





Breast Skin Resistance to Protease in Aging: A Study
Comparison of breast skin resistance against protease digestion between young and elderly individual based on attenuation-of-sound values
Katsutoshi Miura1, Toshihide Iwashita1
- Department of Regenerative & Infectious Pathology, Hamamatsu University School of Medicine, Japan
OPEN ACCESS
PUBLISHED 31 October 2024
CITATION Miura, K., and Iwashita, T., 2024. Comparison of breast skin resistance against protease digestion between young and elderly individual based on attenuation-of-sound values. Medical Research Archives, [online] 12(10). https://doi.org/10.18103/mra.v12i10.5934
DOI https://doi.org/10.18103/mra.v12i10.5934
ISSN 2375-1924
ABSTRACT
The skin is a gateway through which bacteria can establish infection. Evidence has shown that the components of the skin change with age, with elderly individuals exhibiting fewer epidermal rete ridges, dermal collagen, and elastic fibers. In the present study, paraffin sections of breast skin were digested with proteolytic enzymes of bacterial origin, after which skin fragility was assessed by observing attenuation-of-sound (AOS) images over time. Accordingly, studies have shown that AOS values are correlated with tissue viscosity and can serve as a numerical indicator of protein density. Breast skin sections were digested using two types of collagenases and actinase E, a broader peptidase. Notably, our results showed that skin sections from young and elderly patients showed resistance to digestion with the two types of collagenases. However, the epidermis and dermis were successfully digested using actinase over time. All layers of the epidermis, except for the keratin layer, were digested, whereas collagen and elastic fibers in the dermis were broken down, along with a decrease in AOS levels. Although actinase affected both young and aged skin, elderly skin showed much lower AOS values given its naturally reduced thickness and density due to aging. This finding suggests that older patients experience greater damage from proteolytic enzymes. AOS is an excellent approach to visualizing the process of protease digestion over time and statistically comparing proteolytic damage.
Keywords
breast skin, protease digestion, attenuation-of-sound, aging, skin fragility
INTRODUCTION
The skin, which comes in direct contact with the outside environment, is susceptible to trauma, creating a gateway through which pathogens, such as bacteria, invade the body. Studies have shown that aging affects the structure and function of the skin. Histologic changes associated with aging include decreased collagen and elastic fiber production, epidermal thinning with loss of rete ridges, reduced blood flow, and reduced fat content. These alterations induce dry, pale skin with decreased elasticity and increased fragility. Skin aging can be categorized into two types: intrinsic and extrinsic. Intrinsic aging refers to the inevitable physiologic changes occurring with time and genetic and hormonal factors, whereas extrinsic refers to aging that occurs with environmental factors, such as ultraviolet radiation. Bacterial infections develop when bacteria enter through hair follicles or through small breaks in the skin caused by surgery, burns, animal or insect bites, wounds, and pre-existing skin disorders. The prevalence of skin colonization by Proteus mirabilis and Pseudomonas aeruginosa in the over-65-year-old population has increased by about 25% compared with younger people. Bacterial skin and soft tissue infections can occur frequently and occasionally induce life-threatening conditions, such as necrotizing fascitis. Skin and soft tissue infections increased almost two-fold in older adults (>65 years of age), whereas children and adolescents declined 50%. Hence, elderly people are at a particularly high risk for developing skin infections.
Following mastectomy, the skin covering the breast can be a target of infection given that it is exposed to proteolytic enzymes carried by bacteria and leukocytes. Despite considerable evidence suggesting that wound healing is generally delayed in older patients, the effects of age-related factors on the proteolytic response have not been clearly understood. The present study therefore examined the fragility of mammary skin tissues exposed to proteolytic enzymes using ultrasound microscopy.
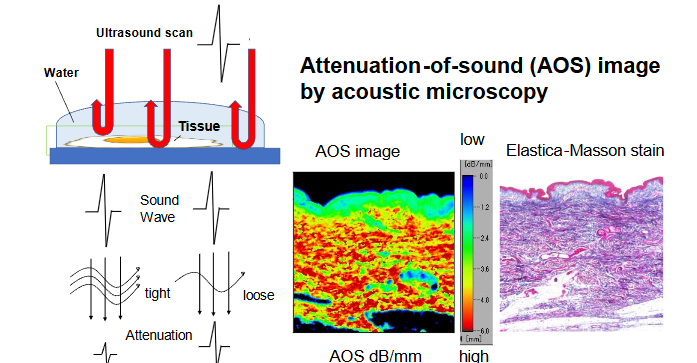
Studies have shown that the attenuation of ultrasonic waves is correlated with viscosity, with higher viscosity levels being associated with greater attenuation. Denser fibers have greater attenuation of energy passing through them, which allows for the inference of fiber density. Given that proteolysis has been considered to decrease fiber density, we hypothesized that sound attenuation values could indicate the degree of fiber fragmentation.
To mimic actual bacterial infection to the skin, tissue sections from young and elderly individuals were digested using three different proteolytic enzymes, namely collagenase types 2 and 3 and actinase E. We then examined the attenuation values over time after protease digestion to clarify whether aging-related alterations affect the ease with which bacteria can invade the skin. This study will help understand elderly people’s susceptibility to skin infections and contribute to the development of infection-control measures.
MATERIALS AND METHODS
HUMAN SPECIMEN PREPARATION
This study used stored paraffin blocks of breast skin that had no link to the patient’s identity. We selected cases who had recently undergone mastectomy due to breast carcinoma, subsequently utilizing the intact skin away from the cancers. The study protocol conformed to the ethical guidelines of the Declaration of Helsinki and was approved by the ethics committee of the Hamamatsu University School of Medicine (approval no. 19-180). Written informed consent was obtained from all subjects. All procedures were conducted in accordance with the guidelines and regulations of the ethics committee. All tissue samples for pathological diagnosis were fixed in a 10% buffered formalin solution, embedded in paraffin, and cut into flat sections. Thereafter, 10-μm-thick sections were prepared for scanning acoustic microscopy (SAM), whereas 4-μm-thick sections were prepared for light microscopy (LM). Breast skin from 12 cases were used, including 6 young (33- to 46-year-old) and 6 elderly (74- to 88-year-old) patients.
PROTEASES
Three endopeptidases, including actinase E (also called pronase, source: Streptomyces griseus, Funakoshi, Tokyo, Japan), collagenase types 2 and 3 (source: Clostridium histolyticum, Worthington, Lakewood, NJ) were used to degrade the skin. All proteases were dissolved in 1 mg/mL in phosphate-buffered saline containing 0.5 mM CaCl2. The enzyme solution was mounted on the section and incubated at 37°C for 1 and 2 h for actinase E and 2 and 4 h for the collagenases. The sections were then washed in distilled water at each time point and observed under an acoustic microscope. After observation, the same section was reincubated in the enzyme solution.
SCANNING ACOUSTIC MICROSCOPE OBSERVATION
The sections were examined using a SAM system (AMS-50AI; Honda Electronics, Toyohashi, Aichi, Japan) with a central frequency of 80 MHz and a lateral resolution of 18 μm. The transducer was excited with a 2-ns electrical pulse to emit an acoustic pulse. Thereafter, the section was placed on the stage, and distilled water was used as coupling fluid between the transducer and the section. The transducer was used for transmitting and receiving the wave signal. Waveforms reflected from the surface and the bottom of the sample were compared to measure the attenuation of sound (AOS) at each point. The waveform from a glass surface without the specimen was considered the zero AOS area (black) and was used as a reference. The section was scanned along the X–Y axis within 2.4 mm × 2.4 mm and 4.8 mm × 4.8 mm square areas. A single scan required a few minutes. After the scan, the AOS value at each point was plotted on the screen according to color code to create an AOS image.
LIGHT MICROSCOPIC OBSERVATION
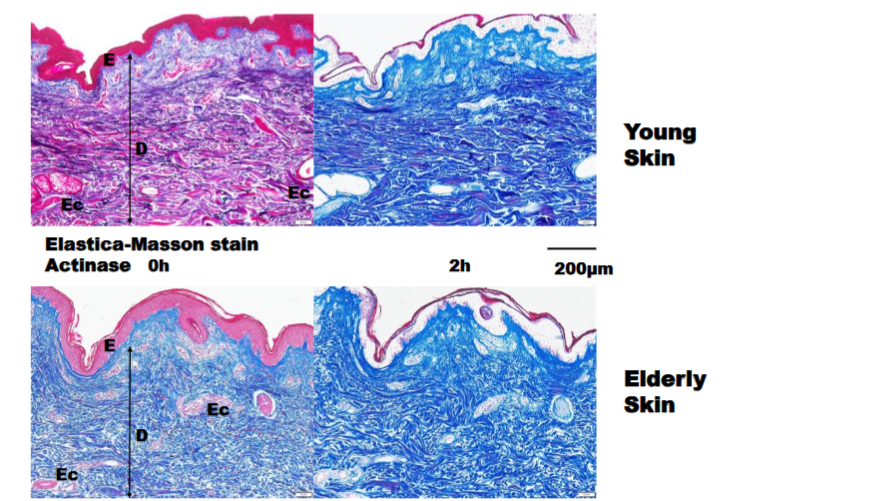
Before and after protease digestion, the slides near the SAM sections underwent Elastica–Masson staining and were compared with the corresponding AOS images. During Elastica–Masson staining, collagen fibers are stained blue, elastic fibers are stained black, and the cytoplasm is stained red.
STATISTICAL ANALYSES
The means and standard deviations of the AOS values were calculated from at least five regions of interest per slide, which were determined using the LM image. Mean AOS values at different time points following protease digestion were compared using Student’s t-test or Welch’s t-test. A commercial statistics software (BellCurve for Excel; Social Survey Research Information, Tokyo, Japan) was used to calculate the mean area-of-interest values and perform the t-tests. Before statistical analyses, all data sets with normal distribution were compared to determine the difference between mean values. A p value of <0.05 indicated statistical significance.
RESULTS
RELATIONSHIP BETWEEN DERMAL AOS VALUES AND THICKNESS
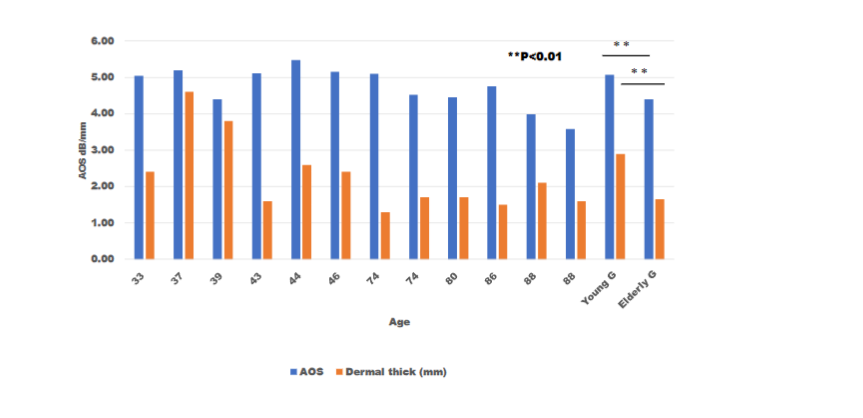
Fig. 2 shows the relationship between dermal AOS values and thickness in young and elderly patients. Notably, young skin had higher AOS values and greater dermal thickness than did elderly skin. Significant differences in both AOS values and thickness were observed between young and elderly groups (p < 0.05).
COLLAGENASE DIGESTION OF YOUNG AND ELDERLY BREAST SKIN
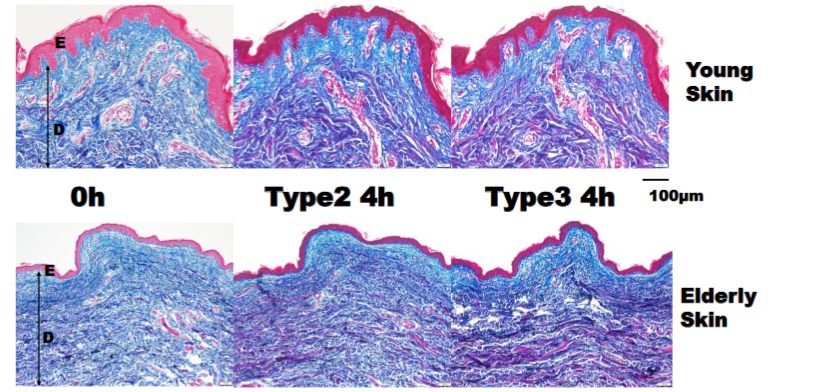
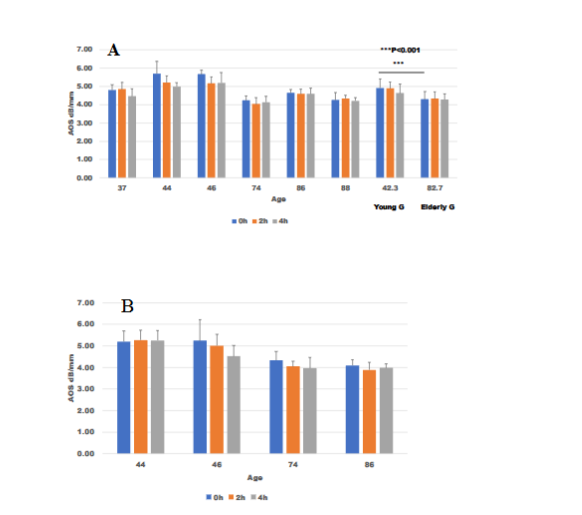
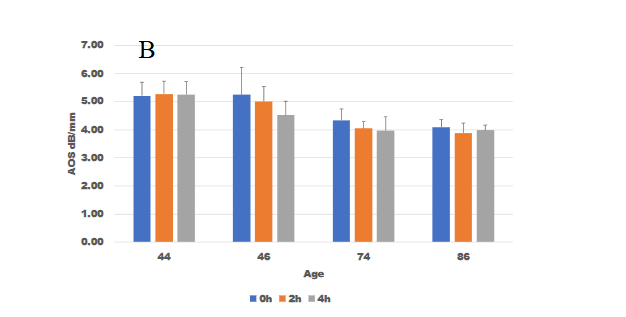
After digestion with two types of collagenases, AOS images of young and elderly showed no conspicuous changes in the dermis and epidermis. LM images of Elastica–Masson staining also showed no remarkable changes after collagenase digestion. A comparison between young and elderly groups showed higher AOS values in the former than in the latter. No significant reduction in AOS values were noted in all cases.
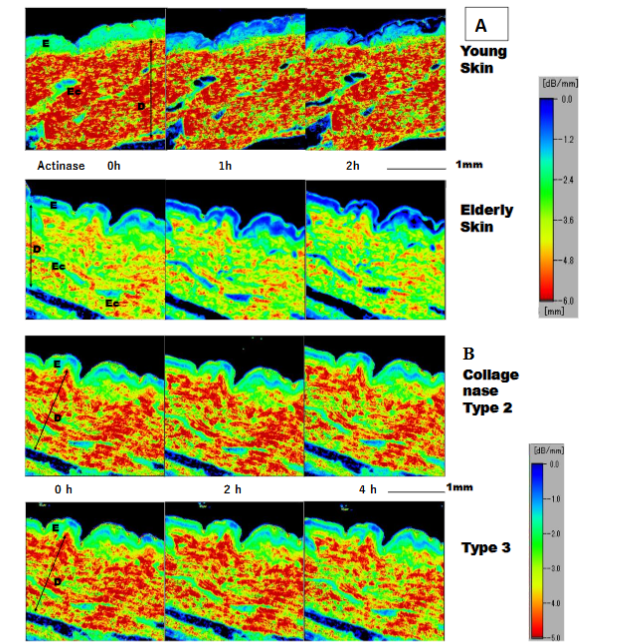
ACTINASE E DIGESTION OF YOUNG AND ELDERLY SKIN
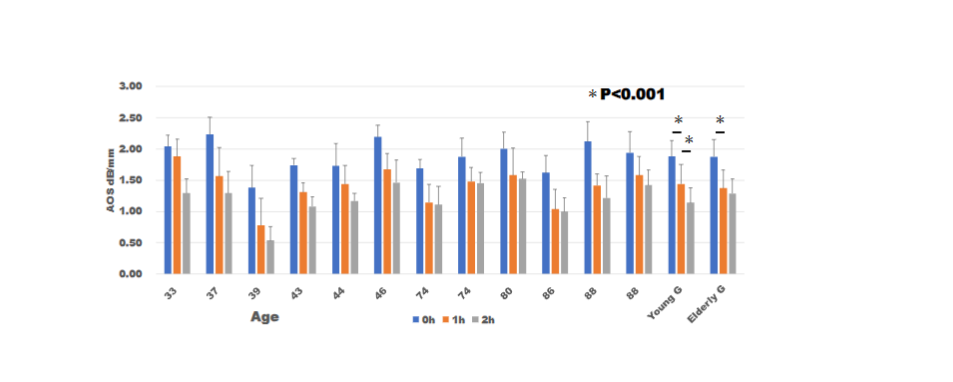
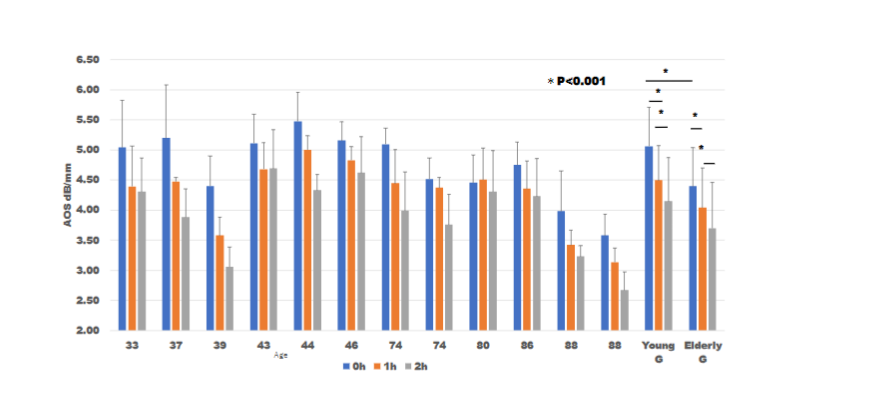
Given no significant AOS reduction following digestion with the two types of collagenases, we sought to determine whether digestion with actinase E, which has a broader peptidase activity than collagenases, would produce different results. Compared to collagenase, actinase E promoted an obvious reduction in AOS values.
ALTERATIONS AFTER ACTINASE E DIGESTION ON LIGHT MICROSCOPY
Epidermal cells, except for the surface keratin layer, became transparent after digestion. Dermal elastic fibers stained on Elastica–Masson trichrome staining disappeared after digestion, whereas the red-colored fibers changed to blue. No remarkable changes in the thinness and thickness of collagen fibers were observed. The cytoplasm and nuclei of the cells that appeared red became transparent or faint after digestion.
DISCUSSION
The two collagenases were barely able to digest collagen fibers in the dermis, which showed resistance. Similarly, the epidermis showed only a slight decrease in AOS value after digestion with the collagenases. Dermal collagen fibrils are stabilized by cross-links that are highly resistant to proteolytic cleavage. Previous studies utilized the two collagenases and verified their activity by digesting other sections.
The epidermis, except for surface keratin, was almost digested by the more proteolytic actinase E. Keratin, which is composed of filament-forming proteins is insoluble in water and serves various functions, such as protection and defense. A decrease in dermal AOS values was observed with time due to digestion. The elderly group had a thinner dermal collagen layer than did the young group, which can be interpreted as mechanical weakening due to fiber degradation.
These results suggest that the epidermis and dermis are less susceptible to degradation by the two types of collagenases. However, both can be degraded by proteolytic reactions against bacteria, which involve multiple proteases. Elderly skin has lesser density and shorter dermis than young skin, which suggests that elderly individuals are more vulnerable to proteolysis.
Our previous study on facial skin aging revealed that dermis speed-of-sound was lower in the elderly than in the young, reflecting a decrease in collagen fiber density in the former. Moreover, our previous study showed that pepsin digestion promoted a decrease in dermal speed-of-sound values over time, similar to the present results.
Although Elastica–Masson trichrome staining can confirm the degree of proteolysis, this approach requires the preparation of a large number of sections from the beginning and struggles to maintain uniform results owing to the inevitable unevenness of the staining procedure. Digital imaging with AOS allows the evaluation of unstained sections over time while having the advantage of visualizing the digestion process. This approach can also easily compare AOS values from one site to another while also allowing for the numerical comparison of the degree of digestion.
Several limitations of this study should be acknowledged. First, the sections were not fresh but all formalin-fixed paraffin-embedded (FFPE). This is because making flat-surfaced 10-μm sections and maintaining structure during protease digestion were challenging with fresh frozen tissues. Conversely, creating 10-μm flat sections that were sustainable in the enzyme solution was much easier with FFPE sections. Moreover, maintaining the structure and antigenicity of FFPE sections is much easier, as indicated by immunostaining methods.
Second, the sample size was quite small, limiting the generalizability of our results. We randomly selected young and elderly patients who had recently undergone surgery. Nonetheless, given that the selected cases had general histological characteristics of aging, they were suitable for comparison with representative samples. Conspicuous differences in the depth and density of the dermal collagen layer were observed. Moreover, statistical analysis was possible with the number of samples included.
Third, the proteases used herein were all sourced from particular bacteria. As such, the proteolytic results must differ with each type of enzyme. In the case of infection, multiple types of proteases, including bacteria, leukocytes, and sera, must function in the lesion. Actinase E was suitable for reflecting real infections due to strong proteolytic activity, with degradation rates reaching 75% to 90%. It cleaves peptide bonds almost indiscriminately.
This study revealed the structure and functional alteration against bacterial infection. AOS values can monitor the degree of protease digestion, whereas LM staining complicates it. This method can apply to any organ and is probably available to glycans using breakdown enzymes.
CONCLUSION
The current study evaluated the protein degradation of breast skin digested using two types of collagenases and actinase E based on AOS values correlated with protein distribution and density. The skin sections of both young and elderly showed resistance to digestion using the two collagenases. However, actinase E was able to break down the epidermis and dermis over time after incubation. The epidermis was lost beside the keratin layer, and dermal collagen and elastic fibers were broken, which resulted in reduced AOS values. Although actinase affected both young and elderly skin, the latter exhibited more severe damages given its initially lower dermal thickness and density caused by aging. Measuring AOS values is a superior approach for visualizing the protease digestion process over time and statistically comparing the damage from protein breakdown.
Conflict of Interest
KM received supporting fees from Honda Electronics for attending meetings. TI has no conflicts of interest to declare.
Funding Statement
No funding was received.
Acknowledgments
The authors acknowledged Drs. Kanna Yamashita, Michio Fujie, and Toshi Nagata of the Department of Health Science, Hamamatsu University School of Medicine provided the research facilities for this study. Miss Mitsue Kawashima and Mr. Yuki Kurita at the Department of Regenerative & Infectious Pathology, Hamamatsu University School of Medicine, helped with the sample staining.
References
- Khalid KA, Nawi AFM, Zulkifli N, Barkat MA, Hadi H. Aging and Wound Healing of the Skin: A Review of Clinical and Pathophysiological Hallmarks. Life. 2022;12(12). doi:10.3390/life12122142
- Khavkin J, Ellis DAF. Aging Skin: Histology, Physiology, and Pathology. Facial Plast Surg Clin North Am. 2011;19(2):229-234. doi:10.1016/j.fsc.2011.04.003
- He T, Fisher GJ, Kim AJ, Quan T. Age-related changes in dermal collagen physical properties in human skin. PLoS One. 2023;18(12 December). doi:10.1371/journal.pone.0292791
- Kerns M, Chien A, Kang S. Skin aging. In: Kang S, Amagai M, Bruckner A, et al., eds. Fitzpatrick’s Dermatology. Vol 1. 9th ed. Mc Graw Hill; 2019:1779-1791.
- Lertzman BH, Gaspari AA. Drug Treatment of Skin and Soft Tissue Infections in Elderly Long-Term Care Residents. Vol 9.; 1996.
- Stevens DL, Bisno AL, Chambers HF, et al. Practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update by the infectious diseases society of America. Clinical Infectious Diseases. 2014;59(2). doi:10.1093/cid/ciu296
- Saijo Y. Recent Applications of Acoustic Microscopy for Quantitative Measurement of Acoustic Properties of Soft Tissues. In: Mamou J, Oelze M, eds. Quantitative Ultrasound in Soft Tissues. Springer; 2013:291–313. doi:10.1007/978-94-007-6952-6_12
- Miura K, Iwashita T. Observations of amyloid breakdown by proteases over time using scanning acoustic microscopy. Sci Rep. 2023;13(1):20642. doi:10.1038/s41598-023-48033-4
- Miura K, Yamamoto S. Histological imaging from speed-of-sound through tissues by scanning acoustic microscopy (SAM). Protoc Exch. Published online 2013. doi:10.1038/protex.2013.040
- Tamura K, Ito K, Yoshida S, Mamou J, Miura K, Yamamoto S. Alteration of speed-of-sound by fixatives and tissue processing methods in scanning acoustic microscopy. Front Phys. 2023;11. doi:10.3389/fphy.2023.1060296
- Hozumi N, Yamashita R, Lee CK, et al. Time-frequency analysis for pulse driven ultrasonic microscopy for biological tissue characterization. In: Ultrasonics. Vol 42.;2004:717-722. doi:10.1016/j.ultras.2003.11.005
- Sachs D, Fisher G, Voorhees J. Skin aging. In: Griffiths C, Barker J, Bleiker T, Chalmers R, Creamer D, eds. Rook’s Textbook of Dermatology. Vol 4. 9th ed. Wiley Blackwell; 2016:155.1-155.9.
- Quan T, Fisher GJ. Role of age-associated alterations of the dermal extracellular matrix microenvironment in human skin aging: A mini-review. Gerontology. 2015;61(5):427-434. doi:10.1159/000371708
- Miura K, Yamashita K. Mechanical weakness of thoracic aorta related to aging or dissection predicted by speed of sound with collagenase. Ultrasound Med Biol. 2019;45(12):3102-3115. doi:10.1016/j.ultrasmedbio.2019.08.012
- Wang B, Yang W, McKittrick J, Meyers MA. Keratin: Structure, mechanical properties, occurrence in biological organisms, and efforts at bioinspiration. Prog Mater Sci. 2016;76:229-318. doi:10.1016/j.pmatsci.2015.06.001
- Miura K, Yamashita K. Evaluation of aging, diabetes mellitus, and skin wounds by scanning acoustic microscopy with protease digestion. Pathobiology of Aging & Age-related Diseases. Published online 2018. doi:10.1080/20010001.2018.1516072
- Bond JS. Proteases: History, discovery, and roles in health and disease. Journal of Biological Chemistry. 2019;294(5):1643-1651. doi:10.1074/jbc.TM118.004156
- Mainz ER, Dobes NC, Allbritton NL. Pronase E-Based Generation of Fluorescent Peptide Fragments: Tracking Intracellular Peptide Fate in Single Cells. Anal Chem. 2015;87(15):7987-7995. doi:10.1021/acs.analchem.5b01929