





Conservative Treatment for Scheuermann’s Kyphosis Case Study
Conservative Treatment of a Typical (Type 1) Scheuermann’s Kyphosis: A Case Report
Fleming, P¹, Dr Potts, MABJ²
- Senior MSK Clinician, The Dorsi Spinal Institute,
- Clinical Director, The Dorsi Spinal Institute
OPEN ACCESS
PUBLISHED:31 March 2025
CITATION: Fleming, P. and Dr Potts, MABJ., 2025. Conservative Treatment of a Typical (Type 1) Scheuermann’s Kyphosis: A Case Report. Medical Research Archives, [online] 13(3).
https://doi.org/10.18103/mra.v13i3.6396
COPYRIGHT:© 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i3.6396
ISSN 2375-1924
ABSTRACT
Background:
Scheuermann’s Kyphosis is a developmental postural deformity seen more often in men than in women and is associated with increased degeneration of the spine and sequelae including reduced quality of life and pulmonary dysfunction. There is limited available high-quality evidence for the non-operative treatment of this condition in the adult population.
Objective:
To describe the successful case of conservative treatment of Scheuermann’s Kyphosis in an adult male office worker using thoracic extension traction, spinal manipulative therapy and a home exercise plan.
Clinical Features:
A 52-year-old male office worker presented to the clinic with chronic lower back pain, stiffness and reduced active range of movement in the thoracic and lumbar spine. A diagnosis of Scheuermann’s Kyphosis was made following lateral and posterior-anterior x-rays of the thoracic spine with a significant sagittal imbalance.
Intervention & Outcome:
The patient was treated with thoracic extension traction, a home exercise plan and a course of spinal manipulative therapy combined with soft tissue work. A clinically significant reduction in thoracic kyphosis was achieved, bringing his curvature into a normal range, along with a lasting reduction in pain and improvements to his quality of life.
Conclusion:
Although there is limited research on the treatment of Scheuermann’s Kyphosis in adults, and what research there is on treating structural thoracic hyperkyphosis is weak, we have found that the methods used herein have proven to be an effective treatment plan.
Keywords:
Scheuermann’s; hyperkyphosis; kyphosis; posture; scoliosis
INTRODUCTION
BACKGROUND
Sagittal plane postures like slouching, forward head posture or sway back postures have documented effects on physical and cognitive function, impacting how we move and interact with the world and each other, our perception, memory, fatigue and mood²²–²⁷. Whilst posture has often been shown to be a window into a person’s mental and physical health, it has also been demonstrated to be a “two-way street” in that adopting certain postures can invoke a change in physical, emotional and psychological state, exacerbating feelings of hopelessness or helplessness²², altering breathing mechanics²⁶, impact brain function²⁵ and negatively impacting mobility and balance, potentially leading to an increased risk of falls, though this may only be relevant for older populations (≥65)²⁷ and may not effect younger people as much²⁸–²⁹. In a study by Peper et al., (2017)²³ it was reported that those who adopted an upright posture reported higher self-esteem, better mood and lower fear than those who slouched, and Nair et al., (2015)²⁴ found that adopting an upright seated posture brings about improvements in mood and resilience to stress. It is therefore important to address skeletal imbalances which contribute to these changes in posture such as a thoracic hyperkyphosis.
Kyphosis refers to the natural convex curvature of the thoracic spine in the sagittal plane and is typically considered ‘normal’ where it does not exceed 20–40°², though it should be noted that more recent investigations have suggested this range is age related and can vary significantly from <40° in the under-40s to >60° in the over-60s¹. Where a thoracic kyphosis exceeds 40° the curvature is described as a hyperkyphosis, a higher degree of hyperkyphosis is associated with a risk of falls, degenerative changes, cardiopulmonary dysfunction and poor quality of life²–⁵.
Hyperkyphosis is classified as either structural (rigid) or non-structural (flexible). Structural kyphosis involves morphological changes to the bones and soft tissues and is less easily corrected, whereas non-structural kyphosis (e.g., postural or “functional” kyphosis) can often be improved with exercise and lifestyle modifications⁶. There are many types of structural kyphosis with many different causes ranging from congenital to degenerative⁷–⁹. Scheuermann’s kyphosis (SK) is a common type of developmental structural hyperkyphosis usually occurring in adolescence and is characterised by anterior wedging of at least 5° in three or more consecutive vertebrae¹⁰. Although the precise cause of SK remains unknown, it is thought to be caused by discordant mineralisation and ossification of the vertebral endplates during growth⁶, along with several other factors acting together. The prevalence of SK is between 0.4–8%, with a male to female ratio of between 2:1 and 7:1⁶. Non-structural or ‘postural’ hyperkyphosis also usually begins to be seen during adolescence, with more females than males being affected¹¹. In general, hyperkyphosis increases with age, especially after the age of 40 with females seeming to have a greater rate of increase during menopause¹¹, though after the age of 50 an average increase of around 3° per decade can expect to be seen in both males and females¹².
Clinical evidence surrounding the non-surgical correction or reduction of pathological thoracic hyperkyphosis is limited in the literature. This case details the steps taken to achieve a significant reduction in thoracic kyphotic curvature of an adult patient with a Scheuermann’s hyperkyphosis, utilising methods which should be easily adaptable to clinicians of various backgrounds and with varying amounts of equipment.
EXAMINATION & CLASSIFICATION
With SK, patients typically present due to progressive deformity, cosmetic concerns, or pain. The most obvious sign seen is the rounded back and forward head posture due to the excessive forward curvature of the spine, especially during an Adam’s forward bend test where the curvature will disappear with a postural hyperkyphosis, but is increased with SK¹³. There may also be skin pigmentation changes around the apex of the curve and often bruising is seen due to the rigid nature of the kyphosis¹⁴. Flexibility testing (forced flexion/extension) can help to differentiate between a postural and rigid hyperkyphosis, in SK, the kyphotic deformity is rigid¹³.
Standing posterior-anterior (PA) and lateral radiographs are essential in aiding diagnosis⁶. Degree of thoracic kyphosis and vertebral body wedging are measured using the Cobb method on the lateral view and sagittal balance can be measured by drawing a plumb-line from C7 to the sacral endplate. Other findings may include endplate irregularities, reduced disc heights, Schmorl’s nodes and other increased degenerative changes⁶. SK is classified into two main types: Type 1 (Typical), where the apex of the deformity is located in the thoracic spine (T7-T9), associated with a compensatory hyperlordosis of the cervical and lumbar spine; and Type 2 (Atypical), where the apex of the deformity is in the thoracolumbar or lumbar spine, which is most often seen in athletic adolescent males and is the most likely to progress⁶. Neurological symptoms are rare but where they are present or for atypical cases an MRI is indicated¹³.
Case Presentation
CLINICAL FEATURES
A 52-year-old male office worker presented to the clinic with a complaint of chronic lower back pain without any radicular symptoms, which had been worsening for the past 6-months since he had moved house and had not been receiving regular chiropractic treatment. The patient reported that his pain was present at all times at an intensity of 3/10 on the Visual Analogue Scale (VAS), with intermittent periods of more intense pain at 9/10 (VAS) intensity. His pain was worsened with prolonged household activities which required increased forward flexion of the spine and heavy lifting and was reduced with rest. The patient also reported a stiffening of the upper back between the shoulder blades and of the neck, which they believed to be related to their posture whilst working sat at a desk. The patient stated that they believed that their symptoms would never improve unless they received regular hands-on treatment for the rest of their life.
PHYSICAL EXAMINATION
Postural assessment revealed a sway back posture in the sagittal view, with a significant thoracic kyphosis and lumbar lordosis. Some mild right lateral shifting in the coronal view was noted in the thoracic spine, with an associated mild left thoracic tilt and left thoracic rotation.
In a movement examination, the patient was experiencing pain and stiffness in flexion and extension of the whole spine, with decreased active range of motion particularly into extension. We observed that the flexion predominantly occurred in the thoracic spine, with the lumbar spine appearing to only contribute minimally to the movement, whereas the extension occurred predominantly at the pelvis, with neither the lumbar nor thoracic regions appearing to contribute much relative motion. A moderate loss of active range of motion was also present in the cervical spine in all directions, but particularly into lateral flexion bilaterally.
Palpation revealed muscular tension and loss of segmental motion in the thoracic spine, with pain noted in particular at C2/3, T2-4, T10 and L4. With mild right rotation at the lumbar spine and a left counter-rotation at the thoracic spine, consistent with the lateral shifting observed in the standing postural assessment.
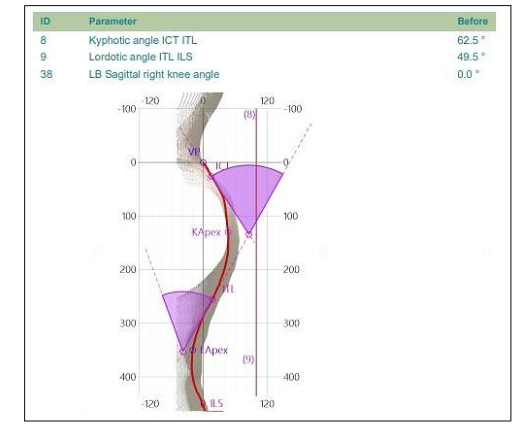
We evaluated the patient further using a Spine3D LiDAR (Light Detection and Ranging) scan to more closely estimate the curvature of the spine in the thoracic and lumbar regions, which indicated a thoracic kyphosis of 62.5° (Fig. 1). This system, from Sensor Medica (Sensor Medica, Guidonia Montecelio, Rome, Italy), has been shown to be an effective tool for estimating Cobb angles and can be a more ethical method for tracking curve progression over time, over the use of repeat x-rays¹⁶. Plain digital lateral and posterior-anterior x-ray images were then taken (Figs. 2 & 3) to accurately assess the kyphotic angle of the thoracic spine.
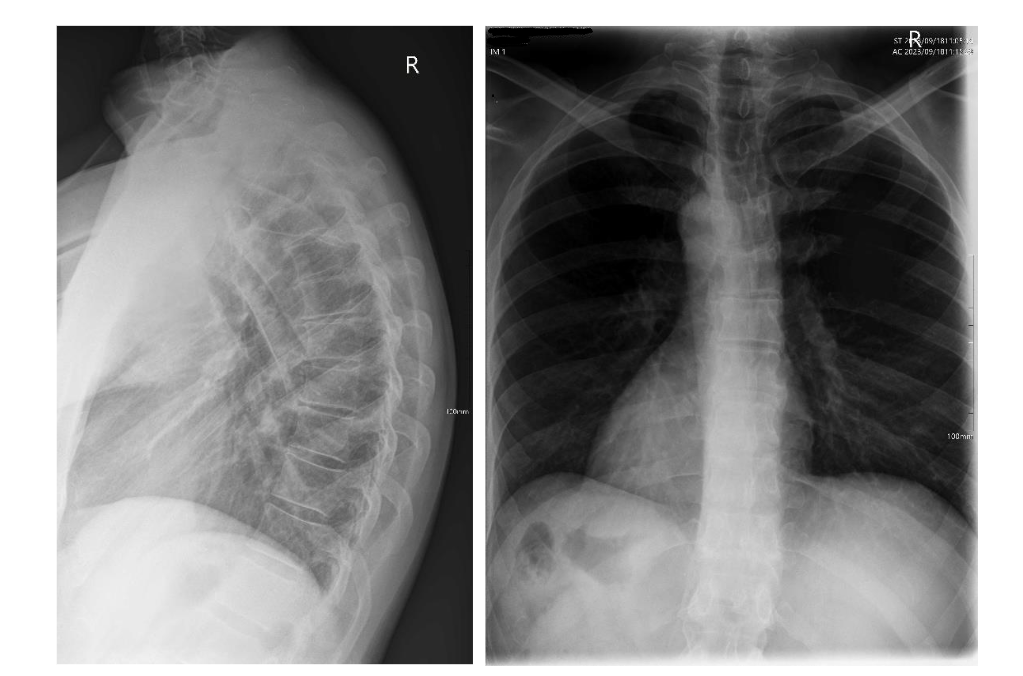
Biomechanical radiographic analysis of the thoracic spine revealed an excessive thoracic kyphosis of 63.39° as measured from the T1 superior endplate to the T12 inferior endplate, with the apex occurring at T7/8. Vertebral wedging of greater than 5° occurred at T7, T8 and T9. Other radiographic features of note were; reduced disc spaces at T5/6, T6/7 and T8/9; degenerative changes at the superior endplates of T4, T6, T7 and T9; and degenerative changes at the inferior endplates of T6, T7 and T8. Other minor changes noted were a mild lateral curvature of the thoracic spine, measured at a Cobb angle of 6°.
On the basis of the above findings, a diagnosis of Typical (Type 1) Scheuermann’s Kyphosis was delivered verbally to the patient, with explanation about the disease and a discussion around the potential interventions including doing nothing, surgical options and conservative treatment.
A conservative treatment plan was decided upon consisting of hands-on care, CBP® thoracic-extension traction, exercise rehabilitation and lifestyle changes, which is detailed below.
Intervention and Outcome
The patient started care on 18/09/23 at a recommended frequency of 2–3 visits per week, initially consisting of primarily hands-on treatment involving spinal manipulative therapy to the cervical, thoracic and lumbar regions, aimed at reducing the patients’ symptoms and increasing mobility of the thoracic and lumbar spine to later aid in the spinal traction and exercise rehabilitation.
Movement coaching began from session 6 onwards. The aim of this coaching was to help the patient increase their proprioceptive awareness surrounding posture and movement, and to improve their general health and mobility. The movements coached over the course of the patient’s treatment consisted of:
-
supine and seated spinal motor control exercises such as lumbar spine extension–flexion patterning (pelvic rolls) and thoracolumbar rotation
-
thoracic extension and lower trap activation movements such as prone YTW arm lifts
-
4-point kneeling movements such as the cat-cow and bird-dog
-
general exercise and movement advice around movement frequency and variability, being advised to do up to 5-minutes of some form of movement for every 30-minutes of continuous sitting/inactivity
After 22 sessions of the combined hands-on treatment and movement coaching, mobility of the spine and patient symptoms had improved enough that it was deemed suitable to begin the CBP® thoracic-extension traction protocol. A foam wedge was provided to the patient to be placed longitudinally on the thoracic spine with the patient lying supine on top of it in a crook knee position, with their arms externally rotated and held out at a roughly 45° angle from their torso. The patient trialled this in-clinic for 4–6 minutes, before being asked to continue at home. The patient was instructed to increase the time by 2 minutes per day until they reached 20 minutes, which research suggests is sufficient to create ligamentous creep, at which point they were to spend 20 minutes on it every day.
From session 23 onwards the patient began supervised exercise and posture rehabilitation sessions. Following introductory sessions using a precision thoracic wedge placed at T8 for up to 6 minutes, suspended two-way thoracic-extension traction for up to 20 minutes was begun from session 28 and lasted for 12 sessions.
From session 30 onwards, supervised exercise sessions began, consisting of:
-
pectoralis major and minor stretches
-
latissimus dorsi stretches
-
hamstring stretches
-
mirror image® thoracic extension exercises to strengthen the thoracic extensor complex
-
auto-elongation posture correction exercises
The patient was instructed to continue the exercises at home and was shown progressions to aid in their self-management outside of the clinic.
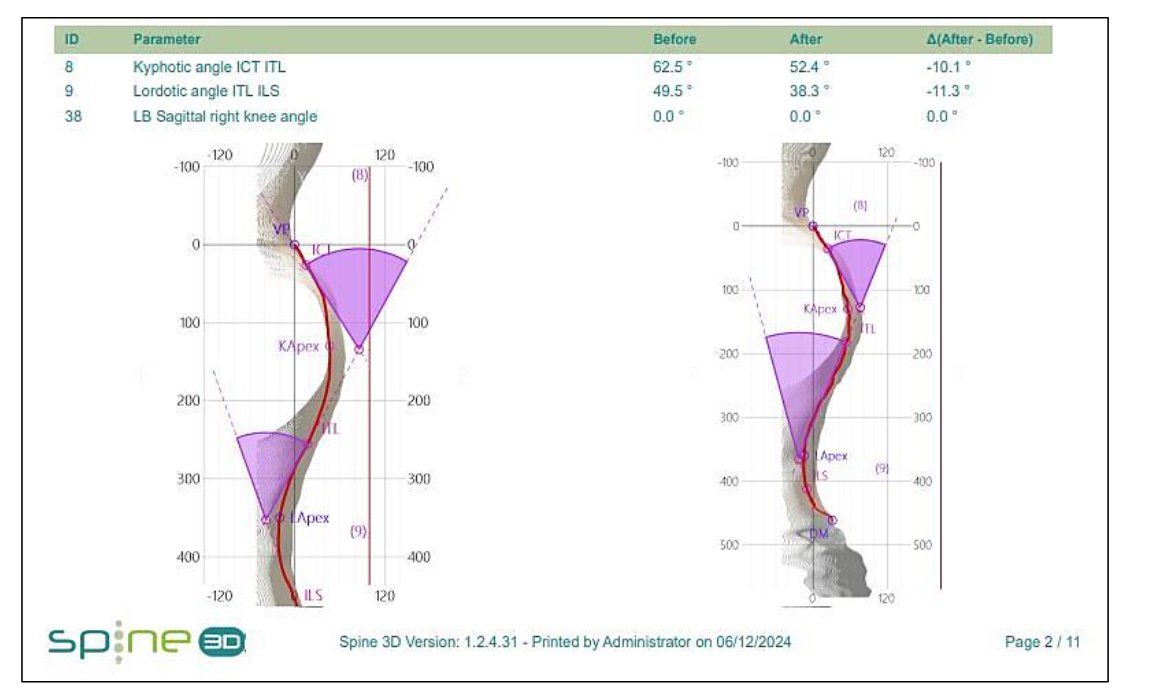
At session 40, a repeat Spine3D LiDAR scan was conducted to assess the amount of correction achieved to that point. The results indicated a significant change from 62.5° measured on their consultation to 52.4°, an improvement of 10.1°.
(Fig. 4). With this change, the patient’s thoracic kyphosis was now in a more ‘normal’ range for their age¹. The patient also reported a significant reduction in their symptoms (e.g. 1–3/10 VAS from 3–9/10), and noted an increased desire to engage with movement more often throughout their day. Happy with their progress, session frequency was reduced to monthly check-ups and the patient advised to continue diligently with their home exercise plan to prevent any collapse into their kyphotic curvature.
Discussion
This case demonstrates the reduction of thoracic hyperkyphosis posture with the resolution of spinal pain and self-reported limitations in active range of motion in a 52-year-old office worker, utilising both novel and well-established rehabilitation protocols including CBP® thoracic-extension traction and a home exercise programme.
Currently, there is not much scientific data on the effective non-operative management of Scheuermann’s hyperkyphosis²⁰. Out of the traditional conservative treatment options, auto-elongation and postural control exercises are reported amongst clinicians to be the most used techniques²⁰, though most of the trials used to evaluate methods have been reported as being underpowered/small in scale²¹.
Spinal bracing can be an effective option for non-surgical curve correction with conditions like SK and scoliosis, particularly when this is done prior to reaching skeletal maturity³²–³³. For adults with SK, bracing can still be an option, however, rather than the goal being correction of the curvature, the emphasis is placed on preventing progression and reducing those symptoms and sequalae associated with an increased thoracic kyphosis³⁴–³⁵.
Conclusion
Much of the current guidelines for the treatment and correction of structural thoracic hyperkyphosis focuses on children and adolescents diagnosed with SK. Given that age-related increases in thoracic kyphosis can be significant¹, the severity of thoracic hyperkyphosis is linked with increasing rates of
degeneration, dysfunction and poor quality of life¹–⁵, and that surgical correction is typically only advised for more advanced cases³⁰–³¹, the non-operative correction of thoracic hyperkyphosis in adults is a research area that we believe requires more focus, and the methods used in this case are worth investigating in a robust and controlled study.
Consent
All authors declare that written informed consent was obtained from the patient prior to the publication of this case report.
REFERENCES
1. Zappalá, M., Lightbourne, S., & Heneghan, N. R. (2021). The relationship between thoracic kyphosis and age, and normative values across age groups: a systematic review of healthy adults. Journal of orthopaedic surgery and research, 16(1), 447.
2. Roaf, R., (1960). Vertebral growth and its mechanical control. The Journal of bone and joint surgery. British volume, 42-B, 40–59.
3. Koelé, M. C., Lems, W. F., & Willems, H. C. (2020). The Clinical Relevance of Hyperkyphosis: A Narrative Review. Frontiers in endocrinology, 11, 5.
4. Katzman, W. B., Wanek, L., Shepherd, J. A., & Sellmeyer, D. E. (2010). Age-related hyperkyphosis: its causes, consequences, and management. The Journal of orthopaedic and sports physical therapy, 40(6), 352–360.
5. Roghani, T., Zavieh, M. K., Manshadi, F. D., King, N., & Katzman, W. (2017). Age-related hyperkyphosis: update of its potential causes and clinical impacts-narrative review. Aging clinical and experimental research, 29(4), 567–577.
6. O’Donnell, J. M., Wu, W., Youn, A., Mann, A., & Swarup, I. (2023). Scheuermann Kyphosis: Current Concepts and Management. Current reviews in musculoskeletal medicine, 16(11), 521–530.
7. Montgomery, S. P., & Hall, J. E. (1982). Congenital kyphosis. Spine, 7(4), 360–364.
8. Mizobuchi, S., Tadokoro, N., Takaya, S., Kiyasu, K., Takemasa, R., & Ikeuchi, M. (2020). Nontraumatic Spondylolisthesis of the Axis with Cervical Kyphosis. Case reports in orthopedics, 2020, 6859474.
9. McCarthy, J., & Davis, A. (2016). Diagnosis and Management of Vertebral Compression Fractures. American family physician, 94(1), 44–50.
10. Lowe T. G. (2007). Scheuermann’s kyphosis. Neurosurgery clinics of North America, 18(2), 305–315.
11. Singla, D., & Veqar, Z. (2017). Association Between Forward Head, Rounded Shoulders, and Increased Thoracic Kyphosis: A Review of the Literature. Journal of chiropractic medicine, 16(3), 220–229.
12. Kobayashi, T., Atsuta, Y., Matsuno, T., & Takeda, N. (2004). A longitudinal study of congruent sagittal spinal alignment in an adult cohort. Spine, 29(6), 671–676.
13. Wood, K. B., Melikian, R., & Villamil, F. (2012). Adult Scheuermann kyphosis: evaluation, management, and new developments. The Journal of the American Academy of Orthopaedic Surgeons, 20(2), 113–121.
14. Sebaaly, A., Farjallah, S., Kharrat, K., Kreichati, G., & Daher, M. (2022). Scheuermann’s kyphosis: update on pathophysiology and surgical treatment. EFORT open reviews, 7(11), 782–791.
15. Oakley, P. A., Harrison, D. D., Harrison, D. E., & Haas, J. W. (2005). Evidence-based protocol for structural rehabilitation of the spine and posture: review of clinical biomechanics of posture (CBP) publications. The Journal of the Canadian Chiropractic Association, 49(4), 270–296.
16. Potts, Dr. M. ABJ. (2024). LiDAR and X-ray: A Retrospective Comparison of Spinal Alignment. Medical Research Archives, 12(9).
17. Oliver, M. J., & Twomey, L. T. (1995). Extension creep in the lumbar spine. Clinical biomechanics (Bristol, Avon), 10(7), 363–368.
18. Weiss, H. R., Dieckmann, J., & Gerner, H. J. (2002). Effect of intensive rehabilitation on pain in patients with Scheuermann’s disease. Studies in health technology and informatics, 88, 254–257.
19. Fisk, J. W., & Baigent, M. L. (1981). Hamstring tightness and Scheuermann’s disease a pilot study. American journal of physical medicine, 60(3), 122–125.
20. De Mauroy, J., Weiss, H., Aulisa, A., Aulisa, L., Brox, J., Durmala, J., Fusco, C., Grivas, T., Hermus, J., Kotwicki, T., Le Blay, G., Lebel, A., Marcotte, L., Negrini, S., Neuhaus, L., Neuhaus, T., Pizzetti, P., Revzina, L., Torres, B., Van Loon, P., … Zaina, F. (2010). 7th SOSORT consensus paper: conservative treatment of idiopathic & Scheuermann’s kyphosis. Scoliosis, 5, 9.
21. Kado D. M. (2009). The rehabilitation of hyperkyphotic posture in the elderly. European journal of physical and rehabilitation medicine, 45(4), 583–593.
22. Wilkes, C., Kydd, R., Sagar, M., & Broadbent, E. (2017). Upright posture improves affect and fatigue in people with depressive symptoms. Journal of behavior therapy and experimental psychiatry, 54, 143–149.
23. Peper, E., Lin, I., Harvey, R., & Perez, J. (2017). How Posture Affects Memory Recall and Mood. Biofeedback. 45. 36-41.
24. Nair, S., Sagar, M., Sollers, J., 3rd, Consedine, N., & Broadbent, E. (2015). Do slumped and upright postures affect stress responses? A randomized trial. Health psychology: official journal of the Division of Health Psychology, American Psychological Association, 34(6), 632–641.
25. Jung, J. Y., Lee, Y. B., & Kang, C. K. (2024). Effect of Forward Head Posture on Resting State Brain Function. Healthcare (Basel, Switzerland), 12(12), 1162.
26. Tassani, S., Chaves, P., Beardsley, M., Vujovic, M., Ramírez, J., Mendoza, J., Portero-Tresserra, M., González-Ballester, M. A., & Hernández-Leo, D. (2024). Breathing, postural stability, and psychological health: a study to explore triangular links. Frontiers in bioengineering and biotechnology, 12, 1347939.
27. Koelé, M. C., Willems, H. C., Swart, K. M. A., van Dijk, S. C., Lips, P., de Groot, L. C. P. G. M., van der Cammen, T. J. M., Zillikens, M. C., van Schoor, N. M., & van der Velde, N. (2022). The association between hyperkyphosis and fall incidence among community-dwelling older adults. Osteoporosis international: a journal established as result of cooperation between the European Foundation for Osteoporosis and the National Osteoporosis Foundation of the USA, 33(2), 403–411.
28. Youssef, H., & Yildiz, A. (2023). Could kyphotic posture disturb body balance in young healthy population? Journal of bodywork and movement therapies, 34, 13–18.
29. Eum, R., Leveille, S. G., Kiely, D. K., Kiel, D. P., Samelson, E. J., & Bean, J. F. (2013). Is kyphosis related to mobility, balance, and disability?. American journal of physical medicine & rehabilitation, 92 (11), 980–989.
30. Sardar, Z. M., Ames, R. J., & Lenke, L. (2019). Scheuermann’s Kyphosis: Diagnosis, Management, and Selecting Fusion Levels. The Journal of the American Academy of Orthopaedic Surgeons, 27 (10), e462–e472
31. Diaremes, P., Braun, S., & Meurer, A. (2022). Morbus Scheuermann [Scheuermann’s disease]. Der Orthopade, 51(4), 339–348
32. Huq, S., Ehresman, J., Cottrill, E., Ahmed, A. K., Pennington, Z., Westbroek, E. M., & Sciubba, D. M. (2019). Treatment approaches for Scheuermann kyphosis: a systematic review of historic and current management. Journal of neurosurgery. Spine, 32( 2), 235–247.
33. Pizzutillo P. D. (2004). Nonsurgical treatment of kyphosis. Instructional course lectures, 53, 485–491.
34. Tribus C. B. (1998). Scheuermann’s kyphosis in adolescents and adults: diagnosis and management. The Journal of the American Academy of Orthopaedic Surgeons, 6(1), 36–43.
35. O’Donnell, J. M., Wu, W., Youn, A., Mann, A., & Swarup, I. (2023). Scheuermann Kyphosis: Current Concepts and Management. Current reviews in musculoskeletal medicine, 16(11), 521–530.