





Boundaries of Disease: Risk vs. Pathology in Medicine
Boundaries of Disease: Disease and Risk
Christopher Boorse1
- Department of Philosophy, University of Delaware, Newark, DE 19716 USA
Email: [email protected]
OPEN ACCESS
PUBLISHED: April 30, 2023
CITATION: Boorse C, 2023. Boundaries of Disease: Disease and Risk, Medical Research Archives, [online] 11(4).
https://doi.org/10.18103/mra.v11i4.3599
COPYRIGHT: © 2023 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v11i4.3599
ISSN: 2375-1924
ABSTRACT
Increasingly, medical care targets conditions, like hypertension and hypercholesterolemia, which are defined as ranges of some clinical variable, not by any concrete physical pathology. These ranges are usually chosen from data on modifiable risk, as well as by other empirical consequences. Such purported disease categories face three main criticisms, one practical and two conceptual. The practical issue is overdiagnosis: the fear that more people suffer harm than benefit from such diagnoses. The second issue is Schwartz’s and Accad’s complaint that disease and risk of disease must not be confused. The third issue is that most of the literature on risk-based diseases wrongly assumes a conceptual connection between disease and medical treatment. In this essay I analyze these issues about risk-based diseases from the viewpoint of my biostatistical analysis of health and disease. I reach no conclusion on the first, the overdiagnosis of specific conditions. But I conclude that the two conceptual criticisms are correct: in traditional medical thought, neither risk nor treatability is an element of pathologicity. So Pickering was right: current categories of hypertension, high cholesterol, and the like are not true diseases, nor even diagnostic criteria for true diseases. They are, at best, only categories of justified medical treatment.
Keywords:
disease, pathology, risk, overdiagnosis, hypertension, hypercholesterolemia, diabetes mellitus, osteoporosis, biostatistical theory
Introduction
In recent decades, medicine has come to define certain diseases by a level of some clinical variable which raises the risk of other diseases. More exactly, some diseases are now explicitly defined via what Peter Schwartz dubs “modifiable risk.” If some level of a variable increases the risk of future disease or death, and safe treatment is available which changes the variable so as to lower that risk, that level is often now called disease. Others, too, have pointed to this new phenomenon and complained, or boasted, that it represents a major change in our concept of disease. Among complainers is cardiologist Michel Accad, who calls it a “departure from the traditional pathologic basis of disease.” Likewise, historian Jeremy Greene asks: “How did we arrive at a state where the line between the normal and the pathological became a numerical abstraction? How did these asymptomatic diseases come to be …?” His book is a detailed history of how three of them (hypertension, diabetes mellitus, and high cholesterol) insinuated themselves into our disease classification as drugs were born to treat them. But Schwartz has done the best job so far of analyzing the conceptual issues in light of leading accounts of the classic medical concept of disease – in particular, of mine and Wakefield’s, which agree in requiring biological dysfunction. Schwartz concludes that at least hypertension, high cholesterol, diabetes mellitus, osteoporosis, and obesity fail the dysfunction test. Hence, they are examples of “an unfortunate trend towards reclassifying risk as disease,” though he discusses only the first two conditions in detail. In this paper, I will reach a conclusion similar to Schwartz’s, but by a different route.
We wish, then, to examine three broad questions. (1) Is there a clear conceptual difference between disease and risk of disease? (2) If so, are contemporary classifications blurring it, confusing concepts of preventive and therapeutic medicine? And (3) if so, why is this important?
1. Background: Recent Classifications and Schwartz’s Critique
a. Recent classifications
Let us begin by listing recent definitions of Schwartz’s five disorders and noting various conceptual similarities.
| Disorder | Current definition | Prevalence (%) | Diseases at Increased Risk |
|---|---|---|---|
| Hypertension | SBP ≥ 140 or DBP ≥ 90 | 31 | CVD including CHD, stroke, heart failure or heart attack, end-stage renal disease |
| Prehypertension | SBP 120-139 or DBP 80-89 | 28 | Peripheral vascular disease |
| Hypercholesterolemia | TC > 240 or LDL ≥ 160 | 24 | CHD |
| Diabetes mellitus | 2HG ≥ 11.1 or FG ≥ 7.0 | 13 | Macrovascular disease, CHD, peripheral vascular disease, microvascular disease, retinal, renal, neural disease |
| Osteoporosis | BMD ≥ 2.5 SD below young women’s mean (women ≥50) | 13 | Bone fractures |
| Obesity | BMI ≥ 30 or BF > 25% (♂) or > 33% (♀) | 42 | Hypertension, CHD, Type-2 diabetes mellitus, sleep apnea |
| Overweight | BMI 25-29.9 | 32 | GE reflux disease |
As is evident, all five conditions are described by levels of a clinically measurable variable. In four of the five cases (all but high cholesterol), there is both a full-blown version of the disease and a less severe version which I shall call a “precursor,” at least sometimes viewed as pathological as well. In four of the five cases, disease plus precursor has fairly high prevalence, ranging from 24% to 74% in the general population (usually Americans ≥20 years old). The fifth case, osteoporosis and osteopenia, is defined in my sources only for adults ≥50, but in this group the total prevalence for women is 56%. Also, the prevalence of several other conditions rises sharply with age; e.g., full-blown hypertension has a prevalence of 50% for adults 55-64 and nearly 75% for those over 70, while prediabetes (27%) plus diabetes (49%) covers fully 76% of adults ≥65. Consequently, these conditions are often called “diseases of aging.” Another important similarity is that for four of the five variables – all but body fat – there is a well-known system of homeostatic regulation. Finally, as we shall see, the stated levels describing at least four of the five conditions rest on evidence that such levels increase the risk of other pathological conditions, possibly in the distant future.
We must, however, distinguish three possible views of categories like those in the table: as disease definitions, diagnostic criteria, or mere bases for treatment. Many diseases defined by pathology or etiology have standard diagnostic criteria, which are only clinical evidence of their presence. A certain level of bacterial cfu/ml in a urine sample does not define urinary-tract infection; it merely justifies its diagnosis. Other diseases, such as diabetes mellitus, are actually defined as clinical syndromes, so their definitions are the same as their diagnostic criteria. For either type of category, there may be standard treatment recommendations; but, obviously, there can also be such recommendations for a group of disease-free people, either to prevent future disease or to serve other goals unrelated to disease. For categories like Schwartz’s five, one must ask both (i) how they are currently viewed and (ii) how they should be viewed. As to (i), by the kind of evidence listed in note 5 – ICD classification and use of terms like ‘normal’, ‘pathological’, ‘disease’, and ‘disorder’ – it seems clear that most physicians, including expert panels, view most of the primary conditions in our table as pathological, and often the precursors too. But that view is not universal: for example, the ATP-III report on cholesterol avoids all such terminology except, perhaps, ‘therapeutic’.
There are three main objections to current categories for risk-based diseases, one purely practical and two conceptual. The purely practical one is the charge that recent expansions of these categories constitute “overdiagnosis”: the diagnosis of people most of whom suffer harm but no benefit from their label. The following table shows the scope of some recent changes, by which tens of millions of Americans were newly declared diseased.
| Condition | Old Definition | New Definition | New Cases | Increase |
|---|---|---|---|---|
| Diabetes | Fasting sugar 140 | Fasting sugar 126 | 11,697,000 | 14% |
| Hypertension | Systolic BP 160 | Systolic BP 140 | 38,690,000 | 35% |
| Hyperlipidemia | Total cholesterol 240 | Total cholesterol 200 | 49,480,000 | 86% |
| Being overweight | BMI ≥ 27 | BMI ≥ 25 | 70,608,000 | 42% |
I am persuaded by Welch et al.’s Overdiagnosis and many related papers that overdiagnosis is indeed a serious problem for at least some diseases. But I shall take no position here on the value of current treatment of any specific condition. Instead, I discuss the two conceptual issues from the viewpoint of my analysis of pathologicity, the “biostatistical theory” (BST). The first issue is the charge by Accad, Fred, and Peter Schwartz that current risk-based categories confuse disease with mere risk of disease. I shall conclude that they are right, insofar as current definitions mark no genuine boundary between the normal and the pathological. The second conceptual criticism is my own: that whether a condition should get medical treatment and whether it is pathological, though distinct questions, are usually confused. This confusion seems just as prevalent, and influential, in the literature as that between disease and risk.
b. Schwartz’s critique
Let us now summarize Schwartz’s discussion. He imagines a woman MH, aged 60, with blood pressure 150/80 and LDL cholesterol level 140. MH’s blood-pressure level (even her systolic number) is near the median for women her age, and her cholesterol level is below it. Not surprisingly, then, until recently both conditions would have been viewed as normal, not pathological, and in no need of treatment. But accumulating evidence of increased risk of organ damage at high levels – of ocular or renal injury from high blood pressure, and of cardiovascular disease in either case – plus the discovery of drugs that can safely lower levels and reduce risk, have led medical authorities to continually expand the definitions of hypertension and hypercholesterolemia. For hypertension, the risk-based motivation for new criteria is explicit in the 2003 committee report; for cholesterol, even to calculate a normal level for a particular patient now requires scoring a set of “risk factors” such as age, smoking, and hypertension. By these new criteria, Schwartz’s patient now has two diagnosable diseases, shared by about half of all women her age.
But according to “dysfunction-requiring” (DR) analyses of what a pathological condition is, Schwartz concludes that neither condition is rightly called disease. As he says, both I and Wakefield require, for a disorder or pathological condition, that some part of the organism fail to perform one of its biological functions with (for me) not much less than average efficiency. Stage-1 hypertension, Schwartz says, involves no dysfunction of any of the organs which fail or suffer injury at much higher pressure, as in “urgent hypertension,” which is genuinely pathological. So only if one thought that the blood-pressure regulation system has the function of “minimizing future cardiovascular risk” could one claim that it was presently dysfunctional. But, he notes, on my account a function is a causal contribution to survival or reproduction at the current time or under specific possible circumstances. So claiming that a system has the function of reducing future risk is odd at least.
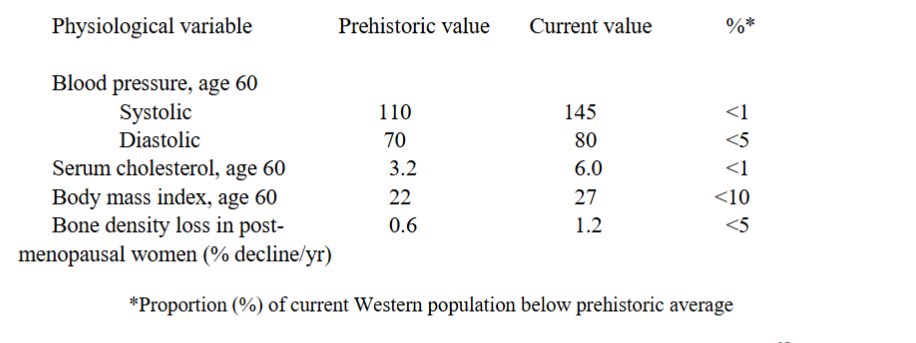
Already, then, according to Schwartz, stage-1 hypertension fails the dysfunction test. Moreover, even if one granted such a risk-reduction function, MH’s blood-pressure system is functioning at typical efficiency, since she is near the average for her age and sex. Schwartz does note that hunter-gatherer societies show much lower blood pressures; e.g., the median 60-year-old has 110/70. But if we judge normal function by a reference class including ancient humans, we must conclude from the risk data that contemporary people even in the current officially normal range are diseased – in fact, that “basically everybody living in contemporary society harbors dysfunction.” So, for either choice of reference class, stage-1 hypertension criteria fail to mark any true border between normality and disease. That is not to say, Schwartz observes, that such conditions should not be treated. On the contrary, it is even better to prevent disease than to cure it. Nevertheless, both conceptual clarity and honesty with patients require us to draw a clear line between risk and disease.
In sum, Schwartz offers three theses in his application of DR analyses of health to risk-based diseases like hypertension and high cholesterol:
- There is no necessary loss of function
- If there were a loss of function, it would be too prevalent to count as disease
- Hence, these conditions are not diseases.
To anticipate, my verdicts on these three theses will be: 1 Probably; 2 No; 3 Probably, and surely as defined by current ranges.
2. Narrowing the field: Osteoporosis, obesity, and diabetes mellitus
Before discussing Schwartz’s treatment of the two examples he does in detail, I wish to glance at the other three conditions he proposes as largely analogous: diabetes mellitus, osteoporosis, and obesity. Each of the five, I think, turns out different in its own way.
a. Osteoporosis
We can deal quickly with osteoporosis because it most clearly raises a different conceptual issue from the rest. As shown in the table, osteoporosis and its less severe twin, osteopenia, are conditions, common in postmenopausal women and in older men, of reduced mineral density of bone. Their definition and diagnosis rely on a measurement of bone mineral density (BMD), usually by X-ray. For women, osteopenia is defined as a BMD between 1 and 2.5 standard deviations below the mean of young, healthy women, and osteoporosis as a BMD more than 2.5 SD below. This results in a prevalence of 56% for one or the other in women over 50. People diagnosed with either condition may be treated with recommendations on lifestyle, such as diet and exercise, or with various drugs, especially bisphosphonates, in the hope of preventing the fractures which are more likely with weak, brittle bones. All this is similar to the other four conditions on Schwartz’s list. But there are three key differences. First, as with reference ranges, the bone-density conditions are defined via standard deviations in a statistical distribution. It is merely a distribution for young people, not for the patient’s age group. Second, the associated risk is risk of immediate, not future, pathology: broken bones. Third, this pathology is, precisely, failure of one of the main functions of bone structure. Thus, to recognize osteoporosis and osteopenia as diseases entails refusing to accept a functional decline typical of aging as normal if it can be reduced by therapy. On my account of health, typical functional declines with age count as normal. That is because I believed the view of traditional medicine to have been that functional limitations typical of an age group, whether young or old, are normal. One could, however, revise my analysis to count all functional declines after maturity as pathological. In that case, osteoporosis would become an ordinary disease of statistically subnormal function, not a risk factor misdescribed as pathological. It may be that osteoporosis is an early example of this important conceptual change in medicine. Anyway, the major issue about osteoporosis is simply whether to count typical aging as pathological – an issue also raised by several of the other four diseases, but dominant for osteoporosis.
b. Obesity and being overweight
At something like the opposite extreme of legitimacy are the categories of obesity and being overweight. Currently, for both children and adults, both categories are most often defined via body mass index (BMI), a simple function of height and weight. However, since BMI does not distinguish between fat and muscle, and I am not aware of claims that large muscles increase the risk of the diseases for which obesity is blamed, clearly on that definition, obesity per se is not pathological. BMI is best regarded as a crude correlate of obesity, suitable mainly for population studies. In the clinical context, various more accurate measures are common, such as four standard skin thicknesses or assorted radiologic techniques. The WHO report actually opens by citing a definition of obesity as “a condition of abnormal or excessive fat accumulation in adipose tissue, to the extent that health may be impaired.” Perhaps we should regard this idea, “excessive fat,” as the basic concept of being overweight or obesity, with all else best seen as diagnostic criteria. It is unclear, however, what ‘may’ means here: epistemic or metaphysical possibility. If the health impairment making fat excessive is to be present (epistemic), this definition defines no disease: fat that does not impair health cannot be pathological. If future (metaphysical), the definition seems intended to be risk-based.
In fact, however, for adults, the BMI-based categories are arbitrary, based neither on any population nor yet on risk data. The current definition for adults is overweight 25-29.9, obese ≥ 30, with several subcategories for increasingly severe obesity. This definition makes roughly three-quarters of Americans overweight or obese; indeed, in only one of 22 countries that WHO surveyed in 1983-6 was a majority of men not overweight by this definition. But, according to Eric Oliver, one of a sizeable group of “obesity skeptics,” WHO and the National Institutes of Health arrived at these ranges – which suddenly made 37 million Americans overweight overnight – with almost no empirical evidence. For example, the major source cited by the NIH board was a 1996 review of studies linking BMI and mortality by the nutritionist Richard Troiano and his associates. Yet, strangely enough, Troiano’s findings actually contradict most of the recommendations of the NIH panel. Not only did he discover that mortality was highest among the very thin as well as the very heavy, but also that the increased mortality was typically not evident until well beyond a BMI level of 30. And until one gets to a BMI of 40 or more, the differences in mortality are still within the bounds of statistical uncertainty. Ironically, although the NIH panel did recalibrate body weight recommendations [as Troiano recommended], they did so in the opposite direction, lowering the BMI designation of what would be considered overweight and obese.
Besides seeing no adequate evidence of increased risk of death or disease at BMI levels currently considered abnormal, many obesity skeptics claim that there is no good evidence that obesity is a causal, rather than a merely probabilistic, risk factor. Oliver regards any correlation as due to a common-cause situation: obesity is an effect of the same causes, probably mainly diet and lack of exercise, as the morbidity and mortality itself. Based on our current evidence, blaming obesity for heart disease, cancer, or many other ailments is like blaming smelly clothes, yellow teeth, or bad breath for lung cancer instead of cigarettes; it conflates an associated trait with its underlying cause. Although space permits no further analysis of obesity skepticism, one more point is worth noting. It is tempting to think that one can bypass all issues about the causal role of obesity in acknowledged diseases by calling its effects on physical fitness dysfunction. Ceteris paribus, the extra weight of fat limits nearly all physical activities. Less-fat people can run faster and farther, jump higher, and so on. Since locomotion and other physical activities are normal physiological functions of our musculoskeletal system, and we in the West are currently much fatter than other current humans and especially than humans in primitive societies past and present, perhaps we fall in the pathological tail of the human spectrum for such functions. But fat also has a function: energy storage. Fat Westerners could survive longer without food than thin, fit primitive people. How to balance these two points is not obvious. Should one assess the relative frequency of dangerous environments favoring running, and famine environments favoring fat, in the history of mankind? Which is a more important human ability: to run from a tiger or to fast like a bear?
c. Diabetes mellitus
By contrast, current diabetes classifications have bases very similar to those for hypertension and high cholesterol. Diabetes and prediabetes are syndromes of high blood sugar, which can eventually cause damage to organs such as the eyes, kidneys, heart, and legs. Like all of Schwartz’s examples, these conditions can be diagnosed purely by a clinical test, as shown in our table.
| Condition | 2-hour glucose (mmol/l) | Fasting glucose (mmol/l) | Hemoglobin A1c (mmol/l) |
|---|---|---|---|
| Normal | < 7.8 | < 6.1 | < 42 |
| Impaired fasting glucose (IFG) | < 7.8 | 6.1 – 7.0 | 42-46 |
| Impaired glucose tolerance (IGT) | 7.8 – 11.1 | < 7.0 | 42-46 |
| Diabetes mellitus | ≥11.1 | ≥7.0 | ≥46 |
The two middle categories together are called “intermediate hyperglycemia” or “prediabetes.” Current criteria are near to counting most Americans as abnormal, as do those for hypertension and obesity. Again, diabetes is like three others in Schwartz’s group in that there is a natural homeostatic system for regulating blood sugar, involving insulin secreted by islet cells of the pancreas and insulin receptors in target organs such as the liver. In type 1 (formerly called juvenile) diabetes, islet cells die, usually from autoimmune attack. In type 2 (formerly called adult-onset) diabetes, target-organ insulin receptors lose their sensitivity to insulin, with an accompanying decline in insulin secretion. The numerical ranges above originally resulted from evidence of increased risk of organ damage, plus the effectiveness of lifestyle, diet, and drug therapy. But in a revealing recent episode, the World Health Organization declined to follow the American Diabetes Association in lowering the fasting-glucose threshold for IFG still further to 5.6. I shall discuss its reasons shortly.
3. Evaluating Schwartz’s analysis
Having now excluded two of Schwartz’s examples from discussion, let us cast a critical eye on his analysis. First, it is not necessarily odd, as he claims, to assign a trait the function of preventing future disease. He says, correctly, that on my analysis functions are “contributions the system makes to survival and reproduction at the current time or under specific possible circumstances.” But since what the BST requires for perfect health is “functional readiness,” there is no reason why the situations in which the trait will be functional cannot be in the future, perhaps the distant future. This is typical in developmental normality or pathology. The embryological origins of the eyes cannot support vision until months after they appear; but their absence in an embryo is pathological. And many traits, such as reproductive organs like the uterus or vasa deferentia, develop in gestation or childhood to prepare for sexual situations that occur solely to adults. In the second place, many traits have the function of preventing disease. In a sense this is trivial on a functional account of health, but it is often true nontrivially as well. An important function of lymphocytes is to prevent infectious diseases. Consequently, I am not so sure as Schwartz that the blood-pressure or glucose-regulating system has no function of preventing future disease, even on my account of function. It might be still clearer on a selectionist account of function: one could imagine discovering that a homeostatic system for blood cholesterol had been developed by selection against heart attacks later in life.
Rather, to assign the blood-pressure system the function of reducing future risk seems odd only if we ignore the mechanism by which it does so. If a clinical variable V is truly a contributing cause of a disease D, there must be a mechanism by which V acts: a present enduring effect. Whatever this present trace is, it may well be a disease by ordinary standards. High cholesterol is a fine example of this point, though with one twist. After all, there is an obvious genuine disease in this context: atherosclerosis. The way that high cholesterol is thought to raise the risk of heart attacks or stroke is precisely by accelerating the deposition of fatty plaques, and later atheromas, in the walls of arteries, which either narrow the lumen or cause clots, eventually blocking blood flow to the heart or brain. If atherosclerosis is a disease, then high cholesterol is not just a dubiously pathological risk factor, but the cause of a hidden, true disease right now. The twist is that the atherosclerotic process begins in everyone in childhood. On the BST, this makes it impossible to call atherosclerosis itself pathological, as opposed to age-excessive atherosclerosis. Still, high cholesterol could cause age-excessive atherosclerosis. Likewise, similar true diseases, though without familiar names, result from hypertension and hyperglycemia. So, at least if we grant that the BST succeeds in calling such tissue changes pathological, it has no trouble finding at least a probability of diminished function here.
Now if a given cholesterol level raises the probability of age-excessive atherosclerosis, which helps cause heart attacks, may we not call it a disease in itself? If X helps cause Y and Y helps cause Z, doesn’t X help cause Z? Actually, on some interpretations, x is a contributory cause of y is not transitive. If X helps cause some cases of Y, while other cases of Y help cause Z, it may be that X never helps cause Z. PMS can cause anxiety, and anxiety can cause impotence, but PMS never causes impotence. Even if we assume transitivity, however, it still does not follow that high cholesterol is pathological in itself, if it only sometimes – not invariably – increases atherosclerosis. Take the simplest model: X (high cholesterol) and W (some other inherited factor, e.g., endothelial abnormality) are individually necessary and jointly sufficient to accelerate atherosclerosis (Y). By my account of function, in persons with X but ~W, ~W is, as I have said, performing the function of blocking this rise; likewise, in persons with W but ~X, ~X is performing that function. But the BST only declares absence of species-typical functions to be pathological. Now if one of X and W is declared a disease, by symmetry both must be. But if the prevalences of X and W are both under 50%, as they must be to be diseases on the BST, neither ~X nor ~W will have a species-typical function. For example, if independent X and W have prevalences of 30% each, neither ~X nor ~W performs the function in more than (0.3)(1 – 0.3) = 21% of the population. Thus, on the BST a condition XW can be pathogenic when neither X nor W is pathological. This is just another example of the fact (which I shall prove in §4) that what raises the probability of disease is not necessarily disease.
Because of this point, high cholesterol may not be pathological, but be only clinical evidence, perhaps weak, for age-excessive atherosclerosis. At any rate, if X and W are genetic risk factors necessary and jointly sufficient for disease, they cannot both be diseases on the BST. Is this the true situation with atherosclerosis and high cholesterol, and likewise for the other conditions? While our understanding of the pathogenesis of these diseases is incomplete, Giroux says that most of the time, one risk factor acts in concert with numerous others, each contributing only a small part of the risk. As to genetic factors, Prohaska et al. agree: Arguably, the most important trend emerging from [large-scale genome-wide association studies] is that most complex disease traits are highly polygenic, affected by many thousands of variants with individually small effects, often only indirectly related to core disease pathways, and that trait-associated variants naturally vary in frequency across the globe.
So, my verdict on Schwartz’s first thesis – no diminished function – is “probably.” It depends, at any rate, on the strength of the link between high cholesterol and accelerated atherosclerosis, or the comparable link to early pathology in other cases – that is, on the size of P(D∣R) for each disease D and factor R.
As to Schwartz’s second thesis – current prevalence is too high for pathology – I do not agree that what is normal or pathological must be determined by “the current population.” On the contrary, I have proposed using a significant time-slice of a species’ history as the reference class, saying that species design is constant except on “evolutionary time scales.” We should not be afraid to say that “basically everybody living in contemporary society harbors dysfunction.” Here again, Schwartz is thinking like the clinician he is, rather than like a pathologist, who would find it a commonplace that every human body shows some pathology. Indeed, essentially all children and adults have some skin pathology, in particular. Similarly, there is no reason why every present human body should not be atypical of the species’ history by showing the same pathology. I am sympathetic to the idea of “Western diseases,” and the clinical data on members of primitive societies are fascinating.
Wald and Law’s main thesis, supported by data, is in fact a near-consensus: there are no thresholds for the effectiveness of treating risk factors. Rather, “a given change in the variables reduces the risk of disease by a constant proportion of the existing risk irrespective of the starting level of the variable or of the existing risk.” Everyone at a certain risk level needs treatment, and this will often include most of the contemporary population. While this is a tenable position, it is inconsistent with current criteria for disease.
Indeed, this is true for both the full-blown diseases and their “precursors.” As Schwartz says, from the hunter-gatherer viewpoint “the current cutoffs for diagnosing stage 1 hypertension would make little sense.” But the same holds for prehypertension or prediabetes. Even using contemporary data, the 2003 JNC-7 hypertension report says: “[D]eath from both ischemic heart disease and stroke increases progressively and linearly from BP levels as low as 115 mm Hg systolic and 75 mm Hg diastolic upward.” 115 is below the threshold for “prehypertension,” in the range called “normal.” Similarly, if a precursor disease to hypercholesterolemia were defined, presumably its boundaries too would fail to exclude all levels of increased risk, since the rise begins at levels as low as 160-199 TC. Likewise, the WHO diabetes report shows prevalence of retinopathy first rising at about the 40th percentile of fasting glucose, while “[t]he hazard of coronary mortality rose in a linear fashion from a threshold 2-h blood glucose of 4.6 mmol/l” – the lower limit of IGT being 7.8! This report repeatedly stresses, for this test, the basic Wald-Law point: for all these conditions, risk of disease increases monotonically at nearly all levels, usually with no detectable threshold.
Hence, it is not merely the risk level that is determining current diagnostic cutpoints, but also, as Schwartz said, its modifiability – the availability of beneficial treatment. This alone suggests that the conditions we are discussing are no conventional diseases. In traditional medicine, treatability of a condition is irrelevant to whether it is pathological. Not only was there no effective treatment of typical diseases during most of the history of medicine, but the best physicians, in retrospect, were those who, like Sydenham, openly admitted this fact. In doing so, they in no way contradicted the disease judgment. Conversely, many conditions treated today, such as unwanted fertility or pregnancy, are still not called pathological.
Charitably, one might imagine that official bodies are using treatability today simply to prove causation – to distinguish between causal and noncausal risk factors. But, in the first place, no such need is plausible: if risk from a clinical variable is monotonic in some range and causation exists in most of it, it is likely to exist in all of it. Besides, official reports openly use treatment criteria with no bearing on causation. For example, the NCEP-III cholesterol report has a paragraph explaining how its classification balances risk with “cost-effectiveness” of treatment. “[A]s drug prices decline it will be possible to extend drug use to lower-risk persons and still be cost-effective.” Thus, if the NCEP-III framework is taken to define a condition of hypercholesterolemia, whether a patient has this condition depends on how much it costs to cure it. Such a criterion has no role in traditional concepts of disease, and for excellent reasons. If the test of disease is affordable treatability, the same condition of the same patient will be normal or pathological at different times and places, depending on his society’s health-care budget, which is peculiar.
The best example of how extraneous factors now influence disease classification is the WHO diabetes report. A long section explains WHO’s decision not to follow the American Diabetes Association in lowering the diagnostic threshold for IFG. First, for such a reduction, WHO found “a lack of evidence of any benefit in terms of reducing adverse outcomes or progression to diabetes.” Its summary of its further reasoning in refusing the change is instructive:
Since risk of adverse outcomes and future diabetes is continuous across the fasting plasma glucose range, the cut-point chosen to define IFG will be somewhat arbitrary. Therefore, other considerations should be taken into account in recommending a cut-point. The Group considered the following points relevant …. Outcomes mortality, cardiovascular disease, microvascular complications, incident diabetes; Prevention of premature mortality and cardiovascular disease progression to diabetes; Impact on prevalence of IFG; Concordance of IFG and IGT; Risk profile of individuals identified with IFG; Economic considerations and cost implications; Implications for health services and policy.
Note, first, the consideration of prevalence. The ADA criteria would have raised the prevalence of IFG in the US from 9.5% to 28.5%, and in India from 10.6% to 37.6%; but, at least from the Wald-Law viewpoint, these facts seem irrelevant. Their main relevance seems to come from the economics of health care – e.g., the explicit fear that to recognize more IFG cases would steal resources from IGT or from diabetes itself. Thus, we see again how current definitions of normal and abnormal depend not just on modifiable risk, but on extraneous factors as well.
Also, the terminology of the diabetes and hypertension reports shows how categories defined via continuous risk factors strain traditional concepts of medicine. The diabetes report calls both diabetes and intermediate hyperglycemia “disorders,” in contrast with “normal glucose regulation.” Yet it also says: “IFG, as with IGT, is a not clinical entity but rather a risk factor for future diabetes and adverse outcomes.” Why are these conditions not “clinical entities,” if they are both abnormal and clinically defined? Stranger still is the language of various expert-committee hypertension reports. The frameworks of three standard reports are as follows:
| SBP/DBP | JNC 6 Category (1997) | JNC 7 Category (2003) | American Heart Association SBP/DBP |
|---|---|---|---|
| <120/80 | Optimal | Normal | Normal <120 and <80 |
| 120-129 and <80 | Normal | Elevated | 120-129/80-84 |
| 130-39/85-89 | Borderline Hypertension | Hypertension | >=130 or >=80 |
| >=140/90 | Hypertension | Stage 1 | Stage 2 >=140 or >=90 |
| 140-159/90-99 | Stage 1 | Stage 1 | Stage 1 |
| 160-179/100-109 | Stage 2 | Stage 2 | Stage 2 |
| >=180/110 | Stage 3 | Stage 3 | Stage 3 |
These frameworks, and controversies over them, again show confused terminology. The main changes from JNC-6 to JNC-7 were that what was previously “optimal” is now “normal,” while what was previously “normal” or “borderline” is now “prehypertension.” Thus the classification became stricter for patients in the 120-129/80-84 range. But, first, since ‘hypertension’ simply means too-high pressure, if “prehypertension” is not normal – i.e., is pathological – then it should be part of the disorder called hypertension. Why isn’t it? Worse yet, the JNC-7 report, like the WHO diabetes report, states: “Prehypertension is not a disease category. Rather it is a designation chosen to identify individuals at high risk of developing hypertension …” So prehypertension is not normal, but not pathological either – something novel and logically mysterious.
What we see here is a conceptual collision between preventive and therapeutic medicine. The JNC-7 writers think that prehypertensive patients need “intervention” by “firm” advice to modify their “lifestyle,” so as to delay or prevent future hypertension. But the authors decline to describe these patients as diseased, or prescribe drugs for them without diabetes or chronic kidney disease. This suggests that a diseased patient is being understood as one who needs specifically medical treatment. As I noted earlier, that is a clear error: being normal or pathological has nothing to do with medical treatment. At any rate, Schwartz and Accad are surely right. Growing conflation of the categories of preventive and therapeutic medicine is flooding the market with counterfeit diseases – risk-factor levels masquerading as pathology. This conclusion is inevitable unless we can say that the authors of the new classifications see them as mere treatment recommendations, not as defining diseases. But we have seen frequent evidence to the contrary. Most official or semi-official medical sources clearly treat these classifications as disease definitions, as do Doust and her coauthors in suggesting a redefinition checklist.
To prevent disease is, of course, an admirable goal, fully justifying medical treatment, including drugs. Indeed, as Schwartz said, preventing disease is usually even better than curing it; hence the proverb, “An ounce of prevention is worth a pound of cure.” But prevention needs its own vocabulary. To pour the new wine of risk into the old wineskins of disease will burst them with conceptual confusion. As to the conditions we have been discussing, within classic medical terminology there are two clean positions. One is Schwartz’s: hypertension, diabetes mellitus, and high cholesterol, and a fortiori the first two’s precursors, as currently defined, are not genuine diseases – either because there is no loss of function, or because such loss affects too much of the contemporary population. The other position, provided we assume loss of function, is Wald and Law’s: not only are all these conditions, including precursors, pathological, but pathology begins far below current diagnostic cutpoints. Schwartz does not dispute, while Wald and Law reject, official bodies’ choice of these points as thresholds for treatment. But on neither the Schwartz nor the Wald-Law view are these thresholds borders between health and disease.
4. Why should risk of disease not be disease?
Even if, in traditional medical thought, risk of disease is not disease, why should we not merge the two into a single category? To begin with, risk of X is not in general a kind of X. One who risks death is still alive, not already dead. A risk of fire burns nothing; a chance of rain waters no plants and ruins no picnics. Even if present disease and risk of future disease can both justify medical treatment, that does not imply that they are the same thing. In the second place, of course, if risk of disease is disease, then so is risk of risk of disease, and so on. The concept becomes recursive, embracing not just the “precursor” conditions, but much more besides.
Still, if we are to give the risk principle a fair hearing, we must first clarify it. In the original and simplest sense, a risk factor R for disease D is any condition given which D has higher probability. In terms of conditional probability, R is a risk factor for D whenever P(D|R) > P(D|~R), or, equivalently, when the conditional probability P(D|R) > P(D), the unconditional probability of D. This is a very weak sense, since there is no implication of causation; for that reason, some writers prefer the term “risk marker” for it. In this sense, a child’s going to a pediatrician is a risk factor for having an ear infection; having antibodies to Vibrio cholerae is a risk factor for having cholera, etc. Two conditions can easily be risk factors for each other, even within the realm of diseases: for example, having uterine cancer is a risk factor for having ovarian cancer and vice versa, since either shows female sex and female sex raises the probability of either cancer. But neither epidemiologists nor analysts of the concept of disease are interested in this weak sense, even with the obvious additional requirement that R precede D. No one in medicine cares about an R that is a risk factor for D only in the same way that wearing a flowered shirt is a risk factor for being killed by a volcano.
Despite the points I began with, some writers have argued that risk either is, or should be, part of the concept of disease. Among philosophers, Culver and Gert define a malady as a condition, other than [a person’s] rational beliefs and desires, such that he is suffering, or at increased risk of suffering, an evil (death, pain, disability, loss of freedom or opportunity, or loss of pleasure) in the absence of a distinct sustaining cause. But as Culver and Gert were forced to admit, this definition counts pregnancy, menopause, and any menstrual discomfort as maladies. Although they defend this result, it proves that whatever their definition is, it is not an analysis of the medical, or even lay, concept of disease or pathological condition.
Among physicians, four surgeons proposed in Science to define disease as “a state that places individuals at increased risk of adverse consequences.” One obvious defect in this definition is that many normal conditions increase risk of disease or death. Inability to fly, breathe underwater, digest cellulose, or smell carbon monoxide has killed millions of human beings; but these are universal normal conditions. To be fair, the Science authors refer several times to “deviations from normal” or “abnormality,” though they fail to include it in their just-quoted definition. Since these terms cannot mean medical abnormality in the sense of disease – that would make the definition circular – presumably they mean statistical abnormality. But even if we add statistical abnormality to their definition, pregnancy and, until recently, male sex are counterexamples if mortality is the test. It is also disadvantageous in other ways to be mildly shorter, uglier, and stupider than average, and especially to be all three. But not even the combination of these three, or of three hundred more pieces of bad genetic luck, is pathological. It would be a huge departure from traditional medical thought to count all significant genetic bad luck as pathological. And the doctrine that whatever increases risk of death is pathology would revolutionize psychiatry, where pursuit of a riskier profession (firefighting, the military) has never been regarded as a mental disorder. These objections are fatal to the Science writers’ definition even before they relativize adversity to culture, on the grounds that menopause is “a medical condition” in North America but not elsewhere. In that case, black skin was a disease in the American South, and having a clitoris is a disease in north Africa today. Both judgments are nonsense.
In any case, it is clear that no one in medicine is willing to declare every significant risk factor for disease, even every statistically abnormal one, a disease. As to sex, there are many diseases that both sexes can get, but males are more likely to get than females (myocardial infarction) or vice versa (systemic lupus erythematosus). Similar differences exist between races: Asians and Hispanics are more susceptible to thalassemia, Ashkenazi Jews to Tay-Sachs, Africans to sickle-cell disease, and Caucasians to cystic fibrosis. No doubt every minority racial group has a higher risk of some disease, but their races can’t all be pathological, else there would be no normal human beings. Nor does it help to limit the principle by demanding a difference not just in the prevalence of specific diseases, but in life expectancy. Women’s life expectancy is substantially greater than men’s, and men were a minority of our species before the mid-1960’s. As to race, with white all-cause mortality at 1.01 in the U.S., the figures for other groups are African-American 1.32, American Indian 0.84, Hispanic 0.78, and Asian 0.60. The same story holds for somatotypes: ectomorphs, endomorphs, and mesomorphs have both unequal risk of specific diseases and unequal life expectancies. Yet no one is ready to call sex, race, and somatotype pathological conditions rather than normal variants.
It might be objected that all these effects are due not to sex, race or somatotype themselves, but to the groups’ varying concentrations of specific genes. A defender of the risk principle might also try to save it by adding a treatability requirement: sex, race, and somatotype are not (currently) changeable. In any event, both objections fall to two simple examples: testes and the postmenopausal uterus. In Hamilton and Mestler’s study, eunuchs lived an average of 13.5 years longer than normal white males under the same conditions. Testes and uteri are both causal and removable. And since frozen sperm and ova are just as effective as fresh ones, testes or ovaries can be removed without loss of reproductive function. Likewise, a uterus after menopause has no function. Nevertheless, anyone tempted to call these organs pathological for their cancer risk simply has no idea what the term means; they are normal parts of human anatomy and physiology, as normal as anything can be.
Since no one applies the risk principle consistently, Accad, Fred, and Schwartz are right: intellectual integrity demands that we stop calling mere risk factors diseases. And there are at least two practical reasons why it may be important to patients’ welfare to separate the two categories. First are the concerns about overdiagnosis already mentioned. In particular, one must worry about psychological harm from giving 75% of the population a diagnosis of disease. Secondly, continual expansion of disease definitions may backfire by exhausting patients’ will to follow medical advice. At some point, the Western population may rebel against the “perpetual birth of risk factors” and physicians’ ever-increasing, seemingly perfectionistic demands to eradicate them. Yet widespread alienation from medicine might harm population health as much as aggressive risk-reduction can help it. For these reasons, conceptual honesty, as well as being a scientific virtue, may be the best public-health policy.
5. Two alternative medical frameworks
Our discussion would be incomplete without mentioning two alternative conceptual frameworks proposed by physicians. One is Anthony Viera’s three-way classification: risk factors, predisease, and disease.
a. Viera on predisease
Besides writers mentioned above, the only discussion I have found of protodisease states is Viera’s analysis and critique of the recently popular category of “predisease.” He writes: Screening often leads to finding conditions that are not at the stage or level that would classify them as disease but, at the same time, are not at a stage or level at which people can be declared entirely disease free. These “in-between” states have sometimes been designated as “predisease.” Examples include precancerous lesions, increased intraocular pressure (“preglaucoma”), prediabetes, and prehypertension. To these examples he later adds osteopenia, latent TB infection, subclinical thyroid dysfunction, and mild cognitive impairment. Especially in relation to screening programs, Viera’s goal is to state conditions under which it is helpful to recognize predisease as a “category on which to act.” He comes up with three requirements: (1) substantially increased risk, (2) effective treatment, and (3) greater benefit than harm.
First, a predisease must carry a high risk – much greater than that of a mere “risk factor” – of progressing to full-blown disease without treatment. In other words, the predisease diagnosis must do an excellent job of discriminating between people who will and will not develop the disease. Second, since predisease will usually be treated, an effective treatment must exist, and third, it must do more good than harm. Viera uses these criteria to analyze four examples. He concludes that screening for cervical intraepithelial neoplasia passes all three tests: although there are some harms from labeling many young women with a “precancerous lesion,” the benefits of treating moderate or severe hyperplasia outweigh them. As to “ocular hypertension,” its ability to predict future glaucoma is weak and evidence of the benefit of treating it is lacking, so a predisease category is unjustified. Viera’s verdict on prehypertension and prediabetes is complex. While lifestyle changes can be effective and to counsel them is probably harmless, to link such advice to a label of predisease, he thinks, probably does little to make it more effective and the label itself causes some harm (“psychological stress and adoption of the ‘sick role’”). Viera is skeptical that a predisease diagnosis is better than the alternative of simple “risk prediction”: to tell each patient his numerical risk of future disease. Viera ends by suggesting that while screening implies a strategy of focusing on a “high-risk” group, a contrasting “population strategy” – e.g., to try to “shift the entire blood pressure distribution curve to the left” – “almost always offers the most potential for prevention.” In this connection, he notes that in countries such as the United States, where the lifetime prevalence of hypertension is 90%, virtually everyone has ‘prehypertension’. The “cases” of hypertension do not come from just a high-risk group; they come from all groups.
b. Risk evaluation instead of diagnosis
Vickers, Basch, and Kattan suggest that for some types of conditions, an individualized risk prediction is better than diagnosis. The act of diagnosis requires that patients be placed in a binary category of either having or not having a certain disease. Accordingly, the diseases of particular concern for industrialized countries – such as type 2 diabetes, obesity, or depression – require that a somewhat arbitrary cut-point be chosen on a continuous scale of measurement. These cut-points do not adequately reflect disease biology, may inappropriately treat patients on either side of the cut-point as two homogenous risk groups, fail to incorporate other risk factors, and are invariable to patient preference.
Vickers et al. see two important advantages for individualized risk prediction. First, a statistical analysis ideally can include multiple risk factors, as is already done in guidelines for cholesterol reduction based on the Framingham Risk Calculator. Second, patients easily understand risk and can weigh different “probabilities of events” according to their own values, without suffering the harms of disease labeling.
Vickers et al. suggest that the diagnostic and risk-prediction frameworks suit different conditions. Ideally, candidates for classic diagnosis are like syphilis or a torn aorta, which contrast with hypertension, hypercholesterolemia, or early prostate cancer in the ways shown in their table:
| Variable | Diagnosis | Risk prediction |
|---|---|---|
| Approach | Patients are given a diagnosis: Either they have the disease or they do not | Patients are given a probability of a future event |
| Lesion | Unambiguous | Nonexistent or equivocal |
| Treatment effectiveness | Often highly effective | Helpful, but patients may have event with treatment or avoid the event even if untreated |
| Course of treatment | Dictated by diagnosis | Open to discussion |
| Patient preference | Generally of minor importance | Often of major importance |
| Symptoms | Patient has distressing symptoms | Patient is often asymptomatic: Disorder is a risk factor for a future event |
To some degree, these writers exaggerate the difference between the two frameworks. It is, of course, untrue that giving two patients the same diagnosis means that their treatment must be the same. Most classic diseases already show a “range of severity,” often being divided, as the writers mention, into “stages” for which treatment may vary, with or without comorbidities. Risk prediction is, in a sense, just the limit of infinitely progressive subclassification. And there are many well-established diseases, such as hyperthyroidism and hypothyroidism, which are, like hypertension, just extremes of a population distribution. Still, the risk-prediction framework may help physicians smoothly incorporate statistical information, while deterring the fallacy of viewing each diagnosis as a “homogenous risk group.” And these writers’ position perfectly fits Accad, Fred, and Schwartz’s demands for medicine to stop confusing risk factors with disease.
6. Summary
Considering this paper’s somewhat complex discussion, readers may appreciate a summary of its conclusions.
- Today many medical conditions are defined purely by levels of a clinical variable. These levels are often (hypertension, hypercholesterolemia), though not always (obesity), based on data about modifiable risk, as well as on treatment costs (diabetes mellitus).
- It is a scientific consensus that for many of these variables, risk increases monotonically, even (log)-linearly, across nearly the whole population distribution.
- Precursor (or predisease) conditions defined on the same clinical spectrum are nearly as good, or bad, candidates for disease, except when they increase prevalence to more than half the human species, which is impossible if the opposite of ‘pathological’ is ‘normal’.
- For many of these conditions, it is unclear whether they involve biological part-dysfunction, which is necessary (Boorse, Wakefield) for genuine disease. Even if they do, current cutpoints, especially with precursors included, look either too low (Schwartz) or too high (Law and Wald). If we trust Law and Wald’s figures on primitive man, then, assuming loss of function, the regions of, e.g., high blood pressure in current classifications may all be pathological, but there still is no reason to think that their boundaries are boundaries of true disease.
- No one is willing to consistently apply the principle that risk of disease is itself disease.
- In classic medical thought, the line between normal and pathological has nothing to do with availability or cost of treatment.
- In view of 1-6, current definitions of hypertension, hypercholesterolemia, diabetes mellitus, and similar conditions mark out no genuine diseases, or even diagnostic criteria for genuine diseases. Since they are usually taken to do so, they are risk factors masquerading as disease (Accad, Fred, and Schwartz).
- Such categories, however, may well be reasonable bases for treatment decisions, by drugs or otherwise. Properly viewed, they are treatment classes, not disease classes.
- Alternatively, where possible, patients may be given a statistically-based individual risk computation, to help them choose among treatments by their own preferences.
I thank my colleagues at University of Delaware, especially Mark Greene, for their help with this paper. And I am grateful to Jefferson Medical College for the privilege of attending lectures in pathology and clinical medicine, first in the 1980’s and again in 2012. Most of what I know about medicine I learned beneath Jefferson’s winged ox.
ENDNOTES
- (957). See also the editorials by Accad and Herbert L. Fred.
- Another philosopher to tackle this topic is Giroux.
- American terminology and criteria differ somewhat from their British and European counterparts; see discussion below in text.
- Again, there is some variation in different sources; see text below.
- One kind of evidence for this view is classification of a precursor in WHO’s International Classification of Diseases. For example, the ICD-10 index entry for ‘overweight’ refers to E66.9 (“obesity, unspecified”), in the category “Endocrine, Nutritional, and Metabolic Diseases.” “Prediabetes” (R73.0) and “hyperglycemia” (R73.9) are placed in a different section called “Symptoms, Signs, and Abnormal Clinical and Laboratory Findings.” While some conditions in this section are disease-free (e.g., R76.2, false-positive Wasserman), not all are (R04.8, pulmonary hemorrhage; R57, shock; R98, unattended death). As for ICD-11, it calls all my precursors “disorders,” except prehypertension.
- For example, blood pressure is regulated by a cardiovascular control center in the medulla oblongata. Reacting to pressure information from baroreceptors in the carotid arteries and aorta, this center raises or lowers pressure by sympathetic and parasympathetic signals to arteriolar smooth muscle, the ventricular myocardium, and the sino-atrial node to change peripheral resistance, the force of ventricular contraction, and heart rate. Additional regulation occurs via hormonal pathways, such as the renin-angiotensin system. For further details, see any textbook of human physiology, such as Silverthorn.
- The first two of these categories are distinguished by Peter Hucklenbroich.
- However, the HbA1c levels shown in the table below are best regarded as only convenient diagnostic criteria, since they have no direct relation to the glucose measures which (if accurate) define the disease.
- Welch defines overdiagnosis as diagnosing “individuals … with conditions that will never cause symptoms or death.” However, his later statement that such conditions are only “pseudodiseases” is untenable. It apparently rests on the etymological fallacy; in reality, ‘disease’ is not even pronounced as “dis-ease,” let alone meaning unease, which can arise from many normal processes like hunger, heat, cold, fear, loneliness, and so on. In any case, Welch’s position implies that an asymptomatic cancer, which would be fatal in time, is not a disease at all if some other cancer kills the patient first. To call the same lesion a disease in one patient but not in another does not fit medical usage.
- Greene notes that in the debate over chlorothiazide, the first blood-pressure drug, “the question of who to treat began to redefine what was normal …. [T]he threshold of the pathological became tied to explicitly pragmatic concerns of treatment efficacy and preventive benefit.”
- “The ultimate public health goal of antihypertensive therapy is to reduce cardiovascular and renal morbidity and mortality.” JNC-6 (1216). Similarly, the 2017 guidelines by the American Heart Association and eleven other professional bodies state: “As was the case in previous BP classification systems, the choice and the naming of the categories were based on a pragmatic interpretation of BP-related CVD risk and benefit of BP reduction in clinical trials.”
- For my biostatistical theory (or BST), see Boorse. For Wakefield’s account, see his (1992) and (1999). The main differences between them are these: (1) Wakefield adds a harm clause to the dysfunction clause; (2) he has a selectionist analysis of function, while I have a goal-contribution account; (3) he believes evolution, not population statistics, determines the normal range of a function; and (4) like Culver and Gert, he excludes disorders maintained by an environmental cause. For more, see my survey chapter.
- In two recent papers, Nicholas Binney shows that current osteoporosis diagnosis diverges in many other ways from the reference class in my BST. He shows that older men are also judged in comparison to young women, and that sometimes population-specific, pathological, or even health-adjusted reference classes are used. Pediatricians, moreover, adjust BMD scores for factors such as pubertal status, bone age, height age, body size, and muscle mass. Space permits no discussion of these issues here.
- Children are judged by data from American children in 1963-70, and called overweight if they are above the 85th percentile for their sex and age group, obese if above the 95th or have BMI above 30. That is, child obesity, like osteopenia and osteoporosis, is currently defined via a statistical distribution, as is reasonable on the BST provided other requirements are met.
- WHO, figure p. 18, p. 20. The only exception was China.
- For two other skeptical surveys, see Gard and Wright and Gard’s supplement, which includes an analytical survey of obesity skeptics themselves; and Taubes. An exposé of the wretched quality of nutritional science underlying dietary recommendations about fat consumption is Teicholz.
- Highlighting the contrast, Accad complains that some advocates of risk-factor medicine oppose research on tools to measure early atherosclerosis.
- Mild chronic hypertension causes a thickening of arterial and arteriolar walls (hyaline arteriosclerosis), which narrows the interior of the vessel. In arterioles this occurs via thickening of the basement membrane and accumulation of plasma proteins; in arteries, new elastin and connective tissue is added. Hypertension also accelerates atherosclerosis as well. Rubin et al.; Cotran et al.
- Hyperglycemia also has each of the above effects, but via the mechanism of glycosylation of numerous cellular proteins. This process progressively causes the characteristic biochemical lesion of irreversible advanced glycosylation end products, a permanent change in protein structure. Rubin et al.; Cotran et al.
- Some writers have criticized the BST for being unable to count early stages of diseases, e.g., cancer, as pathological. My reply has been that early cancer by definition involves cellular dysfunction, while any other early-stage conditions without dysfunction are not yet disease. If the early pathology in our three sample conditions does not involve tissue dysfunction, that is an objection to the BST, since it is quite clear that at least age-excessive atherosclerosis is viewed as a disease at every stage.
- If factor W is not genetic, however, then W could be the occasion for ~X to exercise its function in the whole species. In general, functions are performed only on suitable occasions. Even when factor W is genetic, I am not sure whether Wakefield would reach the same conclusion as I do about X and W. He seems willing to judge normality by reference classes smaller than a species or subspecies, as in his example of north-oriented bacteria. So perhaps he, or other selectionist writers, would consider ~X to have the function of preventing D, at least in the population of W-bearers, if selection were favoring it by that effect. Whether it would then also have such a function in the whole population is unclear to me.
- This consensus ultimately derives from the great mid-20th-century hypertension authority George Pickering, who often criticized “the fallacy of the dividing line”: The practice of making a sharp division between normal and pathologically high pressure is entirely arbitrary and is in the nature of an artefact. … In fact, arterial pressure seems to behave as a graded characteristic: the differences between the lower pressures and the higher are quantitative, not qualitative; they are differences of degree, not of kind.
- As a practical application of their ideas, Wald and Law proposed and patented a “polypill” to be taken by everyone over 55. It would contain three blood-pressure drugs (a diuretic, a beta-blocker, and an ACE inhibitor), a statin, aspirin, and folic acid.
- Sydenham wrote that often in his practice, “I have consulted my patients’ safety and my own reputation most effectually by doing nothing at all.” He also said: “I confidently affirm that the greater part of those who are supposed to have died of gout, have died of the medicine rather than the disease – a statement in which I am supported by observation.”
- One might think NCEP’s actual definition of hypercholesterolemia to be total cholesterol ≥240, with the more complicated risk-factor scheme being only guidelines for therapy. The trouble with this view is that no one really regards 240 TC as a boundary between normal and pathological, any more than anyone regards BMI ≥30 as defining obesity. In that case, a patient with, say, 170 LDL, 150 triglycerides and 39 HDL would be healthier than another with 124 LDL, 150 triglycerides and 87 HDL, which no one believes. The problem is that TC (= HDL + LDL + 20% triglycerides) fails to distinguish between LDL and HDL, just as BMI fails to distinguish fat from muscle.
- Thanks to David Hershenov for this “Cambridge-change” objection.
- An amusing separate confusion is that the National Heart Foundation of Australia, European Society of Hypertension, and British Hypertension Society schemes all call JNC-6’s “borderline” patients’ pressure “high normal,” as distinct from their next lower “normal” group. Obviously, whatever the normal range is, it must include “high normal.” A big fish is still a fish. So many official bodies abandon not only classic medical concepts, but elementary logic itself.
- At first sight, the AHA et al.’s rival 2017 classification may disconfirm this equation of disease status with medical treatability. This report shifts all JNC-7’s “prehypertensives” into stage-1 hypertension, but its only changes in recommended treatment are to extend drug treatment within the high-risk subgroup of (former) prehypertensives to those with a 10-year CVD Framingham risk of ≥10%, and to lower the goal of drug therapy to 130/80 for patients under 65 and <130 for those over 65. Thus it combines a large change in classification with a fairly small change in treatment, which looks inconsistent with the notion that diseased people are those who need medical therapy. Still, the report repeatedly calls lifestyle advice “nonpharmacological therapy,” as do its critics. So perhaps the new classification is still guided by an equation of pathologicity to medical treatability, just with a broader view of what medical therapy is. Since no other explanation of the new classification but redefining medical treatment appears in the report, the change is otherwise a mystery.
- The AHA report provoked significant controversy, but the complaints against it mostly focus on its treatment recommendations. See Moynihan, Clark, and Albarqouni and Whelton and Williams. Some critics, however, such as Bell, Doust, and Glasziou, add concerns about “potential incremental harms from disease labeling,” specifically the “risk of anxiety and depression” and blockage of insurance by a “preexisting condition.”
- One can only wonder to what degree recent disease classifications, including ICD-10, rest simply on the reluctance of most physicians to prescribe drugs, and of insurance companies to pay for them, without a disease diagnosis. In reality, there is no ethical objection to disease-preventing drugs, if the risk-benefit balance is favorable.
- Already, however, it is not clear that all the risk factors cited in definitions of hypertension and hypercholesterolemia are causal ones. Strictly speaking, a family history of early cardiovascular disease cannot cause a heart attack in a current patient. It only raises the probability that the family member had genes which, again with some probability, the patient inherited, in which case the two heart attacks would have a sort of common cause. Family history per se causes nothing. Giroux is also right to note that other risk factors are not states of the patient, but habits (smoking) or features of the environment. Such conditions could not possibly be diseases even if they helped cause disease.
- I say “significant” because the authors later require significant risk for a disease; a “genetic variation” with “minimal” risk of adversity, they say, should just be called a risk factor and left untreated.
- I thank Peter Schwartz for the uterus example.
- Besides the two reasons in my text, Schwartz also suggests that it is important for patients to see hypertension, high cholesterol, and so