





Contraceptive Use and Migraine in Women: Key Insights
Contraceptive use in women with migraine
S. K. Afridi1
- Corresponding author Dr Shaiza Afridi, Consultant Neurologist, Guys and St Thomas NHS Trust, London, UK
OPEN ACCESS
PUBLISHED: 30 April 2025
CITATION: Afridi, S.K. (2025). Contraceptive use in women with migraine. Medical Research Archives, [online] 13(4). http://doi.org/10.18103/mra.v13i4.623
COPYRIGHT: This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
DOI: https://doi.org/10.18103/mra.v13i4.6371
ISSN 2375-1924
Abstract
Migraine affects approximately 18% of women in childbearing age. There are a number of questions and concerns surrounding the use of contraceptives in women with migraine. This review examines the effects of various contraceptive methods and analyzes the safety concerns, in particular reviewing the existing literature regarding the safety of estrogen containing contraceptives in women with migraine.
Keywords
migraine, contraceptives, estrogen, safety, women
Introduction
Hormonal methods are either “combined”, which involves a combination of estrogen and progestogen or progestogen only. The most widely used combined contraceptive formulation is the oral contraceptive pill. There is also a vaginal ring or a patch but these are much less commonly used. With regards to estrogen only methods there is only one version available, the intrauterine device, which releases hormones.
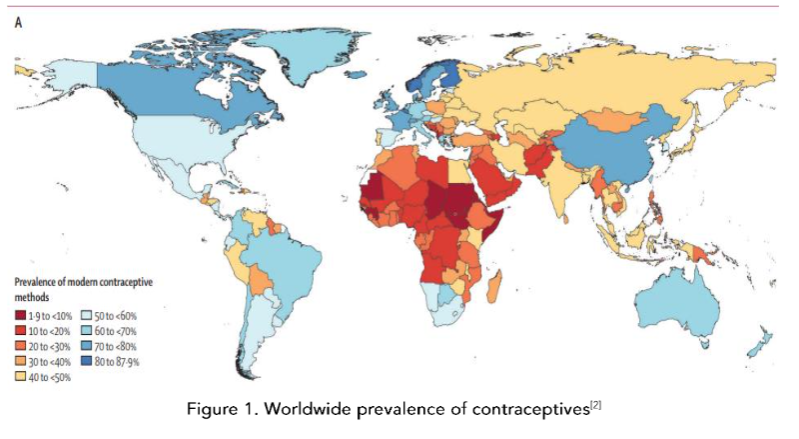
According to the Figure 1 below, the use of contraception in women with migraine is often an issue of contentious debate and the guidelines vary and are constantly changing. This review aims to provide some context and clarification around these issues.
Methods of contraception
Hormonal methods are either “combined”, which involves a combination of estrogen and progestogen or progestogen only. The most widely used combined contraceptive formulation is the oral contraceptive pill. There is also a vaginal ring or a patch but these are much less commonly used. With regards to estrogen only methods there is only one version available, the intrauterine device, which releases hormones.
There are estrogen receptors located in the brain in areas that are thought to be important in migraine, such as the hypothalamus, pons, periaqueductal grey, locus coeruleus. In animal studies estrogen triggers cortical spreading depression which is thought to be the pathophysiological correlate of migraine aura. When a woman starts an estrogen containing contraceptive pill or initiates hormone replacement therapy or is pregnant, there is an estrogen surge and this can sometimes result in aura precipitating migraine.
![Figure 2. Menstrual and perimenopausal susceptibility to migraine. (Onello et al [7])](/pdf-to-wp-converter/uploads/images/contraceptive-use-migraine-women-figure-2.png)
The effect of contraceptives on migraine
There was no difference between the levels of PACAP between the menstrual cycle and the different phases of the menstrual cycle in women with migraine on combined contraceptives; thus, it is not very informative. In women with migraine with aura there may be an exacerbation of migraine with the combined contraceptive pill, which is perhaps linked to the effect of estrogen on cortical spreading depression.
When one is on the combined oral contraceptive pill, she will usually take it for 21 days and then have a 7-day break, during which she will have her menstrual period, and during that time she may have an increased risk of migraine. The cycling can be difficult to manage.
What are the safety concerns?
The safety concerns for migraines regarding oral contraceptives revolve around two issues; venous thromboembolism and the risk of stroke. The former is an issue regardless of migraine. The combined contraceptive pill does increase the risk of venous thromboembolism and the progestin-only contraceptive pill does not. The intrauterine contraceptive device also does not.
![Figure 3. Contraceptive methods and their effects in migraine. Adapted from Lohuisen et al [24]](/pdf-to-wp-converter/uploads/images/contraceptive-use-and-migraine-women-figure-3.png)
Conclusion
The current guidance does not take into account individual risk factors for women with migraine with aura. Further research is required to accurately assess the risk of stroke in migraines using current formulations of contraceptives and their safety in women with migraine with aura.
References
- Jensen R, Stovner LJ. Lancet Neurol 2008;7(4): 354-61 doi:10.1016/S1474-4422(08)70062-0 [published Online First: Epub Date].
- Haakstad A, Angulo O, Irwin CMS, et al. Measuring contraceptive method mix, prevalence, and demand satisfied by age and marital status in 204 countries and territories, 1970-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet 2022;400(0134):2985-3297 doi: 10.1016/S0140-6736(22)00439-X [published Online First: Epub Date].
- Sarajian A, Winterstein A, Cristofoletti R, Vozmediano V, Schmidt B, Vrouvtsas J. Realworld effect of a combined oral contraceptive on stroke: A case-control study using the UK General Practice Research Database. Stroke 2020;51(7):1574-80 doi:10.1161/STROKEAHA.120.030197 [published Online First: Epub Date].
- McGregor EA. Oestrogen and attacks of migraine. Headache Pain 2018;11(1):21 doi:10.1186/s10194-018-0852-4 [published Online First: Epub Date].
- Storch E, Overeem L, Terwindt H, et al. PACAP-38 and sex hormones in women with migraine: exploratory analysis of a cross-sectional, matched cohort study. J Headache Pain 2024;25(1):98 doi:10.1186/s10194-024-01804-4 [published Online First: Epub Date].
- Raffaelli B, Storch E, Overeem L, et al. Sex Hormones and Calcitonin Gene-Related Peptide in Women With Migraine: A Cross-sectional, Matched Cohort Study. Neurology 2023;100(12):1825-35 doi: 10.1212/WNL.0000000000001208 [published Online First: Epub Date].
- Batur P, Piya M, Bucklan J, et al. Ischemic stroke in young women: a nested case-control study using the UK General Practice Research Database. Stroke 2023;54(6):1831-40 doi:10.1161/STROKEAHA.122.018740 [published Online First: Epub Date].
- Nightingale AL, Farmer ROB. Ischemic stroke in young women: a nested case-control study using the UK General Practice Research Database. Stroke 2020;51(7):1574-80 doi:10.1161/STROKEAHA.120.030197 [published Online First: Epub Date].
- UK MEDICAL ELIGIBILITY CRITERIA FOR CONTRACEPTIVE USE: The effect of hormonal contraceptives and risk of stroke in women with migraine. J Headache Pain 2017;18(1):10 doi:10.1016/j.jhpn.2017.01.004 [published Online First: Epub Date].