






Capgras Delusion in Postpartum Psychosis: A Case Study
A case of a patient with a Capgras delusion during the postpartum period
Dr. Elizabeth Nickram-Validum1, Dr. Bhiro Persaud Harry1
- Psychiatrist, GPHC.
OPEN ACCESS
PUBLISHED: 31 October 2024
CITATION: Nickram-Validum, E., Harry, BP., 2024. A case of a patient with a Capgras delusion during the postpartum period. Medical Research Archives, [online] 12(10). https://doi.org/10.18103/mra.v12i10.5748
COPYRIGHT © 2024 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v12i10.5748
ISSN 2375-1924
ABSTRACT
Objective: To describe the case of a patient with a Capgras delusion within the postpartum period and to highlight its link with violence.
Method: The case under consideration in this article serves as an illustrative example of a patient experiencing a psychotic disorder characterized by a Capgras delusion during the postpartum period. The patient is under the conviction that a familiar individual has been supplanted by an indistinguishable impostor. In this instance it is noted that the patient harbors suspicions regarding the malevolent intentions of this impostor, which finally precipitate violent behavior.
Result: This case underscores the importance of comprehensive screening for patients with psychosis, particularly in relation to Capgras delusion and its potential association with malevolent intentions.
Conclusion: The paramount consideration in instances of psychosis within the postpartum period is the safeguarding of the infant’s welfare. It is advised that a meticulous assessment of the patient’s psychotic manifestations be conducted, given that the potential for violent conduct may encompass familial members at large.
Introduction
Capgras syndrome (CS)/Capgras delusion, first described by Joseph Capgras and Reboul-Lachaux in 1923, is a rare delusional misidentification syndrome where patients misidentify familiar figures and perceive them as substitutes, impostors, or doubles of the actual person. It is often associated with other psychoses, particularly paranoid ones. Despite recognizing the person, the individual with CS denies their true identity and often relies on subtle perceived differences in behaviour, personality, or physical appearance to distinguish between the real person and the imagined impersonator¹².
The original account of Capgras syndrome describes madame M’s unsettling experience with a proliferation of doubles. After the loss of two daughters and twin boys, she firmly believed her surviving daughter had been abducted and replaced with an impostor. Over the years, she claimed more than 2,000 versions of her daughter, each perceived as a duplicate. She also suspected her husband had been murdered and replaced. The police force and hospital doctors multiplied, complicating her pursuit of justice. Various explanatory models exist, but Joseph Capgras himself initially proposed a concept similar to contemporary cognitive neuropsychiatric theories: certain faces, despite their unaltered features, no longer evoke the feeling of exclusive familiarity that accompanies direct perception and immediate recognition³.
Capgras syndrome, while descriptive, lacks a precise definition of a mental disorder. Researchers have investigated multiple potential factors contributing to its development. Approaches to understanding Capgras syndrome have examined both functional and organic aspects. There have been cases where the patients have an organic cause for their delusion and cases where there is no organic cause.
Initially, psychodynamic interpretations suggested that it might stem from oedipal issues in women or latent homosexuality in men. Later hypotheses proposed anxiety-induced cognitive regression, pathological splitting of internalized object representations, and projection of conflicting emotions onto the affected individual.
The Capgras delusion associated with medical and neurological conditions, suggests underlying cerebral dysfunction. Dopaminergic overactivity and serotonin abnormalities have been implicated in some studies. Structural and neuroimaging studies support an organic aetiology, with common lesions in the right hemisphere and bilateral damage in most patients. Pathology is widespread, but lesions are mainly found in the frontal, temporal, and parietal lobes.
In studies utilizing CT scans, researchers have observed more pronounced bilateral atrophy in the frontal and temporal cortices of schizophrenia patients with Capgras syndrome compared to those without the syndrome. Other investigations using MRI have identified more pronounced right hemisphere lesions in patients with dementia and CS⁴.
Capgras’s hypothesis posits that the delusion of doubles arises due to inadequate integration of left and right hemispheric processing of familiar faces⁵. However, this model is challenged by tachistoscope study results, which indicate that CS patients perceive visual stimuli presented unilaterally faster than those presented bilaterally⁶. Other explanations focus on specific impairments in face memory and recognition processes.
In a study by Staton and colleagues⁷, they described a case of post-traumatic Capgras delusion in a 23-year-old male. This patient experienced duplications in all three spheres of orientation: time, place, and person. The authors hypothesized that these duplications arise from a disconnection between new memory registration and memory stores. Based on neuropsychological testing and computerized axial tomographic scanning, they suggest that a deep lesion at the right posterior hippocampus and temporo-parieto-occipital junction is the likely site of this primary memory disconnection.
Psychiatrist Michael Cutting proposed that CS arises as a consequence of right hemispheric damage, leading to an inability to access memories associated with individual faces. Although one tachistoscopic study supports this theory, it has been observed that Cutting’s model does not fully account for the specific selectivity seen in CS delusions of misidentification. CS exhibits similarities with prosopagnosia, a neurological condition associated with right hemisphere damage. Prosopagnosia is characterized by impaired recognition of familiar faces due to lesions in the right ventromedial occipitotemporal areas. It is hypothesized that CS may arise from disruptions in pathways connecting face-processing regions within the inferior temporal cortex and limbic structures. These pathways play a role in generating affective responses during face recognition. Support for this model is derived from PET studies conducted on patients with CS and Alzheimer’s disease. These studies reveal bilateral cortical abnormalities, including damage to the left limbic system and paralimbic, and association areas. Additionally, neuroimaging and autopsy studies in CS patients with dementia with Lewy bodies demonstrate multiple lesions in visual and occipital association cortices, as well as frontal and parietal white matter. These findings suggest disrupted connections from face-processing areas in the temporal lobe to the limbic system. Interestingly, reports of CS in blind patients suggest that misinterpretation of senses beyond vision may contribute to this phenomenon⁴.
While CS has been studied from various angles, including phenomenological, psychodynamic, and biological perspectives, forensic attention to the dangerousness of Capgras patients has been limited. There have been a few reports emphasising the risk of violence in persons with a Capgras delusion⁸. According to a systematic review, 6% of individuals experiencing Capgras delusions exhibit violent behaviour, suggesting that the syndrome may pose greater risks than initially believed⁹.
In the study by Doe and Smith (2003)¹⁰, the authors explored the phenomenon of a Capgras delusion and presented two intriguing case reports where the patients presented with violence. The initial incident involved a woman who fatally harmed another patient due to her suspicion that the other patient was planning to harm her daughter’s doppelgänger. In a separate instance, a patient experiencing a Capgras delusion held the belief that his father was a robot and proceeded to decapitate him, searching for batteries and microfilm within his father’s head.
Silva et al.¹¹, also highlighted a few cases of violence in patients with Capgras delusions. The most violent account was of a male with schizophrenia who believed that multiple family members had been cloned and taken over by spirits. Tasked by God to destroy the wicked spirits living in the bodies of his family, he shot and killed his father and seriously wounded his nephew. The other members of his family were spared as he could not find them.Our paper presents a recent case where the incidents of violence equaled or exceeded that of previous instances.
Case Report
Ms. S, a female in her early 20’s, presented to our clinic in 2022. At the time, she was in a common-law relationship and recently underwent a lower segment caesarean section for her first child. Since giving birth, she has experienced distressing auditory hallucinations urging her to harm her baby. Notably, during her hospital stay, she was on the verge of attempting to harm her child by jumping out of a third-floor window, but was interrupted by a nurse.
DEVELOPMENTAL AND SCHOOL HISTORY: Ms. S had an uneventful birth and normal development. Her parents separated after her birth, and she split her time between her mother and stepfather’s home and her paternal grandmother’s residence. Academically successful, she was described as a reserved individual who avoided social activities. Although not prone to quarrels, she occasionally exhibited impulsivity. Prior to childbirth, she worked as a teacher for two years.
PAST PERSONAL AND FAMILY PSYCHIATRIC HISTORY: Five years prior to her current visit, Ms. S underwent an abortion at 8 weeks gestation. In the subsequent eight months, she experienced sadness, frequent crying, intense guilt, restlessness, and suicidal thoughts (without any suicide attempts). Notably, she denied any psychotic symptoms during this period. Additionally, there is a family history of psychotic illnesses on her father’s side, involving two cousins and an aunt.
PAST MEDICAL HISTORY: Ms. S has no significant medical illnesses. Her surgical history includes only one procedure—an elective lower segment caesarean section (LSCS). She has not received any transfusions and has no known allergies. Furthermore, there is no recent history of substance use.
HISTORY OF PRESENT ILLNESS: Ms. S came to our attention when the police found her walking in the rain early one morning, carrying a naked baby. She had blood on her hands and body, which did not belong to her. Upon questioning, she was uncooperative in sharing information, leading to her admission to our inpatient ward.
Upon initial assessment, Ms. S presented as a young female of mixed ethnicity. Her stature was short, with corresponding short arms and legs. She exhibited overweight tendencies, with weight distribution primarily above her hips. No overt physical abnormalities were observed. Her skin tone appeared light, and her short, curly hair was unkempt. She wore no makeup, and her hair was disorganised and secured with an elastic band. Her attire consisted of an oversized, inside-out checked shirt, ankle-length pink tights, and no shoes. Notably, she was restrained with handcuffs on her hands and shackles on her feet, yet her gait remained as normal as possible under the circumstances. Despite her stated age, she appeared older, and her short nails harboured embedded dirt. Additionally, she had a cuticle injury on the second finger of her left hand and a small, superficial cut on the palmar aspect of her right hand near the base of her middle finger (approximately 2 cm in length). Superficial healing cuts were also evident on her right hand. Notably, there were no visible tattoos or scarring indicative of a history of suicide attempts.
During the interview, Ms. S sat slouched in the chair, occasionally leaning back. Initially cooperative, she maintained good eye contact and demonstrated alertness. However, rapport with the examiner was not established. As time elapsed, she became increasingly agitated due to her desire to lie down. Moments of anxiety were apparent and notably, there were no hallucinatory behaviours.
Ms. S’s speech was limited, quiet, and primarily responsive to prompting questions. Her affect displayed a full range but was occasionally inappropriate, intensifying and becoming labile. While her thought process could not be fully assessed, it appeared linear. She exhibited persecutory delusions and perceptual disturbances. She lacked insight and had poor judgment.
ADMISSION TO THE WARD: For the initial three weeks, we observed closely Ms. S’s behaviour without implementing biological treatment. Her demeanour oscillated between pleasant cooperation and hostile outbursts, during which she expressed memory difficulties. When in a positive state, she attributed her unease to postpartum experiences, saying “I feel nervy”. At all times she maintained that everything was well with her grandmother.
Psychological assessments, including the Machover Draw-A-Person Test, the Trait Personality Inventory, and the Thematic Apperception Test, were conducted during this period. The patient exhibited tendencies toward impulsivity and introversion, but no elements suggestive of probable psychotic functioning were identified. Medical and neuroimaging tests returned unremarkable.
With information from Ms. S’s mother, we initiated trifluoperazine at a dose of 1mg twice daily for approximately three weeks after admission. Almost three months postpartum, Ms. S began communicating more openly, sharing details about her illness.
The following is her account of the activities that transpired postpartum.
“Ms. S, previously in good health, began experiencing heightened anxiety following the birth of her baby. She referred to this as feeling “nervy”. During the initial days post-discharge from the hospital, she resided with her mother and stepfather. Approximately six days before her grandmother’s tragic demise, Ms. S requested that her mother cut her hair, explaining that it contributed to her distress, saying “It’s making me mad. There is something in my head making me mad”. She also reported auditory hallucinations—voices of unseen individuals—and a pervasive sense of malevolent forces targeting her. These forces were associated with the presence of ‘jumbies’ in her home. Initially, the malevolent entity assumed the appearance of Ms. S’s common-law husband, although it was a deceptive likeness. Consequently, she dissolved the union—the common-law marriage and sent him away from her mother’s house. Subsequently, the entity appeared as her stepfather, mimicking his form and resemblance. Ms. S mentioned this concern to her stepfather, saying “Mom is not mom. Something evil has replaced mom”. Concerned for her well-being, Ms. S’s mother and stepfather took her to church, even though they suspected nerve-related issues.
Despite this intervention, Ms. S continued to perceive the malevolence associated with her mother. Seeking refuge, she sought solace at her grandmother’s home at twilight that same day. During their conversation, grandmother advised her to seek medical attention for her ‘nerves.’ Notably, S’s grandmother typically covered chairs with sheets at nights. That evening, Ms. S placed her baby on a chair and sprinkled salt—an act that her grandmother disapproved of, citing the saying ‘Salt nah good fuh we mash’. This fuelled Ms. S’s suspicion of her grandmother’s intentions. She had the thought that the only reason why grandmother would not want to walk on or touch the salt was because she was evil. They went to bed together shortly after.
Late that night, Ms. S awoke to find her grandmother facing her. The malevolent spirit, now in bed with them, not only assumed human form but also distorted the grandmother’s features—dark, eyeless, and resembling a man. Fearing for her safety, Ms. S feigned stomach pain and left the room. In the living room, she discovered the folded sheet from the chair that she threw the salt on, confirming her suspicions. She went back into her grandmother’s bedroom, collected the sleeping baby and went to the kitchen. Grandmother was now awake. In the kitchen, Ms. S continued her ritual with salt on the baby, believing it would counteract the evil. Her grandmother, now resembling a man, followed her; S became frightened and a desperate struggle ensued, resulting in the grandmother lying on the floor, bloodied.
Ms. S’s memory fails her regarding her grandmother’s throat-cutting incident, but she vividly recalls cutting off her grandmother’s hair and applying salt. Despite her demise, the grandmother’s entity reappeared to Ms. S the next day, attempting to deceive her. Ms. S went to the police station where the officers noticed a cut she sustained on her hand beginning to heal. Fearing the malevolence might revive, Ms. S left the house with her baby. Tearfully recounting this traumatic history, she expressed remorse, believing she defended herself against an evil spirit rather than her own grandmother.”
On the day when Ms. S recounted the events related to her grandmother, which was almost three months postpartum, her appearance was well-maintained. She wore a multi-coloured, floral knee-length dress without sleeves, paired with slippers. Her clean, shoulder-length, black, curly hair was partially pulled up in a casual bun. Notably, she exhibited good oral hygiene and general cleanliness, emitting a pleasant body odour. Ms. S refrained from wearing makeup, jewellery, or other adornments. Physically, she displayed no abnormalities or distinguishing marks, and the wounds mentioned in the initial mental status examination had healed.
Throughout the interview, Ms. S remained composed, maintaining an upright posture. She actively engaged with the interviewer, responding appropriately to questions while maintaining good eye contact and attentiveness. Rapport was established, and no abnormal movements or sounds were observed. Her psychomotor activity appeared normal. Her speech was clear, well-articulated, and delivered at a typical rate, with appropriate tone and volume. Regarding her emotional state, Ms. S described her mood as “okay.” Her affect was euthymic, displaying normal intensity, a full range of emotions, and appropriate mobility and reactivity. Her thought process followed a linear and organized pattern, demonstrating goal-directed thinking. Importantly, she currently reported no delusions, suicidal thoughts, or homicidal ideations. Denying any perceptual disturbances, she provided an honest account of the events at her grandmother’s house during the interview. Ms. S exhibited good orientation, concentration, calculation abilities, fund of knowledge, abstract reasoning, and visuospatial skills. Her memory remained intact, and she demonstrated sound insight and judgment.”
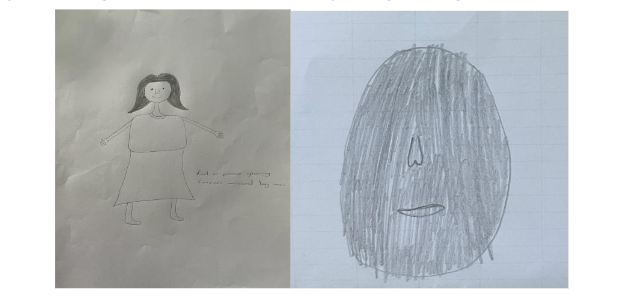
She drew the following to illustrate the changes that occurred with her grandmother.
Below are drawings by S of her grandmother. The image on the left illustrates when grandmother was normal, the image on the right illustrates when the entity changed her grandmother’s face.
Discussion
The postpartum period is a challenging time marked by significant biological, physical, social, and emotional changes. It necessitates considerable personal and interpersonal adjustments, particularly for first-time mothers¹². In the days and weeks following childbirth, many women experience mental disturbances such as mood swings and mild depression. However, some may also develop conditions like PTSD, major depression, or even severe psychosis. Postpartum psychosis is the most extreme form of mental illness in this category¹³. Postpartum psychiatric disorders are traditionally divided into maternity blues, puerperal psychosis, and postnatal depression.
‘Maternity blues,’ also referred to as ‘baby blues’ or ‘postpartum blues,’ is a period of emotional instability following childbirth, characterized by frequent crying, irritability, confusion, and anxiety. This condition is particularly prevalent among women who lack strong, healthy social support. Symptoms typically appear within the first 10 days and peak around days 3 to 5. Generally, these symptoms do not interfere with women’s social and occupational functioning. Maternity blues is self-limiting and usually requires no active intervention other than social support and reassurance from family members.
Postpartum depression is often difficult to distinguish from depression occurring at other times in a woman’s life. One helpful feature is that in postpartum depression, negative thoughts are primarily focused on the newborn. This condition is less common than postpartum blues¹². Postpartum psychosis typically has a sudden and acute onset, usually occurring within the first two weeks after delivery, and at most, within three months postpartum. Women with a history of bipolar disorder are at a higher risk of developing postpartum psychosis. Additionally, mothers who have experienced postpartum psychosis have a 50 to 80% chance of another psychiatric episode, often within the bipolar spectrum. Postpartum psychosis may also be the initial manifestation of bipolar disorder¹⁴.
In a study of parous women with bipolar disorder, sleep loss that precipitated manic episodes was identified as a key marker for assessing the risk of developing postpartum psychosis. The findings indicated that women who experienced sleep deprivation leading to manic episodes were twice as likely to have had an episode of postpartum psychosis at some point in their lives¹⁵.
Postpartum psychosis often presents uniquely compared to other psychotic disorders. Symptoms can include delusions, hallucinations, manic and depressive episodes, and cognitive impairments. These symptoms tend to emerge rapidly and often focus on the infant. Dysphoric mania and cognitive symptoms may resemble delirium. These symptoms typically emerge suddenly within the first few weeks postpartum and often constitute a psychiatric emergency. Women with postpartum psychosis may also exhibit prodromal symptoms that can be mistaken for medical conditions, such as irritability, mood swings, confusion, disorientation, and insomnia¹⁴. In addition to postpartum psychiatric disorders, other psychiatric conditions can also manifest during the postpartum or peripartum period. This is particularly true for major mood episodes and psychotic disorders. Postpartum psychosis poses significant risks to both the mother and the infant. Similarly, psychotic disorders carry the potential for harm, with the extent of risk to individuals in proximity being contingent upon the nature and themes of the psychotic symptoms. Numerous facets of psychosis contribute to its inherent peril. Among these, the Capgras delusion stands out as one of the symptoms that can precipitate hazardous outcomes. Notably, persecutory delusions and commanding hallucinations also feature prominently on this list.
One must exercise caution to avoid labelling prematurely any psychosis occurring during the postpartum period as postpartum psychosis. When this misclassification occurs, clinical focus narrows primarily to concerns of suicide and infanticide. It becomes imperative that patients within this postpartum window receive specialized intervention for managing the psychiatric conditions that arise during this critical phase. Different diagnostic entities carry distinct risks, underscoring the necessity of meticulous symptom analysis to arrive at an accurate diagnosis. Such precision enables healthcare providers to effectively identify all individuals at risk due to the patient’s psychotic symptoms. Ms. S received a diagnosis of schizophrenia spectrum disorder, with a prominent Capgras delusion as the primary feature of her psychotic illness. Initially, many family members attributed her symptoms to postpartum depression. Unfortunately, this delay hindered her access to medical care, which might have allowed early detection of the delusion and potentially prevented harm to Ms. S’s grandmother.
During the postpartum period, women face various risks, including postpartum blues, postpartum depression, postpartum psychosis, and psychosis with onset within the postpartum timeframe. These distinct conditions require different management approaches. Yonkers et al.¹⁶ propose that postpartum psychosis represents an overt manifestation of bipolar disorder following delivery. Brockington¹⁷ described the classic presentation of postpartum psychosis in mothers, while Wisner et al. focused on the clinical features of psychosis during the postpartum period. Brockington (1996)¹⁷ delineated the classic presentation of postpartum psychosis in mothers. This presentation includes features such as an odd affect, withdrawal, distraction due to auditory hallucinations, incompetence, confusion, catatonia, or, alternatively, elation, labile mood, rambling speech, and excessive agitation. The woman’s unusual beliefs often centre around childbirth themes, altered infant identity, or feelings of persecution related to the baby or a perceived changeling.
Wisner et al. (2000)¹⁸ reported that women experiencing psychosis related to childbearing frequently exhibit cognitive disorganization and atypical psychotic symptoms. These symptoms often include mood-incongruent delusions of reference, persecution, jealousy, and grandiosity. Additionally, visual, tactile, or olfactory hallucinations may suggest an organic aetiology. The mean age of onset for postpartum psychosis is 26.3 years, a period when most women are having their first or second child. Compared to women with chronic mental illness, patients with postpartum psychosis typically achieve higher functional levels before the onset of illness. Notably, homicidal behaviour is rare in postpartum psychosis. Among women hospitalized for this condition, approximately 28%–35% describe delusions related to their infants, but only 9% report thoughts of harming the infant. The cognitive disorganization associated with postpartum psychosis may lead to neglect of the infant’s needs and unsafe caregiving practices. The symptoms associated with psychosis with onset during the postpartum period may lead to harm of the family and persons nearby at a large.
Conclusion
The clinical presentation of Ms. S provides compelling evidence that enriches the existing psychiatric literature. She was diagnosed with a schizophreniform disorder with onset during the post-partum period. Notably she experienced a Capgras delusion as part of her illness. Specifically, her experience underscores the perilous association between a Capgras delusion and violent tendencies.
Conflict of Interest:
None.
Funding Statement:
None.
Acknowledgements:
None.
References
2. Todd J, Dewhurst K, Wallis G. The syndrome of Capgras. Br J Psychiatry. 1981;139:319-327.
3. Alexander MP, Stuss DT, Benson DF. Capgras syndrome: A re-duplicative phenomenon. Neurology. 1979;29:334-339.
4. Bourget D, Whitehurst L. Capgras Syndrome: A Review of the Neurophysiological Correlates and Presenting Clinical Features in Cases Involving Physical Violence. Can J Psychiatry. 2004;49:719-725. Available from: https://journals.sagepub.com/doi/pdf/10.1177/070674370404901102
5. Joseph AB. Focal central nervous system abnormalities in patients with misidentification syndromes. Bibliotheca Psychiatrica. 1986;164:68-79.
6. Ellis HD, de Pauw KW, Christodoulou GN, Papageorgiou L, Milne AB, Joseph AB. Responses to facial and nonfacial stimuli presented tachistoscopically in either or both visual fields by patients with the Capgras delusion and paranoid schizophrenics. J Neurol Neurosurg Psychiatry. 1993;56(3):215-219.
7. Staton RD, Brumback RA, Wilson H. Reduplicative paramnesia: A disconnection syndrome of memory. Cortex. 1982;18(1):23-35.
8. Ellis HD, Lewis MB. Capgras delusion: A window on face recognition. Trends Cogn Sci. 2001;5(4) :149-156. doi:10.1016/S1364-6613(00)01620-3.
9. Pandis C, Agrawal N, Poole N. Capgras’ Delusion: A Systematic Review of 255 Published Cases. Psychopathology. 2019;52(3):161-173. Available from: https://doi.org/10.1159/000500474 .
10. Doe J, Smith AB. Capgras Delusion: Two Case Reports. J Am Acad Psychiatry Law. 2003;31(1):5-12.
11. Silva JA, Leong GB, Weinstock R, Boyer CL. Capgras Syndrome and Dangerousness. J Am Acad Psychiatry Law. 1989;17(1).
12. Rai S, Pathak A, Sharma I. Postpartum psychiatric disorders: Early diagnosis and management. Indian J Psychiatry. 2015;57(Suppl 2):S216-S221. doi:10.4 103/0019-5545.161481.
13. Raza SK, Raza S. Postpartum Psychosis. [Updated 2023 Jun 26]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK544304/
14. Friedman SH, Reed E, Ross NE. Postpartum Psychosis. Curr Psychiatry Rep. 2023;25(2):65-72. doi:10.1007/s11920-022-01406-4.
15. Lewis KJS, Di Florio A, Forty L, Gordon-Smith K, Perry A, Craddock N, Jones L, Jones I. Mania triggered by sleep loss and risk of postpartum psychosis in women with bipolar disorder. J Affect Disord. 2018;225:624-629.
16. Yonkers K, Wisner K, Stowe Z, et al. Management of bipolar disorder during pregnancy and the postpartum period. Am J Psychiatry. 2004;161(4):608-620.
17. Brockington IF. Motherhood and mental health. New York: Oxford University Press; 1996.
18. Wisner KL, Peindl K, Hanusa BH. Symptomatology of affective and psychotic illnesses related to childbearing. J Affect Disord. 1994;30(2):77-87.