





COPD Treatment Outcomes: Non-Invasive Ventilation Study
Are patients with Chronic Obstructive Pulmonary Disease treated according to guidelines with non-invasive ventilation within 30-day mortality rates? Results of an internal audit.
Introduction
Chronic obstructive pulmonary disease (COPD) is a global health problem and one of the leading causes of morbidity and mortality worldwide.¹ Danish prevalence studies have estimated that there are around 400.000 persons with COPD in Denmark.² The hospitalizations and total expenditure is a considerable burden on the publicly financed health-care system,³ and the Danish health-care authorities initiated the Danish Clinical Register of COPD (DrCOPD) in 2008 with the purpose to monitor number of COPD admissions, implementation of non-invasive ventilation (NIV) and register 30-day mortality rates among other qualitative out-patient initiatives.⁴ These reports have been published annually, and data have been grouped in the five Danish regions and also in the different sites/hospitals enabling reflection on practice.
Due to the COVID-19 pandemic, the Danish register for COPD did not publish reports for two years. The first report, after the pandemic with data from 2022, revealed fewer COPD admissions nationally (10.174 admissions). At the local university hospital (Odense University Hospital), in all 337 patients were admitted with an exacerbation of COPD with a 30-day mortality rate of 26%,⁵ compared to the national 30-day mortality rate of 17%. Due to the difference in mortality rate, we decided to repeat an internal audit in the next year.
In 2023, DrCOPD reported 15.174 admissions due to an acute exacerbation of COPD in Denmark,⁵ compared to approximately 20.000 acute hospitalizations annually in the last decade.⁴˒⁶
In the Region of Southern Denmark, reasons for reduction in hospitalizations have been attributed among other things implementation of COPD health plans: defining communication methods between the sectors on responsibilities of COPD treatment, daily care, rehabilitation, and palliation between municipalities, General Practitioners (GP), and hospitals.⁷ Secondly, the municipalities have implemented telemedicine as a platform between specialist caregivers and patients with severe COPD for monitoring patients at home.⁸
We have previously documented, that reorganization of the hospital admissions with the newly established emergency department in 2012 (where the patients were initially treated and observed as an outpatient), lowered the admission rate for patients admitted with COPD in exacerbation with 24% (from 393 to 300 in the second half of 2012), but the 30-day mortality rate remained 10%.⁹ Ultimately, Long Term (LT) NIV treatment to patients with COPD, chronic hypercapnia, and a history of readmissions has been implemented as a palliative add-on treatment.
The primary aim of this audit was to evaluate if patients admitted with COPD in exacerbation were treated with NIV as add-on treatment to standard medical treatment according to guidelines, and the secondary aim was to characterize patients who died.
Hypothesis: Treatment of patients with COPD in exacerbation and treatment with NIV is initiated according to guidelines, and the admitted cohort of COPD patients are older contributing to the higher mortality rate.
Methods
ORGANIZATION OF NIV TREATMENT OF COPD PATIENTS AT OUH:
The university hospital serves a population of 230.000 inhabitants.
Patients with suspected COPD exacerbation were initially assessed medically at the Emergency Department.¹⁰ Patients fulfilling NIV criteria started NIV treatment on site, were admitted either to the Emergency Department Ward and later referred to or directly referred to the Department of Respiratory Medicine, unless Intensive Care observation was required, and weaning of treatment was performed according to local guidelines. See Table 1 for NIV criteria.
Table 1. Criteria for NIV indication for patients with COPD in exacerbation
No improvement of condition after initiation of standard treatment including oxygen therapy, bronchodilators, systemic corticosteroids and, if necessary, antibiotics
pH < 7.35
PaCO₂ > 6 kPa
One of the following:
- Exacerbation of dyspnoea
- Respiratory rate > 25
- PaO₂ < 7 kPa without oxygen therapy
Abbreviations: NIV = non-invasive ventilation; COPD = Chronic Obstructive pulmonary disease; pH = Potential of hydrogen; PaCO₂ = Partial pressure of carbon dioxide; kPa = kilopascal; PaO₂ = Partial pressure of oxygen.
STUDY SAMPLE:
In this retrospective cohort study, all patients discharged from OUH, with the discharge diagnosis COPD between 01.01.2023 and 31.12.2023, were retrieved from the Patient Admission System. The following international classification of diseases (ICD)-10 codes were used: COPD (DJ44) as primary diagnosis or respiratory insufficiency (DJ96), pneumonia (DJ13-DJ18), Corona Virus Disease 2019 (DB34ZA, DB972A, DZ038PA1) as primary diagnosis combined with COPD (DJ44) as a secondary diagnosis.
Patients admitted at other hospitals than OUH, or transferred from other hospitals to OUH, were excluded. Patients discharged due to other reasons than COPD in exacerbation, were excluded.
DATA COLLECTION:
Data was retrieved retrospectively from electronic medical journals. If a patient had multiple admissions at OUH during 2023, the data from the first admission was registered. Baseline data registered were: age, gender, height, weight, body mass index (BMI), number of hospital admissions due to COPD in exacerbation in 2023, COPD diagnosed at a primary or secondary health sector, use of long-term oxygen therapy (LTOT), treatment limitations, prehospital treatment in association to hospital admission, indication for NIV according to guidelines, received NIV, 30-day mortality, spirometry (forced expiratory volume in the first second (FEV₁) in litres and percentage, forced vital capacity (FVC) in litres and percentage, and FEV₁/FVC ratio) and comorbidities. Comorbidities registered were: history of asthma, osteoporosis, heart disease, chronic kidney disease, diabetes mellitus, active malignancy, rheumatoid arthritis, hypertension, and liver disease.
STATISTICAL ANALYSIS:
Statistical analysis was performed using STATA ver. 17. For normally distributed data confidence intervals (CI) were calculated by using T-test with a 95% CI. P-value of <0.05 was considered significant. For non-normally distributed data, Wilcoxon rank sum test was performed.
ETHICS:
The study is approved by the Region of Southern Denmark: (Acadre sagsnummer: 23/52066)
Results
STUDY POPULATION:
In total 663 patients were discharged from OUH with the ICD-10 code DJ44 as either a primary or as a secondary diagnosis. After excluding patients who did not meet our inclusion criteria, the final sample size was 396 patients discharged with COPD in exacerbation. See flowchart presented in Figure 1.
Figure 1. Flow chart of patients discharged from Odense University Hospital in Odense with chronic obstructive pulmonary disease in exacerbation in 2023.
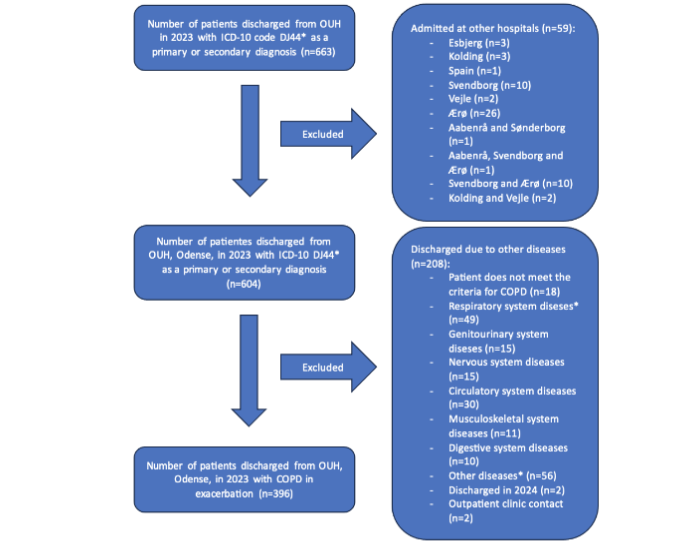
DJ44* = Chronic obstructive pulmonary disease.
Respiratory system diseases* includes: Pleura effusion; pneumothorax; pneumonia without respiratory involvement; pulmonary oedema; lung cancer; covid infection without respiratory involvement; influenza without pulmonary involvement; pulmonary embolism; lung abscess.
Other diseases** includes: Bacterial infection, unspecified; dehydration; delirium; toxic effect of unspecified substance; repeated falls; sepsis; disorientation; anaemia; alcohol abuse; traumatic ischemia of muscle; pain, unspecified; hyponatremia; problem related to care provider dependency, unspecified; anaphylactic shock, unspecified; chronic lymphocytic leukemia.
Abbreviations: COPD = chronic obstructive pulmonary disease; OUH = Odense University Hospital; ICD-10 = International classification of diseases-10.
DEMOGRAPHIC CHARACTERISTICS:
The characteristics of the 396 unique patients are presented in table 2, including 185 males and 211 females, with an average age of 75.7 years and an average BMI of 24.6. The average number of admissions in 2023 was 1.4 per patient. Documented spirometry was available for 64.1% of the patients, with an average FEV₁ of 42.6%. In all, 181 patients (47.5%) had an FEV₁ lower than 50% of expected, and 86 patients (21.7%) used LTOT. The median number of comorbidities was two.
Table 2. Demography of all patients with Chronic Obstructive Pulmonary Disease (COPD) in exacerbation discharged from Odense University Hospital in Odense 2023 grouped according to indication for non-invasive ventilation or not.
| Patients with COPD in exacerbation | All patients (100%) | Patients with indication for NIV (28.3%) | Patients without indication for NIV (71.7%) |
|---|---|---|---|
| Patients n (male/female) | 396 (185/211) | 112 (47/65) | 284 (138/146) |
| Prehospital treatment | 196 (49.5%) | 66 (58.9%) | 130 (32.8%) |
| Age, average years (median) | 75.7 (77) | 76.8 (74) | 80.1 (78) |
| BMI, average (range) | 24.6 (12-49) | 25.7 (14-49) | 24.2 (12-46) |
| Admissions average (range) | 1.4 (1-8) | 1.4 (1-4) | 1.4 (1-8) |
| Documented spirometry n (%) | 254 (64.1) | 75 (67.0) | 171 (60.2) |
| FEV₁%, average (range) | 42.6 (10-107) | 35.5 (12-87) | 45.8 (10-107) |
| Long-term Oxygen Therapy n (%) | 86 (21.7) | 29 (25.9) | 57 (21.0) |
| Received NIV, n (%) | 104 (26.3) | 104 (92.9) | 0 (0) |
| 30-day mortality, n (%) | 64 (16.2) | 29 (25.9) | 35 (12.3) |
| Treatment limitation n (%) | 247 (62.0) | 76 (67.8) | 171 (60.2) |
| Co-morbidity, median (range) | 2 (0-6) | 1 (0-5) | 2 (0-6) |
| Co-morbidities n (%) | |||
| History of asthma | 33 (8.3) | 10 (8.9) | 3 (8.1) |
| Osteoporosis | 119 (30.1) | 32 (28.6) | 87 (30.6) |
| Heart disease | 161 (40.7) | 44 (39.3) | 117 (41.3) |
| Chronic kidney disease | 21 (5.3) | 6 (5.4) | 15 (5.3) |
| Diabetes mellitus | 68 (17.2) | 19 (17.0) | 49 (17.3) |
| Cerebral disease | 77 (19.4) | 16 (14.3) | 61 (21.2) |
| Active malignancy | 30 (7.6) | 16 (14.3) | 61 (21.5) |
| Rheumatoid arthritis | 15 (3.8) | 2 (1.8) | 13 (4.6) |
| Hypertension | 178 (45.0) | 44 (39.3) | 134 (47.2) |
| Liver disease | 11 (2.8) | 7 (6.3) | 4 (1.4) |
Abbreviations: NIV: non-invasive ventilation; BMI: body mass index; FEV₁: forced expiration volume in 1 second.
INDICATION AND INITIATION OF NIV:
Among the 396 patients, 28.3% [CI: 23.9 – 32.7%] were eligible for NIV treatment, and of these patients 92.9% [CI: 88.1 – 97.6%] were offered and received the treatment with NIV (see Table 2).
30-DAY MORTALITY RATE:
The overall 30-day mortality rate was 16.2% [CI: 12.5 – 19.8%] (see Table 2). Patients who died were significantly older compared to patients who did not die, but there was no significant difference in comorbidities between the two groups.
Among patients receiving NIV, the 30-day mortality rate was 25% [CI: 16.7 – 33.3%] and compared to patients without NIV treatment the 30-day mortality rate was 13% [CI: 9.2 – 16.9%].
Patients with NIV indication trended to be younger (76 years vs. 81.5 years) and had more severe COPD (FEV₁ of 35.8% vs 43.1%) (see Table 3), although not significant, but there was a significant difference in comorbidities between the two groups of patients who died.
Table 3. Patients discharged from Odense University Hospital with COPD in exacerbation with a registered 30-day mortality.
| Received NIV and died within 30 days | Did not receive NIV and died within 30 days | |
|---|---|---|
| Patients, n (male/female) | 26 (8/18) | 38 (22/16) |
| Age, years, median (1. Quartile – 3. Quartile) | 76 (67.3-84.3) | 81.5 (74.8-87.8) |
| FEV₁% average (range) | 35.8 (17-84) | 43.1 (17-77) |
| FEV₁% ≤ 50% n (%) | 14 (53.8) | 15 (39.5) |
| Co-morbidities, median (range) | 1 (0-3) | 2 (0-5)* |
Abbreviations: NIV = non-invasive ventilation; FEV₁ = Forced expiratory volume in the first second.
*significant difference.
TREATMENT CEILING:
Of all patients admitted with COPD and evaluated as having an exacerbation, 247 (62%) of the patients had an order: “not-to intubate”. Of the patients who died, 82% of the patients had an order: “not-to intubate”.
Discussion
NIV was implemented due to survival benefit in randomized controlled studies of highly selected patients fulfilling predefined inclusion criteria and not having exclusion criteria. Our data has, in line with other published audits in real life settings,¹¹˒¹³ not shown overall survival benefit, but initiation of NIV was offered to patients with respiratory acidosis secondary to COPD exacerbations.
This is the third audit on patients admitted with COPD exacerbation and use of NIV, since implementation of NIV at the Odense University Hospital in 2004.¹⁴ Others have pointed out the survival benefit of early NIV initiation,¹⁵ and our local setup was therefore organized to enable accessibility for NIV-treatment up-front without need of patient referral.¹⁰ Teaching programs for new staff on NIV initiation was implemented, ensuring awareness of the treatment.
The average age of COPD patients admitted in 2012 was 71.1 years,⁹ similar to data reported from audit data from the UK,¹³ compared to our present cohort 75.7 years. The severity of COPD based on mean FEV₁ was lower in 2012 compared to 2023 (35.5% vs 42.6%). Higher mean age and mean FEV₁% seen in patients admitted in 2023, could be interpreted as survival effects of interventions initiated for patients with COPD in the municipalities, although we do not have data on direct survival effects. Our data support the demography of the patients has changed over the years (survival effects), with better treatments, closer monitoring with treatment at home, and reduction of annual admissions. We can document that patients in need of admission are older than in earlier audits, and that NIV criteria (and initiation of treatment) was met in a higher rate than earlier reported.⁹ Patients who died, were significantly older than patients who did not die, but the comorbidity burden was not significantly different between the groups. Age has been reported to be an independent patient-related factor for death along with presence of respiratory acidosis and Charlson Comorbidity Index.¹⁶
In Denmark there has been introduced a policy of patient involvement on discussion of treatment ceilings. Therefore, if there was a treatment ceiling, it was assessed as a standard evaluation for all elderly and fragile patients at admission.
In 2023 the 30-day mortality rate was lower than in 2022. The COVID-19 pandemic resulted in fewer admissions with COPD in 2020 (unpublished data) due to the isolation policies, and one could speculate, that the higher 30-day mortality rate in 2022, could be a consequence of delayed COPD deaths in the two years of the pandemic, due to isolation of many COPD patients.
The audit cohort was based upon ICD-10 diagnoses, warranting correct diagnose registration at discharge. Patients with COPD and without the predetermined ICD-10 discharge diagnoses are therefore not included, and this is a potential bias. Our audit has, therefore, resulted in local actions to ensure correct discharge diagnose registrations with weekly reviews by senior doctor of all patients discharged from the ward of Respiratory Medicine.
The local audit showed that the 30-day mortality rate was 16.2% which is higher compared to reported data 10 – 15 years ago, but significantly lower than the reported 30-day mortality rate in 2022, and that the patients who died were significantly older than the survivors.
Conclusion
This local audit showed that 396 unique patients with COPD in exacerbation were admitted to OUH, Odense in 2023 and with an annual admission of 1.4. Of those, 112 patients met the criteria for NIV and 104 patients (92.9%) received it.
Conflict of Interest:
The authors have no conflicts of interest to declare.
Funding Statement:
None.
Acknowledgements:
None.
References
1. Global initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease report, 2023. Available from: https://goldcopd.org/2023-gold-report-2/ (19-08-2024)
2. Løkke A, Hilberg O, Tønnesen P, Ibsen R, Kjellberg J, Jennum P. Direct and indirect economic and health consequences of COPD in Denmark: a national register-based study: 1998-2010. BMJ open. 2014;4(1).
3. Bilde L, Svenning AR, Dollerup J, Borgeskov HB, Lange P. The cost of treating patients with COPD in Denmark – a population study of COPD patients compared with non-COPD controls. Respir Med. 2007;Mar:101(3):539-49.
4. Lange P, Tøttenborg SS, Sorknæs AD et al. Danish Register of chronic obstructive pulmonary disease. Clinical Epidemiology 2016;8 673-678
5. RKKPs Videncenter med fagligsparring fra formandsskabet i DrKOL. Dansk register for Kronisk Obstruktiv Lungesygdom – DrKOL. Årsrapport for 2022 – 1. Januar til 31. December 2022. Available from: Dansk register for Kronisk Obstruktiv Lungesygdom (DrKOL) – RKKP (19-08-2024)
6. Sundhedsstyrelsen. KOL – anbefalinger for tidlig opsporing, opfølgning, behandling og rehabilitering. Copenhagen: Sundhedsstyrelsen, 2006. Electronic ISBN: 87-7676-393-5
7. Regional COPD health plan. Available from: Tværsektorielt forløbsprogram for KOL-patienter (regionsyddanmark.dk) (21-07-2024)
8. Danish Telemedicine: Available from: TeleKOL – Telemedicinsk tilbud – sundhed.dk (21-07-2024)
9. Titlestad IL, Bryde J, Øberg-Hansen B, Lassen AT, Vestbo J. Reorganisation of acute referral to an emergency department resulted in fewer admissions for chronic obstructive pulmonary disease but in higher rates of non-invasive ventilation. Dan Med J 2014;61(11):A4958.
10. Emergency Department organization. Available from Emergency Department, OUH (21-07-2024)
11. Roberts CM, Stone RA, Buckingham RJ, Pursey NA, Lowe D. Acidosis, non-invasive ventilation and mortality in hospitalised COPD exacerbations. Thorax 2011;66:43-48.
12. Tøttenborg SS, Johnsen SP, Thomsen RW, Nielsen H, Hansen EF, Lange P. Use of non-invasive ventilation is increasing in patients admitted with a chronic obstructive pulmonary disease exacerbation. Dan Med J 2013;60(8):A4686
13. Hurst JR, Quint JK, Stone RA, Silove Y, Youde J, Roberts CM. National clinical audit for hospitalised exacerbations of COPD. ERJ Open Res. 2020;Sep 21;6(3):00208-2020. doi: 10.1183/23120541.00208-2020. PMID: 32984418; PMCID: PMC7502696.
14. Titlestad IL, Madsen HD. Implementation of non-invasive ventilation in respiratory ward in patients with exacerbations of chronic obstructive pulmonary disease. Ugeskr Laeger. 2008;170(4):240-3.
15. Jayadev A, Stone R, Steiner MC, McMillan V, Roberts CM. BMJ Open Resp Res 2019;6:e000444. doi:10.1136/bmjresp-2019-000444
16. Hartl S, Lopez-Campos JL, Pozo-Rodriguez F, Castro-Acosta A, Studnicka M, Kaiser B, Roberts CM. Risk of death and readmission of hospital-admitted COPD exacerbations: European COPD Audit. Eur Respir J. 2016 Jan;47(1):113-21. doi: 10.1183/13993003.01391-2014. Epub 2015 Oct 22. PMID: 26493806.