential transformation into more aggressive tumor-like cells. The disorganization of germinal center (GC) structures, with the loss of typical GC-resident cells like follicular dendritic cells (FDCs) and tingible body macrophages, further complicates the disease landscape and serves as a diagnostic clue for AITL. These findings were also observed in the present case.
In conclusion, this study integrates the histopathological patterns described by Attygalle et al. with recent insights into the molecular pathogenesis of AITL. The expansion of FDC-MW observed in Pattern I, its diminution in Pattern II, and its disappearance in Pattern III suggest the progression of B-cell maturation and the increasing severity of the histopathological changes. The presence of DLBCL-like pathology in Patterns II-III further underscores the critical role of B-cell dynamics in the progression of AITL. These insights not only deepen our understanding of AITL’s histopathology but also highlight the importance of integrating molecular diagnostics in managing the composite lymphoma, AITL and DLBCL.
References
- Jain S, Mallick S, Ramteke P, Gogia A. Neoplasms of follicular helper T-cells: an insight into the pathobiology. Am J Blood Res. 2022;12(3):64-81.
- Chiba S, Sakata-Yanagimoto M. Advances in understanding of angioimmunoblastic T-cell lymphoma. Leukemia. Oct 2020;34(10):2592-2606. doi:10.1038/s41375-020-0990-y
- Lage L, Culler HF, Reichert CO, da Siqueira SAC, Pereira J. Angioimmunoblastic T-cell lymphoma and correlated neoplasms with T-cell follicular helper phenotype: from molecular mechanisms to therapeutic advances. Front Oncol. 2023;13:1177590. doi:10.3389/fonc.2023.1177590
- Xie Y, Jaffe ES. How I Diagnose Angioimmunoblastic T-Cell Lymphoma. Am J Clin Pathol. Jun 17 2021;156(1):1-14. doi:10.1093/ajcp/aqab090
- Song W, Craft J. T Follicular Helper Cell Heterogeneity. Annu Rev Immunol. Jun 2024;42(1):127-152. doi:10.1146/annurev-immunol-090222-102834
- Suefuji N, Niino D, Arakawa F, et al. Clinicopathological analysis of a composite lymphoma containing both T- and B-cell lymphomas. Pathol Int. Oct 2012;62(10):690-8. doi:10.1111/j.1440-1827.2012.02858.x
- Chihara D, Dores GM, Flowers CR, Morton LM. The bidirectional increased risk of B-cell lymphoma and T-cell lymphoma. Blood. Sep 2 2021;138(9):785-789. doi:10.1182/blood.2020010497
- Attygalle A, Al-Jehani R, Diss TC, et al. Neoplastic T cells in angioimmunoblastic T-cell lymphoma express CD10. Blood. Jan 15 2002;99(2):627-33. doi:10.1182/blood.v99.2.627
- Attygalle AD, Kyriakou C, Dupuis J, et al. Histologic evolution of angioimmunoblastic T-cell lymphoma in consecutive biopsies: clinical correlation and insights into natural history and disease progression. Am J Surg Pathol. Jul 2007;31(7):1077-88. doi:10.1097/PAS.0b013e31802d68e9
- Tan LH, Tan SY, Tang T, et al. Angioimmunoblastic T-cell lymphoma with hyperplastic germinal centres (pattern 1) shows superior survival to patterns 2 and 3: a meta-analysis of 56 cases. Histopathology. Mar 2012;60(4):570-85. doi:10.1111/j.1365-2559.2011.04097.x
- Carbone A, Gloghini A. Follicular dendritic cell pattern in early lymphomas involving follicles. Adv Anat Pathol. Jul 2014;21(4):260-9. doi:10.1097/PAP.0000000000000030
- Du J, Jin S, Zhang M, et al. Precise diagnosis and targeted therapy of nodal T-follicular helper cell lymphoma (T-FHCL). Front Oncol. 2023;13:1163190. doi:10.3389/fonc.2023.1163190
- Attygalle AD, Chuang SS, Diss TC, Du MQ, Isaacson PG, Dogan A. Distinguishing angioimmunoblastic T-cell lymphoma from peripheral T-cell lymphoma, unspecified, using morphology, immunophenotype and molecular genetics. Histopathology. Mar 2007;50(4):498-508. doi:10.1111/j.1365-2559.2007.02632.x