





Comprehensive Sexual Health Education for Youth Needs
Data Supporting a Comprehensive Approach to Reproductive and Sexual Health Education to Meet the Needs of Youth
Elissa Barr¹, Carmen Smotherman², Michele Moore³, Zhigang Xie⁴, Emily Balaguer⁵
- Professor of Public Health, University of North Florida, Department of Public Health, 1 UNF Dr., Jacksonville, FL 32224; 1-904-620-1479.
- Research Administrator, University of Florida, College of Medicine–Jacksonville, Department of Pathology and Laboratory Medicine, 655 W 8th St., Jacksonville, FL 32209; 1-904-244-3119.
- Dean of the Graduate School, University of North Florida, Graduate School, 1 UNF Dr., Jacksonville, FL 32224; 1-904-620-1989.
- Assistant Professor of Public Health, University of North Florida, Department of Public Health, 1 UNF Dr., Jacksonville, FL 32224; 1-904-620-2840.
- Public Health Graduate Assistant, University of North Florida, Department of Public Health, 1 UNF Dr., Jacksonville, FL 32224; 1-904-620-1479.
E-mail: [email protected]
OPEN ACCESS
PUBLISHED: 31 December 2024
CITATION: Barr, E., Smotherman, C., et al., 2024. Data Supporting a Comprehensive Approach to Reproductive and Sexual Health Education to Meet the Needs of Youth. Medical Research Archives, [online] 12(12).
https://doi.org/10.18103/mra.v12i12.6140
COPYRIGHT: © 2024 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v12i12.XXXX
ISSN 2375-1924
ABSTRACT
In the United States, reproductive and sexual health education continues to be greatly debated. Although research documents a more comprehensive approach to sex education is preferred by the majority and is effective in reducing risky sexual behaviors among adolescents, current state level direction in Florida is promoting more abstinence education. This is concerning as adolescents continue to engage in risky sexual behaviors and experience high rates of sexually transmitted diseases, HIV, and unplanned pregnancy. Researchers in this study assessed support for sex education in one large district in the state of Florida to document the preferred approach and to identify specific topics perceived as being important to include. A total of 605 participants completed a 32-item survey administered through random digit dialing to include both landlines and cell phones. Data were analyzed using SAS® for Windows Version 9.4, with significance set at 5%. Pearson’s Chi-square tests were used to investigate differences in responses by participants’ characteristics, and several are noted in this study. Results document overwhelming support for a comprehensive approach to sex education, and support for a variety of topics to include in sex education for both middle school and high school students. These results confirm that the state of Florida’s push for a more restrictive curriculum is not consistent with the preference of the majority and does not meet the needs of youth. It is hoped that these results can better guide policy decisions while also supporting others in determining their local support to help promote positive change.
Introduction
Currently in the United States (U.S.), reproductive and sexual health education in middle school and high school is inconsistent, lacking in most areas, and remains under scrutiny¹. The Centers for Disease Control and Prevention (CDC) identifies 22 critical sexuality education topics. Yet only 24% of middle schools (grades 6–8) and 45% of high schools (grades 9–12) in the U.S. reported addressing all 22 topics in 2022. Additionally, only three states have laws requiring comprehensive sexuality education be taught in all schools, 16 states provide abstinence-only sexuality education, and only 13 states require sex education to include information on consent¹.
In Florida, the focus of this study, there have been major shifts in state policy resulting in discouraging most of these reproductive and sexual health education topics from being taught to students in any grade⁶. This drastic decline in the coverage of sexual health education topics, however, is not consistent with the findings that most people support teaching these topics.
Despite the lack of consistent implementation of sexuality education in schools, and the recent reductions in the topics allowed in Florida, the majority of people continue to support a more comprehensive approach including topics such as contraception, condoms, gender identity, sexual orientation, healthy relationships, and more⁴¹⁴.
In a meta-analysis of 23 completed surveys assessing sexuality education in U.S. schools between 2006 and 2016, Szucs et al. discovered that “across all survey findings, 88.7% of respondents supported sexual health education” (p. 598). In this same analysis, “among surveys that only included parents or oversampled for parents, 90.0% (95% confidence interval = 86.5–93.4) supported sexual health education, and among nationally representative surveys, 87.7% (95% confidence interval = 85.1–90.6) of respondents supported sexual health education” (p. 598).
Additionally, the data-driven national objectives in Healthy People 2030 include improving indicators for sexually transmitted infections, family planning, and violence prevention¹⁵.
This document also specifically states to “increase the proportion of adolescents who get formal sex education before 18 years” (FP-08)¹⁵. From a global perspective, the World Association for Sexual Health states that everyone has a right to education, including comprehensive sexuality education that is “age-appropriate, scientifically accurate, culturally competent, and grounded in human rights, gender equality, and a positive approach to sexuality and pleasure”¹⁶. It is important to continue to document community and professional support at a time when reproductive and sexual health education is lacking.
More sexual health education is needed as adolescent sexual behaviors in the U.S. remain high. According to the CDC’s 2021 Youth Risk Behavior Survey (YRBS), 30% of high school students (grades 9 through 12) reported ever having had sex, ranging from approximately 16% in 9th grade to just over 48% in 12th grade¹⁷.
When reviewing Florida-specific 2021 YRBS data, more Florida youth report having had sex, with 36% responding yes, ranging from 19% in 9th grade to 54% in 12th grade. Among students in 12th grade, almost 11% of females nationally (16% in Florida) and 14% of males nationally (17% in Florida) report having had four or more sexual partners.
Additionally, over half of all 12th grade students (54% nationally, 53% in Florida) did not use a condom at last intercourse, and one in five (20% nationally, 21% in Florida) reported drinking alcohol or using drugs before last sexual intercourse. Finally, 91% of 12th grade students both nationally and in Florida reported never having been tested for HIV¹⁷. These numbers are concerning as risky sexual behaviors affect sexual health outcomes.
Adolescents face serious negative health outcomes of risky sexual behavior, including epidemic rates of STDs and HIV. More than half of Americans will acquire an STD in their lifetime, while young people aged 15–24 account for nearly half of the 26 million estimated new STD infections each year¹⁸.
The highest rates of both Chlamydia and Gonorrhea are among young people aged 20 to 24, closely followed by those 15 to 19¹⁹. Among the estimated 31,800 new HIV infections in 2022, persons aged 13–24 accounted for 6,400 cases (20%), and 42,200 young people in this age group were living with HIV²⁰.
Also, during this same year, the state of Florida was identified as one of eight states that accounted for 57% of all new HIV infections²⁰. According to the Florida Department of Health, one in every 154 adults in Florida were living with HIV in 2020²¹.
Teens also experience high rates of unplanned pregnancy and teen birth. Although on a downward trend since 2013, the teen pregnancy rate was 31 per 1,000 teens in 2017²². Approximately one in four female teens in the U.S. will become pregnant by age 20²², and just over half of teen moms (51–54%) receive a high school diploma²³⁻²⁴.
There were 146,973 births to teens aged 15–19 in 2021, and during this same year, the birth rates for teens aged 15–17 and 18–19 were 5.6 and 26.6, respectively²⁵. The U.S. teen birth rate remains higher than in other high-income countries, despite these steady declines²⁶.
To reduce risky sexual behaviors and the associated negative health outcomes among adolescents, sexual health education is an effective strategy²⁷⁻²⁸. However, sexual health education is still controversial and highly debated in the U.S., particularly in Florida¹².
With research confirming the need for and the effectiveness of reproductive and sexual health programs, documenting local support can be one strategy in supporting districts to improve their sexual health education. This article describes the results of a survey assessing support for offering comprehensive reproductive and sexual health education in a large northeast school district in Florida and includes an analysis of demographic variables influencing support.
Methods
INSTRUMENT
After a review of existing state and national surveys assessing support for school-based sex education, the 2022 Reproductive and Sexual Health Education Survey was developed¹³,²⁹⁻³³.
An expert panel reviewed the survey for content and face validity, along with readability. Members of the expert panel consisted of health researchers, school district personnel (health teachers, grant staff), and health department personnel. Feedback resulted in minor edits, including the rewording of some questions and the rearrangement of others.
The final survey consisted of 32 total close-ended questions. One question asked participants to select one of three approaches to sexual health education they prefer:
- Schools should not teach reproductive and sexual health education
- Schools should only promote abstinence and not teach about birth control and safe sex practices
- Schools should promote abstinence and teach about birth control and safe sex practices
Four-level Likert-style questions also included:
- Overall support for reproductive and sexual health education in middle school and high school
- Support for individual topics as part of a reproductive and sexual health program
- Support for individual reproductive and sexual health services being offered
- Demographic questions
This paper presents findings regarding support for this education in both middle school and high school.
SAMPLE
A sample of the population (adult Duval County residents) was selected using Random-Digit-Dialing (RDD) methodology for both landlines and cell phones. RDD telephone numbers were provided by Marketing Systems Group (MSG).
For individuals answering on a landline telephone, the interviewer asked the first qualified respondent to participate. Cell phone sample respondents were selected by being the first qualified participant to answer the phone.
The breakdown of landline to cell phone responses was 17% to 83%. The final sample consists of 605 Duval County residents, aged 18 or older.
To ensure a representative sample and to adjust for nonresponse bias, all data were weighted
adult population of Duval County. Data were first weighted to educational attainment for individuals 25 and over, and then to age, sex, and race/ethnicity. Demographic weights were calculated using the U.S. Census Bureau’s American Community Survey (ACS) 2020 5-year estimates for the adult population of Duval County. Party registration information was obtained from the election authorities in each county. All weighted demographic variables were applied using the SPSS version 27 rake weighting function, which will not assign a weight if one of the weighting demographic variables is missing. Individuals with missing demographic data were manually assigned a weight of 1.
DATA COLLECTION: Data collection took place at the University of North Florida Public Opinion Research Laboratory with its 27-station Computer Assisted Telephone Interviewing (CATI) system from November 10 to November 18, 2022. Respondents were contacted by live callers via telephone from 4:00 to 9:00 p.m. daily with up to three callbacks. Callers confirmed participant consent by first asking if respondents were willing to participate. This study had a 7.4% response rate, using the American Association of Public Opinion Research (AAPOR) Response Rate 3 (RR3) calculations. The overall margin of error for the study is +/- 4.0 percentage points.
DATA ANALYSIS: Participants’ baseline characteristics and their reported overall support for the three approaches of sexual health education were summarized using crude (unweighted) frequencies and percentages. To determine how important it is to have reproductive and sexual health as part of the high school and middle school curriculum, the participants’ responses to these two questions were combined into “Very or somewhat important” and “Not too important or not important at all.” The responses to questions regarding their level of support for the eight topics in high school and the eight same topics in middle school were combined into “Strongly or somewhat support” vs “Strongly or somewhat oppose.” Pearson’s Chi-square tests were used to investigate if there were differences in responses by participants’ characteristics. Weighted data were used in these statistical analyses and results from weighted analyses are reported. The level of significance was set at 5%. All analyses were done in SAS® for Windows Version 9.4.
Results
There were 605 participants in this study. The majority were over 45 years old (55%), females (57%), white (65%), not Hispanic (91%), and were college or post-college graduates (50%) (Table 1).Variable
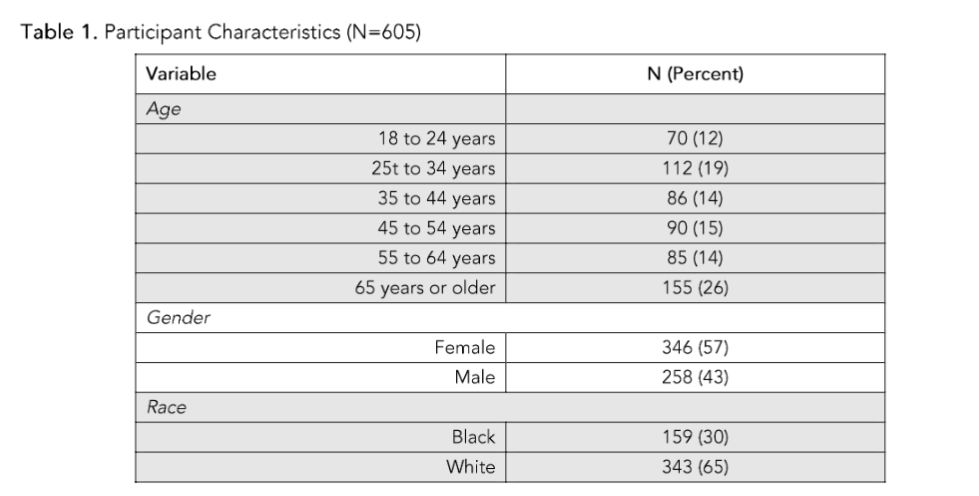
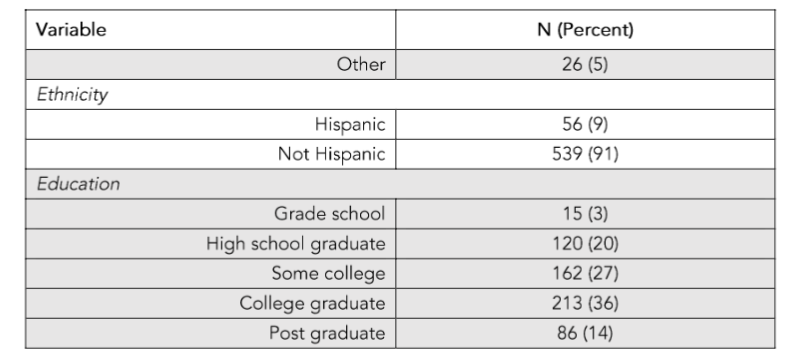
Note: Other race includes American Indian or Alaska Native, Asian, other/mixed races
Overall, 86% of participants reported that they consider sexuality education to be important in high school, with a higher proportion reporting it as important among younger participants (from 95% among 18 to 24 years old, to 80% among 65 years old or older, p=0.004), minority participants (94% black, p=0.001; 86% Hispanic, p=0.004), and those with less education (100% grade school and 88% high school, compared to 85% to 86% with some college or more, p=0.015) (Table 2).
Of all the participants, 69% reported that sexuality education is important in middle school, with more considering it important among younger compared to older ages (p=0.029), females (p=0.005), and Hispanics (p=0.006). Most participants support both promoting abstinence and teaching about birth control and safer sex (83%), while 11% did not support teaching it at all, and 7% support only teaching abstinence. Significant findings include higher support for both promoting abstinence and teaching about birth control and safer sex among younger participants (p=0.004) and those with less education (p=0.046) (Table 2).
Table 2. Support for Sexual Health Education and Education Types
Overall Totals
- High school importance: 511 (86%) important, 80 (14%) not important
- Middle school importance: 407 (69%) important, 180 (31%) not important
- Public school approach:
- 480 (83%) support abstinence + birth control/safe sex
- 61 (11%) do not support teaching
- 38 (7%) abstinence only
By Age (p-values: 0.004, 0.029, 0.004)
| Age Group | HS Important | MS Important | Support Comprehensive |
|---|---|---|---|
| 18–24 | 63 (95%) | 52 (79%) | 59 (90%) |
| 25–34 | 119 (92%) | 98 (77%) | 102 (80%) |
| 35–44 | 88 (92%) | 70 (72%) | 86 (88%) |
| 45–54 | 84 (89%) | 67 (70%) | 83 (88%) |
| 55–64 | 71 (74%) | 60 (63%) | 68 (76%) |
| 65+ | 87 (80%) | 60 (58%) | 81 (79%) |
By Gender (p-values: 0.307, 0.005, 0.060)
| Gender | HS Important | MS Important | Support Comprehensive |
|---|---|---|---|
| Female | 274 (88%) | 234 (75%) | 263 (87%) |
| Male | 240 (84%) | 176 (63%) | 221 (78%) |
By Race (p-values: 0.001, 0.338, 0.168)
| Race | HS Important | MS Important | Support Comprehensive |
|---|---|---|---|
| Black | 156 (94%) | 120 (73%) | 145 (88%) |
| White | 253 (83%) | 197 (66%) | 239 (82%) |
| Other | 37 (71%) | 33 (63%) | 33 (64%) |
By Ethnicity (p-values: 0.004, 0.006, 0.131)
| Ethnicity | HS Important | MS Important | Support Comprehensive |
|---|---|---|---|
| Hispanic | 54 (96%) | 49 (84%) | 52 (89%) |
| Not Hispanic | 453 (85%) | 354 (67%) | 426 (82%) |
By Education (p-values: 0.015, 0.141, 0.046)
| Education | HS Important | MS Important | Support Comprehensive |
|---|---|---|---|
| Grade school | 19 (100%) | 16 (81%) | 21 (100%) |
| High school | 146 (88%) | 108 (68%) | 130 (82%) |
| Some college | 186 (85%) | 144 (65%) | 183 (85%) |
| College grad | 116 (86%) | 104 (77%) | 109 (81%) |
| Post grad | 44 (85%) | 38 (74%) | 39 (80%) |
Notes:
- Percentages are weighted
- p-values calculated using Pearson Chi-square test
- “Important” = very/somewhat important
- “Not important” = not too/not at all important
Table 3. Overall Support for Sexual Health Topics
Topic Middle High How to deal with pressure to have sex 74% 84% How to talk with parents about sex and relationships 78% 85% Human anatomy and reproduction 81% 93% HIV and STDs 80% 93% Abstinence from sexual activity 78% 86% Birth control methods 72% 87% Condom use 70% 87% Gender and sexual orientation 58% 66% Data are counts (percentages) indicating responses of those who selected “strongly important” or “somewhat important” to teach. Other response options included “somewhat oppose,” “strongly oppose,” and “don’t know.”
RELATIONSHIPS BETWEEN DEMOGRAPHICS AND SUPPORT FOR SEXUAL HEALTH EDUCATION TOPICS:
Although all respondents regardless of age, gender, race/ethnicity, and education were supportive of teaching the eight specific sexual health topics in both high school and middle school, there were several significant differences among these demographics. When analyzing support of the topics being taught in high school by demographic variables, all demographics (age, gender, race/ethnicity, education) were found to be significantly associated with at least one of the eight topics (Appendix A). When analyzing support of the topics being taught in middle school by demographic variables, all demographics but one (education) were found to be significantly associated with at least one of the eight topics (Appendix B).SIGNIFICANT DIFFERENCES BY AGE:
Younger respondents were more likely to support teaching about how to deal with pressure (p=0.014), anatomy and reproduction (p < 0.001), HIV and STDs (p < 0.001), abstinence (p=0.040), birth control (p=0.001), condom use (p < 0.001), and gender and sexual orientation (p < 0.001) in high school (Appendix A). Regarding support for topics in middle school, younger respondents were more likely to support teaching how to deal with pressure (p=0.0007), anatomy and reproduction (p < 0.001), HIV and STDs (p=0.025), condom use (p=0.022), and gender and sexual orientation (p < 0.001) (Appendix B).SIGNIFICANT DIFFERENCES BY GENDER:
Female respondents were significantly more likely than males to support teaching about how to deal with pressure (p=0.027) and abstinence (p=0.047) in high school (Appendix A). Regarding support for topics in middle school, female respondents were more likely to support teaching about how to talk to parents (p=0.010) and birth control (p=0.022) (Appendix B).SIGNIFICANT DIFFERENCES BY RACE/ETHNICITY:
Although respondents of all races were supportive of teaching most sexual health education topics in general, blacks were statistically more likely than whites and other races to support teaching about how to talk to parents (p=0.0009), abstinence (p=0.001), birth control (p=0.050), condom use (p=0.008), and gender and sexual orientation (p=0.002) in high school (Appendix A). Also, among topics taught in high school, Hispanic versus non-Hispanic were more supportive of teaching about how to talk to parents (p=0.007), HIV and STDs (p=0.001), condom use (p=0.021), and gender and sexual orientation (p=0.015) (Appendix A).Regarding support for topics in middle school, blacks were statistically more likely than whites and other races to support teaching about abstinence (p=0.044) and gender and sexual orientation (p=0.040) (Appendix B). Also, among topics taught in middle school, Hispanic versus non-Hispanic were more supportive of teaching about how to deal with pressure (p=0.009), anatomy and physiology (p=0.012), abstinence (p=0.018), condom use (p=0.032), and gender and sexual orientation (p=0.005) (Appendix B).
SIGNIFICANT DIFFERENCES BY EDUCATION:
Respondents with less than a high schooleducation were more likely than those with a high school degree, some college, or a college degree to support teaching HIV and STDs in high school (p=0.050) (Appendix A). There were no significant differences in support for topics taught in middle school by education (Appendix B).
Discussion
Results from this study add to the research documenting support for a more comprehensive approach to reproductive and sexual health education¹¹,¹³,¹⁴,²⁷,²⁹,³⁰,³¹,³⁴,³⁵. Among participants, 83% prefer schools teach abstinence, birth control and safer sex, while 11% prefer schools do not teach it at all, and 7% prefer schools only teach abstinence. These results support the widespread adoption of the National Sexuality Education Standards that recommend numerous age-appropriate topics be included in sexuality education³. These findings are also consistent with the views of national and international organizations such as the American Medical Association³⁶, the American Academy of Pediatrics³⁷, and the World Health Organization³⁸ who recommend comprehensive sexuality education for youth.
Comprehensive programs provide medically accurate, age-appropriate, and inclusive information about a variety of topics to include abstinence, anatomy and physiology, safer sex practices, contraception and condoms, gender, sexual orientation, consent and healthy relationships, communication skills, and human development³⁹,⁴⁰. They enable individuals to make decisions about their bodies and are offered throughout the students’ school years⁴⁰.
Overall, participants were supportive of sexual health education with 86% reporting it is important to teach in high school and 69% in middle school. The majority supported all eight topics in both high school and middle school. It was not surprising that one of the topics to receive the most support was HIV and STDs, 80% in middle school and 93% in high school, as Florida ranks among the top three states in the US for the highest incidence and prevalence of HIV⁴¹.
The topic of gender and sexual orientation received the least support yet was still supported by well over half of respondents in both middle school (58%) and high school (66%). This topic also had the greatest range in support by age. Over 80% of participants aged 18 to 24 reported being supportive of this topic, while only about 50% of older adults aged 65 and above did. This suggests that the younger generation is less likely to view this topic as controversial compared to their older counterparts. This finding may also reflect the needs of the younger generation.
Although this topic may be perceived as being controversial, additional studies also document that the majority of people support teaching about gender and sexual orientation in schools¹¹,¹³,¹⁴,³⁴. This topic is particularly important to include when teaching sexual health education as The Trevor Project (2023) confirmed that a more affirming environment for LGBTQ youth can be beneficial, as approximately two-thirds of them face more harassment and mental health challenges than other students⁴².
Several significant differences in support of topics across demographic variables are worth noting. Females were more supportive than males to teach abstinence in high school which is inconsistent with previous studies⁵,¹⁰. Yet, females were also more supportive to teach birth control in middle school, consistent with previous research documenting more support among females for both birth control and condoms being taught in middle schools¹⁰.
Consistent with previous research, younger respondents were more likely to support teaching HIV and STDs along with gender and sexual orientation¹³. Regarding race and ethnicity, blacks and Hispanics were more supportive of several topics across both middle school and high school in this study, similar to previous research documenting more support among blacks and Hispanics for HIV and STDs, gender and sexual orientation, and dealing with pressure¹⁰,¹³.
district in Florida, recent state practice in Florida is not reflective. This relatively new direction towards more abstinence education is coming from the state level government to include the Florida Department of Education. House Bill 1069, approved by the State Board of Education in Florida, became effective in July of 2023³. This bill now requires all materials used to teach reproductive health or any disease including HIV/AIDS to be approved by the Florida Department of Education.
Prior to this bill, local districts had the autonomy to determine and select materials to best meet the needs of their local community. With the movement towards a more abstinence focused approach, Florida schools are becoming very restricted and limited in actual topics they can include³. Specific topics being discouraged include gender, sexual orientation, and contraceptives, while more emphasis on abstinence is being promoted. There is an overall push to do less sexuality education, not more. This is concerning as it does not align with adolescent sexual behaviors, adolescent health needs, and the preference of the majority.
Even more alarming are the risks of moving towards abstinence-only sexual health education, also called sexual risk avoidance. This approach:
- presents abstinence as the only way to prevent pregnancy, STDs and HIV,
- presents failure rates of contraceptives and condoms, and
- teaches abstinence as the expected standard of behavior for teens, with some programs suggesting sex is only acceptable in heterosexual marriage³⁹.
Often, these programs shame or fail to address the lived experiences of young people⁴³,⁴⁴. A nine year congressionally mandated study followed four abstinence-only programs starting in 2007⁴⁵. These programs had no positive effect on the sexual behaviors of youth, who were no more likely to abstain from sex than teens not enrolled in abstinence only programs. Also, youth in these programs were also less likely to correctly report the effectiveness of condoms in preventing STDs⁴⁵.
Although proponents of abstinence only education suggest this method delays sexual initiation and leads to a reduction in teen pregnancy and STDs⁴⁶, no body of evidence supports these claims. Conversely, one study discovered higher rates of teen pregnancy and births in states with policy requiring schools stress abstinence when teaching sex education⁴⁷.
On the other hand, decades of research confirm that comprehensive sexuality education is most effective. Goldfarb and Lieberman (2021) completed an extensive systematic review of 80 articles spanning three decades of research to determine the impact of comprehensive sexuality education²⁸. They documented that this approach not only reduces teen pregnancy and STDs, but can also reduce relationship violence, prevent child sexual abuse, increase healthy relationships, create safer school spaces for LGBTQ youth, improve social-emotional learning, and increase media literacy.
Additional benefits included improved mental health, safety, and school success²⁸. Furthermore, the Future of Sex Education report concluded that using accurate language, such as that used in comprehensive sexuality education curriculum, increases the likelihood that a child will report abuse⁴⁰.
Strong community and professional support for reproductive and sexual health education is well documented, and sharing this data with school district leadership has shown to be effective in helping to change policy and practices⁴⁸. Another study found that demonstrating community support for offering sexual health services through School-based Health Clinics is important to successfully adding sexual health services to those clinics⁴⁹.
Moving forward, it is critical to continue to share data such as in this study to urge decision makers to make data driven decisions. By documenting the need for comprehensive sex education, the effectiveness of these programs, and the overall support for this type of education, policy makers will be equipped with information to make educated decisions to better support the needs of youth. Sharing this data can support and encourage others to collect and share local data as one effective strategy to improve related policy.
LIMITATIONS:
The study had several limitations. First, the sample is representative of the residents of this county, but results cannot be generalized to other counties, the state, or other states. Second, for questions regarding support for each of the eight topics being taught in middle school and high school, only brief descriptions were used to imply the content of the specific topics to be taught. The support for the nature and depth of each topic is still not known. Finally, only quantitative questions were used. Including qualitative questions would have added to the richness and depth of the results allowing participants to explain why or why not they support the specific topics and sexual health education in general.
Conclusion
Results from this study provide substantial support for reproductive and sexual health education at both the middle school and high school levels. Most participants overwhelmingly support a more comprehensive approach to school-based sexuality education to include instruction in abstinence, birth control, and safer sex methods.
Although the state of Florida has changed its policy to drastically reduce the amount of sexuality education in public schools, results from the study can be used to advocate for policy including more sexual health topics to better represent the beliefs of the majority and address the needs of youth.
Conflict of Interest:
The authors have no conflicts of interest to declare.
Funding Statement:
This research was supported by funding from the Centers for Disease Control and Prevention, Division of Adolescent Health, Promoting Adolescent Health through School-Based HIV Prevention: Jacksonville Partnership for Promoting the Health of Emerging Adults. (2018). NCHHSTP, PS18-1807.
Acknowledgements:
This study was conducted in collaboration with the University of North Florida Public Opinion Research Lab (PORL) under the direction of Dr. Michael Binder, PORL faculty director and UNF professor of political science.
References
1. Sexuality Information and Education Counsel of the United States (SIECUS). The SIECUS state profiles 2022. Published 2022. [online] Available: https://siecus.org/state-profiles-2022/.
2. Centers for Disease Control and Prevention (CDC). Division of adolescent and school health, school health profiles 2022: Explore school health profiles questions – Nationwide, 2022, health education. [online] Available: https://profiles-explorer.cdc.gov/. Updated 2024.
3. Florida Department of Education. 2023. Approval of Health Materials per House Bill 1069. 2023; 1003.42(1)(b). Available: https://info.fldoe.org/docushare/dsweb/Get/Document-9960/dps-2023-167.pdf
4. Planned Parenthood, What U.S. parents think about sex education in schools, Published 2023 [online] Available: https://cdn.plannedparenthood.org/uploads/filer_public/f8/d6/f8d6439d-dbf2-4205-b447-cc9f70815f82/parent_data_fact_sheet_english.pdf?_gl=1*gxr81y*_ga*MTQ4Mjk0ODM3MC4xNzMxMjY5Njkw*_ga_ENXC8KHJL8*MTczMTI2OTY5MC4xLjEuMTczMTI2OTcwNS4wLjAuOTY5MzkzMzEy
5. Howard-Barr E, Moore MJ, Weiss JA, Jobli E. Public opinion toward sexuality education: Findings among one south Florida county. Am J Sex Educ. 2011;6(2):176–191. doi:10.1080/15546 128.2011.571955.
6. American Public Health Association Policy Statement. Sexuality education as part of a comprehensive health education program in K to 12 schools – Policy number 20143. Published November 18, 2014. [online] Available: https://www.apha.org/policies-and-advocacy/public-health-policy-statements/policy-database/2015/01/23/09/37/sexuality-education-as-part-of-a-comprehensive-health-education-program-in-k-to-12-schools
7. Moore P. Poll results: Sex ed. Published January 7, 2015 [online] Available: https://today.yougov.com/health/articles/11294-poll-results-sex-ed.
8. Power to Decide. Survey says. Published 2017. [online] Available: https://powertodecide.org/sites/default/files/resources/primary-download/survey-says-may-2017.pdf
9. Jones RP, Cox D. How race and religion shape millennial attitudes on sexuality and reproductive health. Published March 27, 2015 [online] Available: https://www.prri.org/wp-content/uploads/2015/03/PRRI-Millennials-Web-FINAL.pdf
10. Barr EM, Moore MJ, Johnson T, Forrest J, Jordan M. New evidence: Data documenting parental support for earlier sexuality education. J School Health. 2014;84(1): 10–17. doi:10.1111/josh.12112.
11. Szucs LE, Harper CR, Andrzejewski J, Barrios LC, Robin L, Hunt P. Overwhelming support for sexual health education in U.S. schools: A meta-analysis of 23 surveys conducted between 2000 and 2016. J Adolescent Health. 2022;70(4):598–606. doi:10.1016/j.jadohealth.2021.05.016. Available: https://doi.org/10.1016/j.jadohealth.2021.05.016
12. Davis CJ, Cox D, Griffin R, Jones RP. Young People Set to Impact the Debate on Women’s Health Issues. Published April, 2018. [online] Available: https://www.prri.org/research/young-people-set-to-impact-the-debate-on-womens-health-issues/.
13. Barr E, Moore MJ, Wilson K, Parisi T, McCann H. Documenting support for ongoing and improved efforts in sexuality education. Florida Public Health Review. 2017;14: 45–55. https://scholars.unf.edu/ws/portalfiles/portal/40651347/Documenting%20Support%20for%20Ongoing%20and%20Improved%20Efforts%20in%20Sexuality.pdf
14. Kantor L, Levitz N. Parents’ views on sex education in schools: How much do Democrats and Republicans agree? PloS One. 2017;12(7): e0180250. doi:10.1371/journal.pone.0180250.
15. US Department of Health and Human Services, Office of Disease Prevention and Health Promotion, Healthy People 2030. Reduce pregnancies in adolescents – FP‑03. Published 2020. [online] Available: https://odphp.health.gov/healthypeople/objectives-and-data/browse-objectives/family-planning/reduce-pregnancies-adolescents-fp-03
16. World Association for Sexual Health (WAS). WAS statement on comprehensive sexuality education. Published July 26, 2023. [online] Available: https://www.worldsexualhealth.net/statement-on-comprehensive-sexuality-education
17. Centers for Disease Control and Prevention (CDC). 1991-2021 High school youth risk behavior survey data. [online] Available: http://nccd.cdc.gov/youthonline/. Accessed October 11, 2024.
18. Centers for Disease Control and Prevention (CDC). Sexually transmitted disease surveillance. Published 2021. [online] Available: https://www.cdc.gov/std/statistics/2022/2021-STD-Surveillance-Report-PDF_ARCHIVED-2-16-24.pdf
19. Centers for Disease Control and Prevention, (CDC). Sexually Transmitted Infections Surveillance 2022. [online] Available: https://www.cdc.gov/std/statistics/2022/default.htm. Updated 2024.
20. Centers for Disease Control and Prevention, (CDC). Estimated HIV incidence and prevalence in the United States, 2018–2022. HIV Surveillance Supplemental Report, 29(1). Published May 21, 2024. https://www.cdc.gov/hiv-data/nhss/estimated-hiv-incidence-and-prevalence.html
21. Florida Department of Health. 2022. State HIV slide set: State of Epidemic, 2022. [online] Available: https://www.floridahealth.gov/diseases-and-conditions/aids/surveillance/epi-slide-sets.html
22. Power to Decide (formerly The National Campaign to Prevent Teen and Unplanned Pregnancy). Fast facts: Teen pregnancy in the United States. Published April 2016. [online] Available: https://powertodecide.org/sites/default/files/resources/primary-download/fast-facts-teen-pregnancy-us.pdf
23. Centers for Disease Control and Prevention (CDC). About teen pregnancy. Published May 14, 2024. [online] Available: https://www.cdc.gov/reproductive-health/teen-pregnancy/.
24. Hendrick CE, Maslowsky J. 2019. Teen mothers’ educational attainment and their children’s risk for teenage childbearing. Dev Psychol. 2019;55(6):125 9–1273. doi:10.1037/dev0000705.
25. Osterman MJK, Hamilton BE, Martin JA, Driscoll AK, Valenzuela CP. Births: Final data for 2021. National Vital Statistics Reports. 2023;72(1). doi: https://dx.doi.org/10.15620/cdc:122047
26. Sedgh G, Finer LB, Bankole A, Eilers MA, Singh S. Adolescent pregnancy, birth, and abortion rates across countries: levels and recent trends. J Adolesc Health. 2015;56(2):223 – 230. doi:10.101 6/j.jadohealth.2014.09.007. Available: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4852976/
27. Kirby D. 2007. Emerging answers 2007: Research findings on programs to reduce teen pregnancy and sexually transmitted diseases. Washington DC: The National Campaign to Prevent Teen Pregnancy.
28. Goldfarb ES, Lieberman LD. Three decades of research: The case for comprehensive sex education. J Adolescent Health. 2021;68(1):13–27. doi:10.1016/j.jadohealth.2020.07.036.
29. Eisenberg ME, Bernat DH, Bearinger LH, Resnick MD. Condom provision and education in Minnesota public schools: A telephone survey of parents. J School Health. 2009;79(9): 416–424. doi:10.1111/j.1746-1561.2009.00429.x.
30. Ito KE, Gizlice Z, Owen-O’Dowd J, Foust E, Leone PA, Miller WC. Parent opinion of sexuality education in a state with mandated abstinence education: Does policy match parental preference? J Adolescent Health. 2006;39(5):634–641. doi:10. 1016/j.jadohealth.2006.04.022.
31. National Public Radio, Kaiser Family Foundation, Kennedy School of Government. 2004. Sex education in America general public/ parents survey. The Henry J.Kaiser Family Foundation. Published January 2004. [online] Available: https://www.kff.org/wp-content/uploads/2013/01/sex-education-in-america-general-public-parents-survey-toplines.pdf
32. Yarber WL, Milhausen RR, Crosby RA, Torabi MR. Public opinion about condoms for HIV and STD prevention: A midwestern state telephone survey. Perspect Sex Repro H. 2005;37(3):148–154. doi:10.1363/3714805.
33. Future of Sex Education Initiative. National sexuality education standards: Core content and skills, K-12. J School Health. 2012;43(1). https://healtheducationresources.unesco.org/sites/default/files/resources/ssr_tpg_1_sexualityeducationstandards.pdf
34. Kantor L, Levitz N, Holstrom A. Support for sex education and teenage pregnancy prevention programmes in the USA: Results from a national survey of likely voters. Sex Education. 2020;20(3): 239–251.https://doi.org/10.1080/14681811.2019.1652807
35. Kershner SH, Corwin S, Prince M, Robillard A, Oldendick R. Support for comprehensive sexuality education and adolescent access to condoms and contraception in South Carolina. Am J of Sexuality Education. 2017;12(3): 297-314. doi:10.1080/1554 6128.2017.1359803.
36. American Medical Association. AMA adopt new public health policies to improve health donation. Published June 15, 2018. [online] Available: https://www.ama-assn.org/press-center/press-releases/ama-adopts-new-public-health-policies-improve-health-nation-1
37. Breuner, CC, Mattson, G. American Academy of Pediatrics, Committee on Adolescence, Committee on psychosocial aspects of child in the family health. Sexuality Education for Children and Adolescents. Pediatrics. 2016;138(2):e20161348
38. World Health Organization, comprehensive sexuality education, May 18, 2023, Available: https://www.who.int/news-room/questions-and-answers/item/comprehensive-sexuality-education
39. Kaiser Family Foundation. Women’s Health Policy: abstinence education programs: definitions, funding, and impact on teen sexual behavior. Published June 1, 2018 [online] Available: https://files.kff.org/attachment/Fact-Sheet-Abstinence-Education-Programs-Definition-Funding-and-Impact-on-Teen-Sexual-Behavior
40. Future of Sex Education. 2020. National sex education standards core content and skills, K-12. 2nd ed. Available: https://advocatesforyouth.org/wp-content/uploads/2020/03/NSES-2020-web.pdf
41. Centers for Disease Control and Prevention (CDC). HIV testing and youth. [online] Available: https://www.cdc.gov/healthyyouth/youth_hiv/hiv-information-and-youth.htm. Updated 2024
42. The Trevor Project. 2023 US national survey the mental health of the LGBTQ young people. Available:https://www.thetrevorproject.org/survey-2023/
43. Chin, H, et al. Community Preventive Services Task Force. The effectiveness of group-based comprehensive risk-reduction and abstinence education interventions to prevent or reduce the risk of adolescent pregnancy, human immunodeficiency virus, and sexually transmitted infections: Two systematic reviews for the guide to community preventive services. Am J of Preventive Medicine. 2012;42(3):272-94
44. Santelli JS, et al. Guttmacher Institute. Abstinence-only-until-marriage: An updated review of U.S. policies and programs and their impact. J of Adolescent Health, 2017;61: 273e280. [online]Available:https://www.jahonline.org/article/S1054-139X(17)30260-4/pdf
45. Trenholm C, Devaney B, Fortson K, Quay L, Wheeler J, Clark M. Impacts of Four Title V, Section 510 Abstinence Education Programs. Mathematica Policy Research, Inc. 2007. Published April 12, 2007. [online] Available: https://aspe.hhs.gov/reports/impacts-four-title-v-section-510-abstinence-education-programs-1
46. Heritage Foundation (2010). Evidence on the Effectiveness of Abstinence Education: An Update. Available:https://www.heritage.org/education/report/evidence-the-effectiveness-abstinence-education-update
47. Stanger-Hall KF, Hall DW. Abstinence-only education and teen pregnancy rates: Why we need comprehensive sex education in the U.S. PLoS One, 2011;6(10): e24658 doi: 10.1371/journal. pone.0024658
48. Plastino K, Quinlan J, Todd J, Tevendale HD. Stakeholder education and community mobilization garner support for sex education. J Adolesc Health. 2017;60(3S):S24-S29. doi: 10.1016/j.jado health.2016.09.028. available: https://pubmed.ncbi.nlm.nih.gov/28235431/
49. Moore MJ, Barr E, Wilson K, Griner S. Support for offering sexual health services through school based health clinics. J of School Health. 2016;86(9): 660-668.