






Child Intervention for Drug Use: Insights from New Delhi
Implementation of the Child Intervention for Living Drug-free (CHILD): A Qualitative Study of Children, Parents and Treatment Staff in New Delhi
Hendrée E. Jones¹,², Rachel Middlestadt-Ellerson¹, Senga Carroll¹, Shannon Micklewright¹, Bilal Ahmad Naqati³, Manish Kumar³, Thom Browne⁴, and Rajesh Kumar³
- UNC Horizons (https://www.facebook.com/unchorizons/)
and Department of Obstetrics and Gynecology, University of North Carolina at Chapel Hill, NC USA - Department of Psychiatry and Behavioral Sciences, Johns Hopkins University, Baltimore, MD USA
- Society for Promotion of Youth and Masses, New Delhi, India
- Colombo Plan Secretariat, Colombo, Sri Lanka
OPEN ACCESS
PUBLISHED: 31 October 2025
CITATION: JONES, Hendree E. et al. Implementation of the Child Intervention for Living Drug-free (CHILD): A Qualitative Study of Children, Parents and Treatment Staff in New Delhi. Medical Research Archives, [S.l.], v. 13, n. 10, oct. 2025. Available at: <https://esmed.org/MRA/mra/article/view/7018>.
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI: https://doi.org/10.18103/mra.v13i10.7018
ISSN 2375-1924
Abstract
There is a growing and urgent worldwide need to reduce the number of children under 12 years of age using drugs. The Child Intervention for Living Drug-Free (CHILD) curriculum has been developed and implemented around the world to help clinicians treat children between the ages of 4-12 for drug use problems. The aim of the present study is to determine the barriers and benefits of the Child Intervention for Living Drug-Free for children enrolled in residential treatment for drug problems, for their parents/caregivers, and for the staff providing care to the children. Within two treatment programs operated by the Society for the Promotion of Youth and Masses (SPYM) in New Delhi, India, six focus groups were conducted. Focus group 1 had n=15 children, focus group 2 had n=8 children, focus group 3 had n=12 parents/caregivers, focus group 4 had n=6 parents/caregivers, focus group 5 had n=7 parents/caregivers and focus group 8 had n=8 staff. Findings revealed that children valued interactive, expressive activities that promoted personal growth and emotional well-being. Caregivers reported improvements in their child’s behavior but voiced concerns about their child’s possible future return to substance use, the impact of stigma on their families, and the lack of educational and vocational support in their communities. Staff praised the Child Intervention for Living Drug-Free curriculum’s engagement strategies but suggested simplifying content and increasing the use of visual and activity-based tools. Common themes across groups emphasized the importance of emotional resilience, decision-making skills, family support, and life skills linked to future employment. This qualitative evaluation underscores the importance of developmentally appropriate, family-centered, and community-supported approaches to child substance use treatment. While these findings are rooted in the Indian context, the challenges and solutions resonate globally. Given similar risk factors in the U.S., including lack of community support and peer pressure, the Child Intervention for Living Drug-Free curriculum offers a promising, adaptable model for early intervention especially for illicit drugs like fentanyl. Broader implementation and further research are recommended to support its effectiveness across diverse cultural settings.
Keywords
Child Interventions for Living Drug-Free (CHILD) curriculum, child substance use disorder, treatments, parenting, drug supply, barriers to implementation, focus groups
Introduction
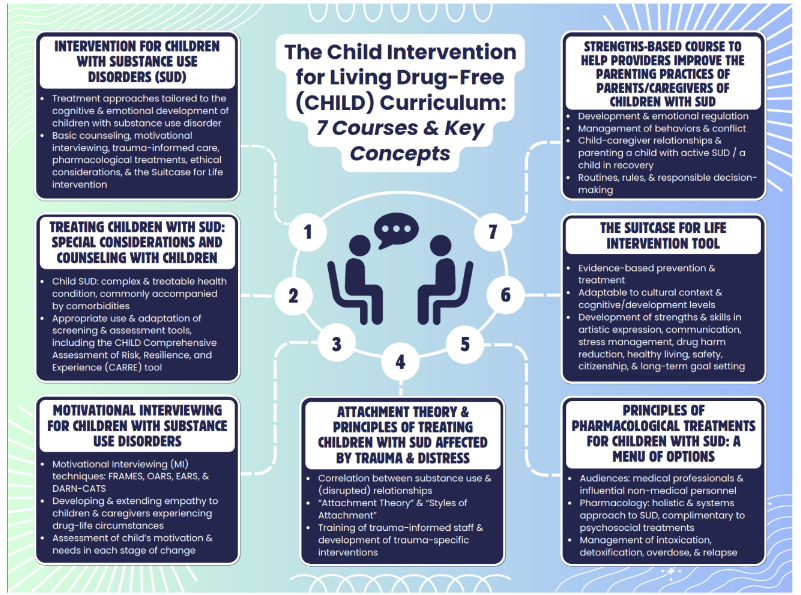
Worldwide, an expanding population of children are using psychoactive substances. This trend reiterates significant implications for the health and wellbeing of young individuals. For example, in the African country Sudan, 89% of surveyed children living in street circumstances reported substance use, primarily glue sniffing (87%) and tobacco smoking (67%). In Asia, risky behavior was also highlighted in Iran where children ages 7-19 years were engaging in harmful substance use including tobacco smoking (11%), alcohol use (14%), and other drug use (2%). Similarly, 88% of surveyed children in Nepal, half of whom were living in street circumstances, reported glue sniffing. Nearly half of this sample reported experiencing health complications such as headaches, chest pain, and stomach aches. While any drug use by children is concerning, the extent of children using heroin or opium in Afghanistan, Bangladesh, India and Pakistan has warranted an urgent need for both prevention and treatment strategies. For example, among children 7-12 years old in India initiating drug use disorder treatment, they report solvents (39%), cannabis (37%) and opioid (18%) use at treatment entry. Of those children, nearly 80% reported illegal activities for survival and half report using multiple drugs and growing up in a family with active drug use happening in their home. The urgent need for effective drug prevention and treatment were also heard in Argentina, Brazil, Ecuador, Central America, Paraguay, Peru, and Uruguay where cocaine and crack cocaine are used by young children. For example, a study in Brazil of children 8-17 years living in street circumstances reported that 60% were using drugs within the past year and 40% of these children considered themselves to have a substance use disorder. These global prevalence rates underscore social and environmental factors such as lack of community, school or government support, peer pressure, stress, and negative family interactions as significant contributors to higher rates of drug use among children. These findings highlight the need for early intervention programs tailored to the unique developmental and social needs of young children. The Child Intervention for Living Drug-Free (CHILD) curriculum was created to train treatment providers on how to screen, assess, and treat children between the ages of 4-12 years of age who are exposed to or actively using psychoactive substances (See Figure 1 for the seven modules). This was the first protocol developed for the treatment of substance use, especially opioid use, in children under 12 years old and was tailored to children’s ages and developmental stages. Among the 700+ children treated in Afghanistan with the initial version of the CHILD curriculum, there were substantial improvements in psychiatric disturbances, anxiety-related emotional disorders, social problems and overall perceived quality of life. Multiple studies of aspects of CHILD suggest a broadly impactful and possibly enduring intervention.
The Child Intervention for Living Drug-Free curriculum was most recently implemented in India. As such, the aim of the present paper is to identify the barriers and benefits for children who are enrolled in treatment for substance use problems, parents of the children in treatment and staff members providing treatment to children using the CHILD curriculum in India. By assessing barriers and benefits of the curriculum, this study seeks to inform future implementation of the CHILD curriculum and contribute to the broader discussion of early intervention strategies for child drug use, especially potentially lethal drug use like illicit fentanyl and other dangerous compounds found in the drug supply.
Materials and Methods
This study was determined to be exempt by the Institutional Review Board at the University of North Carolina in Chapel Hill.
SETTING AND PARTICIPANTS
The focus groups were held in spaces of the Society for the Promotion of Youth and Masses (SPYM) treatment centers that included the Delhi Gate Drug Treatment Centre for Children and the Nizamuddin Children Centre in Central Delhi. The Delhi Gate Drug Treatment Centre for Children offers residential treatment for children and adolescents struggling with substance use problems. The residential facility provides a range of services, including detoxification, psychotherapy, family counseling, and return to use prevention. The Nizamuddin Children Centre program focuses on children under six years of age, aiming to improve their health, nutrition, and early education. Key components include strengthening local aanganwadis (government-run childcare centers), implementing a pre-primary curriculum, and engaging the community through parenting programs. The initiative also addresses issues like malnourishment and school readiness among young children.
The participants in this study included 23 children receiving services at SPYM, 25 parents/caregivers of the children, and 8 staff members at SPYM. Six focus groups were conducted: two with children enrolled in services (one with 15 children and the other with 8 children), three with parents/caregivers (one with 12 participants, another with 6 participants, and the final one with 7 participants); and one with staff (8 participants). Eligibility criteria included the children being 7-12 years old and enrolled in SPYM treatment services. The parents and caregivers were invited to participate if they had children enrolled in the SPYM treatment services. The staff were invited to participate if they are currently employed with SPYM and working with children in the center. All who were invited agreed to participate. All participants were given small tokens of appreciation like snacks and beverages or supplies for living such as hygiene items.
PROCEDURES
Each focus group began with the introduction by the group facilitators who spoke Hindi and are part of the SPYM management team. The introduction included an overview of substance use disorder and elucidated the rationale behind conducting the focus group. A notetaker fluent in both Hindi and English took notes in Hindi and then translated the notes into English, ensuring that nuances of quotes were maintained. Other team members who were fluent in both languages reviewed the notes for accuracy.
MEASURES
Separate written focus group question guides for children, parents/caregivers and staff were used during the relevant focus group sessions. All focus groups were conducted in March of 2024. Questions for children and staff covered the same topics that included: What parts they liked best and why?; What parts they liked least and why?; What would they change about the modules?; What topics are missing that they want to learn about? And an open-ended question about what else they wanted to share about the modules? For the parents/caregivers, the questions included the topics of: What changes do they see in their children after they have been part of the program?; What are the biggest challenges that they face in parenting children who have drug problems?; What do they see as their biggest strengths in parenting?; What have you done well?; If we were to create special help for parents of children in our center, what would you want it to have?; And What are your hopes and dreams for your children?
Demographics were not collected on the participants in any of the focus group sessions in order to maintain the complete anonymity of participants.
DATA ANALYSIS
The listening sessions were hand transcribed. The transcript was reviewed for accuracy in Hindi and translated into English. We used line by line coding for the transcript and assigned each quotation or chunk of text a code corresponding to each of our topics of inquiry. We then read all of the quotations in each large code category and continued the analysis by dividing some of the codes into smaller sub-codes, adding some new codes that emerged from the data and looking for themes within and across the codes.
Results
For ease of presentation and to meet the aims of the study, the results are summarized by themes within each question by participant group.
CHILD RESPONSES
| Question | Themes | Example Quotes |
|---|---|---|
| What parts do you like best and why? |
|
|
| What parts do you like least and why? | Specific Activities Perceived as Less Enjoyable or Challenging |
|
| What would you change about the modules? |
|
|
| What topics are missing that you want to learn about? |
|
|
| What else would you like to tell us about the modules? |
|
|
Note: a total of 23 children participated in the focus groups.
In response to the question of what parts they like least and why, there was little that was found to be negative given the high level of enjoyment expressed in the first question. There were a few mentions of specific activities perceived as less enjoyable or challenging that included more passive and less interactive tasks like painting on the computer.
In terms of what they would change about the modules, there were three themes that emerged that included a greater focus on mental and emotional well-being, with participants expressing a desire for content focused on fostering a positive mindset and addressing emotional resilience. They also desired more information on decision-making and consequences as well as future planning and goal setting to structure their future and to establish meaningful life goals.
The main two themes from responses to topics that are missing underscore that the participants are young children. They reported a desire for more play opportunities. Children value playing and want more time or access to games, suggesting a need for unstructured or recreational activities as well as more time outside in open spaces—a challenging goal for programs in densely urban areas like New Delhi. A further theme was the positive impact of sports-based learning. Children appreciated the structured programs that combine physical activity with life skills or educational messages, indicating that sports are a meaningful and engaging way for them to learn.
Finally, the wisdom and insights of the children were seen in their additional recommendations. First, they expressed strong interest in sports, exercise, and facilities that support physical health as well as a desire to experience more creative and broader support structures for well-being and learning.
PARENT/CAREGIVER RESPONSES
| Question | Themes | Example Quotes |
|---|---|---|
| What changes do you see in your children after they have been part of the program? |
|
|
| What are the biggest challenges that you face in parenting children who have drug problems? |
|
|
| What do you see as your biggest strengths in parenting? What have you done well? |
|
|
| If we were to create special help for parents of children in our center, what would you want it to have? |
|
|
| What are your hopes and dreams for your children? |
|
|
Note: a total of 25 parents/caregivers participated in the focus groups.
There were two main themes that emerged in response to the question as to what are the biggest challenges that they face in parenting children who have drug problems. The theme of stigma and social isolation was almost universal. Parents/caregivers reported facing significant social stigma associated with their child’s drug use, which leads to secrecy, isolation, and sometimes contributes to family breakdown and violence. Related yet distinct from theme one was the theme of family conflict and safety concerns. Substance use among children often leads to conflict, violence, and safety concerns within the home, particularly affecting mothers, who are often the only ones caring for the child inside the home. Finally, there was the theme of environmental and peer influences. The community and peer environment heavily influence children’s drug use and risk for return to drug use, making sustained recovery more difficult despite family efforts.
In regard to what parents/caregivers see as their biggest strengths in parenting, there were three distinct themes. First was the idea of emotional regulation and positive role modeling. Many parents emphasized the importance of staying calm, avoiding anger, and acting as positive role models, recognizing that their behavior deeply influences their children. Their second theme of strengths included their active engagement in and support of their children’s lives. Parents described their efforts to be more present, create structure, and actively participate in their children’s lives to foster growth, connection, and resilience. Finally, a theme of protecting children from negative influences and substance use was found in the parent/caregiver responses. There were strong concerns about drug use and peer influence. Parents see it as their duty to guide children away from harmful environments and behaviors, despite challenges.
Parents/caregivers responded with answers that fell into three themes with regard to creating special help for parents of children in the center. The first theme was a desire for parental support and education. Parents/caregivers wanted structured support that educates them on substance use, the recovery process, and parenting strategies in greater detail than what is currently offered. The second theme was a greater emphasis on counseling and emotional support for families. There was a strong call for mental health support for both children and parents, including counseling and stress management. Finally, parents/caregivers wanted more educational and economic opportunities for children. Parents expressed concern about their children’s future, highlighting needs for education, vocational training, and employment support.
The focus groups intentionally ended with a positive focused question as to what their hopes and dreams for their children are. Three themes emerged that included supporting individual growth and interests, the desire for their child’s educational success and opportunity, and the desire for their child’s holistic development and well-being. Education emerged as a common hope, both as a path to success and as a way to overcome past disadvantages. Parents also expressed a wish for balance in their children’s lives that encompasses a focus on mental, emotional, and social growth alongside academic and educational achievement for economic independence.
STAFF RESPONSES
| Question | Themes | Example Quotes |
|---|---|---|
| What parts do you like best and why? |
|
|
| What parts do you like least and why? | Unintended Social Consequences |
|
| What would you change about the modules? |
|
|
| Staff were invited to share their opinions regarding any additional topics that could be incorporated into the modules for the children, as well as any potential topics that might be missing. |
|
|
Note: a total of 8 staff members participated in the focus groups.
Staff provided one theme in response to what they liked least and that was the unintended social consequences of using CHILD materials in a group. They reflected that some of the visual materials intended to aid understanding can unintentionally lead to negative peer interactions with children teasing each other about the material.
Staff recommendations for changes to CHILD fell into two themes. One was the need for simpler and more accessible content. Staff expressed a desire for the modules to be easier for children to understand, both in language and presentation. Secondly, staff expressed a desire for more interactive and engaging elements. Staff emphasized the importance of fun, activity-based learning to hold children’s attention.
Further, staff were invited to share their opinions regarding any additional topics that could be incorporated into the modules for the children, as well as any potential topics that might be missing. Their responses to these questions were categorized into three themes. The first included enhancing learning through engaging and visual tools. Staff emphasized the value of using multimedia and interactive formats to better communicate important messages to children. The second theme was promoting personal development and identity building of the children. Specific quotes provide ideas on how to enhance the focus on activities that support children’s personal growth, confidence, and self-awareness. The final theme was strengthening rehabilitation through real-life connections and skills. Staff suggested introducing real-life skills, support networks, and success stories to foster a sense of direction and hope among the children.
Discussion
The present study aimed to identify the barriers and benefits of the CHILD curriculum by learning from the responses of children who are enrolled in treatment for substance use problems, the parents of the children in treatment, and the staff providing treatment to children using the CHILD curriculum in India. By assessing barriers to and benefits of the curriculum, this study seeks to inform future implementation of the CHILD curriculum and contribute to the broader discussion of early intervention strategies for child drug use.
These findings suggest that children enrolled in treatment in New Delhi are experiencing serious problems with substance use, and that their families of origin are significantly stressed in a number of ways, particularly with concerns for their children’s future. These findings are consistent with previous studies in this patient population. The qualitative findings from the child, parent/caregiver, and staff focus groups present both converging and diverging perspectives on the effectiveness, impact, and areas for improvement of the CHILD intervention.
Children consistently endorsed their enjoyment of interactive, creative, and hands-on learning methods that allowed for self-expression and skill-building, such as games, storytelling, dancing, and computer use. Their feedback emphasized a desire for more play, emotional wellness support, decision-making skills, and future planning. Similarly, staff praised the modules for their ability to foster communication and engagement, while recommending enhancements to make content simpler, more visual, and more interactive. Children and staff shared a common preference for engaging formats that promote personal growth and real-life relevance.
In contrast, the parents’ perspectives centered more on long-term behavioral change, recovery sustainability, and the broader systemic and environmental challenges they face in raising their children. Parents reported initial improvements in their children’s behavior post-treatment but remained concerned about return to drug use due to peer influence and a lack of community support. Unlike children and staff, parents focused heavily on structural support needs, such as educational reintegration, vocational training, counseling, and help navigating stigma. While children asked for more engaging content and life skills, parents emphasized the need for holistic family support systems that could sustain change beyond the treatment center and the intervention. These differing focal points underscore the importance of tailoring interventions not only to children’s immediate learning needs but also to the familial and social ecosystems influencing their recovery.
Conclusions
The findings from this study reveal a rich and multifaceted portrait of the CHILD curriculum’s impact across key stakeholder groups that include children enrolled in residential treatment for drug use problems, their parents/caregivers, and the staff treating the children. The results highlight CHILD’s relevance and potential as an early intervention strategy for child substance use in India and beyond. Children enthusiastically endorsed the curriculum’s interactive and expressive elements, suggesting that hands-on, playful activities are crucial for meaningful engagement and learning. Their feedback also revealed a strong desire for additional content that supports emotional resilience, decision-making, and future planning. Children underscored their own potential and need for holistic development beyond traditional education. Similarly, staff echoed the value of engaging content and advocated for simpler, more accessible materials that foster connection, growth, and real-world relevance. These perspectives point to the power of dynamic, child-centered pedagogy in building life skills and encouraging personal transformation.
Conversely, parents offered a grounded lens into the long-term and structural challenges facing families of children with substance use disorders. While they observed notable positive behavior changes following treatment, parents remained deeply concerned about their child’s return to drug use potential, the social stigma on the child and family, and barriers to educational and economic advancement. Their feedback emphasizes that interventions like CHILD must extend beyond the treatment setting to address family and community ecosystems that influence recovery. Informed by these insights, this study recommends that future updates of the CHILD curriculum integrate deeper life-skills and employment skills, expand mental health and counseling support for both children and families, and be adapted for implementation in other contexts such as the United States. With childhood substance use emerging as a global concern, the CHILD model offers a promising, adaptable framework grounded in collaboration, empowerment, and whole-family care.
Conflicts of Interest Statement
The authors have no conflicts of interest to declare.
Funding Statement
Financial support for this project was provided by the National Institute on Drug Abuse (NIDA) R01 042822, The Bureau of International Narcotic and Law Enforcement Affairs (INL), US Dept of State, through Cooperative Agreement #GLO K42 with the Colombo Plan until a stop work order concluded funding on 1/28/25. The funding agencies had no involvement in study design, data collection, analysis, interpretation, or manuscript preparation. No contractual constraints on publishing have been imposed by NIDA or INL. The authors alone are responsible for the content and writing of this article. No honorarium, grant, or other form of payment was given to any author or any other individual to produce the manuscript.
Acknowledgements
The authors thank the SPYM staff for their hard work on this project. We also thank the children and families who gave their time and generously shared their experiences and knowledge with us.
References
- Aly SM, Omran A, Gaulier JM, Allorge D. Substance abuse among children. Arch Pediatr. 2020 Nov 1;27(8):480-4.
- Castelpietra G, Knudsen AK, Agardh EE, Armocida B, Beghi M, Iburg KM, et al. The burden of mental disorders, substance use disorders and self-harm among young people in Europe, 1990-2019: Findings from the Global Burden of Disease Study 2019. Lancet Reg Health Eur. 2022 May 1;16:100350.
- Embleton L, Mwangi A, Vreeman R, Ayuku D, Braitstein P. The epidemiology of substance use among street children in resource-constrained settings: A systematic review and meta-analysis. Addiction. 2013 Oct;108(10):1722-33.
- Hassan SM, Satti SA, Alhassan MA. Reasons for leaving home and pattern of child abuse and substance misuse among street children in Khartoum, Sudan: A cross-sectional survey. Pan Afr Med J. 2023;46:1.
- Motazedian N, Sayadi M, Beheshti S, Zarei N, Ghaderi J. High risky behavior and HIV/AIDS knowledge amongst street children in Shiraz, Iran. Med J Islam Repub Iran. 2020;34:138.
- Sah SK, Neupane N, Pradhan A, Shah S, Sharma A. Prevalence of glue-sniffing among street children. Nurs Open. 2020 Jan;7(1):206-11.
- Bhattacharjee S, Kumar R, Agrawal A, O’Grady KE, Jones HE. Risk factors for substance use among street children entering treatment in India. Indian J Psychol Med. 2016;38(5):419-23.
- Sultana MT, Hossain S, Parvin R, Islam MT, Mithy SA. Impact of drug addiction on street children: Perspective Dhaka City. Open Access Libr J. 2024;11:1-19.
- SGI Global, LLC. Afghanistan national drug use survey [Internet]. 2015 [cited 2025 Jun 28]. Available from: http://www.colombo-plan.org/?wpfb_dl=305
- Waheed A, Sarfraz M, Mahfooz A, Reza T, Emmanuel F. Risk factors for narcotic use in street children: A cross-sectional analysis from a low-middle-income country. Inq J Health Care Organ Provis Financ. 2025;62:00469580251324047.
- Peruvian children victims of narco-trafficking [Internet]. [cited 2025 Aug 4]. Available from: https://dialogo-americas.com/articles/peruvian-children-victims-of-narco-trafficking/
- Paco: Une histoire de drogue [Internet]. [cited 2025 Aug 4]. Available from: https://www.visapourlimage.com/en/festival/exhibitions/paco-une-histoire-de-drogue
- Torales J, González I, Castaldelli-Maia J, Waisman M, Ventriglio A. Early age of onset of drug use in Paraguayan children and adolescents: A public health challenge. Med Clín Soc. 2018;2(2):102-7.
- Gomes NM, Caldas ED. Street and drug use experiences among sheltered children and adolescents in the Federal District of Brazil. J Child Adolesc Psychiatr Nurs. 2022 Dec 1;36(2):105-13.
- Momand AS, Mattfeld E, Morales B, Ul Haq M, Browne T, O’Grady KE, et al. Implementation and evaluation of an intervention for children in Afghanistan at risk for substance use or actively using psychoactive substances. Int J Pediatr. 2017;2017:1-7.
- Jones HE, Momand AS, Lensch AC, Browne T, Morales B, O’Grady KE. Increasing substance use disorder treatment professionals’ knowledge: The Child Intervention for Living Drug-free (CHILD) curriculum. Children (Basel). 2021 Jan 23;8(2):1086.
- Interventions for children with substance use disorders [Internet]. International Society of Substance Use Professionals; [cited 2025 Aug 4]. Available from: https://www.issup.net/training/universal-treatment-curriculum/utc-31-interventions-children-substance-use-disorders
- Carroll S, Jones HE, Middlesteadt-Ellerson R, et al. Patterns of substance use among children ages 7-12 entering treatment for drug problems in India. J Addict Addictv Disord. 2023;10:146.
- Dhawan A, Pattanayak RD, Chopra A, Tikoo VK, Kumar R. Pattern and profile of children using substances in India: Insights and recommendations. Natl Med J India. 2017;30(4):217-21.
- Sharma N, Joshi S. Preventing substance abuse among street children in India: A literature review. Health Sci J. 2013;7(2):137-44.
- Tikoo VK, Dhawan A, Pattanayak RD, Chopra, A. Assessment of pattern and profile of substance use among children in India. National Commission for Protection of Child Rights (NCPCR) by National Drug Dependence Treatment Centre [NDDTC], All India Institute of Medical Sciences [AIIMS], New Delhi. 2013 [cited 2025 Sept 15].
- Dhawan A, Pattanayak RD, Chopra A, Tikoo VK, Kumar R. (2016). Injection drug use among children and adolescents in India: Ringing the alarm bells. Indian J Psychiatry, 2016;58(4), 387.
- HIV/AIDS Forum. Children, young people and HIV/AIDS. (http://www.indianngos.com/issue/hiv/resources/children.htm, accessed in September 2025).
- Texas School Survey of Substance Use. Texas A&M Health Science Center. [Internet]. [cited 2025 May 30]. Available from: https://www.texasschoolsurvey.org/
- Kaplow JB, Curran PJ, Dodge KA. Child, parent, and peer predictors of early-onset substance use: A multisite longitudinal study. J Abnorm Child Psychol. 2002;30(3):199-216.
- Whitesell M, Bachand A, Peel J, Brown M. Familial, social, and individual factors contributing to risk for adolescent substance use. J Addict. 2013;2013:579310.