

Congenital Muscular Torticollis: Insights for Pediatric Care
Congenital Muscular Torticollis: A Chapter that Led to the Establishment of the Specialty of Paediatric Orthopaedics
Gheorghe Burnei1; Mioara Georgescu, MD, Ph.D2.; Maricela Dragomir, MD, Ph.D3.; Mihaela Banculescu, MD, Ph.D4
- Professor of Paediatric Orthopaedics, Constanţa Macta Clinic, Bucharest Tinos Clinic, Romania
- Paediatric Surgeon and Orthopaedist, ‘Sf. Apostol Andrei’ County Emergency Hospital in Constanţa, Romania
- University Assistant, ‘Dunărea de Jos’ University in Galaţi, Faculty of Physical Education and Sports, ‘Health with Ozone’ Clinic of Integrative Medicine in Galaţi, Romania
- Anaesthesiology-Intensive Care, ‘Sf. Apostol Andrei’ County Emergency Hospital in Constanţa, Romania
OPEN ACCESS
PUBLISHED: 31 October 2025
CITATION: BURNEI, Gheorghe et al. Congenital Muscular Torticollis: A Chapter that Led to the Establishment of the Specialty of Paediatric Orthopaedics. Medical Research Archives, [S.l.], v. 13, n. 10, oct. 2025. Available at: <https://esmed.org/MRA/mra/article/view/6943>.
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI: https://doi.org/10.18103/mra.v13i10.6943
ISSN 2375-1924
ABSTRACT
Background: The importance of knowing about congenital muscular torticollis also lies in the fact that it ranks third as frequency among paediatric orthopaedic conditions, after congenital foot deformity and developmental dysplasia of the hip. The average incidence of this condition is 1.1%. As a result of spontaneous resolution and physiokinetotherapy, the cure rate also reached in our statistics to 98% when the diagnostic was established in the first days after birth and the treatment was initiated in the first days in special centres for newborns and infants. However, 9-21% of the patients had an indication for surgery after the age of 1 year.
Purpose: The article aims to elucidate some aspects regarding clinical signs and evolution, the importance of differential diagnosis, the implementation of appropriate recovery techniques in specialized centers for newborns and infants in order to improve current results and to make known the surgical technique designed by Romanian School of Paediatric Orthopaedics.
Study design: The article presents and illustrates the experience accumulated by the Romanian School of Paediatric Orthopaedics over the last 50 years, in the period 1975-2024. It integrates the study data with the experience of other clinics and authors, and it compares some debatable or controversial results.
Patient sample: This experience was analysed in multicentre studies that included 5,648 cases that were treated in all large specialty clinics using various procedures, and the essential notions of the most frequently used procedures are presented.
Method: The analysis and synthesis of data carried out in sessions and Consensus Conferences covered 5 distinct periods: 1) 1975-1980, the study of physiokinetotherapy methods and the results obtained up to the age of one year. 2) 1985-1990, types of surgical interventions performed and results. 3) 1990-2000, difficulties and causes that led to unfavourable results. 4) 2000-2005, histopathology studies on samples taken from resected sclerotic tissues. 5) 2005-2010, consensus for a surgical technique in different variants, adapted to each type of lesion. The documents were filed and submitted to the Romanian National Library.
The Romanian School of Pediatric Orthopedics, through Vereanu D., Pesamosca A., Socolescu M., Zamfir T., Goţia D.G., Aprodu G., Gavrilescu S.L., Gliga V., Ţepeneu P., Mironescu A., Tica D., Stan V. and Moldovan Z., made an important contribution the determination of a differentiated therapeutic attitude, in relation to the clinical form, extent, and age, in order to achieve a maximum beneficial effect. The Romanian School of Paediatric Orthopaedics procedure was initiated in university paediatric orthopaedic clinics and subsequently in county hospitals.
Results: When the diagnostic was established early, within the first 30 days, the treatment was limited to conservative measures, with good and excellent results. Most patients heal through spontaneous resolutions and by physiokinetotherapy in the first year of life. After the age of 1, surgical treatment is instituted both for aesthetic reasons, and to correct cervical mobility. The best results were obtained in patients operated on between 1 and 5 years of age. Most authors argue that surgical treatment after the age of 5 has a limited value, and when the surgical intervention is performed after puberty, the results are unsatisfactory and major complications may occur. Schoolchildren and adolescents submitted to surgical intervention for congenital muscular torticollis remain with craniofacial dysmorphism and limited head mobility. Of the total of 5,648 patients analyzed at Consensus Conferences during the period 1975-2024, 582 (10%) were operated on: 477 (82%) up to the age of 5 years, 86 (15%) between 5 and 18 years and in adulthood, between 18 and 40 years, 19 (3%).
Conclusion: The objective of surgical treatment is aesthetic and functional, and it aims to correct cervical mobility. The study confirms that current results can be improved and that Romanian School of Paediatric Orthopedics procedure is an effective alternative for schoolchildren, adolescents, and adults.
Keywords
Vicious posture of the cephalic extremity, spontaneous evolution, physiotherapy and surgical options, Romanian School of Paediatric Orthopaedics procedure, paediatric orthopedics as a separate specialty.
Introduction
Torticollis is a deformity characterized by permanent tilting of the cephalic extremity to one side and the rotation to the opposite side. The condition was described for the first time by Heusinger in 1812. The name comes from the Latin words tortus (twisted) and collum (neck). This condition is also called loxia (Greek loxos = oblique). The vicious position of the head is induced by the contracture and retraction of the sternocleidomastoid (SCM) muscle. The most common and representative form of torticollis is congenital muscular torticollis (CMT), with other forms (arthrogenic, ocular, osseous, infectious, nervous, and drug-induced) being much rarer.
The causes of occurrence are not fully elucidated. The incidence of CMT in newborns varies depending on certain geographical areas, countries and ethnic factors. In recent years, the prevalence of the malformation has been increasing. Early diagnosis, in the newborn, followed by prompt and effective treatment, increases the cure rate to 98%. The results obtained depend on the time of initiation of treatment and may reach significantly lower percentage values if they are started after 4 months. Currently, there is no international consensus on diagnostic criteria and treatment methods. The Romanian School of Pediatric Orthopedics (RSPO) has contributed to the stability of some diagnostic indices and to the conceptualization of an operative technique with differentiated operative times in relation to the anatomopathological form.
At 2-3 weeks, in the SCM region, on a portion or the entire area, a round oval-shaped mass appears, visible or palpable, called sternocleidomastoid pseudotumor. This pseudotumor was detected in 60% of patients and it was an indication for early physiotherapy, even before the occurrence of cephalic extremity deviation.
The resolution of these pseudotumors may occur spontaneously by the age of one year. The detection of these pseudotumors in the first weeks of life allows the early initiation of conservative treatment, and the cure rate reaches to 95–97%.
Etiopathogenesis
Congenital muscular torticollis is the result of contracture and retraction of the SCM muscle, caused by interstitial myositis. The etiology of interstitial myositis in CMT has not yet been elucidated.
Idiopathic intrauterine embryopathies or vicious intrauterine position may cause CMT syndrome. The high incidence of obstetric difficulties may be the result rather than the cause of SCM contracture and retraction syndrome. Pseudotumor of the SCM muscle occurs in newborns and it is detectable upon examination, most commonly between 2 and 4 weeks, but it may also be present in the first week of life, up to 2 months of age. Currently, there are no publications providing data on the antenatal detection of sternocleidomastoid tumours by ultrasound examination.
The main histological lesion is fibrosis of the sternocleidomastoid muscle. The notion of endomysial fibrosis defines the deposit of collagen and fibroblasts around muscle fibers that are atrophying. The sarcoplasmic nuclei are merged to form giant muscle cells that appear to be multinucleated. These histological abnormalities are common in CMT.
The maturity of fibrous tissue in newborns suggests that the disease may have begun before birth and thus contribute to difficulties during delivery. The incidence of breech delivery reaches to 20-30% in children with CMT, much higher than the incidence in the normal population.
Clinical Data
1. The pseudotumor appears as a discrete swelling in the SCM region, either in a specific area or across the entire region, it has a renitent consistency, elliptical configuration, and it is indolent. The dimensions can range from 1 to 2 cm. It develops 2-3 weeks after birth and it occurs in 52% of newborns and 8% of infants.
In some cases, a thorough and rigorous examination of the newborn reveals this pseudotumor without any obvious manifestations or signs of torticollis. The obvious tilting of the head to one side and the rotation to the opposite side of the pseudotumor, without significant flexion of the head on that side, occurs later. Pseudotumor at the tendinomuscular junction is a prognostic clue in the occurrence of CMT.
Pesamosca shows that 19 newborns in a group of 84 patients with CMT who had pseudotumors without signs of torticollis, 10 underwent physiokinetotherapy and they were cured after 1 year, while the other 9 who were untreated and neglected later developed torticollis and underwent surgery after 1 year of age. We followed 38 newborns presented for orthopaedic consultation with pseudotumors in the SCM muscle without signs of torticollis. All underwent physiokinetotherapy and upon the re-evaluation performed after one year, they showed no signs of torticollis. The presence of these pseudotumors without signs of torticollis should be followed by competent recovery treatment.
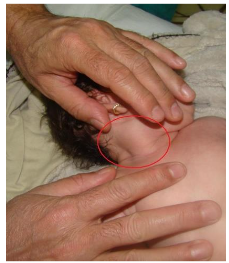
In other patients, the pseudotumor is more prominent and the SCM muscle appears thickened and stiff along its entire length. The rotation and lateral tilt are limited. The rotational capacity of the SCM muscle can be measured by passively rotating the head with both hands while standing behind the patient. The sternocleidomastoid muscle is stretched to its maximum length by rotating the head toward the affected side. The fibrous portion of the muscle cannot be stretched to its maximum, and the ipsilateral rotation is greatly diminished.
As a result of the contraction and retraction of the SCM muscle, induced by interstitial myositis, clinical examination reveals complex deviation of the cephalic extremity: the head is tilted slightly backward and toward one of the shoulders, the auricle approaches the acromion, the face is turned toward the opposite side, and the palpebral fissures and oral commissures are no longer at the same level. The angle between the plane of the eyes and the plane of the mouth estimates the degree of facial hemihypoplasia. Normally, these lines are parallel, but they form an angle between them when the face presents an asymmetry. The occurrence of hemihypoplasia requires surgical intervention to eliminate the cause and to allow a normal growth. Significant facial hemihypoplasia occurs at around 8 months of age, but it becomes obvious between 3 and 4 years of age. If torticollis is treated surgically, after the surgical intervention, the hemihypoplasia becomes less obvious or it disappears.
2. Progressive facial deformation, accentuated head deviations, and changes in the cervical region in children over 6 years of age lead to the development of cranio-cervico-facial dysmorphism, which also affects bone structures. Hypoplasia of the zygomatic bone and flattening of this prominence accentuate facial dysmorphism. The mandible and maxilla are also hypoplastic due to inhibition of local growth and development.
3. Plagiocephaly may be obvious in toddlers who have a fixed head rotation. The head, which is relatively soft, becomes deformed because it is held in the same position for a long time. Flattening (occipital bevelling) secondarily induces contralateral frontal flattening. Plagiocephaly develops in the first months of life, and it is best noticed when looking at the head from above. The incidence of plagiocephaly varies from 18% to 19.7% and it affects approximately 720,000 infants per year in the United States. The association between plagiocephaly and CMT is present in 70% to 95% of infants. After 5 months, once the child sits up or after the torticollis disappears, plagiocephaly tends to disappear. This deformity can take several years to disappear completely, and in some cases a slight deformity may remain permanently. A retrospective analysis on a group of 184 patients with CMT found that the association of torticollis with plagiocephaly after 3 years disappears, and there are significant increases in children who have plagiocephaly exclusively.
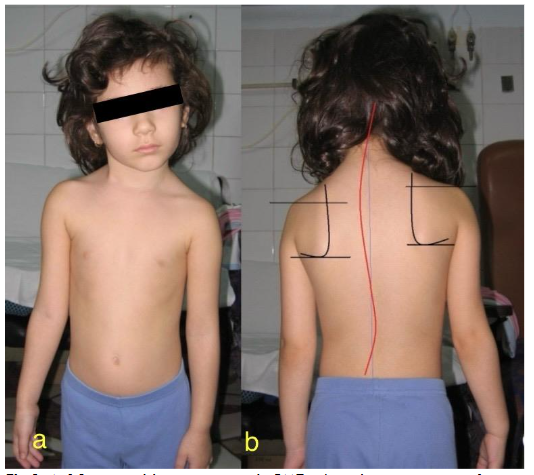
4. The spine, in 8 out of 10 children over the age of 6, shows changes in configuration. At the level of the cervical and thoracic rachis, the congenital torticollis syndrome causes double scoliosis: one proximal, cervical or cervico-thoracic, with concavity on the affected side, and another compensatory thoracic, with concavity on the opposite side.
POSTURAL AND DYNAMIC ATTITUDE
In order to walk comfortably, the plane of the palpebral apertures must be horizontal. This allows the child to maintain balance and the eyeballs to move horizontally. The correction of the attitude induced by torticollis is compensated by raising the ipsilateral shoulder or by the appearance of cervical and thoracic scoliosis. The adjacent trapezius muscle becomes hypotrophic because of inactivity.
Children with bilateral CMT also experience changes in locomotion. Bilateral congenital muscular torticollis is extremely rare. With the cranial extremity fixed in flexion, the gaze is directed downward and the visual field is significantly reduced. Between 1994 and 1998, I cared for and treated three patients from a Children’s Home who were living in poor conditions and had bilateral CMT, who were subject to surgical intervention after the age of 6, at 7, 8, and 10 years of age, respectively. All of them showed static and dynamic changes. The cervical segment was straight, thoracic kyphosis was exacerbated, lumbar lordosis was attenuated, and the pelvis was positioned in antepulsion when walking. In this context, the dyssynergia of the kinematic chains makes walking extremely difficult and tiring, and energy consumption excessive.
Differential Diagnosis
The evaluation of a case in which the cephalic extremity is positioned in a vicious lateral tilt and twist must determine whether this is due to myofibrosclerosis of the SCM muscle, characteristic of CMT, or another cause. CMT is characterized by a typical lateral tilt attitude and contralateral rotation of the head, associated to myofibrosis of the SCM muscle, detectable by the prominence of the muscle as a rigid band, although some children have a relatively short neck and the muscle may be difficultly noticed. Therefore, the muscle should be palpated along its entire length to detect whether there is a thickened or fibrous area on a specific portion or throughout the muscle. The sclerosis process particularly affects the clavicular insertion bundle. In 60% of cases, a well-localized tumour occurs and the entire SCM muscle seems to be affected. If the muscle is neither prominent nor reduced in size, the patient does not have CMT and other investigations must be performed to establish the diagnostic.
Ocular muscular torticollis. Strabismus can cause the head to tilt as a result of unbalanced eye rotation. The tilt compensates the abnormal position of the eyes so that the strabismus is not obvious at first glance. When the head is passively straightened, the strabismus can be easily corrected. Myofibrosis of the SCM muscle can occur in ocular torticollis if the diagnostic is established in 5-6 months.
Posterior fossa tumour. A posterior fossa tumour can compress a portion of the brain and it can engage in the foramen magnum, causing the head to tilt to one side. The cephalic extremity is blocked in this position and it is difficult to move passively or actively. Torticollis usually occurs after the tumour has been diagnosed and it appears only occasionally as the first manifestation. The neurological examination can distinguish lower cranial nerve dysfunction and brain function disorders.
Congenital cervical scolioses. Congenital cervical scolioses can lead to head tilt since birth. Vertebral lesions can be identified clinically, upon the inspection and palpation of the cervical vertebrae, and confirmed by radiography.
Grisel’s syndrome occurs as a complication of upper respiratory tract infections. It is also known as nasopharyngeal torticollis or subacute osteitis of the atlas, following a cervical suppuration. Radiological examination of the rachis highlights anterior subluxation through atlanto-odontoid diastasis, the odontoid apophysis being intact. This condition occurs in the first two years of life.
Brissaud’s mental torticollis occurs in psychasthenic adolescents and adults.
Spasmodic torticollis. The contracture affects the trapezius and SCM muscles, the lesion being located on the striated nuclei on the opposite side. The manifestation consists of seizures of 10-30 seconds, after which the cephalic extremity returns to its initial position. The event can be repeated at varying intervals, sometimes rarely, sometimes it is subintrant.
Occupational torticollis occurs especially in adolescents or youth, more frequently in men, in connection with a moment of overwork, hyperactivity, excessive effort, or vicious postures. This type of torticollis is found in violinists, pianists, photographers, etc.
Stiffness of the neck with lateral fixation of the cervical rachis. It occurs in older children or adults as a vertebro-myopathic rigidity. Laboratory, radiological, and imaging tests can establish the cause as sequelae of tuberculosis, meningitis, spondylitis, spondylosis, Klippel-Feil syndrome, post-inflammatory sclerosing myositis, rheumatic myositis, metabolic disorders, trichinosis, etc.
Medication-induced torticollis. Certain chemicals, administered abusively, such as ketamines, amphetamines, cocaine, or neuroleptics, can induce acute dystonia crises with sudden, involuntary, reversible onset, manifested by acute torticollis, with or without oculogyric and buccolingual crises. These manifestations are exceptional and accidental in children.
Physiokinetotherapy
If newborns and infants with CMT are not treated by the age of 6 months for various reasons, the cure rate through physiotherapy treatment at the age of one year drops to 70% for those who have followed the therapeutic protocol and 50% for those who have undergone occasional, irregular physiotherapy. In the absence of improvement in the characteristic attitude present at the beginning of physiokinetotherapy or the significant persistence of mobility restrictions, a surgical consultation is indicated for further investigation and for the reassessment of the diagnostic. In this case, the physiotherapist may be obliged to change the methods of conduct and continue the treatment until the age of 1 year. If at the age of one year the muscular balance and postural symmetry of the neck are not restored, it is surgically intervened.
Physiokinetotherapy is most effective before the age of 1. Canale et al., after a long-term statistical study, highlight the fact that conservative treatment rarely brings improvement or healing after the age of 1. Most cases of CMT heal either spontaneously in the first months after birth or after early conservative measures initiated and controlled by passive movements. Sönmez et al. showed that 95% of patients with CMT, diagnosed and treated by physiokinetotherapy before the age of 1 did not require surgical treatment. Data recorded by RSPO in a multicenter study highlight that the spontaneous recovery rate was 24.6%. Neonatologists from 8 university centers diagnosed a group of 1,878 newborns with CMT during the first 3 days of life over a two-year period, from 1996 to 1997. The diagnostic was confirmed by paediatric orthopaedists. All patients were taken over by family doctors and sent for physiokinetotherapy. Out of the total number of patients, 138 newborns were unable to undergo physiotherapy. At 6 months of age, 34 (24.6%) no longer had torticollis and 104 showed obvious signs of torticollis. Out of those 104, 92 followed the therapeutic protocol and 76 were cured (75%), while 12 underwent sporadic treatment and only 6 were cured (50%).
We recommend that passive movement exercises be performed by parents under the guidance of a physiotherapist in order to reduce costs and facilitate the access to physiotherapy for more children. The attempts to position the child’s head on a higher pillow during sleep, with the body lying on the affected side in lateral decubitus, seem to be useful only when the rigidity of the SCM muscle is not severe. Some physicians consider that it is important to advise parents to place toys or other objects desired by the child on the side of the lesion to encourage them to turn their head to that side. These exercises do not harm the child and can facilitate the beneficial effect of physiotherapy.
Surgical Treatment
A. INDICATIONS
1. Surgical intervention is performed after the age of 1 year. Most cases of CMT are solved with conservative treatment, especially physiotherapy, with higher success rates if the intervention is initiated before the age of 4 months. However, in 9-21% of the cases, the condition persists, requiring surgical correction. The maximum surgical effect is achieved in children between 1 and 5 years of age, before facial dysmorphism structurally affects the neurocranium, viscerocranium, and the spine.
2. Sternocleidomastoid muscle rigidity associated with limited head rotation.
3. Sternocleidomastoid muscle rigidity associated with progressive facial hemihypoplasia.
4. In bilateral CMT, the intervention is performed bilaterally during the same surgical procedure.
B. SURGICAL TECHNIQUES
The procedure is performed under general anaesthesia with laryngeal or endotracheal intubation, following the evaluation and according to the preference of the paediatric anaesthesiologist. The main objectives are to ensure optimal conditions for surgery, alleviate perioperative pain, minimize risks specific to paediatric patients, and facilitate a quick and comfortable recovery. The combination of general anaesthesia with ultrasound-guided locoregional techniques, such as the intermediate cervical plexus block and the interscalene brachial plexus block, is the modern standard of care.
The child is positioned in dorsal decubitus with the affected shoulder raised and the head rotated to the contralateral side to best expose the sternocleidomastoid region. There are various surgical procedures for treating CMT. Romanian School of Paediatric Orthopedics has included in its surgical repertoire the entire therapeutic arsenal recorded in the history of this disease. The most commonly used techniques consisted of muscle relaxation through distal, proximal, bipolar, and Foederl tenoplasty approaches.
Sternocleidomastoid tenotomy with von Volkmann’s distal approach. After positioning the patient and preparing the surgical field, a 2 cm incision is made, centered on the relief of the two caudal ends of the sternocleidomastoid muscle. To avoid unsightly scarring, the incision is placed 1 cm cranially to the clavicular relief. The platysma muscle is dissected at the level of its clavicular insertion. After sectioning the superficial cervical fascia, the two distal ends of the SCM muscle can be exposed. The clavicular end is sectioned under the protection of a grooved guide positioned underneath it. Once sectioned, the muscle end retracts spontaneously. The correction is checked, and if it is not achieved, the incision is extended medially, over the sternal extremity of the SCM muscle, and then the sternal end and the middle cervical fascia are sectioned. The correction is checked again by tilting the head in the opposite directions of the vicious positioning. This technique is frequently used. The most likely complication is damage of the external jugular vein. Care should be taken to protect the internal jugular vein, the common carotid artery, the superior cervical arch, and the vagus nerve.
Sternocleidomastoid tenotomy with cranial approach was described by Tillaux and Fritz Lange. The incision can be longitudinal or transverse, of approximately 3 cm, from the mastoid to the muscle belly, avoiding its extension anteriorly so as not to damage the facial nerve. The transverse incision is made directly under the mastoid process. The retracted muscle insertion is highlighted near the mastoid, after the dissection of the superficial cervical fascia, and it is sectioned under the protection of a grooved guide.
Bipolar tenotomy (Hellstadius, Putti) is indicated in children over 7 years of age. The surgical technique is a combination of caudal and cranial tenotomy, including also the excision of the middle cervical fascia. The complication rate is no higher than that of cranial or caudal tenotomy.
Sternocleidomastoid muscle removal (Mikulicz) is used in severe forms of CMT in older children and adults or in cases where torticollis has relapsed. A median transverse incision is made on the relief of the SCM muscle. The muscular belly of the SCM muscle is exposed and separated caudally to the clavicular and sternal ends and cranially to the mastoid process. The two ends are sectioned caudally and the cranial end is sectioned proximally, under the mastoid process. This step carries the risk of damaging the accessory nerve, which runs obliquely along the posterior surface of the SCM muscle or may penetrate the perimysium. The excision of the deep cervical fascia is necessary and enhances the correction of torticollis. The placement of a drainage tube eliminates the risk of complications and ensures a smooth postoperative recovery.
Possible complications include the damage of the common carotid artery, internal jugular vein, vagus nerve, accessory nerve, and cervical motor branch of the facial nerve. The rate of accessory nerve damage and trapezius muscle paralysis can reach to 14%.
The tenoplasty procedure (Foederl) corrects the deformity through caudal approach. After separating the sternal and clavicular ends, the sternal end is sectioned at the tendinomuscular junction, and the clavicular end at the insertion. The cervical aponeurosis is sectioned to allow correction, and the two ends are sutured. If the two ends remain distanced, the aponeurotic portion can be split to facilitate suturing. This suture by elongation and splitting restores a fragile and inefficient tendon that does not allow early mobilization and requires immobilization in a cast or customized orthoses. The correction of the deformity is sometimes limited by the dimensions obtained by elongation and splitting. The effectiveness of this technique can be achieved by applying the tenomyoplasty technique described by Burnei for the correction of genu flexum in spastic, arthrogryposis, and post-traumatic cases.
Approach and Technique of the Romanian School of Paediatric Orthopedics. After 2010, all patients underwent surgery using the RSPO technique. In order to maximize the effect of the intervention, the patient undergoes preoperative physiokinetotherapy, 1-2 courses of 14 days. The perimisial fibrous tissue and the tissue adhering to the cervical fascia become better contoured and are more easily separated from the muscular and vascular-nervous tissues.
Surgical times
- The patient is placed in the supine position, with the affected shoulder elevated and supported by a bracket, so that the SCM region be well exposed. In this position, the head is placed in slight hyperextension and rotation, depending on the degree of myosclerosis of the SCM muscle.
- An incision of approximately 3-4 cm is made at 1-2 cm cranially to the clavicle, centered on the relief of the SCM muscle.
- The platysma muscle is sectioned; the use of electrocautery minimizes bleeding.
- The sternal and clavicular ends are separated and sectioned. The sternocleidomastoid muscle is retracted significantly and then digitally detaches to allow for its complete relaxation. The lack of intraoperative recovery tested passively may require the incision or excision of the SCM primissium covered by the adherent and sclerotic middle cervical fascia.
- An assistant outside the surgical field (orthopaedist, anaesthesiologist, or nurse) holds the head between their hands so that the anesthetized patient “looks forward”.
- The surgeon identifies the middle cervical fascia and performs its complete resection, not just the areas of sclerosis. We carried out a multicenter study in the period between 1994 and 1998 on 112 patients aged between 1 and 5 years. Samples were taken from the excised cervical fascia of each patient for histopathological examination. The results showed the presence of cellular changes specific to mature fascial fibrosis. Therefore, the excision of the middle cervical fascia should be performed in all cases, even if it does not appear sclerotic. It has already been demonstrated that the nature of the soft tissue that replaces degenerated muscle tissue differs depending on the age of the patient.
- Identification of the omohyoid muscle illustrates the total excision of fascial sclerosis.
- The assistant outside the surgical field holds the head between hands and performs a lateral tilt movement on the side opposite the lesion (head resting on the shoulder) and a lateral rotation movement (“look at the wound”).
- In this position, the surgeon digitally assesses the remaining sclerotic branches of the middle cervical fascia to be excised: the sclerosis of the carotid vascular sheath, areas of sclerosis in the remaining cervical fascia.
- The distal section of the anterior scalene muscle. We resorted to this surgical technique in 17 patients. In the final test, this muscle had the disposition of a fibrous band that opposed intraoperatively to the correction of the vicious position. These patients were over 5 years of age and had severe forms that were neglected by CMT.
- A meticulous dissection and rigorous haemostasis do not require drainage.
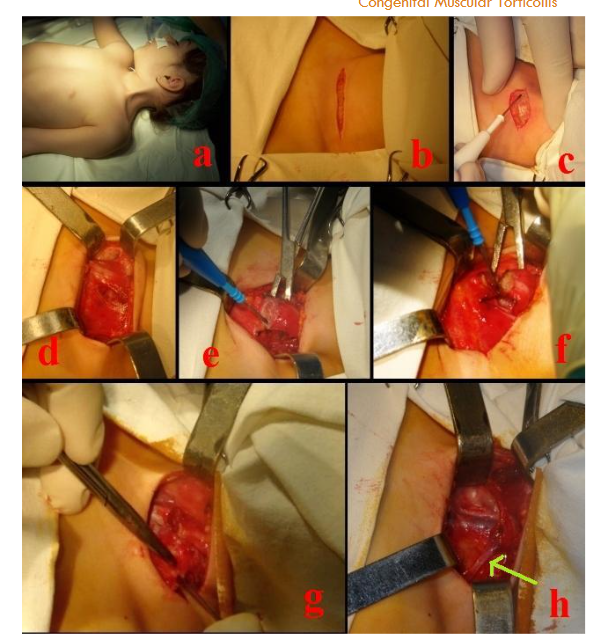
Fig. 3. Romanian School of Paediatric Orthopaedics technique:
a. Positioning the patient in the supine position with exposure of the SCM region.
b. Transverse incision at 1-2 cm cranially to the clavicle.
c. Sectioning the platysma muscle.
d. Exposure of both distal ends of the sternocleidomastoid muscle.
e. and f. Sectioning the two distal muscle ends of the SCM muscle, detachment of the muscle belly, and excision of the perimysium.
g. Exposure of the middle cervical fascia with normal macroscopic appearance but with sclerogenic potential; in children older than 5 years, it is frequently fibrotic and retracted.
h. Exposure of the omohyoid muscle, which ensures complete and correct release of fascial retractions.
Endoscopic sternocleidomastoid tenotomy
Endoscopic sternocleidomastoid tenotomy is performed using two types of approaches. The procedure described by Burstein and Cohen in 1998 is performed by inserting the trocar into the hairy supramastoid region of the head in a craniocaudal direction. After identifying and bypassing the greater auricular and accessory nerves, the muscle is sectioned from the lateral to medial side, until all muscle fibers are sectioned. The proof of complete sectioning is the appearance of the carotid artery and jugular vein in the inferior plane of the surgical field. The second technique is subcutaneous endoscopic transaxillary tenotomy (SETT), described by Sasaki in 2000. A zigzag incision of about 3 cm is made in the anterior axillary fold, followed by the creation of a subcutaneous tunnel, perpendicular to the longitudinal axis of the SCM muscle. Endoscopic access is easy and quick to the fibrous bands of the sternocleidomastoid muscle, which will then be sectioned with electrocautery or scissors, sometimes requiring sectioning of the anterior scalene muscle.
C. COMPLICATIONS COMMON TO ALL TECHNIQUES.
Postoperatively, a hematoma may occur as a result of inadequate haemostasis. Dissection by diathermocoagulation minimizes blood loss. Veins of no surgical importance can be sectioned and ligated if they cannot be reclined and removed from the surgical field. Persistent torticollis is due to incomplete sectioning of the SCM muscle ends or failure to resect sclerotic tissue. In children aged 1 to 5 years, postoperative evaluation should be performed periodically until the torticollis disappears completely, the SCM muscle appears normal, and the scoliotic deviation is healed.
D. POSTOPERATIVE TREATMENT.
Postoperative care is essential for all cases of torticollis surgery. The postoperative immobilization protocol for CMT is controversial. Depending on the technique used, position maintenance can be achieved by traction, plaster cast, fixation vest, or immobilization with a collar. We are advocates of the use of a cervical collar in all patients, including children between the ages of 1 and 2. Physiotherapy, initially passive, then passive and active, begins between the 3rd and 7th postoperative day. We resort to the application of a plaster cast in exceptional cases. Throughout the treatment period, patients must be treated in a manner that provides them comfort and restores the correct position of the head and mobility of the cephalic extremity, thereby improving their quality of life.
Methods
The synthesis of data extracted from the Consensus Conferences was made by the Heads of Pediatric Surgery Clinics gathered in working sessions with the Heads of Pediatric Orthopedics Departments from university clinics. All extracted and confirmed data were compared with those recorded in treatises, monographs and articles. As a result of this analysis, new data emerged showing that clinical signs and manifestations have interferences in evolution and are reflected in the results obtained; the presence of SCM tumors without clinical manifestations at birth followed by the appearance of CMT, spontaneous resolutions in neglected batches and others.
The most experienced surgeons of RSOP conceptualized a surgical procedure that includes differentiated operating times depending on the type of anatomopathological changes. This experience was integrated and presented didactically for both orthopedists and other specialties.
THE EXPERIENCE AND CONTRIBUTIONS OF THE ROMANIAN SCHOOL OF PEDIATRIC ORTHOPEDICS
The emergence of the RSPO was circumstantially interdependent on the final solutions of the Consensus Conferences on CMT. The lack of common approaches in specialized centers was considered a deficiency caused by the lack of a paediatric orthopedics (PO) specialty. In Romania in 2010, for the first time in the world, Professor Burnei established PO as a separate specialty. Initially, in 2008, he founded the Romanian Association of Paediatric Traumatologists and Orthopaedists and, following some legal proceedings, by Decision 2958/2010, the specialty of Paediatric Surgery and Orthopedics was split into two specialties, Paediatric Surgery and PO. Resident physicians in PO underwent a 6-year residency and had an individualized study program in paediatric traumatology and orthopedics. Paediatric surgeons and orthopaedists who had a predominantly orthopaedic activity, over 50% of paediatric traumatology and orthopedics interventions, chose to continue their activity in the PO departments. In a short time, the progress was remarkable. Limb lengthening, surgical treatment of idiopathic and congenital scoliosis, treatment of distortions in osteogenesis imperfecta, resection of malignant tutors, and endoprosthetics quickly became routine procedures, and the quality of medical services improved substantially.
Professor Pesamosca, head of Romanian paediatric surgeons and orthopaedists, was a passionate advocate for the separation of the 2 specialties, with the aim of developing them. In 2011, at the beginning of my first year of residency in PO, he entrusted me with all the documents from the Consensus Conferences on the diagnosis and treatment of CMT. They were placed in a separate compartment in the hospital’s personal library, next to another compartment containing all the consensus documents on Parathyroid Surgery. He said a few words that I will never forget. “Here lies the work and ideas of many physicians. Some of them have passed away, some you don’t know, but their hope will now live on in your conscience. Be fair, take what is most effective for patients, and finalize a surgical protocol for the Romanian School.”
In Romania, there has been a particular focus on establishing early diagnosis, streamlining the procedures described in medical literature, and reducing and avoiding possible complications with major intraoperative risks. After several Consensus Conferences organized in several University Centers, it was decided in 1990 to apply a Consensus Surgical Protocol in the treatment of children with CMT only in university centers and then in all county hospitals.
Orthopedic surgeons were joined by a number of dedicated anaesthesiologists such as Stoicescu M., Teianu M., Mârza L., Ilie L., Pick D., and Rusu F. Younger colleagues such as Tanase C. and Popa E. achieved resounding successes. Banculescu Mihaela, in perfect symbiosis with the nurse Oprea A, who is rarely seen, through dedication, strength, and knowledge in anaesthesia and intensive care for children, transformed Medical Analysis Constanta from a small hospital into a university clinic thanks to a revelation that seemed to give them an impetus towards the absolute.
INNOVATIVE MEDICINE AND EPIGONES
Epigones understand nothing about innovative medicine. They are tempted to go through their residency like “a goose through water”. They adore the quiet life of those who want to do nothing. If you guide them to do research, you encounter visceral resistance. It is impossible to build with ignorant and incompetent people because they refuse to think! However, if they work in a high-level environment, dedicated to medical performance, they believe themselves to be important people, but later reality forces them to live their destiny as irresponsible scoundrels. Then they confer the pinnacle of mediocrity on their performance. An envious lich also bears the pathognomonic seal of a lack of common sense and education. This lich is a perfect villain and bites the hand of the one who nourished him physically, spiritually and professionally.
If they happen to be part of a medical team that practices innovative medicine, not only are they completely out of place, but they are also receptive to the conversations of the envious who, whether they know it or not, in order to compromise everything, qualify these innovations, some of which are simple in their differentiated approach, as malpractice. In fact, they come to the hospital to have somewhere to go, or rather to be busy.
Innovative medicine means knowledge and experience adapted to each individual case. They cannot understand this simple and eloquent definition because they have neither knowledge nor experience. They are dependent only on what they have learned and retained, that “this is how it’s done, and that’s it!” They are the advocates of some medical gestures that do not require involvement and responsibility. They have taken advantage of circumstantial situations and influences that they have exploited commercially for their own personal gain, and in order to appear interested, they simulate a thoughtful attitude like the thinker in Hamangia’s masterpiece of civilization entitled “The Thinker” and “The Seated Woman”. They are certified scoundrels who, at the signal of an “authorized” ion, are ready to destroy you when you are unjustly assaulted, not only through indifference but also through direct attack. Before assaulting you, they refer to the Hippocratic Oath. They stand up abruptly when you enter a room where there are several colleagues, they want to kiss you when you appear after a period of absence to show their respect, and they offer to drive you home in their car to show that they behave like a “son” detached from the sacredness of the Hippocratic Oath. In reality, these models are empty inside, ordinary scoundrels with the airs of disciples who want to be labelled by you as a younger colleague who is educated and full of character, but they want to gain your trust in order to kill and devour you.
The epigones want to take your place no matter what, even though they are incompetent and irresponsible. They destroy almost everything, and if anything remains, it will soon become nothing.
Modern medicine is not the same as the medicine practiced 50 or 100 years ago, and in the future it will be completely different from what it is today. It has taken what has proven to be best in the medicine of the past and assimilated new methods of diagnosis and treatment thanks to innovative medicine applied according to standards and criteria that focus on maintaining health and healing patients.
Scoundrels want comfort and lack of responsibility. Thanks to this group of individuals, we must be careful to know, identify, and isolate the most important opponents who stand in the way of normal progress that can be achieved in medicine, as has been done so far, and the joy of patients to be healed.
It is hard to believe that you can meet such people in the medical world. Medicine seems to be a destiny, not a profession. Physicians are exceptional destinies. However, often scoundrelism goes hand in hand with imbecility. Imbecile scoundrels, whether physicians or not, influence their peers and have a limited impact on those around them (a physician and his family) or an entire community (a group of patients with certain diseases). The harmful potential of the imbecile depends on genetic factors and the degree of influence he can have in society, whether it be himself or those aligned behind him for material or pecuniary interests, such as the export of patients.
Discussion
The unsightly effect and typical attitude of the cephalic extremity in patients with CMT has aroused interest since ancient times. Plutarch believed that Alexander the Great had torticollis. In 350, Antyllus performed the first tenotomies, which were commented on by his contemporaries and then by his followers. The first recorded tenotomy was performed in 1641 in Amsterdam by Minnius. Dupuytren published important works on torticollis and treated it as a subject of interest. Most cases of congenital torticollis are benign and are solved spontaneously or by manual stretching. With proper treatment, 90% to 95% of children improve before their first year of life, and 97% of patients improve if treatment begins before the first 6 months. Craniofacial asymmetry also improves, especially in cases treated early. When patients present late or when physical therapy is unsuccessful, a surgical approach may be necessary. The results of surgical treatment are generally good, with improvement in neck range of motion and correction of deformity.
Congenital muscular torticollis is the most common and representative form of torticollis, with an incidence ranging from 0.3 to 1.9%. The goal of surgery is to facilitate normal growth by removing the unsightly effects of facial asymmetry and improving head mobility. Rehabilitation of facial asymmetry after 5 years is difficult to achieve. After this age, residual deformities remain: contralateral flattening of the occipital bone, hypoplasia of the ipsilateral zygomatic prominence, and the asymmetry of the eye, ear, and mouth corner on the affected side. Bone deformities can be corrected after surgery if the surgical intervention is performed at a young age.
In addition, residual scoliosis deformity after surgical intervention was between 10-15% in the older patient group (age > 15 years). Young patients have a greater potential for scoliosis remodeling after surgical intervention, and scoliosis may progress to a fixed deformity. Using three-dimensional computed tomography, Hussein et al. demonstrated that there were definitive vertebral deformities along the cervical spine in patients with long-standing CMT. Therefore, we suggest that it may be better to perform surgery on patients with CMT and scoliosis when the potential for growth is still present. Correction or reduction of secondary cervical scoliosis in patients with CMT depends on age and preoperative Cobb angle. Kim and all. published the first study to analyze the effect of age on the improvement of secondary scoliosis in CMT. In these cases, pain, degenerative arthritis, or spinal fusion may occur.
In some Asian countries, patients come late, after the age of 6. At this age, especially the parents of girls seek surgical treatment for aesthetic reasons. Lee and Minamitani reported that the results after this age are acceptable. Patients with congenital muscular torticollis may benefit from surgical treatment even in adulthood. Bipolar surgical sectioning of the sternocleidomastoid muscle should be considered even in adults with irreversible facial and skeletal deformities. Surgical intervention restores the range of neck movement and resolves head tilt; therefore, it can improve the quality of life. After establishing the RSPO surgical protocol, older children, adolescents, and adults were no longer operated on using the bipolar procedure or SCM muscle excision, but rather using this technique, which allowed distal disinsertion, intraoperative testing, digital detachment, anterior scalene section, or excision of perivascular fascial sclerosis. The results were significantly similar, and the complication rate decreased considerably, from 14% to 2%.

Ippolito and Tudisco, following a study on a group of 8 adult patients aged between 20 and 27, reported that facial asymmetry was not resolved, but neck movements improved in all patients. Coventry and Harris reported that the upper age limit for achieving good results in CMT surgery is 12 years. Sudesh et al., following the retrospective analysis of 14 patients over the age of 10 (between 10 and 19 years), state that bipolar relaxation in the treatment of CMT allows partial functional and aesthetic resolutions, labelled as good results. The authors’ surgical protocol involved complete sectioning of the clavicular end and “Z-shaped” elongation of the sternal end. The postoperative protocol included head traction for 3 weeks and active and passive physiotherapy.
It is possible for a patient with CMT to also suffer from clubfoot and developmental dysplasia of the hip (DDH) as related disorders. Between 2018 and 2024, we performed 12 foot arch reconstruction surgeries on elastic titanium rods passed transosseously through the radius of the first metatarsal for congenital rigid equinus foot in patients who had this malformation associated with CMT. However, in a group of patients with DDH, only 1.9% of patients were reported to have a deformed foot, which means that the association between DDH, deformed foot, and CMT is not significant. Our experience with hip ultrasound as a screening test for newborns and infants has proven its effectiveness in patients with CMT who also have DDH. Often, in this situation, the CMT-DDH association remains undetected. In countries where screening is not practiced, in order to avoid the occurrence of developmental dislocation of the hip, some authors confirm that patients with CMT should be screened for DDH.
Conclusions
Improving the treatment of this disease, given its high impact on a patient’s daily life, must focus not only on early diagnosis and the initiation of treatment in the first days after birth, but also on the implementation of appropriate rehabilitation techniques in specialized centers for the rehabilitation of newborns and infants. The recovery program should also include algorithms for teaching caregivers how to perform recovery at home, to facilitate accessibility for all children.
The Romanian School of Paediatric Orthopedics procedure improves standards of care in CMT treatment, reduces the risk of complications, and it is an optimal treatment alternative.
References
- Xiong Z, Zeng S, Chen H, Qiu X, Tang G, Tang Y, Tang S. Unique finding in congenital muscular torticollis: Clinic screening on the neck of one day old neonate and ultrasonographic imaging from birth through 3 years of follow-up. Medicine (Baltimore). 2019 Mar;98(11):e14794.
- Cheng JC, Tang SP, Chen TM, et al. The clinical presentation and outcome of treatment of congenital muscular torticollis in infants–a study of 1,086 cases. J Surg.2000;35:1091-1096
- Kim MW, Kim DY, Lee DW, Ryoo DH, Kim J, Jang DH. Concurrence of Congenital Muscular Torticollis and Congenital Torticollis Due to Other Anomalies: Two Case Reports. Front Pediatr. 2021 Oct 27;9:709616. doi: 10.3389/fped.2021.709616. PMID: 34778123; PMCID: PMC8578520.
- Agrawal D, Mohanty BB, Sarangi R, Kumar S, Mahapatra SK, Chinara PK. Study of incidence and prevalence of musculoskeletal anomalies in a tertiary care hospital of eastern India. J Clin Diagn Res. 2014;8:AC04-AC06. Doi: https://doi.org/10.7860/JCDR/2014/7882.4380
- Vanassi BM, Parma GC, Magalhaes VS, Santos ACCD, Iser BPM. Congenital anomalies in Santa Catarina: case distribution and trends in 2010–2018.Rev Paul Pediatr.2021 ;40:e2020331. DOI: 10.1590/1984-0462/2022/40/2020331
- Gliga V, Gozar H. Do tumors of the sternocleidomastoid muscle have diagnostic and therapeutic significance? Consensus Conference in Pediatric Orthopedics: Congenital Muscular Torticollis, Iasi 2000;12: 40-43
- Jaber MR, Goldsmith AJ. Sternocleidomastoid tumor of infancy: two cases of an interesting entity. Int J Pediatr Otorhinolaryngol. 1999 Mar 15;47(3):269-74. doi: 10.1016/s0165-5876(98)00186-4. PMID: 10321783.
- Kaplan SL, Coulter C, Sargent B. Physical Therapy Management of Congenital Muscular Torticollis. Evidence-Based Clinical Practice Guideline From the APTA Academy of Pediatric Physical Therapy. Pediatr Phys Ther. 2018 Oct;30(4):240-290. doi: 10.1097/PEP.0000000000000544. PMID: 30277962; PMCID: PMC8568067.
- Bredenkamp JK, Hoover LA, Berke GS, Shaw A. Congenital muscular torticollis. A spectrum of disease. Arch Otolaryngol Head Neck Surg. 1990 Feb;116(2):212-6. doi: 10.1001/archotol.1990.01870020088024. PMID: 2297419.
- Chen HX, Tang SP, Gao FT, Xu JL, Jiang XP, Cao J, Fu GB, Sun K, Liu SZ, Shi W. Fibrosis, adipogenesis, and muscle atrophy in congenital muscular torticollis. Medicine (Baltimore). 2014 Nov;93(23):e138. doi: 10.1097/MD.0000000000000138. PMID: 25415668; PMCID: PMC4616345
- Leung, A.K.C. (2009). Sternocleidomastoid Tumor of Infancy. In: Lang, F. (eds) Encyclopedia of Molecular Mechanisms of Disease. Springer 2009, Berlin, Heidelberg. https://doi.org/10.1007/978-3-540-29676-8_3349
- Vereanu D, Socolescu M, Bîscă N . Small tumor at the tendinomuscular junction: prognostic index in the occurrence of CMT. Consensus Conference in Pediatric Orthopedics: Congenital Muscular Torticollis, Iasi 1972;12:31- 37
- Pesamosca A, Puiu St et all. Small tumor at the tendinomuscular junction: prognostic index in the occurrence of CMT. Consensus Conference in Pediatric Orthopedics: Congenital Muscular Torticollis, Iasi 1972;12:6-11
- Fenton R, Gaetani SA. A pediatric epidemic: Deformational plagiocephaly/brachycephaly and congenital muscular torticollis. February 1, 2019 Contemporary PEDS Journal Vol 36 No 2 Issue 2
- Hwang, Lisa Ann Change-Yee, “Screening for Torticollis and Plagiocephaly: The Role of the Pediatrician” 2014. Loma Linda University Electronic Theses, Dissertations & Projects. 211. https://scholarsrepository.llu.edu/etd/211
- Moldovan Z, Soiu M, Trailescu M, Osakwe H. The effect of congenital muscular torticollis in children over 4 years of age who have not undergone surgery. Consensus Conference in Pediatric Orthopedics: Congenital Muscular Torticollis, Constanța 2004;11:31-33
- Burnei G, Ciobanu C, Neagoe P. Three cases of bilateral congenital muscular torticollis operated on in series. Consensus Conference in Pediatric Orthopedics: Congenital Muscular Torticollis, Brașov 1999;4:12-19
- Goția DG, Aprodu G, Gavrilescu SL. Results of physiotherapy treatment in children with congenital muscular torticollis. Consensus Conference in Pediatric Orthopedics: Congenital Muscular Torticollis, Iasi 2000;12: 7-11
- Michalska A, Śliwiński Z, Pogorzelska J et al. Congenital muscular torticollis – a proposal for treatment and physiotherapy. Med Rehabil. 2019;23(3):21-30. https://doi.org/10.5604/01.3001.0013.3728
- Canale ST, Griffin DW, Hubbard CN. Congenital muscular torticollis. A long-term follow-up. J Bone Joint Surg Am. 1982 Jul;64(6):810-6. PMID: 7085709
- Sönmez K, Türkyilmaz Z, Demiroğullari B, Ozen IO, Karabulut R, Bağbanci B, Başaklar AC, Kale N. Congenital muscular torticollis in children. ORL J Otorhinolaryngol Relat Spec. 2005;67(6):344-7. doi: 10.1159/000090046. Epub 2005 Dec 1. PMID: 16327275
- Țepeneu P, Tepeneu N Junior, Lazea St. Multicenter Study in the period 1986-1987 (Bucharest, Timisoara, Cluj, Iasi, Craiova, Constanta, Targu Mures, Brasov); Evolution of congenital muscular torticollis treated conservatively up to 1 year of age. Consensus Conference in Pediatric Orthopedics: Congenital Muscular Torticollis, Timisoara 1998;12:2-11
- Borgeat A, Blumenthal S. Chapter 25. Interscalene Brachial Plexus Block. In: Hadzic A, ed. NYSORA Textbook of Regional Anesthesia and Acute Pain Management. The McGraw-Hill Companies; 2007.
- Banculescu (Coșofreț) M. Doctoral Thesis; Postoperative Pain Management in Pediatric Surgery. Constanta. 2011: 155-160. Ovidius University Library Constanta