

Computerized Insulin Dose Adjustment for Diabetes Care
Review of Comprehensive Computerized Insulin Dose Adjustment Algorithms: a Technology to Aid Primary Care Clinicians
Mayer B. Davidson, MD1, S. Joshua Davidson, AB2
- Mellitus Health, Inc; Beverly Hills, California; Charles R. Drew University; Los Angeles, California
- Mellitus Health, Inc; Beverly Hills, California
OPEN ACCESS
PUBLISHED: 31 October 2025
CITATION: Davidson, M.B. and Davidson, S.J., 2025. Review of Comprehensive Computerized Insulin Dose Adjustment Algorithms: a Technology to Aid Primary Care Clinicians. Medical Research Archives, [online] 13(10). https://doi.org/10.18103/mra.v13i10.7008
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI: https://doi.org/10.18103/mra.v13i10.7008
ISSN 2375-1924
ABSTRACT
Background – Primary care clinicians, who take care of 90% of people with diabetes, are challenged managing patients taking insulin. Insulin-requiring patients remain poorly controlled, especially those on intensive insulin regimens. The senior author developed and taught detailed treatment protocols to 50 non-physician primary care clinicians so that they could independently manage patients with diabetes. The principles of adjusting insulin doses were computerized and subsequently cleared by the Federal Drug Administration and registered by the Confirmite Europeene.
Aims to evaluate the effectiveness and safety of these comprehensive computerized insulin dose adjustment algorithms (called Insulin Insights).
Methods Insulin Insights interacts with over 60 glucose meters as well as continuous glucose monitors, handles all approved insulins and analyzes 11 different insulin regimens. Insulin Insights algorithms that are located in electronic health records or office computers generate reports within 1-2 minutes after glucose readings are downloaded. Algorithms located on a secure, approved icloud source for remote monitoring send reports at agreed upon time intervals to primary care clinicians. The generated report includes a scatterplot of glucose readings, the values organized into before and after each meal and before bedtime, an analysis of the glucose patterns that are presented in bar graphs and recommendations for dose adjustments (if necessary) that can be accepted or modified. The new doses serve as the basis for the next report.
Results – There were 104 patients in formal studies (2 pre- post and 2 randomized control trials) evaluating the response to Insulin Insights in which changes in scheduled measured HbA1c levels were the primary outcome. Baseline HbA1c levels fell 1.8% from 9.8% to 8.0% over 4.7 months. Another 161 patients were followed in real world situations. Since HbA1c tests were not at scheduled intervals, estimated HbA1c levels based on average glucoses were analyzed in all 265 patients and also showed a significant decrease. There was no increase in hypoglycemia attesting to the safety of Insulin Insights.
Conclusion Insulin Insights, utilized by primary care clinicians, enabled them to significantly improve glycemic control. They also educate the primary care clinicians and save them time.
Keywords
Insulin, diabetes, computerized algorithms, primary care, glycemic control
Background
Ninety percent of patients with diabetes are cared for by primary care clinicians (PCCs), 25-30% of whom take insulin. Unfortunately, primary care clinicians are challenged in managing patients requiring insulin. For example, there was a 3-7 year delay in starting insulin in patients with HbA1c levels >8.0% after failing non-insulin drugs. In the United States, the mean level of HbA1c when insulin was initiated was 9.3%. After failing basal insulin alone, the mean HbA1c level was 9.7% when patients were prescribed an intensive insulin regimen (2 different types of insulin injected 2 or more times per day). Insulin intensification occurred in only 25-30% of patients and was discontinued in a similar number. Major challenges for primary care clinicians in managing patients on insulin, especially those on intensive insulin regimens, are time constraints and lack of experience.
This situation has resulted in many insulin-requiring patients remaining in poor glycemic control. HbA1c levels in patients receiving insulin have remained the same, at least in the United States, over the past 30 years. The percent meeting the American Diabetes Association’s target of <7.0% was 40% with 15-20% experiencing severe hyperglycemia defined as a HbA1c level exceeding 10%. This has occurred in spite of the development of insulin analogues with even more rapid pharmacokinetic/pharmacodynamic characteristics in an attempt to more closely mirror the pattern of endogenous insulin secretion. In a review of 26 randomized control trials involving over 9,500 participants, the mean difference in HbA1c levels between rapid-acting insulin analogues and regular insulin users was only 0.05% with no difference in hypoglycemia. Furthermore, in comparisons of rapid-acting with ultra-rapid-acting insulins in randomized control trials, there were no significant differences in changes of HbA1c levels between insulin aspart vs faster-acting insulin aspart, insulin lispro vs ultrarapid-acting insulin lispro, or insulin aspart vs inhaled Technosphere insulin. Thus, these small (but statistically significant) decreases in post-prandial glucoses after ultrarapid-acting bolus insulins are very unlikely to make any clinical difference. This shifts the responsibility of achieving near euglycemia in patients using intensive insulin regimens to clinicians who manage their insulin doses.
The senior author has developed detailed diabetes treatment protocols and taught them to approximately 50 registered nurses, nurse practitioners, physician assistants and clinical pharmacists involved in primary care so that they could independently manage their patients with diabetes. Adjusting insulin doses for all types of available insulins and their combinations was part of the protocols. After being trained, a registered nurse hired by Los Angeles County was placed in a Family Medicine Clinic where the physicians referred their poorly controlled patients to her. She was allowed to use the officially approved treatment protocols with their rules for adjusting insulin doses. After some initial hesitation, the physicians realized that she was more experienced in diabetes management than they were and simply turned over their poorly controlled patients to her. The senior author was not involved in supervising her diabetes care. Over the course of several years, she managed 151 insulin-requiring patients. Only NPH and regular insulins were available at the clinic at that time. Ten percent of these poorly controlled patients ended up on bedtime NPH insulin alone, 87% on self-mixed/split NPH/regular insulin and 3% on premixed NPH/regular insulin. Their baseline HbA1c levels fell from 11.0% to 7.2% over 9-12 months of in-person clinic visits. A more recent study of the effectiveness of the (non-computerized) insulin dose adjustment algorithms involved primary care nurse practitioners specially trained in diabetes care by the senior author at the Venice Family Clinic. They spend 30% of their time managing routinely referred, poorly controlled (HbA1c level 9.0%) patients with diabetes. The clinic is a Federally Qualified Health Center serving a similar population as the county Family Medicine Clinic. In 149 patients receiving insulin in an intensive regimen requiring bolus insulin doses, baseline HbA1c levels fell from 10.3% to 7.1% within a year of telephonic and in-person visits.
Methods
Based on the results of the first study, the insulin dose adjustment algorithms (called Insulin Insights) were computerized to aid primary care clinicians to manage insulin-requiring patients. The algorithms are based on the following three principles:
- Depending on when injected, each component of the insulin regimen has a maximal effect on a specific period of the 24 hour cycle, e.g., overnight, morning, afternoon, evening.
- The glucose pattern in that period determines whether the dose of that component of the insulin regimen requires adjusting or not.
- There needs to be enough glucose readings in a period to reflect the patient’s current lifestyle for a decision to be made about that component of the insulin regimen that maximally affects that period.
The third principle is important to observe. Many patients will measure their glucose levels only when they feel hyper- or hypoglycemic. These values do not represent their usual lifestyle and dosing decisions made on these readings can be inappropriate and sometimes dangerous.
The characteristics of Insulin Insights are summarized in Table 1. They are cleared by the Federal Drug Administration for use in the United States and registered by the Confirmite Europeene in Europe. By virtue of the latter, Insulin Insights can be used almost anywhere else in the world. The algorithms can handle all of the available types of insulins including the recently approved premixed insulin (Ryzodeg) that combines a basal insulin and a rapid-acting insulin analogue. Finally, all eleven of the commonly used insulin regimens, including the more unusual delayed responses to NPH and U-500 regular insulins, can be analyzed by Insulin Insights.
The following information is needed to register a patient into Insulin Insights:
- De-identified code
- Height
- Weight
- Sex
- Year of birth
- Insulin regimen insulin type, times of injections, doses of each
- Approximate times of meals and bedtime (usually 2-hour ranges)
- Clinician-selected high/low pre- and post-prandial glucose targets
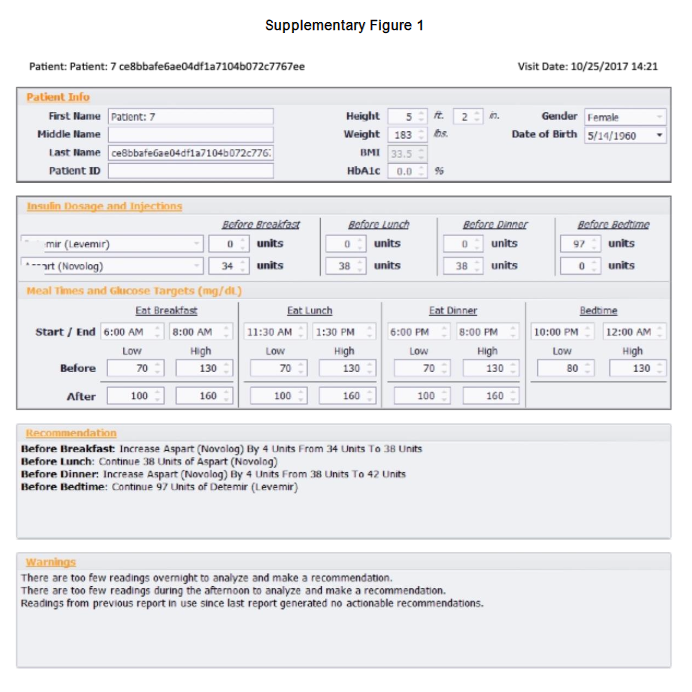
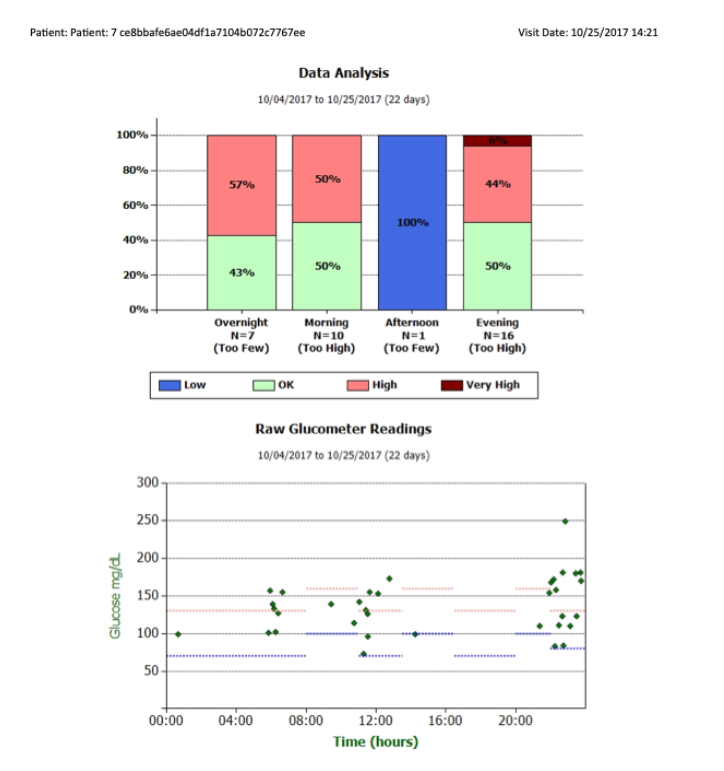
No further administrative inputs are necessary during patient management. A code is assigned to the patient which is used on all reports rather than the name. If Insulin Insights algorithms are located in an electronic health record or an office computer, the report is generated within 1-2 minutes after downloading the glucose readings from either meters or continuous glucose monitors. If the algorithms are located on a secure approved icloud source that remotely receive the measured glucose readings, reports are generated and routinely sent to primary care clinicians at intervals determined by them or the medical care system in which they work. The generated report includes a scatterplot of all glucose readings, the glucose values organized into before and after each meal and before bedtime, an analysis of the glucose patterns that are presented in bar graphs and recommendations for insulin dose adjustments (if necessary) that primary care clinicians can accept or modify (see supplementary Figure 1). Once the clinical decision by the primary care clinician for the new doses is made by simply pressing a button, these serve as the basis for the subsequent report.
Table 1 Characteristics of the Computerized Insulin Dose Adjustment Algorithms
FDA cleared (U.S.) and CE registered (European Union)
Interacts with over 60 glucose meters and CGMs
Handles all types of insulins
Short-acting (regular) insulin
All rapid-acting analogue insulins
Intermediate-acting (NPH) insulin
All basal insulins
All premixed insulins
U-500 regular insulin
Analyzes 11 insulin regimens
Basal alone
Bedtime NPH alone
Basal/Bolus (1, 2 or 3 bolus doses)
Self-mixed/split human insulins
Self-mixed/split analogue insulins
Premixed human insulins
Premixed analogue insulins
Premixed basal/rapid-acting insulin*
U-500 Regular insulin
Delayed response to NPH insulin
Delayed response to U-500 regular insulin
CE – Conformité Européene; CGM – continuous glucose monitor; FDA – Federal Drug Administration; *Ryzodeg – degludec/aspart
Pre- Post Studies of Insulin Insights
The results of the pre- post studies that have evaluated the effectiveness of Insulin Insights are presented in Table 2. In the first study, a primary care nurse practitioner, specially trained in diabetes care, spent 50% of her time independently managing routinely referred patients taking insulin with HbA1c levels 9.0%. After the initial education session to teach patients how to measure their glucoses on the meter that would send the readings to a secure approved icloud, all further interactions with the patient occurred telephonically. The marked preponderance of type 2 diabetes reflected the minority population served in this clinic. The nurse practitioner utilizing Insulin Insights significantly lowered HbA1c levels. Only 17 of the 28 patients completed the 6-month study. It is common for the Los Angeles Latino population to visit their families in Mexico over the Christmas/New Year holidays and remain there for relatively long periods. If they were there for more than a month, they had to be discontinued from the study. Before she had used Insulin Insights, the nurse practitioner spent about 10 minutes obtaining, organizing and analyzing the glucose readings and making her clinical decisions regarding any dose changes. With Insulin Insights, the time was reduced to about 3 minutes.
In the second study carried out in another clinic, a clinical pharmacist, who was experienced in providing diabetes care, was also routinely referred patients with HbA1c levels 9.0%. The insulin-requiring patients there used fingerstick blood glucose meters. The pharmacy purchased 13 Free Style Libre Pro continuous glucose monitors to test them which were offered to the first 13 patients who were interested in using them. The population was similar to the first study. Unfortunately, the clinic terminated the pharmacist-directed diabetes program relatively soon after the study was started. However, in the average follow up of 3.2 months, time in range >250 mg/dl markedly fell, time in range 70-180 mg/dl markedly increased and there was a decrease of 3.2% in HbA1c levels in these very poorly controlled patients. There was no increase in hypoglycemia.
Table 2 Pre-Post Studies of the Effectiveness of Insulin Insights
Study #1 – Davidson²⁸; Clinician – NP; Number of patients – 28
Inclusion Criteria – Insulin-requiring >6 months and HbA1c level ≥8.0%
Population – low SES containing majority of minorities
Race/Ethnicity – Latino – 20; Black – 4; White – 3; Asian – 1
Types of Diabetes – Type 1 – 1; Type 2 – 27
Glucose monitoring – Self monitoring of blood glucose with results sent remotely
Insulin Regimens – Basal alone – 11; basal/bolus – 14; self-mixed/split (NPH/reg) – 3
HbA1c Levels – Baseline – 10.0%; 3-months – 8.1%; 6-months – 7.6%; P <0.001*
Total Daily Dose of Insulin – increased by 24%
Study #2 – Davidson²⁹; Clinician – Pharmacist; Number of patients – 13
Inclusion Criteria – HbA1c level ≥9.0% and agreement to use CGM
Population – low SES containing majority of minorities
Types of Diabetes – Type 1 – 1; Type 2 – 12
Glucose monitoring – CGM results of glucose readings presented at in person visits
Insulin Regimens – Basal alone – 10; basal/bolus – 3
HbA1c Levels – Baseline – 11.5%; mean follow up – 3.2-months – 8.3%; P <0.001*
TIR >250 mg/dl – Baseline – 44%; 3.2 months – 23%; P <0.01*
TIR 181-250 mg/dl – Baseline – 26%; 3.2 months – 24%; P = 0.58*
TIR 70-180 mg/dl – Baseline – 29%; 3.2 months – 51%; P = 0.01*
TIR 55-69 mg/dl – Baseline – 0.5%; 3.2 months – 1.6%; P = 0.15*
TIR <55 mg/dl – Baseline – 0.2%; 3.2 months – 0.6%; P = 0.32*
Total Daily Dose of Insulin – increased by 42%
Randomized Control Trials of Insulin Insights
The results of these trials that have evaluated the effectiveness of Insulin Insights are presented in Table 3. In the first randomized study, after the initial education session to teach patients how to measure their glucoses on the meter that would send the readings to the secure approved icloud, all further interactions with the patient occurred telephonically similar to the first pre- post study.
The proportional similarity of the insulin regimens among the 3 cohorts means that the significant decrease in HbA1c levels in the Insulin Insights group cannot be due to differences in their insulin regimens. In the remote patient monitoring program, glucose readings >200 and <70 mg/dl are automatically sent to health educators who contact the patient and discuss lifestyle changes to avoid future episodes. Pharmaceutical changes were not made. The identical HbA1c level responses in the two Usual Care groups indicate that remote patient monitoring did not improve glycemic control. The difference in the number of alerts <70 mg/dl in the 2 remote patient monitoring groups were non-significant attesting to the safety of Insulin Insights. Remote patient monitoring was helpful in preventing episodes of severe hypoglycemia which mirror the results of another study in which remote patient monitoring also did not improve glycemic control but was beneficial for mitigating hypoglycemia. Lowering glycemia requires ongoing insulin dose adjustments by experienced clinicians.
The second randomized study took place in rural Australia where a few endocrinologists serve large geographic areas making in person visits to them very difficult when referred by their primary care clinicians. The insulin-requiring patients randomized to the Insulin Insight group were given meters allowing their glucose readings to be sent to a central Australian server with subsequent transfer to Insulin Insights for the first 2 months before returning the patient to usual care by their primary care clinician at 3 months. Reports were sent weekly to the endocrinologist who messaged the patient to ascertain that the prescribed insulin doses were being taken correctly. If so, the endocrinologist reviewed the recommendations, accepted or modified them and sent the dose changes (if necessary) directly to the patient without further contact with them. HbA1c levels were no different at baseline between the Insulin Insight and Usual Care groups but had significantly fallen by 1.2% at 3 months compared with 0.2% in the control group. At 6 months, the HbA1c level (% ±SD) in the Insulin Insight group had increased to 8.5 ± 1.5 demonstrating that ongoing algorithmic dose adjustments were necessary to maintain or continue to improve glycemic control and prevent regression.
There were 104 patients in the formal studies evaluating the response to Insulin Insights in which changes in scheduled measured HbA1c levels were the primary outcome. The weighted average of the results showed that baseline HbA1c levels fell 1.8% from 9.8% to 8.0% over a mean of 4.7 months.
Table 3 – Randomized Control Trials of the Effectiveness of Insulin Insights
Study #1 – Pulicharam³⁰; Clinicians – 2 physicians, 1 physician assistant
Inclusion criteria – Insulin-requiring >6 months and HbA1c level ≥8.0%
Population – Medicare Advantage (age ≥65 years with private Medicare plan)
| Cohorts | Insulin Insights + RPM | RPM + Usual Care | Usual Care Alone |
|---|---|---|---|
| Groups | A | B | C |
| Number of patients | 40 | 42 | 33 |
| Baseline HbA1c (% ± SD) | 9.5 ± 1.3 | 9.2 ± 8.5 | 9.0 ± 0.9 |
| Six Month HbA1c (% ± SD) | 8.0 ± 1.0 | 8.5 ± 1.6 | 8.3 ± 0.9 |
| HbA1c Change (% ± SD)† | -1.5 ± 1.0 | -0.7 ± 1.5 | -0.7 ± 1.2 |
| Outcomes | A | B | C |
|---|---|---|---|
| All Alerts (N)‡ | 1177 | 1320 | NA |
| Alerts >200 mg/dl (N)§ | 942 | 1111 | NA |
| Alerts <70 mg/dl (N)! | 235 | 209 | NA |
| Emergency Department Visits (N) | 0 | 0 | 6 |
| Basal/Bedtime NPH Insulin Alone (N) | 18 | 18 | 17 |
| Basal/Bolus Insulin (N) | 15 | 18 | 11 |
Premixed Insulin (N) – 0 | 3 | 1
U-500 Regular Insulin (N) – 1 | 1 | 0
Lispro Insulin Only (N) – 0 | 1 | 0
Total Daily Dose of Insulin increased by 40%
Study #2 Menon³²; Clinicians; Endocrinologists without personal patient contact
Inclusion criteria – Insulin-requiring >6 months and HbA1c level ≥8.0%
Population – Patients living in rural Australia
| Cohorts | Insulin Insights | Usual Care | P value |
|---|---|---|---|
| Number of patients | 23 | 24 | |
| Baseline HbA1c (% ± SD) | 9.2 ± 1.3 | 9.3 ± 1.4 | 0.60 |
| Three Month HbA1c (% ± SD) | 8.0 ± 1.2 | 9.1 ± 1.3 | 0.001 |
Real World Experience with Insulin Insights
In addition to the 104 patients in the formal studies, primary care clinicians utilized Insulin Insights under real world situations in 138 patients using blood glucose meters and in 23 patients using continuous glucose monitoring. The primary care clinicians ordered their HbA1c levels at various times, the results of which were not available to the authors. Therefore, to be able to assess the effect of Insulin Insights, estimated HbA1c levels were calculated from the average glucose concentrations in their reports. The initial estimated HbA1c levels in these 265 patients fell from 8.3% to 7.6% over 6.4 months. Because the relationship between average glucose concentrations and estimated HbA1c levels are based on either 7 blood glucose meter readings including both pre- and post-prandial values or continuous glucose monitoring, and 242 of these 265 patients mostly measured pre-prandial glucoses, these estimated HbA1c levels were lower than measured ones would be. Thus, these patients were more poorly controlled than reflected by these estimated HbA1c levels. However, since the absolute decrease in HbA1c levels is proportional to baseline values, the fall from a higher baseline HbA1c level would also be greater than 0.7% supporting the effectiveness of Insulin Insights.
Identification of Over Prescribed Insulin Doses
When changes in the total daily dose of insulin were calculated in the 3 formal studies that utilized Insulin Insights throughout the entire study, the analysis showed that 19 of the 81 patients (23%) had either no change or a decrease in their total daily dose of insulin. Comparing these patients with those whose total daily doses of insulin increased revealed that baseline HbA1c levels were similar (10.0% vs 9.9%) and changes in HbA1c levels were actually non-significantly greater in those without an increase in their total daily dose (-2.2% vs -1.9%). It is common for patients given insulin not to take their prescribed doses. When not taken as prescribed, primary care clinicians, noting the hyperglycemia, would continue to raise insulin doses. Patients do not usually divulge their insulin nonadherence so as not to disappoint those managing their insulin doses. The more frequent interactions between patients and primary care clinicians that combined remotely monitored glucose readings with resultant recommendations by Insulin Insights were probably an important reason for the improvement in glycemia without an increase in total daily doses of insulin. Under the more infrequent interactions with usual care, only one-third of insulin-requiring patients achieved the American Diabetes Association’s target HbA1c level of <7.0%. However, 88% achieved that target when their insulin dose adjustments were supervised by endocrinologists every 1-4 weeks. Thus, Insulin Insights, in its role as the endocrinologist, gave primary care clinicians the opportunity to recognize insulin nonadherence, adjust doses appropriately and significantly improve glycemia.
Hypoglycemia and Therapeutic Inertia for Insulin Intensification
When surveyed, most physicians (88%) agreed that insulin-treated patients have inadequate control of glycemia and 76% stated that they would have treated more aggressively if not for concern about hypoglycemia. However, hypoglycemia is extremely common in patients taking insulin. In those using blood glucose meters or continuous glucose monitoring to measure glucoses, hypoglycemic episodes occurred in >80% and >90%, respectively. Patients with type 1 and insulin-treated type 2 diabetes experienced 6.7 and 2.1 episodes of hypoglycemia per week, respectively. These are usually due to behavioral issues, not inappropriately prescribed insulin doses. Gavin and colleagues have reviewed the literature on therapeutic inertia and delays in insulin intensification and concluded that the delay is largely driven by concerns over hypoglycemia.
The results of a pre- post study evaluating Insulin Insights in a Southern California Permanente endocrinology clinic would seem to support the conclusion of Gavin and colleagues. Twenty-eight patients were followed for a mean of 5.2 months at which time the endocrinologist suddenly terminated the study without explanation. There was a mean of 5 reports per patient with recommendations to increase the total daily dose of insulin by 9 units on average per report. In contrast, total daily doses of insulin were decreased from 112 to 98 units (12.5%). In spite of multiple attempts to receive an explanation for the termination of the study and the measured HbA1c values, neither were forthcoming. This necessitated calculating estimated HbA1c levels which showed an increase of 0.4% (probably less than measured HbA1c changes would have been as glucose tests were mostly pre-prandial). Hypoglycemic values did not change, being 7% and 6% of all glucose readings in the initial and final reports, respectively. These results show that Insulin Insights does not respond inappropriately to sporadic low glucose values (as did the Kaiser clinicians) but only appropriately if more consistent hypoglycemic patterns are seen.
Conclusions
Primary care clinicians, who take care of 90% of people with diabetes, are challenged in managing patients receiving insulin. Two important factors underlying this difficulty are time constraints and inexperience for some, both of which are mitigated by Insulin Insights. Use of these comprehensive computerized insulin dose adjustment algorithms helps primary care clinicians to safely adjust insulin doses appropriately and significantly improve glycemic control. By saving time, it also enables primary care clinicians to address more non-insulin issues at a visit and/or to see more patients. Other additional benefits include; a) education of primary care clinicians as they match glucose patterns and ongoing recommendations for insulin dose adjustments, b) decreased complications of diabetes, especially the microvascular ones, c) subsequent decreases in costs for both the medical care system and patients, and d) for medical care systems and primary care clinicians who bill for telephonic interactions, the generated reports provide documentation for the visit saving them or their office staffs even more time.
Acknowledgments
The authors are employees of Mellitus Health. There was no outside funding for this review.
Patient: Patient: 7 ce8bbafe6ae04df1a7104b072c7767ee
Visit Date: 10/25/2017 14:21
10/17/2017 10:01 PM 168 mg/dL
10/19/2017 10:10 PM 172 mg/dL
10/21/2017 11:07 PM 110 mg/dL
10/22/2017 10:14 PM 83 mg/dL
10/24/2017 11:26 PM 180 mg/dl
Legend to Supplementary Figure – Report in patient receiving basal insulin alone. The high and low pre-and post-prandial and before bedtime glucose targets are shown in the scatterplot as horizontal broken lines. This report shows that Insulin Insights will recommend initiation of bolus doses of insulin if the appropriate glucose pattern is not at target. In this case, the evening glucose pattern was very high generating the recommendation to start a bolus dose of insulin before dinner but the number of glucose tests during the morning and afternoon periods were too few for the algorithms to make recommendations.
References
- Davidson JA. The increasing role of primary physicians in caring for patients with type 2 diabetes mellitus. Mayo Clin Proc 2010;85(Suppl 12) S3-S4.
- Calvert MJ, McManis RJ, Freemantle N. Management of type 2 diabetes with multiple oral hyperglycaemic agents or insulin in primary care retrospective cohort study. Br J Gen Pract 2007;57: 455-460.
- Harris SB, Kapor J, Lank CN, Willan AR, Houston T. Clinical inertia in patients with T2DM requiring insulin in family practice. Can Fam Physician 2010;6: e418-e424.
- Home P, Naggar NE, Khamseh M, Gonzalez-Galvez G, Shen C, Chakkarwar P, et al. An observational non-interventional study of people with diabetes beginning or changed to insulin analogue therapy in non-Western countries: the A1chieve study. Diabetes Res Clin Pract 2011;94: 352-363.
- Mata-Cases M, Franch-Nadal J, Real J, Gratacos M, Lopez-Simarro F, Khunti K, et al. Therapeutic inertia in patients treated with two or more antidiabetics in primary care: factors predicting intensification of treatment. Diabetes Obes Metab 2018;20:103-112.
- Kostev K, Rathmann W. Changes in time to insulin initiation in type 2 diabetes patients: a retrospective database analysis in Germany and UK (2005-2010). Prim Care Diabetes 2013;7:229-233.
- Jeavons D, Hungin APS, Cornford CS. Patients with poorly controlled diabetes in primary care: healthcare clinicians beliefs and attitudes. Postgrad Med J 2006;82:347-350.
- Meece J. Dispelling myths and removing barriers about insulin in type 2 diabetes. Diabetes Educ 2006;32:1342-1349.
- Cuddihy RM, Philis-Tsimikas A, Nazeri A. Type 2 diabetes care and insulin intensification: is a more multidisciplinary approach needed? Results from the MODIFY Survey. Diabetes Educ 2011;37:111-123.
- Patrick AR, Fischer MA, Choudry NK, Shrank WH, Seeger JD, Liu J, et al. Trends in insulin initiation and treatment intensification among patients with type 2 diabetes. J. Gen Intern Med 2013;29:320-327.
- Khunti K, Nikolajsen A, Thorsted BL, Andersen M, Davies MJ, Paul SK. Clinical inertia with regard to intensifying therapy in people with type 2 diabetes treated with basal insulin. Diabetes Obes Metab 2016; 18:401-409.
- Ascher-Svanum H, Lage M, Perez-Nieves M, Reaney MD, Lorraine J, Rodriquez A. Early discontinuation and restart of insulin in the treatment of type 2 diabetes mellitus. Diabetes Ther 2014;5:225-242.
- Bonafede M, Chandran A, DiMano S, Saltiel-Berzin R, Saliu D. Medication usage, treatment intensification, and medical cost in patients with type 2 diabetes: a retrospective database study. BMJ Open Diabetes Research and Care 2016:4e000189. doi:10.1136/bmjdrc-2015-00189.
- Andreozzi F, Candido R, Corrao S, Forengo R, Giancaterini A, Ponzani P, et al. Clinical inertia is the enemy of therapeutic success in the management of diabetes and its complications: a narrative literature review. Diabetol Metab Syndr 2020;12:52.
- Venkatraman S, Echouffo-Tcheugui J, Selvin E, Fang M. Trends and disparities in glycemic control and severe hyperglycemia among US adults with diabetes using insulin, 1988-2020 JAMA Netw Open, 2022. 5(12): p. e2247656.
- Davidson MB. Insulin analogues: is there a compelling case to use them? No! Diabetes Care 2014;37:1771-1774.
- Bowering K, Case C, Harvey J, Reeves M, Sampson M. Strzinek R, et al. Faster aspart versus insulin aspart as part of a basal-bolus regimen in inadequately controlled type 2 diabetes: the onset 2 Trial. Diabetes Care 2017;40:951-957.
- Russell-Jones D, Bode BW, De Block C, Franek C, Heller SR, Monthieu C, et al. Fast-acting insulin aspart improves glycemic control in basal-bolus treatment for type 1 diabetes: results of a 26-week multicenter, active-controlled, treat-to-target, randomized, parallel-group trial (onset 1). Diabetes Care 2017:40:943-950.
- Bode BW, Iotova V, Kovarenko M, Laffel LM, Rao PV, Deenadayalan S, et al. Efficacy and safety of fast-acting insulin aspart compared with insulin aspart, both in combination with insulin degludec, in children and adolescents with type 1 diabetes: the onset 7 Trial. Diabetes Care 2019;42:1255-1262.
- Bowering K, Harvey J, Kolaczynski JW, Snyder JW, Bode BW. A randomized trial evaluating the efficacy and safety of fast-acting insulin aspart compared with insulin aspart, both in combination with or without metformin, in adults with type 2 diabetes (ONSET 9). Diabetic Med 2019;36:771-775.
- Lane WS, Favaro E, Rathor N, Jang HC, Kjaersgaard MIS, Oviedo A, et al. A randomized trial evaluating the efficacy and safety of fast-acting insulin aspart compared with insulin aspart, both in combination with insulin inulin degludec with or without metformin, in adults with type 2 diabetes (ONSET 9). Diabetes Care 2020;43:1710-1716.
- Lee MH, Paldus B, Vogrin S, Morrison D, Zaharieva DP, Lu J, et al. Fast-acting insulin-aspart versus insulin aspart using a second-generation hybrid closed-loop system in adults with type 1 diabetes: a randomized, open-label, crossover trial. Diabetes Care 2021;44:2371-2378.
- Blevins T, Zhang Q, Frias J, Jinnouchi, H, Chang A, for the PRONTO-T2D Investigators. Randomized double-blind clinical trial comparing ultra rapid lispro with lispro in a basal-bolus regimen in patients with type 2 diabetes: PRONTO-T2D. Diabetes Care 2020;43:2991-2998.
- Bode BW, McGill JB, Lorber D, Gross JL, Chang P-C, Bregman DB, for the Affinity 1 Study Group. Inhaled technosphere insulin compared with injected prandial insulin in type 1 diabetes: a randomized 24-week trial. Diabetes Care 2015;38:2266-2273.
- Hirsch IB, Beck RW, Marak MC, Kudva Y, Atkurk HK, Bhargava A, et al. A randomized trial comparing inhaled insulin plus basal insulin versus usual care in adults with type 1 diabetes. Diabetes Care 2025; 48:353-360.
- Davidson MB, Blanco-Castellanos M, Duran P. integrating nurse-directed diabetes management into a primary care setting. Am J Manag Care 2010; 16:652-656.
- Scarlett LD, Jenne KW, Duran P, Woodcock E. Goodman KM, Davidson MB. Glycemic effect of using patient-defined meal sizes instead of CHO counting to determine bolus doses of insulin. Diabetes 2025 Jun, 74 (Suppl 1).
- Davidson MB, Davidson SJ. Effect of remote glucose monitoring utilizing computerized insulin dose adjustment algorithms: a pilot project. Diabetes Ther 2019;10:523-533.
- Davidson MB, Davidson SJ: Effective use of computerized insulin dose adjustment algorithms on continuous glucose monitoring results by a clinical pharmacist proof of concept. J Diabetes 2021;13:439-441.
- Pulicharam J, Davidson SJ, Bubb C, Evans S, Davidson MB, 2022. Effect of incorporating computerized insulin dose adjustment algorithms into a remote patient monitoring program on HbA1c levels in patients with type 2 diabetes. Medical Research Archives, [online] 10(12). doi.org/10.18103/mra.v10i12.3396.
- Amante DJ, Harlan DM, Lemon SC, McManus DD, Olaitan OO, Pagoto SL, et al. Evaluation of a diabetes remote monitoring program facilitated by connected glucose meters for patients with poorly controlled type 2 diabetes: randomized crossover trial. JMIR Diabetes 2021;6:e25574.
- Menon A, Tornvall I, Bennetts D, Nugapitiya S, Varnfield M, Davidson M, Russell A. Rethinking the model of care of outpatient diabetes service. ATTD-ASIA 2024: Diabetes Conference, 18-20 November (kenes.com).
- Stone RA, Rao RH, Sevick MA, Cheng C, Hough LT, Macpherson DS, et al. Active care management supported by home telemonitoring in veterans with type 2 diabetes: the DiaTel randomized controlled trial. Diabetes Care 2010;33:478-484.
- Tildesley HD, Mazanderani AB, Ross SA. Effect of internet therapeutic intervention on A1C levels in patients with type 2 diabetes treated with insulin. Diabetes Care 2010;33:1738-1740.
- Bashan E, Herman WH, Hodish I. Are glucose readings sufficient to adjust insulin dosage? Diabetes Technol Ther 2011;13:85-92.
- Nathan DM, Kuenen J, Borg R, Zheng H, Schoenfeld D, Heine RJ, A1c-Derived Average Glucose Study Group. Translating the A1C assay into estimated average glucose values. Diabetes Care 2008;31:1473-1478.
- Robinson S, Newson Rs, Liao B, Kenndey-Martin T, Battelino T. Missed and mistimed insulin doses in people with diabetes: a systematic literature review. Diabetes Technol Therap 2021;23:844-856.
- Peyrot M, Barnett AH, Meneghini LF, Schumm-Draeger P-M. Insulin adherence behaviours and barriers in the multinational Global Attitudes of Patients and Physicians in Insulin Therapy study. Diabet Med 2012;29:682-689.
- Divilly P, Martinez-Edith G, Zaremba N, Soholm U, Mahmoudi A, Cigler M, et al. Relationship between sensor-detected hypoglycemia and patient-reported hypoglycemia in people with type 1 and insulin-treated type 2 diabetes: the Hypo-METRICS Study. Diabetes Care 2024;47:1769-1777.
- Gavin JR, Abaniel RM, Virdi NS. Therapeutic inertia and delays in insulin intensification in type 2 diabetes: a literature review. Diabetes Spectr 2023;36:379-384.