

Cone-Beam CT Analysis of Maxillary Molar Roots
Interpretation of Cone-Beam Computed Tomography Scans of Mesio-buccal Roots of Maxillary Molars: Developmental and Technological Considerations
Prof. Zvi Metzger1, Prof. Anda Kfir2
- Departments of Endodontics and Oral Biology, The Goldschleger School of Dental Medicine, Tel Aviv University, Tel Aviv, Israel
- Department of Endodontology, The Goldschleger School of Dental Medicine, Tel Aviv University, Tel Aviv, Israel
OPEN ACCESS
PUBLISHED 31 October 2025
CITATION Metzger, Z., and Kfir, A., 2025. Interpretation of Cone-Beam Computed Tomography Scans of Mesio-buccal Roots of Maxillary Molars: Developmental and Technological Considerations. Medical Research Archives, [online] 13(10). https://doi.org/10.18103/mra.v13i10.6980
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i10.6980
ISSN 2375-1924
ABSTRACT
Maxillary molars have usually three roots. The palatal and disto-buccal roots have a roughly round cross section with a single root canal. The third root, the mesio-buccal root has commonly an oval cross section and often has two canals. One canal is larger and located in the buccal part of the root, referred to as MB1 canal and another, which has usually a smaller diameter and is located in the more palatal part of the root is referred to as MB2 canal. Failure of endodontic treatment of maxillary molars is often related to the second MB2 root canal that was not recognized and not treated, thus containing necrotic tissue and bacteria. When considering the developmental pattern of the mesio-buccal root, it is rather predictable that if the root has an oval cross-section it is most likely to have an MB2 canal. Oval cross section may be best demonstrated in an axial view of a Cone-Beam Computerized Tomographic (CBCT) scan of the tooth. Yet, such scan may often have no evidence of the presence of MB2 canal. When voxel size of the CBCT scan is considered, absence of an MB2 canal in the scan may mean that its diameter may be smaller than can be detected in a clinical CBCT image. MB2 canals with a diameter of 100 µm cannot be expected to be seen even in a high resolution clinical CBCT scan, yet failing to find and treat them may lead to failure of the endodontic treatment of maxillary molars. Thus, when an oval cross section is detected in the MB root, the operator should use all his skills to find and treat the “invisible” MB2 canal.
Keywords
- Maxillary molars
- Cone-Beam Computed Tomography
- Mesio-buccal root
- Endodontic treatment
- Root canal anatomy
INTRODUCTION
FAILURE RATE OF ROOT CANAL TREATMENT OF MAXILLARY MOLARS.
Failure rate of endodontic treatment in maxillary molars is relatively high. A study found that 44.4% of endodontic failures occurred in maxillary molars. Another study reported that maxillary molars account for 31.6% of failed root canal treatments. In many cases the failure was caused by an MB2 (second Mesio-buccal) canal that was not detected and thus not treated. Getting familiar with the anatomy of the MB root and the development of its canal system is essential for adequate endodontic treatment of this complex root morphology. The aim of this Editorial is to enhance the understanding of the development of the MB root of maxillary molars on one hand and the limitations of the resolution of a CBCT scan on the other, thus allowing better interpretation of images derived from a CBCT scan of a MB root of maxillary molars.
DEVELOPMENT OF THE MESIO-BUCCAL ROOT OF MAXILLARY MOLARS.
The development of any root, including the MB (mesio-buccal) roots is initiated and dictated by the Hertwig’s epithelial root sheath (HERS). This temporary two-layer epithelial structure develops from the cervical loop of the enamel organ during the late bell stage of tooth development. It is made of the inner enamel epithelium and outer enamel epithelium, and guides the shape, length, and number of roots. Its function is to induce differentiation of dental papilla cells into odontoblasts, which then form root dentin. The root dentin develops from where the HERS initially was (the outer surface of the root), inwards to the place that will later be the root canal. The dentin gradually develops in layers (Figure 1). At early stages the root contains a very large and patent root canal. With maturation of tooth this gradual dentin apposition process will eventually stop, leaving the root canal of a mature tooth.
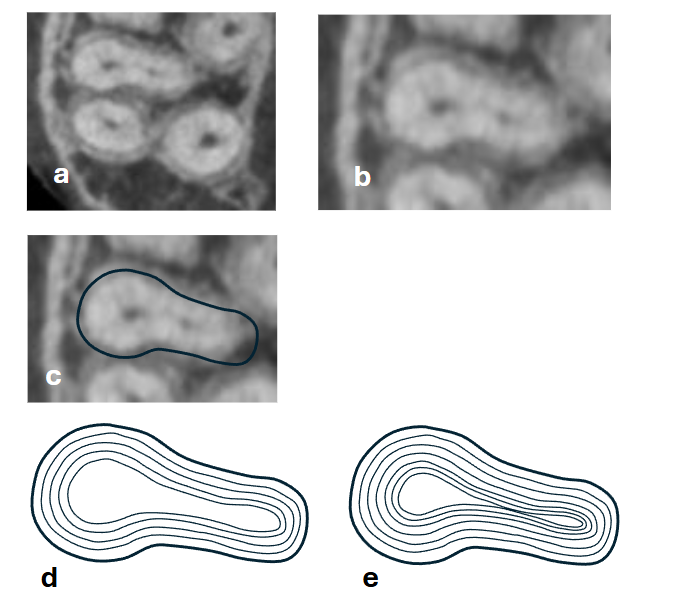
If the HERS had initially a round shape, the mature tooth will have one canal with a round cross section. In the case that HERS was oval, as in the case of many of the MB roots of maxillary molars, the end-result will be different. At early stages the young root canal will have an oval cross section, but at later stages the continued apposition of dentin may eventually separate the root canal into MB1 and MB2 canals (Figure 1).
When examining an axial section of a CBCT scan of the MB root, we should appreciate that the outline of the root represents the line at which the HERS initiated the process. If the outline is oval, we usually can see a clear MB1 canal on the buccal side of the root and either see or not another canal on the palatal side of the root. Sometimes we do not see a clear MB2 canal, yet considering the process described above we may understand the location at which the MB2 canal should be or was once located (Figure 1). The case will be different if the outer surface of the root had originally a round cross section. Only in such cases can we expect to have a single round canal. The shape of the outer surface of the MB root, as seen in an axial section of a CBCT scan is thus an important indicator for potential presence of an MB2 canal. However, one should keep in mind that the cross section examined should be in a plane really perpendicular to the long axis of the root. Sections of a round root may seem oval if the plane of the section is diagonal axis of the root, like diagonal salami slices of a perfectly round salami.
To obtain adequate axial view of the MB root, one may often have to tilt and align the scan along the axis of the specific root. It should be kept in mind that the 3 roots of a maxillary molar are often diverging from each-other and an optimal axial section of each root may require an individual alignment for each of the roots. A simple axial view of the whole tooth (rather than of the MB root alone) may be misleading.
LIMITATION OF CONE-BEAM COMPUTERIZED TOMOGRAPHY RESOLUTION
When examining a well aligned axial section of a MB root, one may often see an oval cross section with the MB1 canal clearly visible at the buccal area of the section. The MB2 canal may be seen as well, yet often no such canal can be seen in the place where it may be expected. Does it really mean the MB2 canal does not exist or that it is fully calcified?
We tend to think about CBCT as the most accurate and reliable radiographic-clinical tool to detect root canal anatomy. Yet, like every tool, it has its limitations. The image seen in CBCT is composed of voxels, the size of which greatly affects the resolution of the image. Scans that were generated with larger voxel size may provide less resolution than those generated with smaller voxel size.
One should also keep in mind other factors that may affect the resolution, which include unit-related factors such as field of view (FOV), as well as image acquisition and processing parameters such as exposure settings, detector technology, and reconstruction algorithms. Additionally, patient-related factors like motion, image noise and artifacts can significantly degrade image quality.
The best resolution of root canal details may be currently provided by microCT. Such excellent resolution often involves voxel size of 3-9 µm. Consequently, microCT is often related to as a “gold standard” in the analysis of extremely fine anatomical structure of teeth. Such small voxel size involves very high radiation exposure that may be used on extracted teeth but not on a patient. Currently the smallest voxel size that may be generated with most modern clinical CBCT scanners is commonly around 75 µm.
What does voxel size mean in terms of ability to detect very small root canal structures? It has been established that spatial resolution in planar radiographic images requires that the smallest structure that can be detected will be at least with the size of two pixels (voxels in the case of a three-dimensional image). Consequently, if a structure is smaller than 75×2 = 150 µm, we cannot expect to be able to detect it in a scan built of 75 µm pixels. As a clinical illustration, the diameter of the tip of a # 15 endodontic file is 150 µm.
An easy way to understand this issue is presented in a study by Bai et al. In this study extracted mandibular incisors were examined for presence of double canal and of accessory canals, using CBCT with voxel size of 300, 250, 200 and 125 µm and compared with a microCT image with voxel size of 9 µm, that was used as the “gold standard”. The ability of the observers to detect the dual canal in the CBCT scans increased with the reduction of the voxel size. Yet, most accessory canals which had a diameter of 131-192 µm, as measured from a microCT reconstruction, could not be reliably detected even when the voxel size used was 125 µm.
All the above leads to the understanding that when we cannot radiographically detect a very delicate structure such as an MB2 canal in a place where it should have been found, it does not essentially mean that the canal does not exist or that it is totally blocked by calcification. It may simply mean that the size of the structure/canal is smaller than 150 µm. In clinical terms such narrow canal may be accessed only by using #10 endodontic files or smaller. In biological terms we should keep in mind that the average size of a bacterium is about 1 µm. Therefore, a canal with a 100 µm diameter, may potentially contain as much as 10,000 bacteria per cross section. Thus, a small canal, even with a diameter of only 100 µm, and thus one that cannot be expected to be seen in the clinical CBCT axial section, has a great potential to lead to endodontic failure if not negotiated and properly endodontically treated.
Conclusion
CLINICAL IMPLICATIONS.
A significant proportion of maxillary first molars have two canals in the mesio-buccal (MB) root. Its prevalence can range from 48% to 96%, depending on the study and population. Less than one-third of MB roots of maxillary molars have a single canal. When the outer shape of the MB root, in its axial cross section, is oval with a buccally located MB1 canal, one should assume the presence of an MB2 canal even when no such canal is seen in the CBCT axial cross sections. The shape of the section will indicate where it should be found: In general, it should be located in the center of the palatal curved surface of the oval root (Figure 1).
Finding a narrow MB2 canal, that cannot be seen on a CBCT, requires knowledge and skill by an experienced operator. Knowledge that such canal may be patent even if the CBCT does not show it, and skill in the use of endodontic microscope, ultrasonic tips, spreaders and files that may allow the penetration of such a canal and performing an adequate endodontic treatment in a canal that though not seen in a CBCT scan, may lead to failure of the endodontic treatment if not found.
References
- Iqbal A. The factors responsible for endodontic treatment failure in the permanent dentitions of the patients reported to the College of Dentistry, the University of Aljouf, Kingdom of Saudi Arabia. J Clin Diagn Res. 2016 May;10(5): ZC146-8.
- Rao S, Niker V, Telikapalli M, Gala K. Incidence of endodontic failure cases in the department of conservative dentistry and endodontics, DY Patil School of Dentistry, Navi Mumbai. Cureus. 2023 May 10;15(5): e38841. doi: 10.7759/cureus.38841. PMID: 37303357; PMCID: PMC10254946.
- Fernando Peña-Bengoa, Carolina Cáceres, Sven-Eric Niklander, Patricio Meléndez. Association between second mesiobuccal missed canals and apical periodontitis in maxillary molars of a Chilean subpopulation. J Clin Exp Dent. 2023 Mar 1;15(3): e173-e176. doi: 10.4317/jced.60156. eCollection 2023 Mar.
- Hao J, Liu H, Shen Y. Periapical lesions and missed canals in endodontically treated teeth: A Cone-Beam computed tomographic study of a Chinese subpopulation. Med Sci Monit. 2023 Jul 4;29: e940533. doi: 10.12659/MSM.940533. PMID: 37401049; PMCID: PMC10329408.
- Yamamoto H, Cho SW, Kim EJ, Kim JY, Fujiwara N, Jung HS. Developmental properties of the Hertwig’s epithelial root sheath in mice. J Dent Res. 2004 Sep;83(9):688-92. doi: 10.1177/154405910408300906. PMID: 15329373.
- Jeong JK, Kim TH, Choi H, Cho ES. Impaired breakdown of Herwig’s epithelial root sheath disturbs tooth root development. Dev Dyn. 2024 Apr;253(4):423-434. doi: 10.1002/dvdy.667. Epub 2023 Oct 18. PMID: 37850829.
- Pires M, Martins JNR, Pereira MR, Vasconcelos I, Costa RPD, Duarte I, Ginjeira A. Diagnostic value of cone beam computed tomography for root canal morphology assessment – a micro-CT based comparison. Clin Oral Investig. 2024 Mar 8;28(3):201. doi: 10.1007/s00784-024-05580-y. PMID: 38453706; PMCID: PMC10920457.
- Bai B, Tang Y, Wu Y, Pei F, Zhu Q, Zhu P, Gu Y. Ex vivo detection of mandibular incisors’ root canal morphology using cone-beam computed tomography with 4 different voxel sizes and micro-computed tomography. BMC Oral Health. 2023 Sep 9;23(1):656. doi: 10.1186/s12903-023-03376-2. PMID: 37689620; PMCID: PMC10492267.
- Pauwels R, Araki K, Siewerdsen JH, Thongvigitmanee SS. Technical aspects of dental CBCT: state of the art. Dentomaxillofac Radiol. 2015;44(1):20140224. doi: 10.1259/dmfr.20140224. PMID: 25263643; PMCID: PMC4277439.
- Ghavami Lahiji M, Davalloo R.T, Tajziehchi G, Shams P. Micro-computed tomography in preventive and restorative dental research: A review. Imaging Science in Dentistry. 2021;51(4). Doi:10.5624/isd.20210087
- Brüllmann D, Schulze RK. Spatial resolution in CBCT machines for dental/maxillofacial applications-what do we know today? Dentomaxillofac Radiol 2015;44(1):20140204. doi: 10.1259/dmfr.20140204. PMID: 25168812; PMCID: PMC4614158.
- Park JW, Lee JK, Ha BH, Choi JH, Perinpanayagam H. Three-dimensional analysis of maxillary first molar mesiobuccal root canal configuration and curvature using micro-computed tomography. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2009 Sep;108(3):437-42. doi: 10.1016/j.tripleo.2009.01.022.
- Aung NM, Myint KK. Diagnostic accuracy of CBCT for detection of second canal of permanent Teeth: A systematic review and meta-analysis. Int J Dent. 2021 Jul 20;2021:1107471. doi: 10.1155/2021/1107471. PMID: 34335767; PMCID: PMC8315866.