






Barefoot vs. Shod Walking: Health Impacts and Risks
Walking barefoot: a literature review of sensory, biomechanical aspects and injury risks
Zoltan Derzsi1,2
- New York University Abu Dhabi, United Arab Emirates; [email protected], [email protected]
- Heaviside Institute, Dubai, United Arab Emirates
OPEN ACCESS
PUBLISHED: 31 December 2025
CITATION: Derzsi, Z. Walking barefoot: a literature review of sensory, biomechanical aspects and injury risks. [online] 13(12). https://doi.org/10.18103/mra.v13i12.7126
COPYRIGHT:This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i12.7126
ISSN 2375-1924
ABSTRACT
Running barefoot and in minimalist footwear as a sports activity has received much more attention than walking during everyday activities, despite humans typically spending more time and covering more distance walking than running. This article investigates common similarities and differences in health, anatomy and sensory aspects from publications that review and compare habitually barefoot with habitually shod walking. Compared to barefooters, shod walkers have narrower feet with less evenly distributed pressure patterns, and thinner bones in the toes. Barefoot walking offers additional sensory input, which is beneficial for balance and gait stability, and is a good motivation for exercise. It is also linked with improving attention and working memory. Barefoot locomotion has shorter strides, offers lower peak mechanical loads in soft tissue, bones and joints. The hot, moist and cramped environment of footwear is a primary cause of excessive microbiome growth and ingrown toenails, and long-term use correlates with bunions and increased likelihood of developing high-pressure spots and degenerative arthritic conditions. The majority of affected people do not choose surgical treatment, and accept the loss of quality of life from chronic pain and reduced mobility with its increased economic and healthcare costs. While 87% of shod walkers develop long-term chronic issues, there is no study that measures the injury probability of habitually barefoot people. At work, only 10-12% of all injuries are on the feet and ankles. Footwear offers mechanical and thermal protection, but it does not reduce the severity of injuries. Along with the injury probability, the unverified claims of electrical grounding are controversial. Evidence suggests that long-term risks of shod walking may outweigh the short-term risks of barefoot walking, but more data is needed to have a definitive conclusion.
Keywords:
Barefoot walking; Hallux valgus; Somatosensory input; Development; Gait; Balance; Earthing
THE EUROPEAN SOCIETY OF MEDICINE
Medical Research Archives, Volume 13 Issue 12
REVIEW ARTICLE
Introduction
The health and biomechanical aspects of running barefoot and while wearing minimalist footwear have received much attention and controversy in recent years, especially in sports science. However, most people walk significantly more than they run during their daily lives while participating in many activities ranging from recreation through transport and work. Understanding the implications of walking barefoot with respect to being shod in these situations have received relatively little attention, probably due to their varied nature and because it is not practised commonly in modern contemporary environments. It is very difficult to establish proper controls that allow focusing on particular aspects and conduct reliable studies, or to systematically compare findings from one such study to another.
Instead of narrowing down and comparing specifics, this review covers varied, interdisciplinary topics with the aim to compare the implications of habitually walking shod and barefoot, in order to establish the common themes and contractions and identify research gaps. This article is the result of the interdisciplinary approach put into practice: it covers relevant findings from anthropology, neuroscience, clinical studies, psychology, engineering, and physics. Relevant collected works span over a century, and includes the most recent ones as of 2025.
Therefore, it is not possible for this paper to be a systematic review in the traditional sense where all the data from all studies are pulled together and converted into the same format for statistical operations to be performed upon. Instead, this article is written as a narrative review with the scope of comparing the sensory and biomechanical aspects of habitually shod and barefoot populations in everyday situations and not specifically sports activities, such as running or climbing.
subsection covers the reporting of key findings of prominent reviews. In subsequent sections, the common themes and contradictions are identified for walking habitually barefoot and shod, along with some possible future directions and recommendations as suggested by the findings and the research gaps.
Risk of bias, search strategies and methods, inclusion criteria
In 2014, to raise funds for two charities funding research for chronic fatigue syndrome, the author, then PhD student, decided to experiment on himself and report the experience of somatosensory hypersensitivity and the health aspects of barefoot walking in a number of outside environments. The original article appeared in the Newcastle Chronicle, and there is a copy of it available on the Free Library’s and the ME Association’s websites. As the author published his own experience, he also looked for similar cases or studies in the scientific literature to determine whether the experience is typical and how the observations might progress. Therefore the author may have exhibited unintended bias when the purpose of the search was explicitly to confirm or contradict his findings. At that time, there was no distinct search strategy; anything that was relevant on the theme of barefoot and shod walking was included, including health and biomechanical aspects, clinical studies and psychology, as long as it was published in a peer-reviewed scientific journal. Searches included direct search in the Walton Library of the Newcastle Medical School in the UK, and online databases and search engines such as PubMed, Google Scholar or IEEE Xplore.
Over the years the search terms and strategies went through several iterations. The keywords others. With the exception of three books and a monograph, all references are peer-reviewed scientific publications. This was not done specifically to impose a quality barrier for non-peer-reviewed studies, but to ensure that the works are indexed into different databases and will be found in the future. All cited works are in English, except two: one article is in German, and the other is in Japanese both of them have the abstract available in English, and translatable using currently available online tools.
Results
Findings from existing systematic reviews
The earliest and the shortest article (one could argue that it is more of a commentary than an actual review) found was from 2008, and was published as a response to an online newspaper article in the New Zealand Herald from March 2008. It is still available for reading as of 2025. In the newspaper article, controversy was sparked due to the increased risk of acute injury while barefoot in contemporary urban environments. This includes a clinician reporting that their practice has treated “hundreds” of cases of acute injuries every year resulting from school events, and the proposed solution was to “wear appropriate shoes for the duration of the event”. Rome et al highlighted attention that while they considered the area as poorly researched at the time, there are studies that linked a number of chronic foot issues with shoe wearing in childhood. While saying that walking on hard surfaces (concrete, pavement, etc.) may include the development of arthritis and reduced foot function, a much greater concern is low physical activity and obesity and diabetes. They acknowledge that walking barefoot with diabetic neuropathy is risky due to lack of plantar sensation and poor circulation, and children with type 2 diabetes and neuropathy need “podiatric surveillance for complications”. At the same time, they include a study that shoes themselves have been known to cause injuries, especially when they are rigid and thick-soled. They recommend the use of shoes that do not limit foot movement and therefore does not interfere with development. They also include a study about the foot shapes of German and Australian children, where they find that the Australian children, who are predominantly barefoot, have shorter and wider feet. Besides advocating further research in the area, they imply that since shoe manufacturers do not “accommodate intercontinental difference in foot morphology based on racial and/or environmental factors”, they have not found evidence that shoes improve foot pain and flat feet in New Zealander children.
Perhaps one of the most comprehensive and systematic reviews found about barefoot walking is Franklin et al 2015. They meticulously went through a number of online databases (Medline, EMBASE, Web of Science, Cochrane Library, SCOPUS and AMED), identified risks of biases, detailed conflict resolution of article choices between co-authors, and grouped studies together by similarity in methodology and findings. They paid particular attention to gait kinematics, kinetics, and muscle activity when walking barefoot, minimalist footwear and conventional shoes. They found that the strides are shortest while walking barefoot, followed by minimalist footwear, and longest when wearing conventional shoes. They suggest that the origin of this phenomenon is due to a sort of a pendulum lengthening effect: shoes are heavier and thicker, therefore it may be considered as an extension of the legs, and they only found one study that is at odds with this theory.
Kinematically, they found that barefoot walkers exhibit larger ankle plantarflexion while the foot’s flexion range is larger, barefoot walkers exhibit a reduced “heel strike”, which results in a lower and slightly delayed Tibialis Anterior muscle contraction. Interestingly, they argue that the reduced contact surface area of bare feet when compared to shoes presents an increased risk of slipping, and that the increased plantarflexion may be considered as a strategy to increase surface contact area. Moving on to pressure, they found that habitually barefoot people have larger surface contact areas and lower, more evenly distributed surface pressures than minimalist footwear wearers or habitually shod people. Those who grew up habitually barefoot, still exhibit the gait characteristics of walking barefoot, even if they wear minimalist footwear. They make a very clear argument that the population of people who habitually walk barefoot and habitually shod people who decide to walk barefoot are not identical, and shod people who walk barefoot have increased plantar pressures and reduced foot contact surface. They support their argument with the ground reaction force distribution, which shows that habitually barefoot people have lower and more widely distributed peaks than habitually shod people who walk barefoot. Moving further up to the knees and the hips, they found that due to the increased plantarflexion of the foot, the mechanical load is more absorbed in the muscles and the “windlass mechanism” action of the gait reduces peak pressures on the knee and hip joints, and increases flexion. Both of these properties are linked to the prevention or reduction of progression of arthritis. They, however, warn that there is an age dependence of gait, and that the studies used to support this argument mostly focused on young and early middle-aged adults.
When examining mechanical load, they found that the feet tend to spread out laterally when carrying heavy objects, and shoes and even minimalist footwear restrict this type of movement. They imply that this type of restriction might be the primary reason for shoe-induced chronic anatomical changes (i.e. hallux valgus) and suggest that 87% of habitually shod people suffer from at least one type of foot problems, and more than half will have hallux valgus (45.5% of all the people as reported 51% of the people who have foot problems) to a degree where it affects mobility. They also argue that these observed foot problems are also associated with reduced gait performance and increased risk of falls, and one of the causes of these deformities is “insufficient room in the forefoot region of the shoes”, which is the area where shod and habitually barefoot people exhibit the largest anatomical difference. They stress the importance of sufficient toe space during development, and argue that the use of shoes during childhood is preventing the windlass mechanism from developing and operating properly, which is more likely to cause joint-related problems later-on in life.
Anatomically, Franklin et al 2015 reports that habitually shod people have a much wider range foot arch sizes (from flat feet to extreme arches) than habitually barefoot people, which the authors argue is due to the types of shoes worn. They argue that “modern footwear design such as arch supports could be forcing our feet into unnatural positions not allowing for normal foot functions” and ultimately resulting in muscle weakness, which is what they attribute the prevalence of arch-related foot problems of shod people to. And finally, they state that “shoes do offer a protective surface against the likelihood of cuts, abrasions and infections from mechanical insult and debris” (i.e. against acute injuries), but the problems caused by inflexible, poor fitting shoes are more likely to cause chronic problems.
Another, similarly meticulous systematic review on the matter is Hollander et al 2017. While they were more interested in running locomotion techniques, they also analysed the literature for walking as well to a smaller extent. In their search strategy, they include the exact search terms for the online databases and even specified the languages they included. They only considered cross-sectional studies and works which had randomised control trials, case control, cohort. They specifically excluded review articles, meta-analyses, commentaries and anything with single-case studies. The co-authors were also reviewers for articles to be included and they re-computed all the statistical analyses of all the studies that they compared. They even include a geographical analysis of their sources most of their included habitually barefoot samples came from Asia and Africa involving healthy children and young adults except for one study which included fishermen (of older age than young adult). In their motion analysis, they found that barefoot runners exhibit a reduced ankle dorsiflexion at footstrike. They also found conflicting evidence in the effect size for knee kinematics, they argue that there is limited evidence, especially since some of the data are self-reported. For walking, they only found limited evidence for longer ground contact times.
Anatomically, they confirmed that habitually barefoot people have wider and more pliable feet, and a “reduced hallux angle” than shod people. With the exception of one study, they found that habitually barefoot people have a lower incidence of flat feet, but overall they found no statistical evidence in foot arch height difference to shod people. Otherwise, mainly due to lack of available data at the time, they did not report any relationship between footwear type and motor performance. They also have not reported any studies that compare acute injuries when walking. Finally, Hollander et al 2017 argues that barefoot locomotion is important for optimal foot development and partially for preventing foot pathologies from occurring. Should the use of footwear be unavoidable, it should be flexible, flat, lightweight and not constrictive.
Additional studies
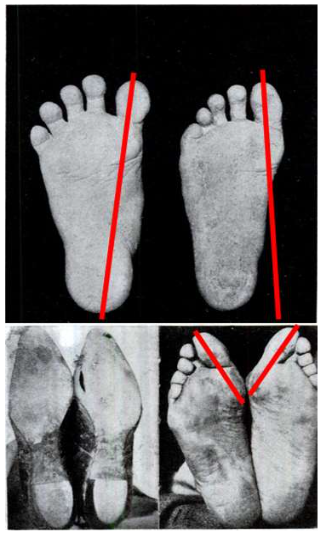
Footwear and footwear-related anatomical changes date back to about 40000 years ago, mostly in hostile environments where thermal insulation was required: people who wore shoes had sleeker pedal phalanges than people who did not require wearing them. The first direct evidence of leather/plant fiber footwear originated much later, about 12000 years ago. Although the narrowing of bones is a slight anatomical change, it has been known since 1905 that wearing shoes even for a short period of time induces progressive and permanent changes in the pedal anatomy to comply with the narrow and pointed shape of shoes (see Figure 1), and certain health problems such as hallux valgus and flat feet are virtually non-existent in barefoot populations. This has been replicated over and over again, and further confirmed that the feet of habitually barefoot people are wider with the plantar pressures having lower peaks and being more evenly distributed than those of shod people. While the review articles reported above are extensive and there are a number of articles that were mutually selected for review, there are some articles that were published in the same era but were not included by either of them, and since research is ongoing in this area, there are new findings and development.
The biomechanical aspect
Perhaps the oldest one that was not included is Robbins et al 1994: In the 1990s, thick foam-soled training shoes came into fashion, and they analysed how well their participants can maintain balance by asking them to walk on an extruded aluminium beam barefoot and while wearing different training shoes. To make sure that they only use their vestibular systems to maintain balance, the participants wore frosted glasses to reduce visual acuity. They found that taller people are slightly more prone to lose balance, and they found a much stronger relationship between the probability of losing balance and the midsole thickness and hardness of the shoes worn. In all cases, they reported significantly more balance failures than when the participants walked across the beam barefoot.
While Franklin et al 2015 touched on mechanical load, Arndt et al 2002 was particularly interested in understanding metatarsal stress fractures and the effect of muscle fatigue. When carrying heavy objects for an extended period of time, such as through military exercise, they noticed that there is an increased number of second metatarsal fracture cases and local bone deformations reported, especially with new recruits. They correlated these injuries along with flat feet and metatarsalgia with the reduced soft tissue volume that surrounds the bone. To measure the mechanical load and fatigue, they implanted an instrumented staple strain gauge into participants’ second metatarsals, and inserted intramuscular electromyography probes to the medial flexor digitorum longus muscle. Then they made their participants walk at 3 km/h, with a 20 kg backpack on a treadmill for an hour. They found that as fatigue onsets, the windlass mechanism during barefoot walking no longer functions properly, which results in peak tension on the metatarsal bone. The state of the plantar muscles and lipid layers (the “fat pads”) play an important role in protecting the bones from deformation and cracking.
Shoes with narrow toe boxes have been primarily correlated with the incidence of hallux valgus and flat feet in numerous studies, review articles and meta-analyses over the decades, with one study going further, saying that they are assuming that it is an acquired condition. Fitting footwear the right way is particularly important for children because the earlier in life poorly fitted shoes are worn, the more severe these problems get later-on. Habitually barefoot populations are virtually unaffected: this has been replicated in a number of studies in similar settings: with Indian children; with Congolese children; in New Zealand; with German and South-African children; with Austrian and Japanese children; and with Spanish children. The effects are cumulative: by the time people reach old age, habitually barefoot people are more physically active and do not tend to develop chronic biomechanical problems, unlike their habitually shod peers in the same country.
As of the time of writing, the hallux valgus is a progressive medical condition that affects most people who wear shoes, which can only partially be resolved with conservative treatment such as splints and therapeutic footwear. Similarly to hallux rigidus, a similar arthritic degenerative disease, it often requires therapeutic footwear and ultimately, surgical intervention. Another problem which also requires surgical treatment is Morton’s neuroma, where a nerve chronically pressed between the metatarsal bones causes chronic pain, which is aggravated by wearing tight shoes. There are other, less severe diseases correlated with habitual footwear use. For example, ingrown toenails are caused by the increased pressure from improperly fitting shoes that drives nail growth into the wrong direction; a primary cause of tinea pedis is the warm and humid environment, which is positively correlated to bacterial growth on the plantar skin as well.
Closed, unventilated footwear worn for an extended period of time combined with the cramped position of the forefoot which creates a favourable environment for microbiomial growth. All these conditions practically are non-existent with the habitually barefoot populations. While surgical solutions may be required to resolve hallux valgus and ingrown toenails, as Heifetz expressed it: “incapacitation from surgical treatment requires too much time and are frequently ineffective”. While there are advances in surgical techniques that increase success, the long recovery time along with its potential financial burden made many people decide not to seek treatment and accept the resulting pain and discomfort as it is. They let the condition worsen until they are no longer able to walk and be physically active. The resulting sedentary lifestyle carries risks on its own: among others, diabetes and cardiovascular disease, which can shorten life span and quality.
Gait-wise, shod people walk with more dorsiflexion footwear wearers are somewhere in between. There are other studies that agree with the findings of Franklin et al 2015: Walking strides are shortest and stability is the best when barefoot, with minimalist footwear being an interim. This was found to be the case with Australian children; with obese people; both with younger and older German people; with patients suffering from chronic ankle instability; when wearing minimalist shoes, the strides are becoming slightly longer; and finally, the strides are the longest when wearing shoes. Similarly, footwear also affects other aspects of the walking pattern: participants who wear shoes touch their heels to the ground first, and this, combined with the longer strides, increases peak acceleration, muscle activity, peak forces and overall energy cost of walking. However, these differences tend to diminish, when walking faster. Nevertheless, the increased muscle activity from walking barefoot has been successfully exploited in the clinic, for example for improving heel pain.
The sensory aspect
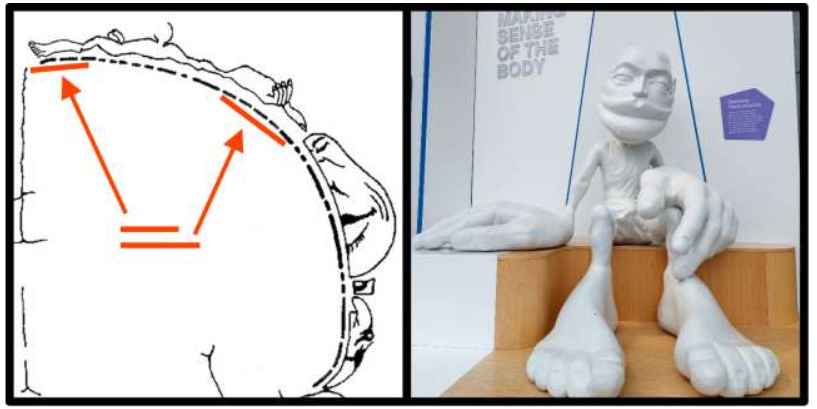
The somatosensory homunculus shown in Figure 2 is an artist’s impression of how human anatomy would change if the receptor density were uniform. In earlier editions shown in neuroscience textbooks for example, the hands were much larger than the feet, but new evidence has surfaced that they are more comparable in size and behave very similarly when representing different size proportions. The feet have over 100 types of mechanoreceptors alone, which not only provide very accurate somatosensory spatial resolution, but they are developed to handle large dynamic range in intensity and in the time domain as well. Multisensory integration improves walking performance and balance accuracy, and the reduction of sensory input adversely affects this process. Luckily the loss is not permanent, and improvements are shown from just minutes of walking in minimalist footwear. Considering that we humans live in a haptic world and rely on non-visual information to a great degree, this is not surprising. While there are many optical illusions, creating contradictory haptic stimuli is considerably more difficult because when humans touch an object (or in this case, walk on it and feeling it), a lot of extra sensory information elements are being collected that mutually depend on each other.
Perhaps the earliest example in the context of locomotion to this is Robbins et al 1994, where they intentionally blocked visual acuity and rely on vestibular/proprioceptive/somatosensory senses only. When they reduced this haptic feedback by giving the participants thick foam-soled shoes, their performance worsened considerably. Sometimes, the plantar sensory loss is due to a chronic disease, such as diabetes: in cases where diabetic neuropathy is present, not only is the sensory threshold and the latency increase (for pressure, vibration, temperature, etc.), but the participants also struggled to maintain their balance, especially with their eyes closed. Suboptimal gait has been observed when plantar sensory feedback is reduced: when the feet are desensitised by immersing them into icy water, the rollover process during a stance is less smooth: people use their feet as if it was a single surface with minimal plantarflexion, and it also changes the weight distribution during walking, in such a way that the center of mass of the body is closer and above the ground contact point for an extended time during a stance. A similar effect was observed when the feet were desensitised with lidocaine, which is a more targeted approach than the ice immersion or the use of a tourniquet: in every stance, the first peak of ground reaction force increased, which resulted in increased muscle activity and knee flexions, which implies that walking becomes more demanding for energy when the sensory feedback is diminished. With physiotherapy, some of the diminished sensation may be gained back, which may be beneficial for balance and daily activities.
When walking barefoot, the plantar somatosensory feedback will not diminish when calluses and soft tissue are developed from friction and exercise. Holowka et al 2019 found while the thicker plantar skin and soft tissue over the heel and metatarsal heads offers increased mechanical protection, it does not reduce sensitivity but it increases its dynamic range. The sensory feedback is not just used to optimise gait for energy use: the haptic perception of the flooring one walks on decides the appropriate gait pattern. Where the surface has a lower friction coefficient and therefore slips are more likely to be a concern, barefoot walkers adjust their stances to have a longer support phase, and this effect is sex and age-dependent. Many studies found that older people especially benefit from increased somatosensory input and similarly, when special insoles are inserted into shoes to provide some of the missing somatosensory feedback, a meta-analysis found that it not only improves various aspects of gait (including energy use), but also reduces the chance of falls and resulting injuries with the elderly.
The role of this extra sensory information does not stop at efficiency and safety. The subjective experience of it also plays an important role, which can be a motivation for exercise, which perhaps makes it no coincidence that in developed industrial cultures such as New Zealand where it is widely acceptable not to sport footwear, being at home and for exercise is where they are most likely to be barefoot. Additionally, not only is the increased sensory experience beneficial for gait, but barefoot walking in a laboratory environment has been demonstrated to improve metabolism. Walking on barefoot trails in urban forests has been shown to improve serotonin levels and reduce chronic inflammatory response, suspected to be because of improved circulation in the lower extremities. There is electroencephalography evidence and working memory tests that walking barefoot, even when done in an urban environment, improves cognitive abilities. The increased sensory input that is also reported to give higher levels of neural functionality other than cognition has contributed to the popularity of barefoot trails, and has implications for future environmental design.
Controversies and contradictions
Perhaps the most controversial aspect of barefoot walking is the perceived higher risk of injury and infection. In the original newspaper article that Rome et al 2008 responded to, the prevalence of acute injuries was a primary concern. Considering that the plantar skin’s pain threshold is about six times higher and that it regenerates at about twice the speed than the hairy skin on the thighs and the increased mechanical durability there is minimal trade-off in sensitivity. The common nature of barefoot-walking-related acute injuries is that they are principally small and transient. None of the studies included, not even on an individual case-study level, reported long-term chronic infections caused by acute injuries from walking barefoot. A study focused on occupational hand injuries reported that wearing gloves reduces the risk of acute problems by about 20%. Assuming that the primary acute injury types suffered while walking barefoot are similar to occupational acute injury types (i.e. lacerations, crushes, punctures), there is no data available to support the hypothesis that a similar increase of injury risk when one walks barefoot. Occupational foot injury statistics do not show that safety footwear actually reduces foot and ankle injuries. Considering that there is a 15% probability of occupational hand injuries (half of this takes up lacerations) per year, and about 2% require hospital treatment, a similar if not lower probability may be estimated for the risk of acute injuries when walking barefoot. This is additionally supported by Conti and Silverman 2002, where plantar injuries took up 5-6% of all the occupational injuries.
However, being consciously aware of the increased likelihood of injury from being barefoot may actually reduce this number considerably: a Japanese study found that schoolchildren who do not wear footwear are more likely to display safety-aware behaviour such as avoiding or relocating hazardous objects, and they reported fewer injuries than shod Japanese schoolchildren of similar age.
Chronic foot injuries, however, are a different matter. As much as 87% of shod people develop some sort of a foot problem from improperly fitting shoes (hallux valgus, ingrown toenails, abrasion injuries, infections from excessively growing microbiome, etc.), and a rather sizeable portion of them would require surgical intervention, but will choose not to, and instead accept the reduction in life quality originating from chronic pain and reduced mobility.
Having established that elevated plantar pressures can cause foot injury, another study reported a similar, if not the same problem. If the same population who wear shoes all their lives (elderly people in California, USA) will suddenly, without any training or preparation start walking barefoot, the local plantar pressures may be high enough to cause problems. This is a popular topic in barefoot and minimalist running literature as well which is outside of the scope of this paper, but these injury types may be more specific to age and lack of transitioning rather than barefoot walking itself.
Shoes, however, can be used to improve locomotor performance. While children and adolescents who walk barefoot have a healthier anatomy and better motor skills, a study found that shod children tend to sprint faster.
In order to attempt to restore some of the anatomical changes experienced by shod people, there are a number of approaches developed. One of them is the introduction of the “Masai Barefoot Technology” shoes, which mimics the gait pattern of a barefoot walker: the strides are shorter and the recorded muscle activity is similar as well. These effects are attributed to the rounded soft soles of the shoes changing the gait pattern, with the intention of promoting muscle activity that was absent with shod people for an extended period of time. Another approach to mimic barefoot walking to a smaller extent is the design of an insole that redistributes the pressure pattern of the foot inside the shoe, or to create an insole that creates increased sensory feedback. While studies reported that barefoot walking is the most energy efficient when compared to shod walking, there is a study that reports that high-heel wearers may walk even more efficiently due to induced anatomical changes from footwear and gait.
Claims related to earthing and grounding
Another controversial aspect of being barefoot is the subject of earthing or grounding. As human skin is somewhat conductive, walking or standing barefoot on a similarly conductive surface would form an equipotential surface. While the phenomenon is of practical use and there are wearable devices that purposefully electrically connect a human body to ground, its applications are mainly in the semiconductor industry where any static electricity discharge would effectively vaporise a thin layer of metal oxide between electrodes found in chip-scale transistors, and in the chemical industry, where the spark from electrostatic discharge may be an ignition source.
In both of these applications, any static electrical charge is slowly conducted away to ground via a resistor, which is similar in nature to when one stands on the ground with bare feet. In addition to the industry applications, the following studies claim that the physical phenomenon of earthing offer some health benefits.
Perhaps the earliest study is Ghaly and Teplitz 2004, where they reported that the cortisol levels of 12 individuals connected to ground, who self-reported to have sleep disorders, had shifted. Most of the subjective evaluation of sleep quality showed it had improved: they fell asleep quicker and woke up less often, 9 of the 12 participants reported better energy levels during the day.
Another study, Chevalier 2010 attached conductive patches on the feet of 28 healthy people who lied down, and measured a number of health parameters (skin conductance, blood oxygenation, respiratory rate, pulse rate and perfusion index) during a 2-hour grounding session. They reported that when compared to pre-grounded, some of the measured parameters, such as respiratory rate and skin conductance have decreased.
Sokal and Sokal 2012 used DC voltage measurements on various anatomical features of four healthy people lying in a Faraday-cage in a climate-controlled environment. For both the earthed and non-earthed conditions, they used a set of metal electrodes to measure the voltage. Chevalier et al 2015 demonstrated that their six healthy participants who got electrically connected had lower, less varied and more symmetrically distributed body surface temperature, which they measured with a thermal camera. These results seem to be different than when the same measurements are obtained after a 10-minute session of full-body vibration.
Oschman et al 2015 demonstrated that electrical grounding can reduce some inflammatory markers, which can have implications with diabetic ulcer treatments.
Note that these studies are all controversial, this section only contains what they reported as key findings, and they have been included for the sake of completeness and fairness, without any scrutiny applied to their methods or statistics and have not been replicated a third party.
Discussion
Due to the varied nature of these studies, it is very difficult, or even impossible to analyse with scientific-level rigour without being inherently flawed. In the last century alone, there have been two world wars; some countries where some included studies were conducted no longer exist; there have been massive technological developments; human society, and to a lesser degree, even human anatomy has changed. These are simply not possible to take into account flawlessly when converting findings and data: humans are too different, their environments are too different, the societal structures are too different, and the economic statuses are also too different. Therefore, when one would take these inherently masks the differences originating from these aspects. Walking is always going to be subject to variations in culture, in the environment and in the human anatomy and ultimately it is only applicable to specific circumstances. For example, a habitual barefoot walker would wear shoes differently than a habitually shod walker and vice versa. In addition, there are very clear differences in age, sex, short- and long-term walking practices that may well skew or contradict results. At the same time, masking these differences may be useful, when one looks for aspects of the human condition in general. After all, we humans breathe air, drink water and eat food, and we use our feet to walk naturally there are exceptions to this out of billions of people living on the planet, and it is important that one recognises that.
reference to readily available mass-produced clothing items that are available in a certain deterministic sizing convention that are being worn without any adaptation or precise fitting. Only one study reported long-term effects from footwear that is customised and/or tailored to take individual anatomy into account. Footwear may also be mass-produced, more attention is paid for the fitting process during acquisition, and they are purposefully designed to more or less mimic locomotion similar to barefoot walking.
Changes of foot anatomy
The most common theme is the permanent and often degenerative changes that correlate with footwear. Time and time again, across the millennia, it has been established that the use of footwear correlates with reduced bone robustness, flat feet and hallux valgus and to a lesser extent, hallux rigidus, and children are particularly affected irrespective of their geographical location or their cultural or socio-economic background. While correlation does not imply causation, only one study went further, and stated that they “assume” that hallux valgus is an acquired condition. It is methodologically impractical to establish a cause-effect relationship through direct evidence it would just be impossible to find the Donald Unger of the feet somebody having the necessary clinical background and with the scientific discipline to wear poorly fitted shoes on one foot and not wear anything on the other for fifty years and then compare the anatomical changes.
None of the included studies reported that footwear is beneficial for pedal anatomy or locomotion (besides performance) in any way, when compared to barefoot walking. Review articles and meta-analyses have repeatedly found the opposite. The only benefits reported are mechanical and thermal protection, and with certain medical conditions, the restoration of function for walking. For sports activities, running shoes have been shown to improve performance, but ultimately this is what they were designed for.
Probability of injury
Another common theme is the health and safety issue. While some of the included studies reported exact statistics of occupational acute foot injuries, these are mostly limited to occupations involving heavy manual labour mining, transportation, and construction, to name a few. Their focus was further analysis into demographics, medical costs, and longer-term economic costs. However, there is an older study by Conti and Silverman from 2002, who not only did a detailed analysis on the costs and their trends over the years, but also looked into the nature of injuries and their resulting days off work. They found that a foot and ankle injury will result in more days off work than a hand injury this is hardly surprising, as one is more likely to be able to go to work with an injured hand than with an injured foot. However, they establish that overall probability of foot and ankle injury is 9.5% across all workplace injuries, and slightly less than half of these are concerning the ankle. They also argue that the use of personal-protective equipment (in this case, steel-toe-capped shoes) change the nature of injuries. However, unlike with the safety equipment of the passenger car (seatbelt, airbags) that reduce the overall severity of injuries, safety shoes have not been found to effectively reduce severity.
There were a series of military studies that confirmed this further. During the literature search, no studies were found that analysed the probability of foot and ankle injury of habitually barefoot people and compared it with shod people; and no studies were found that establishes if at all, and if so by how much footwear reduces the probability of acute injury that uses habitual barefoot walkers as control. At the same time, evidence points toward the opposite: barefoot walkers are more safety-aware, and the added sensory feedback is beneficial for balance which in turn reduces the risk of falls, especially with elderly. Compared with conventional footwear, wearing minimalist footwear also offers some of these benefits, but at a reduced level.
For argument’s sake, rather naïvely, if one neglects Conti & Silverman’s and Knapik et al’s work and assumes that footwear reduces the overall severity of injuries, and ignores evidence that barefoot walkers display more safety-aware behaviour, and one were to approximate the effect of foot protection, one could directly convert data from occupational hand-injury statistics. The probability of hand injury would be somewhere around 10-15%. This includes the most minor ones as well, equivalent to the level of paper cuts. Acute injuries that require medical attention would be much lower, about 2-3% in the general population, which includes non-manual-labour-heavy occupations as well. Not wearing gloves at work where required increases this figure by 20%, to around 2.5% probability of suffering an injury that requires medical attention. So, by neglecting the fact that biomechanically the hand is different from the foot, one could transpose this 20% increment from not using gloves to occupational foot and ankle injuries (~10%). One could arrive to the hasty and pessimistic conclusion that the probability of suffering injury on the foot when not wearing footwear would be about 12%.
When this 12% figure (involving the foot and ankle, of all the workplace injuries, and ignorantly extrapolating from existing hand injury statistics) is put into context with the 87% probability of developing chronic foot problems originated from improperly fitting footwear with 51% being hallux valgus, one might question the validity of footwear use in situations where it is not absolutely required, especially considering the elevated risk of acquiring a degenerative joint disease later in life that is known to have limited success with conservative treatment. As it progresses with age, surgical intervention will be necessary to relieve pain and regain mobility. This is in addition to all the other footwear-related health problems, such as ingrown toenails or Morton’s neuroma, which, when severe enough, will also require surgical intervention. Even with this naïve and pessimistic approach, the evidence of chronic harm induced by mass-produced and poorly fitted footwear is overwhelming and the resulting loss of life quality and economic activity are considerable.
However, a there is a scenario where someone is likely to suffer injuries from walking barefoot: when suddenly, without any further thought and preparation, after being shod for decades, one decides to go full-time barefoot without any regard to physique and the environment. As the necessary soft tissue (muscles and lipid layers) and plantar skin have not yet adapted to the increased mechanical load, crush injuries and metatarsal bone damage from local pressure spots that may occur. This is extensively covered in barefoot running literature and is currently being actively investigated. As of the time of writing, the consensus is to build up muscle volume and tolerance in small increments in order to avoid acute injuries while transitioning. This can be done in environments where it is safe to do so: perhaps in a home or office, or spending half a day in a park at first.
Lastly, along with the injury risk, the probability of infection is also mentioned in of barefoot walking. It is important to mention that everyone’s plantar skin is host to bacteria, viruses, fungi and parasites. Normally, none of these can grow excessively due to environmental limitations: microbiome growth requires warmth and humidity, which are more likely to be present in the internal environment of footwear. While there is no direct evidence is available as some studies cited touched the subject tangentially at most, walking barefoot in modern contemporary environments can safely be assumed to be much less beneficial for plantar microbiome growth than the internal environment of unventilated closed footwear. However, one must be aware that in certain hot and damp tropical climates or when the environment is heavily contaminated with faecal matter for example in agricultural lands, the risk of bacterial and parasitic infections can indeed be elevated. However, in these environments, the use of further hygiene steps and protective equipment has been advised already, to reduce the spread of diseases originated from contaminated food and drinking water. The same applies to certain chronic medical conditions such as diabetes, but the other way around: in these cases, it is not that the environment is overly hostile, but one’s immune response is limited, due to poor circulation for example.
Socio-economic and pseudo-scientific statements
Another aspect, which was only partially considered here, is the socio-economic stigma of walking barefoot. Historically, possessing footwear was considered to be a sign of wealth, development and high social status, and not wearing them was a sign of poverty and low social status. More recently, especially in industrialised countries, perhaps with the exception of South Africa and New Zealand, the choice of walking barefoot has been associated with counterculture movements and is often considered a political statement or a protest against the establishment. Perhaps a most iconic sign of this is the ‘No Shirt, No Shoes, No Service’ sign in the United States of America, which gained popularity in the 1970s mainly to keep members of the hippie movement and people of colour (after racial segregation was no longer legal) from entering a business. The use of this sign is legal even nowadays, as a business owner has the right to refuse service to anyone. At the same time, footwear design is a large industry where the prices exchanged for items are greatly above their functional value. As such, the socio-economic aspect of barefoot and shod walking is difficult to measure directly and can be divisive, and due to its abstractness, this aspect was not considered in the review.
Perhaps, to a degree, a manifestation of the anti-establishment stance is most apparent in the works about the health aspects of grounding/earthing. All these works suffer from issues, such as inadequate control measures or in some cases the complete absence of statistical analyses of results, or the implication of a direct cause-effect relationship without excluding any other possibility. The common pattern of offering simple solutions to complex problems (restoring diabetic ulcers with grounding, for example) is not dissimilar to the political anti-establishment rhetoric. However, these studies should not be dismissed based on political opinions or due to the fact that some of the authors have declared a conflict of interest. Clinical applications of scientific findings have been dismissed for no scientific reason in the past that costs hundreds of lives: Ignac Semmelweis for example, who merely suggested that clinicians should wash their hands between patients that just gave birth to reduce deaths from sepsis, was ridiculed by the scientific community. He lost his career, and by the time someone else replicated his findings, he had died in a mental asylum as a result of the abuse received.
Conversely, these studies should not be embraced just because they passed the peer-review process in a scientific journal, but rather, treated as proof that peer-reviewing is not flawless and is not guaranteed to improve scientific quality. These studies, however, despite their shortcomings, must be considered seriously, irrespective of how far-fetched they may look, once the findings reported inside them have been successfully replicated by someone else, in a controlled setting.
Future research directions
While anatomy, gait and other health aspects have been extensively studied in the past, practically no data exist about injuries suffered while walking barefoot and shod, especially in modern contemporary environments. While some indicative data was extrapolated here from occupational injury statistics, it is only a rough approximation that is based on broad assumptions. Rather than using workplace injury statistics which mostly focus on economic impact (time off work, healthcare expenses, etc.), a better measure of injury probability would be the number of injuries suffered for a given number of steps. Further, as injuries vastly differ in severity, a modified version Baker et al 1974’s severity score should be developed: For example, acute injuries could be scaled by severity between 0 and 1, and the cumulated number of injuries weighed by severity could be expressed for every 100000 steps taken for every 1000 people. This would yield a more accurate probability, and would tell how often medical attention would be needed for a given site community, which can be directly inferred to healthcare costs as well. While there is no data available about this, there are subjective evaluations that the probability of acute injuries are much lower than what was reported in occupational statistics.
Another research direction is in microbiology: At the time of writing, very few studies conducted a microbiome growth analysis of plantar skin inside footwear, and this was not compared with the same for habitually barefoot people across different climates. However, one would expect a high variance in microbiome distribution based on climate, health, hygiene habits and cultural differences.
Unfortunately, more pessimistic, and non-scientific (political and societal prejudices, for example) assumptions tend to be the basis of legislation, which contributed to the spread of myths and misinformation about the safety, hygiene and the possibility of litigation in industrialised societies when it comes to the context of barefoot walking. This might be changed if a study would focus on reliably correlating habitually barefoot walking with healthcare costs. A small step into this direction would be a public outreach programme that introduces the findings of some of the cited studies: millions of missed working hours and related healthcare expenses could be saved globally, simply reducing the chronic foot problems by wearing minimal or no footwear, provided that the transition from habitually shod can be done safely. This would also contribute to the improvement of physique and mental health as well with its own health benefits.
Aside from the lack of acute effect studies, no longitudinal studies exist about to what degree foot anatomy can restore when participants decide to be habitually barefoot after years of shod walking, and whether there is the possibility of developing any chronic problems from walking barefoot in modern contemporary environments. Perhaps the closest equivalent to this would Barnett 1962, which demonstrated that the hallux angle can be somewhat restored after years of wearing purpose-made, wide toe-box shoes.
In a more broader sense, since it is widely accepted that multisensory integration leads to more accurate perception and less error in action, simple and constructive ways should be explored in exploiting this property in human-machine interaction: increased plantar sensory feedback may play a role to improve safety and energy efficiency in machines with pedal control, for example.
In situations when the environment demands that shoes must be worn, the footwear design process should include taking human anatomy into account to a greater degree, with either minimally diminishing, or artificially generating the corresponding sensory stimuli. Unfortunately, having understood that the footwear industry prioritises aesthetics over function, the probability of paradigm change in footwear design is very little.
Conclusions
Here, a number of studies were reviewed to establish the similarities and differences in barefoot and shod walking in modern contemporary environments. While wearing footwear may offer mechanical and thermal protection, it also induces adverse anatomical and functional changes in the foot, reduces gait efficiency and diminishes sensory feedback. While stride length and walking performance may be enhanced, this comes with the increment of impact forces and acceleration of joints, which has been linked with chronic degenerative conditions. The ability to maintain balance is diminished, which carries the increased risk of injuries from falls, especially in older age. Wearing precisely fitted, thin-soled, flexible footwear tends to mitigate these effects.
The collected studies cover more than a century of data with significant methodological, demographic and analytical differences. Despite these differences which makes direct comparison unfeasible, most of them send a corresponding message: while footwear offers some degree of protection, it does not significantly reduce the severity of acute injuries. Mass-produced, poorly fitted footwear also induces chronic problems when used long-term. The effects are cumulative, and affected people are more likely to choose not to resolve them by old age. This in turn encourages sedentary lifestyle, with its own health risks and medical expenditure. However, these long-term chronic problems may be considerably reduced if human anatomy is taken into account with more weight in the design process of footwear.
More studies are needed to establish reliable injury statistics and whether long-term chronic effects arise from barefoot walking in modern contemporary environments. Further, the controversial claims of health benefits from electrical grounding should be independently replicated to compensate for the bias and methodological shortcomings in these studies.
Based on the above, it is concluded that walking barefoot in modern contemporary environments may be more beneficial for physical health, gait and mental health when compared with shod walking, and it is suggested that the elevated risk of acute injuries may actually be much smaller than the harm suffered from footwear-induced chronic problems. Therefore, for everyday activities in most but not all environments, wearing minimal or no footwear may be recommended.
Conflict of Interest:
The author declares no conflict of interest, apart from personal motivation about the subject. The original article about the author appeared in the Newcastle Chronicle in 2014, and there is a copy of it available on the Free Library’s and the ME Association’s websites.
These links are accessible as of June 2025: https://www.chroniclelive.co.uk/news/north-east-news/watch-newcastle-phd-student-dumps-7825092, https://www.thefreelibrary.com/Barefoot+to+aid+charity.-a0383599818, https://meassociation.org.uk/2014/09/newcastle-phd-student-dumps-shoes-to-raise-chronic-fatigue-syndrome-awareness-newcastle-chronicle-24-september-2014/.
Funding Statement:
This research received no external funding. In fact, the paper and the author were reverse-funded: the author raised funds during the initial stages of literature search. The author used his personal funds in order to publish this article.
Acknowledgements
The author would like to thank Mel Knott for her valuable input during preparing the initial draft, and Matthias Blümke for additional stimulating discussion about the subject, the paper’s format and additional references.
References:
- Rome K, Hancock D, Poratt D. Barefoot running and walking: the pros and cons based on current evidence. Published online April 18, 2008. Accessed October 26, 2022. https://openrepository.aut.ac.nz/handle/10292/1839
- Franklin S, Grey MJ, Heneghan N, Bowen L, Li FX. Barefoot vs common footwear: A systematic review of the kinematic, kinetic and muscle activity differences during walking. Gait Posture. 2015;42(3):230-239. doi:10.1016/j.gaitpost.2015.05.019
- Hollander K, Heidt C, van der Zwaard B, Braumann KM, Zech A. Long-Term Effects of Habitual Barefoot Running and Walking: A Systematic Review. Med Sci Sports Exerc. 2017;49:752-762. doi:10.1249/MSS.0000000000001141
- Trinkaus E, Shang H. Anatomical evidence for the antiquity of human footwear: Tianyuan and Sunghir. J Archaeol Sci. 2008;35(7):1928-1933. doi:10.1016/j.jas.2007.12.002
- Trinkaus E. Anatomical evidence for the antiquity of human footwear use. J Archaeol Sci. 2005;32(10):1515-1526. doi:10.1016/j.jas.2005.04.006
- Hoffmann P. CONCLUSIONS DRAWN FROM A COMPARATIVE STUDY OF THE FEET OF BAREFOOTED AND SHOE-WEARING PEOPLES. Published online 1905:33.
- Shulman SB. Survey in China and India of feet that have never worn shoes. J Natl Assoc Chirop. 1949;49:26-30.
- effects of habitual footwear use: foot shape and footwear Sci. 2009;1(2):81-94. doi:10.1080/19424280903386411
- Mei Q, Gu Y, Xiang L, et al. Foot shape and plantar pressure relationships in shod and barefoot populations. Biomech Model Mechanobiol. 2020;19(4):1211-1224. doi:10.1007/s10237-019-01255-w
- Lythgo N, Wilson C, Galea M. Basic gait and symmetry measures for primary school-aged children and young adults whilst walking barefoot and with shoes. Gait Posture. 2009;30(4):502-506. doi:10.1016/j.gaitpost.2009.07.119
- Morio C, Lake MJ, Gueguen N, Rao G, Baly L. The influence of footwear on foot motion during walking and running. J Biomech. 2009;42(13):2081-2088. doi:10.1016/j.jbiomech.2009.06.015
- Wirth B, Hauser F, Mueller R. Back and neck muscle activity in healthy adults during barefoot walking and walking in conventional and flexible shoes. Footwear Sci. 2011;3(3):159-167. doi:10.1080/19424280.2011.633104
- Keenan GS, Franz JR, Dicharry J, Croce UD, Kerrigan DC. Lower limb joint kinetics in walking: The role of industry recommended footwear. Gait Posture. 2011;33(3):350-355. doi:10.1016/j.gaitpost.2010.09.019
- Zhang X, Paquette MR, Zhang S. A comparison of gait biomechanics of flip-flops, sandals, barefoot and shoes. J Foot Ankle Res. 2013;6(1):45. doi:10.1186/1757-1146-6-45
- Ker RF, Bennett MB, Bibby SR, Kester RC, Alexander RM. The spring in the arch of the human foot. Nature. 1987;325(6100):147-149. doi:10.1038/325147a0
- Robbins S, Waked E, Gouw GJ, McClaran J. Athletic footwear affects balance in men. Br J Sports Med. 1994;28(2):117-122.
- Arndt A, Ekenman I, Westblad P, Lundberg A. Effects of fatigue and load variation on metatarsal deformation measured in vivo during barefoot walking. J Biomech. 2002;35(5):621-628. doi:10.1016/S0021-9290(01)00241-X
- Shine LB. Incidence of Hallux Valgus in a Partially Shoe-wearing Community. Br Med J. 1965;1(5451):1648-1650.
- Rao U, Joseph B. The influence of footwear on the prevalence of flat foot. A survey of 2300 children. J Bone Joint Surg Br. 1992;74-B(4):525-527. doi:10.1302/0301-620X.74B4.1624509
- Abdel-Fattah MM, Hassanin MM, Felembane FA, Nassaane MT. Flat foot among Saudi Arabian army recruits: prevalence and risk factors. East Mediterr Health J. 2006;12(1):7.
- Piqué-Vidal C, Vila J. A geometric analysis of hallux valgus: correlation with clinical assessment of severity. J Foot Ankle Res. 2009;2(1):15. doi:10.1186/1757-1146-2-15
- Buldt AK, Menz HB. Incorrectly fitted footwear, foot pain and foot disorders: a systematic search and narrative review of the literature. J Foot Ankle Res. 2018;11(1):43. doi:10.1186/s13047-018-0284-z
- Hollander K, Petersen E, Zech A, Hamacher D. Effects of barefoot vs. shod walking during indoor and outdoor conditions in younger and older adults. Gait Posture. 2022;95:284-291. doi:10.1016/j.gaitpost.2021.04.024
- Yu G, Fan Y, Fan Y, et al. The Role of Footwear in the Pathogenesis of Hallux Valgus: A Proof-of-Concept Finite Element Analysis in Recent Humans and Homo naledi. Front Bioeng Biotechnol. 2020;8. Accessed October 26, 2022. https://www.frontiersin.org/articles/10.3389/fbioe.2020.00648
- -Lizis E, Zarzyczna P, Mikuľáková W. Impact of footwear fitting on foot shape in primary schoolgirls. Acta Bioeng Biomech. 2020;Vol. 22(nr 1). doi:10.37190/ABB-01425-2019-02
- Sachithanandam V, Joseph B. The influence of footwear on the prevalence of flat foot. A survey of 1846 skeletally mature persons. J Bone Joint Surg Br. 1995;77-B(2):254-257. doi:10.1302/0301-620X.77B2.7706341
- Echarri JJ, Forriol F. The development in footprint morphology in 1851 Congolese children from urban and rural areas, and the relationship between this and wearing shoes. J Pediatr Orthop B. 2003;12(2):141.
- Wolf S, Simon J, Patikas D, Schuster W, Armbrust P, Döderlein L. Foot motion in children shoes A comparison of barefoot walking with shod walking in conventional and flexible shoes. Gait Posture. 2008;27(1):51-59. doi:10.1016/j.gaitpost.2007.01.005
- Hollander K, van der Zwaard BC, de Villiers JE, Braumann KM, Venter R, Zech A. The effects of being habitually barefoot on foot mechanics and motor performance in children and adolescents aged 6-18 years: study protocol for a multicenter cross-sectional study (Barefoot LIFE project). J Foot Ankle Res. 2016;9(1):36. doi:10.1186/s13047-016-0166-1
- Hollander K, de Villiers JE, Sehner S, et al. Growing-up (habitually) barefoot influences the development of foot and arch morphology in children and adolescents. Sci Rep. 2017;7(1):8079. doi:10.1038/s41598-017-07868-4
- Hollander K, de Villiers JE, Venter R, et al. Foot Strike Patterns Differ Between Children and Adolescents Growing up Barefoot vs. Shod. Int J Sports Med. 2018;39(2):97-103. doi:10.1055/s-0043-120344
- Klein C, Groll-Knapp E, Kundi M, Kinz W. Increased hallux angle in children and its association with insufficient length of footwear: A community based cross-sectional study. BMC Musculoskelet Disord. 2009;10(1):159. doi:10.1186/1471-2474-10-159
- Kinz W, Groll-Knapp E, Kundi M. Hallux valgus in pre-school-aged children: the effects of too-short shoes on the hallux angle and the effects of going barefoot on podiatric health. Footwear Sci. 2021;13(1):29-42. doi:10.1080/19424280.2020.1853826
- González-Elena ML, Castro-Méndez A, Coheña-Jiménez M, Córdoba-Fernández A. Relationship of the Use of Short Footwear with the Development of Hallux Valgus in a Sample of Andalusian Schoolchildren. Int J Environ Res Public Health. 2021;18(21):11244. doi:10.3390/ijerph182111244
- Agussalim, Mumin KBHA, Ingkaninan K. Barefoot Walking Habits and their Potential Protective Effect Against Rheumatoid Arthritis: A Qualitative Study among the Kajangand Highland Papua Communities: Research Article. Open J Nurs Res. 2025;1(01):08-13.
- Barnett CH. The normal orientation of the human hallux and the effect of footwear. Published online 1962:7.
- Nilsonne H. Hallux Rigidus and Its Treatment. Acta Orthop Scand. 1930;1(1-4):295-303. doi:10.3109/17453673008991145
- Yee G, Lau J. Current Concepts Review: Hallux Rigidus. Foot Ankle Int. 2008;29(6):637-646. doi:10.3113/FAI.2008.0637
- Ho B, Baumhauer J. Hallux rigidus. Published online January 25, 2017. Accessed May 29, 2025. https://eor.bioscientifica.com/view/journals/eor/2/1/2058-5241.2.160031.xml
- Alzurahi A. Bunion Symptom Disorder: Surgical and Non-Surgical Treatment. Engineering Archive. Preprint posted online April 20, 2021. doi:10.31224/osf.io/pfqvt
- Gougoulias N, Lampridis V, Sakellariou A. Published online January 23, 2019. Accessed June 5, 2025. https://eor.bioscientifica.com/view/journals/eor/4/1/2058-5241.4.180025.xml
- Heifetz CJ. Ingrown toe-nail: A clinical study. Am J Surg. 1937;38(2):298-315. doi:10.1016/S0002-9610(37)90439-2
- Sasagawa Y. Internal environment of footwear is a risk factor for tinea pedis. J Dermatol. 2019;46(11):940-946. doi:10.1111/1346-8138.15060
- Miao T, Wang P, Zhang N, Li Y. Footwear microclimate and its effects on the microbial community of the plantar skin. Sci Rep. 2021;11(1):20356. doi:10.1038/s41598-021-99865-x
- Davis IS, Hollander K, Lieberman DE, Ridge ST, Sacco ICN, Wearing SC. Stepping Back to Minimal Footwear: Applications Across the Lifespan. Exerc Sport Sci Rev. 2021;49(4):228-243. doi:10.1249/JES.0000000000000263
- Petersen E, Zech A, Hamacher D. Walking barefoot vs. with minimalist footwear influence on gait in younger and older adults. BMC Geriatr. 2020;20(1):88. doi:10.1186/s12877-020-1486-3
- Dames KD, Heise GD, Hydock DS, Smith JD. Obese adults walk differently in shoes than while barefoot. Gait Posture. 2019;70:79-83. doi:10.1016/j.gaitpost.2019.02.016
- Abdelraouf OR, Abdel-aziem AA. Ankle and foot mechanics in individuals with chronic ankle instability during shod walking and barefoot walking: A cross-sectional study. Chin J Traumatol. 2021;24(03):174-179. doi:10.1016/j.cjtee.2021.02.010
- Broscheid KC, Zech A. Influence of Barefoot, Minimalist, and Standard Footwear Conditions on Gait and Balance in Healthy Older Adults. J Am Geriatr Soc. 2016;64(2):435-437. doi:10.1111/jgs.13980
- activity in minimal footwear increases foot strength. Sci Rep. 2021;11(1):18648. doi:10.1038/s41598-021-98070-0
- Futrell E, Kaufman R, Chevan J. Long-Term Effects and Impressions of Minimal Footwear in Older Adults. Gerontology. 2024;70(11):1137-1147. doi:10.1159/000540957
- Shakoor N, Block JA. Walking barefoot decreases loading on the lower extremity joints in knee osteoarthritis. Arthritis Rheum. 2006;54(9):2923-2927. doi:10.1002/art.22123
- Muğrabi S, Feyzioğlu Ö. Comparison of short controlled ankle motion boots and barefoot walking on spatiotemporal gait parameters and plantar pressure distribution. PLOS ONE. 2025;20(3):e0319671. doi:10.1371/journal.pone.0319671
- Shultz SP, Houltham SD, Kung SM, Hume P, Fink PW. Metabolic Differences Between Shod and Barefoot Walking in Children. Int J Sports Med. 2016;37(5):401-404. doi:10.1055/s-0035-1569349
- Yu B, Kramer PA. Walking Speed Alters Barefoot Gait Coordination and Variability. J Mot Behav. 2022;54(4):410-421. doi:10.1080/00222895.2021.1990005
- Rickard SC, White MP. Barefoot walking, nature connectedness and psychological restoration: the importance of stimulating the sense of touch for feeling closer to the natural world. Landsc Res. 2021;46(7):975-991. doi:10.1080/01426397.2021.1928034
- Brown KM. The haptic pleasures of ground-feel: The role of textured terrain in motivating regular exercise. Health Place. 2017;46:307-314. doi:10.1016/j.healthplace.2016.08.012
- Francis P, Schofield G, Mackay L. Being barefoot. Prevalence at home, in school and during sport: a cross-sectional survey of 714 New Zealand secondary school boys. J Foot Ankle Res. 2018;11(1):42. doi:10.1186/s13047-018-0285-y
- Kim JS, Lee MM, Kim DS, Shin CS. Effects of Barefoot Walking in Urban Forests on CRP, IFNγ, and Serotonin Levels. Healthcare. 2024;12(23):2372. doi:10.3390/healthcare12232372
- Kim T, Seo DY, Bae JH, Han J. Barefoot walking improves cognitive ability in adolescents. Korean J Physiol Pharmacol Off J Korean Physiol Soc Korean Soc Pharmacol. 2024;28(4):295-302. doi:10.4196/kjpp.2024.28.4.295
- Oschman JL, Chevalier G, Brown R. The effects of grounding (earthing) on inflammation, the immune response, wound healing, and prevention and treatment of chronic inflammatory and autoimmune diseases. J Inflamm Res. 2015;8:83-96. doi:10.2147/JIR.S69656
- Adamczyk K, Garncarczyk A, Antończak P, Dziadecka D. The foot microbiome. J Cosmet Dermatol. 2020;19(5):1039-1043. doi:10.1111/jocd.13368
- Burnfield JM, Few CD, Mohamed OS, Perry J. The influence of walking speed and footwear on plantar pressures in older adults. Clin Biomech. 2004;19(1):78-84. doi:10.1016/j.clinbiomech.2003.09.007
- Zech A. Beinflussbarkeit des Gang- und Laufverhaltens durch Schuhbedingungen. Orthop. 2023;52(8):626-630. doi:10.1007/s00132-023-04407-0
- Zech A, Venter R, de Villiers JE, Sehner S, Wegscheider K, Hollander K. Motor Skills of Children and Adolescents Are Influenced by Growing up Barefoot or Shod. Front Pediatr. 2018;6. doi:10.3389/fped.2018.00115
- Romkes J, Rudmann C, Brunner R. Changes in gait and EMG when walking with the Masai Barefoot Technique. Clin Biomech. 2006;21(1):75-81. doi:10.1016/j.clinbiomech.2005.08.003
- Müller S, Baur H, Ewald A, Hirschmüller A, Mayer F. Redistribution of Load under the Child´s Foot While Walking Shod and with Different Insoles Compared to Barefoot.; 2003.
- Beck ON, Schroeder JN, Sawicki GS. Habitually wearing high heels may improve user walking economy in any footwear. J Appl Phys