

Comorbid ADHD and Anxiety: Treatment Prioritization Insights
Who’s on First? Case Report on Prioritizing Treatment for Comorbid Attention-Deficit/Hyperactivity and Anxiety Disorders
Kelly C. Lee, Pharm.D., MAS, BCPP¹; Natasha Bilinsky²; Jamie Kneebusch, Pharm.D., BCPS, BCPP³
- Professor of Clinical Pharmacy and Associate Dean, University of California San Diego Skaggs School of Pharmacy and Pharmaceutical Sciences, La Jolla, CA
- Research Assistant, University of California San Diego Skaggs School of Pharmacy and Pharmaceutical Sciences, La Jolla, CA
- Assistant Clinical Professor, University of California San Diego Skaggs School of Pharmacy and Pharmaceutical Sciences, La Jolla, CA
OPEN ACCESS
PUBLISHED: 31 October 2024
CITATION: Lee, KC., Bilinsky, N., et al., 2024. Who’s on First? Case Report on Prioritizing Treatment for Comorbid Attention-Deficit/Hyperactivity and Anxiety Disorders. Medical Research Archives, [online] 12(10). https://doi.org/10.18103/mra.v12i10.5906
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v12i10.5906
ISSN 2375-1924
Abstract
Early and optimal treatment of attention-deficit/hyperactivity disorder (ADHD) has been shown to prevent comorbid conditions. Unfortunately, due to delayed diagnosis or treatment of ADHD, psychiatric comorbidities often emerge that can also result in more disabling symptoms. Stimulants remain the gold standard for treatment of ADHD whereas serotonergic antidepressants are first line for anxiety disorders. Treatment of patients with ADHD and anxiety disorders presents a clinical conundrum due to the potential for stimulants to worsen anxiety symptoms. Many clinicians may defer treating ADHD initially and treating the anxiety disorder first. Unfortunately, untreated ADHD may worsen anxiety symptoms and expose patients to long-term treatment with anxiolytics that may be unnecessary. In this Clinical Case Discussion, we present the clinical and pathophysiological overlap between ADHD and anxiety disorders along with a clinical case. We present how a complete evaluation of the patient, including disturbance of symptoms on functioning and symptom onset, may help prioritize treatment strategies. Despite the reluctance to prescribe stimulants especially to adults due to stimulant misuse and exacerbation of other disorders, it may be optimal to treat ADHD first in order to reduce other manifestations.
Keywords: attention-deficit, hyperactivity, ADHD, anxiety, insomnia
Introduction
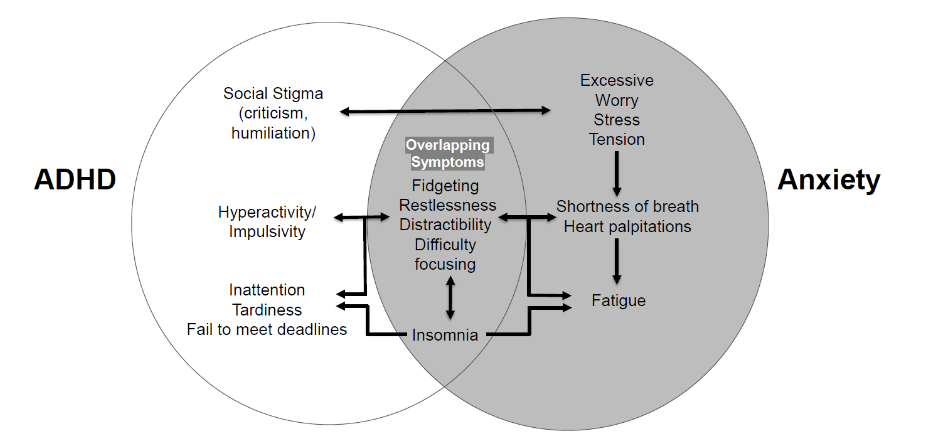
Adult attention-deficit hyperactivity disorder (ADHD) is often unrecognized or diagnosed later in life, with delayed or inadequate treatment resulting in psychiatric comorbidities. There is often a reluctance to prescribe stimulants in those with ADHD and comorbid anxiety; however, delaying treatment of ADHD in these individuals may result in worsening of both conditions. It is estimated that 2.5 percent of the general adult population has ADHD. Between 65-90% of adults diagnosed with ADHD suffer from at least one comorbidity, often anxiety disorder, that either precede or presents concomitantly with ADHD and complicates both diagnosis and treatment of ADHD. Generalized anxiety disorder has an estimated prevalence rate between five and six percent of the general adult population. Comorbid anxiety conditions may occur because of similar biological pathways involved in dopamine signaling within the frontal lobe being affected. Symptoms of ADHD such as impulsivity resulting from pathway dysfunction may increase behavioral and social problems that further contributes to anxiety (Figure 1). Those with ADHD may have procrastination as part of their ADHD symptoms, which induces anxiety by their failure to meet occupational and social expectations. Anxiety and ADHD are both affected by deficits in reward processing in ventral striatum with altered monoamine signaling. When comorbid with ADHD, anxiety becomes more severe, with earlier onset. Due to the interconnected nature of the disorders, it is essential to identify an effective treatment which may include treating one or both of the conditions. Leaving ADHD untreated may have negative consequences including deficient inhibition, attention, and executive functioning. Deficiencies in these areas can complicate self-esteem, time management, and academic success, leading to academic dismissal/voluntary leave, social impairments, employment and financial problems, motor vehicle accidents, and substance abuse. When ADHD is left untreated, comorbidities that may worsen over time inflict more burden on the patient.
In order to illustrate the complexities of treating an adult patient with ADHD and anxiety, we present a clinical case. We describe the presenting symptoms, treatment challenges and clinical considerations in managing such a patient.
Case Scenario
A 35-year-old female presents to the general psychiatry clinic with a history of ADHD, obesity, hyperlipidemia and prediabetes. The patient endorses symptoms of distractibility, difficulty focusing, difficulty with task initiation and task completion, disorganization, and losing personal items such as keys and cell phones. These symptoms significantly affect her functioning at home and work including a recent poor job performance review. She also endorses significant problems with difficulty falling asleep (reports constant thoughts in her head) where it would take about 3-4 hours to fall asleep. She also reports significant anxiety that interferes with her ability to interact with her co-workers and friends. She has had depressive episodes that have waxed and waned during her lifetime.
Psychiatric History:
- Depressive episodes during 18-19 years old along with passive suicidal ideation
- Suicide attempt at 19 years old
- Diagnosed with ADHD, primarily inattentive type, through Neuropsychiatric Testing at age 19 years and again in 26 years after being dismissed from college for poor performance
- Diagnosed with generalized anxiety disorder at 35 years old
- No inpatient psychiatric hospitalizations.
- Psychotherapy for 2 years after being dismissed from school for depression
- Psychotherapy and ADHD skills training at 33 years old
- No psychological trauma history; family psychiatric history notable for depression in maternal grandfather.
Medication Trials:
- Escitalopram up to 10 mg/day: Felt angry after 2 weeks and discontinued
- Adderall XR up to 30 mg/day: Tried for 1 year; Ineffective; discontinued
- Methylphenidate up to 10 mg/day: For breakthrough symptoms, caused excessive somnolence.
Social History:
- Caffeine: avoids due to sedation
- Alcohol: minimal (<1 drink/week)
- Other substances: denies except for prescription stimulants
Clinical Conundrum and Discussion
Treatment of comorbid ADHD and anxiety brings forth a paradox. Stimulants used to treat ADHD may exacerbate anxiety and antidepressants used to treat generalized anxiety may negatively affect ADHD symptoms. Treatment of the comorbid conditions only seems counterintuitive until the cyclical nature of the conditions is considered; treating one may alleviate both. Attention-deficit hyperactivity disorder and anxiety disorders have been theorized to have a bi-directional relationship with overlapping symptoms (Figure 1). In one study of adolescents, there appeared to be reciprocal within-person relationship between ADHD and anxiety symptoms. The association between ADHD and anxiety symptoms seems to be stronger in females but there remains lack of clarity on the relationship between these two disorders. Stimulants remain the preferred treatment of ADHD. However, a well-known side effect of these agents is increased or worsening anxiety. The clinical conundrum in this situation is how stimulants can be used effectively in patients with comorbid ADHD and anxiety. Ultimately, in cases where ADHD is the primary underlying condition, stimulants can lead to improvement in ADHD-related anxiety symptoms.
Identifying ADHD as the primary underlying condition can be established based on an effective psychiatric interview. It is important to gather sufficient information on which symptoms are causing the most impact in the patient’s day-to-day functioning. Triggers that worsening anxiety symptoms may be related to an alternate condition, like ADHD. If symptoms worsen from treatment of ADHD comorbidities, or if patients are nonadherent due to forgetfulness, ADHD could be considered the primary condition. By treating ADHD, comorbid conditions are more likely to improve.
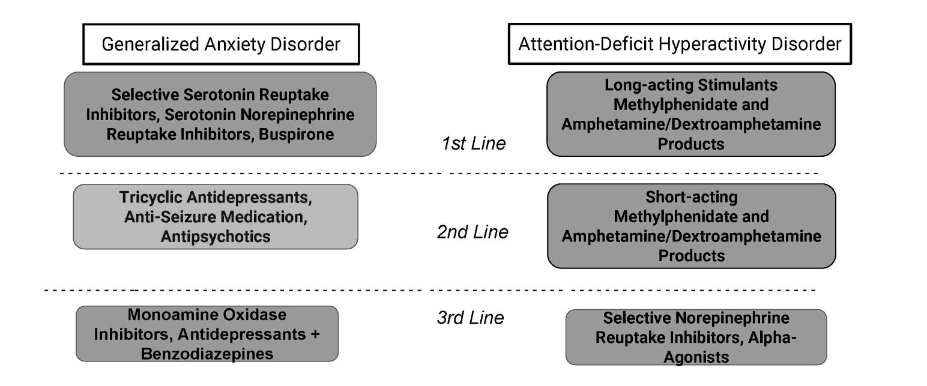
Treatment goals include providing evidenced based treatment for both conditions while minimizing side effects or worsening of one syndrome in the process (Figure 2). There are no contraindications to using stimulants alongside serotonergic antidepressants. However, initiation of two agents at one time can cloud the picture of what was helpful as the patient improves and potentially lead to unnecessary polypharmacy. Additionally, stimulants are one of the fastest working psychotropics available. Unlike antidepressants that can take weeks or months to appreciate the full benefit, stimulants typically show benefits to patients within days. Therefore, it could be appropriate to target ADHD initially with stimulants, given treatment provides rapid improvement and subsequently evaluate if treatment of anxiety is even needed. In those with an anxiety disorder and ADHD, a stimulant may be tried alone, or in combination with a selective serotonin reuptake inhibitor (SSRI). In those patients who fail stimulants or may have comorbid substance use disorder where stimulants would not be preferred first-line, non-stimulants such as atomoxetine can be used. Results of a study by Geller support the consideration of the non-stimulant atomoxetine for treatment of ADHD and comorbid anxiety. Atomoxetine effectively reduced ADHD symptoms in patients with comorbid ADHD and anxiety and was well tolerated, with a reduction in independently assessed anxiety symptoms. It is recommended that primary sleep disorders (such as sleep apnea and restless leg syndrome) should be ruled out before initiating ADHD treatment.
Case Conclusion
Upon conducting a thorough history, the patient’s depressive and anxiety symptoms were deemed primarily due to her lifelong struggles with ADHD symptoms. Her difficulty with school and work performance along with impacted interactions with her friends and co-workers due to her inattentiveness and distractibility have resulted in social and generalized anxiety symptoms.
She was open to trialing a long-acting methylphenidate, Concerta, for her daytime symptoms. The patient was titrated to an effective dose of 54 mg/day. She was also prescribed Adderall IR 10mg/day in the afternoon for residual symptoms.
Physical activity and sleep hygiene should always be encouraged in patients with ADHD and mood/anxiety disorders. Physical activity has been demonstrated to help with mood and anxiety disorders as well as ADHD and should be recommended for children and adults. Psychotherapy such as CBT should also be recommended along with structured serial assessments to ensure response to treatment and treatment adherence.
Conclusions
Attention-deficit/hyperactivity disorder, while not as prevalent as mood and anxiety conditions, can be disabling due to the myriad symptoms that affect functioning but also the psychiatric comorbidities. The comorbidity of ADHD and anxiety disorders present a particularly difficult treatment conundrum due to worsening of anxiety symptoms caused by the gold standard treatment for ADHD, namely stimulants. There is a vicious cycle between untreated ADHD that can worsen anxiety, treatment of ADHD that can worsen anxiety and untreated anxiety that can worsen symptoms of ADHD. Ultimately, comorbid ADHD and anxiety should be considered as interdependent conditions.
Treatment of comorbid ADHD and anxiety should be individualized, by focusing on identifying symptoms that are most distressing or disabling in each patient. Providers should exercise caution before initiating multiple pharmacologic therapies for both ADHD and anxiety disorders at one time. This strategy may result in unnecessary treatment or even worsening of symptoms or adverse effects. Stimulant use should not be discouraged in patients with anxiety disorders and may provide the clinician with a clear picture sooner rather than later due to the fast acting nature of stimulants. Patients with ADHD should also be screened for sleep disorders and other anxiety disorders to ensure that other causes for ADHD symptoms are not missed.
Conflicts of Interest and Source of Funding:
The authors have no conflicts to disclose and there were no funding sources for this project.
Take Home Points
- Patients with ADHD often have comorbid conditions that complicate the clinical picture and treatment.
- Clinicians may be faced with a clinical conundrum of managing a patient with ADHD and comorbid anxiety disorders.
- Treatment of comorbid ADHD and anxiety should be individualized, by focusing on identifying symptoms that are most distressing in each patient.
- Stimulants should be initiated in patients with disabling ADHD symptoms; this may alleviate anxiety symptoms rather than worsening them.
References
- Oliva F, Malandrone F, Mirabella S, Ferreri P, di Girolamo G, Maina G. Diagnostic delay in ADHD: Duration of untreated illness and its socio-demographic and clinical predictors in a sample of adult outpatients. Early Interv Psychiatry 2021;15(4):957-965. Doi: 10.1111/eip.13041.
- Katzman MA, Bilkey TS, Chokka PR, Fallu A, Klassen LJ. Adult ADHD and comorbid disorders: clinical implications of a dimensional approach. BMC Psychiatry 2017;17(1):302. Doi: 10.1186/s12888-017-1463-3.
- Quenneville AF, Kalogeropoulou E, Nicastro R, Weibel S, Chanut F, Perroud N. Anxiety disorders in adult ADHD: A frequent comorbidity and a risk factor for externalizing problems. Psychiatry Res 2022;310:114423. Doi:10.1016/j.psychres.2022.114423.
- Sobanski E. Psychiatric comorbidity in adults with attention-deficit/hyperactivity disorder (ADHD). Eur Arch Psychiatry Clin Neurosci 2006;256 Suppl 1:i26-31. Doi: 10.1007/s00406-006-1004-4.
- Generalized Anxiety Disorder. National Institute of Mental Health. Available: https://www.nimh.nih.gov/health/statistics/generalized-anxiety-disorder. Accessed September 24, 2024.
- Managing ADHD in children, adolescents, and adults with comorbid anxiety in primary care. Prim Care Companion J Clin Psychiatry 2007;9(2):129-38.
- Shaw M, Hodgkins P, Caci H, et al. A systematic review and analysis of long-term outcomes in attention deficit hyperactivity disorder: effects of treatment and non-treatment. BMC Med 2012;10:99. Doi: 10.1186/1741-7015-10-99.
- Murray AL, Caye A, McKenzie K, et al. Reciprocal developmental relations between ADHD and anxiety in adolescence: a within-person longitudinal analysis of commonly co-occurring symptoms. J Atten Disord 2022;26(1):109-118. Doi:10.1177/1087054720908333.
- Baldwin JS, Dadds MR. Examining alternative explanations of the covariation of ADHD and anxiety symptoms in children: a community study. J Abnorm Child Psychol 2008;36(1):67-79. Doi:10.1007/s10802-007-9160-1.
- Becker SP, Luebbe AM, Stoppelbein L, Greening L, Fite PJ. Aggression among children with ADHD, anxiety, or co-occurring symptoms: competing exacerbation and attenuation hypotheses. J Abnorm Child Psychol 2012;40(4):527-42. Doi:10.1007/s10802-011-9590-7.
- Jarrett MA, Wolff JC, Davis TE, 3rd, Cowart MJ, Ollendick TH. Characteristics of children with ADHD and comorbid anxiety. J Atten Disord 2016;20(7):636-44. Doi:10.1177/1087054712452914.
- Jensen CM, Amdisen BL, Jorgensen KJ, Arnfred SM. Cognitive behavioural therapy for ADHD in adults: systematic review and meta-analyses. Atten Defic Hyperact Disord 2016;8(1):3-11. Doi: 10.1007/s12402-016-0188-3.
- Biederman J, Monuteaux MC, Spencer T, Wilens TE, Faraone SV. Do stimulants protect against psychiatric disorders in youth with ADHD? A 10-year follow-up study. Pediatrics 2009;124(1):71-8. Doi:10.1542/peds.2008-3347.
- The ADHD Diagnostic Process. Children and Adults with Attention-Deficit/Hyperactivity Disorder (CHADD). Available: https://chadd.org/for-professionals/the-adhd-diagnostic-process/. Accessed September 8, 2024.
- Clinical Practice Guideline for the Diagnosis, Evaluation, and Treatment of Attention-Deficit/Hyperactivity Disorder in Children and Adolescents. Children and Adults with Attention-Deficit/Hyperactivity Disorder (CHADD). Available: https://chadd.org/for-professionals/clinical-practice-guidelines/. Accessed September 8, 2024.
- Khoodoruth MAS, Ouanes S, Khan YS. A systematic review of the use of atomoxetine for management of comorbid anxiety disorders in children and adolescents with attention-deficit hyperactivity disorder. Res Dev Disabil 2022;128:104275. Doi: 10.1016/j.ridd.2022.104275.
- Geller D, Donnelly C, Lopez F, et al. Atomoxetine treatment for pediatric patients with attention-deficit/hyperactivity disorder with comorbid anxiety disorder. J Am Acad Child Adolesc Psychiatry 2007;46(9):1119-1127. Doi:10.1097/chi.0b013e3180ca8385.
- Hvolby A. Associations of sleep disturbance with ADHD: implications for treatment. Atten Defic Hyperact Disord 2015;7(1):1-18. Doi:10.1007/s12402-014-0151-0.
- Heissel A, Heinen D, Brokmeier LL, et al. Exercise as medicine for depressive symptoms? A systematic review and meta-analysis with meta-regression. Br J Sports Med 2023;57(16):1049-1057. Doi:10.1136/bjsports-2022-106282.
- Leon-Barriera R, Ortegon RS, Chaplin MM, Modesto-Lowe V. Treating ADHD and Comorbid Anxiety in Children: A Guide for Clinical Practice. Clin Pediatr (Phila) 2023;62(1):39-46. Doi:10.1177/00099228221111246.