






Coping and Recovery in Yazidi Genocide Survivors
Healing after Genocide: A Cross-Sectional Study on Emotion-Focused Coping and Psychosocial Recovery among Yazidi Survivors
Jan Ilhan Kizilhan1,2, Anna Weigelt1,
- Institute of Transcultural Health Science, Baden-Wuerttemberg Cooperative State University, 70178 Stuttgart, Germany
- Institute for Psychotherapy and Psychotraumatology, University of Duhok, Duhok 42001, Iraq
OPEN ACCESS
PUBLISHED: 31 July 2025
CITATION:Kizilhan, JI., Weigelt, A., 2025. Healing after Genocide: A Cross-Sectional Study on Emotion-Focused Coping and Psychosocial Recovery among Yazidi Survivors. Medical Research Archives, [online] 13(7). https://doi.org/10.18103/mra.v13i7.6772
DOI: https://doi.org/10.18103/mra.v13i7.6772
ISSN: 2375-1924
ABSTRACT
Background: A decade after the 2014 genocide, Yazidi survivors in Northern Iraq continue to face intersecting challenges of psychological distress, displacement, and inadequate access to care. While prior research has documented elevated symptom burdens, little is known about current coping preferences and structural risk factors in this population. This cross-sectional study investigates the relationships between emotion-focused coping strategies, psychotherapy access, structural vulnerabilities, and mental health symptoms among Yazidi survivors.
Methods: A total of 346 Yazidi adults, both displaced and non-displaced, participated in structured interviews across various settings in the Kurdistan Region of Iraq. Participants completed validated measures of posttraumatic stress disorder, depression, and anxiety, and rated the perceived helpfulness of culturally relevant coping strategies. Statistical analyses included group comparisons, repeated-measures analysis of variance, and correlational analyses.
Results: Only 36.4% of participants had any contact with mental health services, with psychotherapy rated as one of the least helpful strategies. Spiritual and internal coping mechanisms such as prayer and belief in personal or collective strength were perceived as most helpful. Psychotherapy use was higher among those with the greatest symptom burden. Structural vulnerability (camp residence, unstable income) significantly predicted elevated distress.
Conclusion: Yazidi survivors rely primarily on culturally grounded coping strategies rooted in spirituality and community, while access to formal care remains limited and stratified. Psychosocial support must be integrated with structural assistance, justice mechanisms, and cultural traditions to foster sustainable recovery.
Keywords: Yazidi, Genocide, Recovery, Resilience, Cultural Coping, Mental Health Access, Transgenerational Trauma.
1. Introduction
The Yazidi people, a small ethnoreligious community from Northern Iraq, have endured centuries of systemic persecution. Oral histories document at least 74 historical genocide attempts, collectively referred to as Ferman, which form a cornerstone of Yazidi cultural identity and memory. The 2014 attacks by the so-called Islamic State of Iraq and Syria (ISIS) marked the most devastating assault in modern history, involving mass executions, forced conversions, abductions, and sexual enslavement in the Sinjar region, Northern Iraq. Thousands were killed or displaced, and entire communities were forced into refugee camps across Iraq, Syria, and diaspora settings in Europe, North America, and Australia. In 2016, the United Nations High Commissioner for Human Rights officially recognized ISIS’s actions as genocide, crimes against humanity, and war crimes. Today, returning to Sinjar remains dangerous due to ongoing violence, destroyed infrastructure, and unexploded improvised explosive devices.
1.1. PSYCHOLOGICAL CONSEQUENCES
The psychological repercussions of these atrocities are severe and enduring. Numerous studies report high prevalence rates of posttraumatic stress disorder (PTSD), depression, and anxiety among Yazidi survivors. PTSD rates range from 43% to 79%, while major depression affects approximately 40% to 49%, and anxiety disorders reach up to 51%. Symptoms include flashbacks, nightmares, emotional withdrawal, and hyperarousal, often exacerbated by chronic uncertainty and loss of social cohesion. Beyond standard diagnostic categories, survivors particularly women and older adults often exhibit culturally shaped expressions of distress such as somatic symptoms, dissociative states, and spiritual confusion.
1.2. GENDER-SPECIFIC TRAUMATIZATION
Gender-based violence forms a core dimension of Yazidi suffering. ISIS deliberately targeted women and girls for sexual enslavement and captivity, inflicting not only extreme physical and psychological harm but also long-term stigma within their communities. Despite calls by Yazidi religious leaders for reintegration, many survivors continue to face exclusion rooted in patriarchal norms and concepts of “honor” and shame. This social marginalization compounds mental health risks for female survivors. In a clinical study of Yazidi women who had survived the 2014 genocide and endured captivity by IS, 97.9% exhibited symptoms consistent with PTSD, and 88.1% met criteria indicative of major depression.
1.3. LIVING CONDITIONS AND STRUCTURAL VULNERABILITY
The challenges faced by Yazidi survivors extend far beyond the psychological aftermath of violence. Many continue to live in precarious conditions shaped by long-term displacement, limited access to health care, and restricted economic and educational opportunities. Structural factors such as inadequate housing, food insecurity, and unstable income contribute substantially to psychological distress and complicate recovery trajectories. Internally displaced Yazidis (IDPs), particularly those residing in refugee camps, exhibit significantly higher levels of psychological burden compared to those living in urban or resettled environments. One study reported that Yazidi camp residents had 19% higher distress scores than their non-IDP counterparts. These trends were most pronounced among individuals who had undergone prolonged and repetitive exposure to traumatic events. Among Yazidi IDPs living in a refugee camp within the KRI, a striking 79% reported experiencing PTSD symptoms. These findings highlight the cumulative impact of prolonged exposure to instability, trauma reminders, and social isolation.
In addition, the deterioration of security and infrastructure following the 2017 independence referendum in the KRI further compounded the humanitarian situation. Tensions between the Kurdish Regional Government and the Iraqi central government led to military interventions, border closures, and severe restrictions on air travel and trade. These structural conditions often also disrupt protective cultural practices, such as communal rituals and religious gatherings, that traditionally serve as sources of resilience and meaning-making. For those resettled in Europe or North America, language barriers, isolation, and potential discrimination pose new challenges. As a result, displaced populations experienced interruptions in aid delivery and increasing economic hardship. Refugees living in camps reported sporadic access to food and medication, while those in urban settings faced soaring living costs and limited access to health services due to the absence of health insurance or civil documentation.
The Kurdistan Region, home to around 5.2 million people, has absorbed more than six million IDPs and refugees since 2014. Around 40% of these populations remain in formal camp settings, while the rest live in informal shelters among host communities. Despite relatively high levels of acceptance by local authorities and host populations, integration remains a persistent challenge. Ongoing threats to personal safety, lack of livelihood opportunities, and barriers to civil registration hinder long-term stability and psychological recovery. Even basic needs remain unmet in many settings: as of 2022, 86% of Syrian refugees living in camps in Iraq were considered food insecure. This environment of structural vulnerability continuously interacts with psychological trauma, magnifying distress and impeding access to care. In addition, disrupted religious and communal rituals important pillars of Yazidi resilience are often difficult to maintain under such unstable conditions.
1.4. TRANSGENERATIONAL TRAUMA AND COLLECTIVE MEMORY
In addition to the immediate psychological impact of the 2014 genocide, many Yazidi survivors are affected by transgenerational trauma a process through which the experiences of persecution and violence are transmitted across generations. These transmissions occur not only through biological pathways (e.g., epigenetic or stress-response mechanisms), but also through collective memory, family narratives, religious practices, and symbolic cultural frameworks. Children and adolescents within Yazidi families often interpret current events in light of ancestral suffering, reinforcing existential fears and chronic hypervigilance. This phenomenon intensifies in contexts of ongoing instability, where the line between historical persecution and present-day threat remains blurred. At the same time, these inherited narratives can serve as powerful sources of resilience. Stories of communal endurance, spiritual faith, and survival against all odds foster a sense of continuity and identity, helping individuals make meaning of their own trauma.
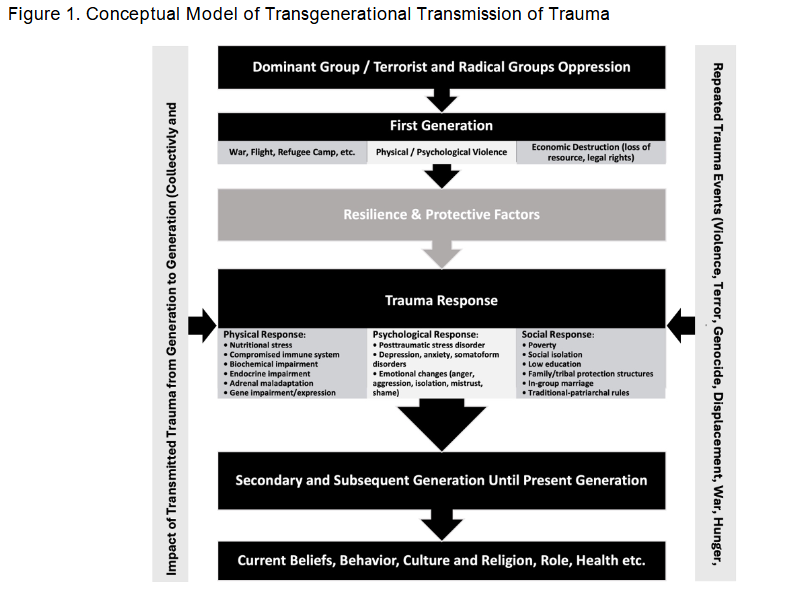
The first generation typically experiences direct exposure to violence, forced displacement, and structural breakdown. These experiences lead to complex trauma responses, including physiological (e.g., endocrine disruption), psychological (e.g., emotional withdrawal, PTSD symptoms), and social (e.g., marginalization, poverty) consequences. Subsequent generations inherit these burdens biologically, behaviorally, and symbolically but also develop adaptive mechanisms, including spiritual coping, group identity, and cultural rituals that reaffirm dignity and cohesion. Understanding the dual nature of transgenerational trauma as both a source of vulnerability and resilience is essential for designing psychosocial interventions. It also provides a theoretical framework for interpreting current coping strategies and mental health outcomes among Yazidi survivors. In this context, trauma is not only an individual or clinical condition but a historically situated, culturally embedded process that continues to shape collective identity and recovery.
1.5. ACCESS TO PSYCHOTHERAPY
Despite the high psychological burden among Yazidi survivors, access to professional mental health care in the Kurdistan Region of Iraq (KRI) remains limited. While the KRI has historically offered relatively better healthcare infrastructure compared to central and southern Iraq partly due to international programs like the Oil-for-Food Initiative and greater political stability the system continues to suffer from chronic underfunding, uneven service provision, and significant personnel shortages. Mental health care is embedded within the broader public health system, which operates through a tiered model of primary, secondary, and tertiary care. Primary mental health care is provided in primary health care centers, while secondary and tertiary mental health care is almost only available in larger hospitals with teaching responsibilities. However, only a small number of facilities offer dedicated psychiatric services, and mental health remains underrepresented in both health policy and education. Clinical psychology, psychotherapy, and social work are similarly underdeveloped professions, with few specialized training programs and unclear professional recognition.
In the KRI specifically, international and local non-governmental organizations have stepped in to fill critical gaps. Organizations such as the Jiyan Foundation and the Free Yezidi Foundation provide low-threshold mental health and psychosocial support (MHPSS) in displacement camps and community settings. These services often rely on task-shifting strategies, whereby lay counselors or community health workers frequently trained refugees themselves deliver basic psychosocial interventions under supervision. Programs like Problem Management Plus (PM+), were community workers provide low-intensity psychosocial support, have shown promise in such settings, though their applicability is limited in cases of severe or complex trauma. Despite these efforts, key challenges persist. The majority of displaced persons in the region live outside official camps, where access to non-governmental organizations services is significantly lower. Public clinics in urban areas are often under-resourced and difficult to reach due to transportation barriers, lack of health insurance, and administrative hurdles. Additionally, stigma around mental illness and skepticism toward Western therapeutic models further discourage professional help-seeking. Combined with high levels of burnout and secondary traumatization among mental health workers themselves, these factors contribute to a fragmented and insufficient system of care.
1.6. AIM OF THE STUDY AND RESEARCH QUESTIONS
Given the complex interplay of historical persecution, ongoing displacement, gender-based violence, and limited access to mental health care, there is an urgent need for empirical data on the psychosocial well-being of Yazidi survivors. While previous research has documented high levels of psychological distress, few studies have examined how survivors currently cope with trauma, which structural factors affect mental health outcomes, and to what extent psychotherapy services are accessible and perceived as helpful. This study addresses these gaps by presenting findings from a cross-sectional survey conducted in displacement settings in the Kurdistan Region of Iraq, ten years after the 2014 genocide. The primary aim of the study is to investigate the interactions of psychological distress with psychotherapy access, structural vulnerabilities and emotion-focused coping strategies among Yazidi survivors. The study seeks to understand how these factors interact in shaping recovery trajectories in a context where both trauma and resilience are deeply culturally embedded. To operationalize this aim, the study was guided by the following research questions:
- How many survivors have had access to psychotherapy, and how does psychotherapy status relate to levels of psychological distress?
- What structural factors such as income level and housing situation are associated with variations in psychological symptom severity?
- Which emotion-focused coping strategies are perceived as most or least helpful, and how are these perceptions associated with sociodemographic factors (e.g., gender, education) and mental health symptoms?
By addressing these questions, the study aims to contribute to a culturally grounded understanding of recovery processes among Yazidi survivors and to inform the development of trauma-informed, accessible, and community-based psychosocial interventions in post-conflict settings.
2. Methods
2.1. RESEARCH DESIGN AND SETTINGS
This study employs a cross-sectional design. Data collection took place between November 2023 and March 2024 in the Kurdistan Region of Iraq, where both internally displaced Yazidis residing in refugee camps and non-displaced individuals in and around Duhok were surveyed. Recruitment was facilitated by psychotherapists and refugee camp workers, with data collected in Bajidkandala, Bersive, Chamishko, Eissyan, Kabarto 1, Kabarto 2, Khanke, Qadya, and Shariya refugee camps. All interviews were conducted orally by students and lecturers from the Master of Advanced Studies in Psychotherapy and Psychotraumatology program at the University of Dohuk. Surveys were administered in Kurdish and English, with non-translated English items orally translated into Kurmanji by the interviewers. Data collection used KoboToolbox on laptops, tablets, and mobile phones, with responses entered directly into the software. Data were collected in accordance with international ethical standards for research involving human subjects, including the principles outlined in the Declaration of Helsinki. The study protocol received approval from the Ethics Committee of the Institute of Psychotherapy and Psychotraumatology at the University of Dohuk, which served as the responsible institutional review board. Participants received detailed information about the study, provided informed consent, and participated voluntarily without monetary compensation. To minimize participant burden, the survey took approximately one and a half hours.
2.2. PARTICIPANTS
The demographic characteristics of the sample are shown in Table 1. The sample consisted of n = 346 Yazidi participants residing in the Kurdistan Region of Iraq. Participants ranged in age from 18 to 70 years (M = 30.60, SD = 9.39). Of these, 56.07% identified as female (n = 194), 43.64% as male (n = 151), and gender information was missing for one individual (0.29%). In terms of displacement status, 61.85% (n = 214) were internally displaced persons (IDPs), while 38.15% (n = 132) were non-displaced Yazidis residing in Iraq. Regarding marital status, 46.53% were married (n = 161), 50.58% were single (n = 175), and 2.60% were widowed (n = 9); one participant (0.29%) did not report marital status. Literacy levels were relatively high, with 71.39% (n = 247) categorized as literate and 26.88% (n = 93) as illiterate; literacy status was missing for 1.73% (n = 6). Educational attainment varied: 25.14% (n=87) reported no formal education, 6.36% (n = 22) had incomplete primary education, and 7.23% (n = 25) had completed primary school. Additionally, 7.51% (n = 26) had attained intermediate-level education, and 50.29% (n = 174) had completed high school. Educational data were missing for 4.47% (n = 12) of participants.
| Min | Max | M | SD | |
|---|---|---|---|---|
| Age | 18 | 70 | 30.60 | 9.39 |
| N | % of Total Sample | |
|---|---|---|
| Group | ||
| Non-displaced Iraqis | 132 | 38.15 |
| Iraqi IDPs | 214 | 61.85 |
| Gender | ||
| Female | 194 | 56.07 |
| Male | 151 | 43.64 |
| NA | 1 | 0.29 |
| Level of education | ||
| None | 87 | 25.14 |
| Incomplete primary school | 22 | 6.36 |
| Primary school | 25 | 7.23 |
| Intermediate | 26 | 7.51 |
| High school | 174 | 50.29 |
| NA | 12 | 4.47 |
| Literacy | ||
| Literate | 93 | 26.88 |
| Illiterate | 247 | 71.39 |
| NA | 6 | 1.73 |
| Marital status | ||
| Married | 161 | 46.53 |
| Widowed | 9 | 2.60 |
| Single | 175 | 50.58 |
| NA | 1 | 0.29 |
Note. Min = Minimum, Max = Maximum, M = Mean, SD = Standard deviation, N = Sample size.
2.3. TRANSLATION PROCESS
The translation process for the Posttraumatic Stress Disorder Checklist (PCL-5) into Kurmanji was conducted following modern guidelines for translating medical questionnaires. Initially, two native speakers of Kurmanji independently translated the questionnaire from English to Kurmanji, carefully resolving any differences between their versions. The Kurmanji translations were then independently back-translated into English by another individual. Finally, all translators engaged in a collaborative review to address any inconsistencies identified between the original English text and the back-translated version.
2.4. MEASURES
2.4.1. Demographic measures
Participants provided information on a range of sociodemographic variables. These included age (open numeric entry), gender (female, male), marital status (single, married, widowed), and literacy status (literate, illiterate). Education level was captured using five ordinal categories: no formal education, incomplete primary education, completed primary education, intermediate education, and completed high school. In addition, participants were asked to report their current housing situation (camp, rented housing, or owned home), as well as their monthly household income, categorized into six ordinal groups based on Iraqi Dinar ranges: no income, very low (1–250,000), low (250,001–750,000), medium (750,001–1,500,000), high (1,500,001–5,000,000), and very high (>5,000,000). Participants were also asked about their experiences with psychotherapy. Response options were coded nominally as follows: currently in psychotherapy, previously received psychotherapy, on a waiting list, or never received psychotherapy nor on a waiting list.
2.4.2. Emotion-focused coping strategies
To assess culturally relevant approaches to emotional regulation and trauma processing, participants rated seven emotion-focused coping strategies. These items were developed specifically for this study based on semi-structured interviews with local psychotherapists and Yazidi community leaders, as well as a targeted literature review on transgenerational trauma coping across collectivist and post-conflict societies. Each coping strategy was rated on a 5-point Likert scale ranging from 1 (not at all helpful) to 5 (very helpful) in dealing with psychological distress. The strategies included:
- Belief in personal strength
- Praying
- Belief in collective strength (e.g., community or group resilience)
- Social retreat (spending time alone)
- Seeking help within the Yazidi community
- Exchanging trauma-related experiences with others
- Seeking professional help (e.g., doctor or therapist)
The internal consistency of the coping scale was acceptable, with a Cronbach’s alpha of .96.
2.4.3. Patient Health Questionnaire-9 (PHQ-9)
The PHQ-9 is a widely used self-report measure for assessing the intensity of depressive symptoms. It comprises nine items, each corresponding to a diagnostic criterion for major depressive disorder as outlined in the Diagnostic and Statistical Manual of Mental Disorders-5 (DSM-5). Participants rate how often they have experienced each symptom over the preceding two weeks using a 4-point scale. Scores of 5, 10, and 15 serve as conventional thresholds for mild, moderate, and severe depression, respectively. Extensive validation studies have demonstrated the PHQ-9’s high reliability (α = .89), strong test-retest reliability with an Intraclass Correlation Coefficient (ICC) of .84, and excellent diagnostic accuracy, with 88% sensitivity and specificity for major depression.
2.4.4. Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5)
The PCL-5 is a self-report instrument designed to assess posttraumatic stress disorder symptoms in accordance with DSM-5 diagnostic criteria. It includes 20 items, each representing one symptom of PTSD. Participants rate the extent to which each symptom has bothered them in the past month on a 5-point scale. While cutoff values between 31 and 33 are commonly used to indicate probable PTSD, this study employed a conservative threshold of 33. Prior research has demonstrated the PCL-5’s high reliability (α = .94), strong test-retest stability (ICC = .82), and solid construct validity.
2.4.5. Hopkins-Symptom-Checklist-25 (HSCL-25)
The Hopkins Symptom Checklist-25 (HSCL-25) is a frequently employed screening tool for assessing anxiety and depressive symptoms, particularly in refugee and post-conflict populations worldwide. Its cross-cultural robustness has been confirmed through psychometric studies in various regions, including Sub-Saharan Africa, Eastern Europe, and parts of Asia. These investigations have consistently demonstrated high internal consistency (α = .85 for anxiety), along with strong inter- and test-retest reliability. Given recent methodological concerns regarding the cross-cultural validity of the depression subscale, the present study focused exclusively on the anxiety subscale. Items were rated on a 4-point Likert scale, and scores exceeding an established threshold of 1.75 were classified as exhibiting clinically relevant anxiety. In our sample, the anxiety subscale demonstrated excellent internal consistency (α = .87).
2.5. DATA ANALYSIS
The data were analyzed using the statistical software R. Descriptive statistics, including means, standard deviations, and frequency distributions, were computed to summarize demographic characteristics and key study variables. To examine group differences in psychological distress, we conducted one-way analyses of variance (ANOVA) and Kruskal-Wallis tests, depending on the distributional properties of the data. Post-hoc comparisons were adjusted as appropriate. Differences in PTSD symptoms across housing conditions were assessed using ANOVA, while differences in depression and anxiety across income groups were evaluated using non-parametric Kruskal-Wallis tests due to skewed distributions. To compare the perceived helpfulness of emotion-focused coping strategies, a repeated-measures ANOVA was conducted with Greenhouse-Geisser correction applied for violations of sphericity. Pairwise comparisons were adjusted using Bonferroni correction. Additionally, Pearson correlations were calculated to explore associations between perceived helpfulness of individual coping strategies and symptom severity across depression, PTSD, and anxiety. A priori power analysis for repeated-measures ANOVA indicated that a minimum sample size of 331 was required to detect a small to medium effect (f = .15) with a power of .80 and alpha of .05 across seven within-subject conditions. The final sample size of 346 met this criterion, ensuring sufficient power to detect meaningful differences in coping strategy evaluations.
3. Results
3.1. PSYCHOTHERAPY STATUS
Among participants in our study, 8.7% reported currently being in psychotherapy, 20.2% had previously received therapy, 5.2% were on a waiting list, and 63.6% had never received psychotherapy nor were on a list. Overall, 36.4% of respondents had some form of contact with mental health services. Importantly, participants with psychotherapy experience reported significantly higher levels of psychological distress across all domains (depression: r = .33, PTSD: r = .23, anxiety: r = .20; all p < .01). While this likely reflects treatment-seeking behavior rather than therapeutic inefficacy, it highlights that those in care represent the most burdened segment.
3.2. INCOME AND PSYCHOLOGICAL DISTRESS
In our study, participants were grouped based on monthly income levels in Iraqi Dinar (IQD): no income (0), very low (1–250,000), low (250,001–750,000), medium (750,001–1,500,000), high (1,500,001–5,000,000), and very high (>5,000,000).
| Income Group | Monthly Income (IQD) | Approx. EUR | n (%) |
|---|---|---|---|
| No income | 0 | 0 | 40 (11.6%) |
| Very low | 1–250,000 | <1 | 86 (24.9%) |
| Low | 250,001–750,000 | 170–520 | 121 (35.0%) |
| Medium | 750,001–1,500,000 | 520–1,030 | 49 (14.2%) |
| High | 1,500,001–5,000,000 | 1,030–3,450 | 13 (3.8%) |
| Very high | >5,000,000 | >3,450 | 5 (1.4%) |
| NA | 32 (9.2%) |
Note. NA = missing data, IQD = Iraqi Dinar, EUR = Euro, n = number of respondents.
While no significant group differences emerged for PTSD symptoms, the Kruskal-Wallis test revealed significant differences in anxiety (χ2(5) = 11.82, p = .04) and depression (χ2(5) = 12.41, p = .03). Post-hoc tests indicated that participants in the “very low income” group had significantly higher anxiety than those with “no income” (p = .021), and higher depression scores than those in the “medium income” group (p = .023). These results suggest that survivors with minimal but unstable income may experience heightened psychological distress.
3.3. HOUSING SITUATION
In our survey, housing conditions were significantly associated with PTSD symptom severity. An ANOVA revealed that participants living in camps reported significantly higher PTSD scores than those residing in rented or owned homes (F(2, 335) = 7.00, p = .001). Tukey’s Honestly Significant Difference post-hoc tests confirmed that PTSD scores were higher for camp residents compared to individuals in owned homes (mean difference = -0.44, p = .001) and rented homes (mean difference = -0.35, p = .027). No significant differences were observed between the latter two groups.
3.4. EMOTION-FOCUSED COPING STRATEGIES
Descriptive statistics for the perceived helpfulness of each emotion-focused coping strategy are presented in Table 4.
| Coping Strategy | M | SD |
|---|---|---|
| Belief in personal strength | 2.62 | 1.16 |
| Praying | 2.62 | 1.24 |
| Belief in collective strength | 2.53 | 1.30 |
| Social retreat (spending time alone) | 2.37 | 1.24 |
| Seeking help within the Yazidi community | 2.13 | 1.37 |
| Exchange trauma contents with others | 2.09 | 1.28 |
| Seeking professional help (e.g., doctor, therapist) | 1.99 | 1.38 |
Note. M = mean, SD = standard deviation.
The most helpful strategies included belief in personal strength, praying, and belief in collective strength. Strategies rated as less helpful included social retreat, seeking help within the Yazidi community, exchanging trauma content with others, and seeking professional help. A repeated-measures ANOVA revealed significant differences between strategies (F(6, 1614) = 19.18, p < .001, η² = .042; Greenhouse-Geisser corrected). Bonferroni-corrected comparisons indicated that professional help, communal help-seeking, and trauma-sharing were significantly less helpful than spiritual or internal strategies like belief in collective strength, belief in personal strength, and praying (all p < .001). The strategy ‘Social retreat’ occupied a middle position, being perceived as less helpful than the belief in personal strength, but more helpful than exchange of trauma contents and seeking professional help. No significant differences emerged between internally displaced persons (IDPs) and non-IDPs. However, women rated professional help as significantly more helpful than men (M = 2.16 vs. 1.79, t(312) = 2.42, p = .016). Educational level also influenced perceived helpfulness: individuals with higher education rated praying, social retreat, and trauma-sharing as significantly less helpful than those with lower education (all p < .05).
Correlation analyses revealed that individuals with higher symptom severity perceived certain strategies as more helpful. For example, depression was most associated with social retreat (r = .21) and seeking help within the community (r = .16). PTSD correlated most with belief in collective strength (r = .18), and anxiety with social retreat (r = .23).
| Coping Strategy | Depression | PTSD | Anxiety |
|---|---|---|---|
| Belief in collective strength | .07 | .18 | .13 |
| Belief in personal strength | .01 | .07 | .09 |
| Praying | -.03 | .00 | .06 |
| Social retreat | .21 | .16 | .23 |
| Exchange trauma contents | .08 | .01 | .12 |
| Seeking professional help | .14 | .13 | .09 |
| Seeking help within the Yazidi community | .16 | .16 | .11 |
Note. PTSD = Posttraumatic Stress Disorder.
4. Discussion
This study examined the psychological burden and recovery processes among Yazidi survivors of the 2014 genocide, with a focus on psychotherapy access, structural vulnerability, and culturally grounded emotion-focused coping. A decade after the genocide, our findings reveal persistent psychological distress, widespread underutilization of mental health services, and reliance on traditional coping frameworks underscoring the complex interplay of trauma, resilience, and systemic barriers in post-conflict recovery.
4.1. STRUCTURAL VULNERABILITY AND TRAUMA BURDEN
Our data confirm that structural hardship especially precarious income and camp-based housing remains a potent predictor of psychological distress. Participants with very low, unstable income reported the highest levels of depression and anxiety, suggesting that economic insecurity may exacerbate feelings of hopelessness and diminish perceived control. Similarly, living in refugee camps was associated with significantly higher PTSD scores, likely reflecting the impact of overcrowding, reduced privacy, and daily reminders of past trauma. These findings echo prior research showing that structural vulnerability acts not only as a contextual background but as a direct psychological stressor. They also reinforce calls for integrated psychosocial and socioeconomic interventions. Mental health support alone cannot be effective without addressing the environmental and material conditions that sustain distress.
4.2. UNDERUTILIZATION AND STRATIFICATION OF PSYCHOTHERAPY
Only about one-third of participants reported any prior engagement with mental health services. Among those with therapy experience, distress levels were significantly higher, pointing to a selective pattern of care-seeking among the most burdened individuals. Notably, professional help was rated as one of the least helpful coping strategies particularly among men and individuals with lower education reflecting both cultural incongruence and stigma. This highlights a fundamental disjunction: those who might benefit most from formal care are often least likely to access it. These findings align with broader literature on post-conflict mental health, where barriers such as stigma, provider shortages, cultural mismatch, and political instability persistently limit access and impact.
4.3. CULTURAL COPING, SPIRITUALITY, AND PATHWAYS FOR CULTURALLY GROUNDED HEALING
Yazidi survivors overwhelmingly favored emotion-focused strategies rooted in spiritual and communal frameworks. Belief in personal and collective strength, as well as prayer, were rated as the most helpful coping mechanisms while strategies involving professional help or trauma-sharing were perceived as least helpful. This pattern reflects a culturally grounded resilience framework that prioritizes introspection, spirituality, and communal meaning-making over biomedical or individualistic models of care. Rather than viewing this preference as an obstacle, it should be embraced as a foundation for culturally responsive intervention. The Yazidi tradition offers rich symbolic resources rituals, oral histories, and spiritual narratives that can be leveraged to support healing and post-traumatic growth. These cultural elements serve both to validate survivors’ suffering and to reaffirm identity, continuity, and meaning. Positive psychotherapy, particularly its second-wave iteration, provides a fitting framework for such integration. Unlike earlier models that focus solely on symptom reduction, second-wave approaches acknowledge suffering as a fertile ground for growth. They honor both the darkness and the resilience inherent in trauma narratives. For Yazidi communities, such approaches may involve:
- Validating horror and betrayal to avoid superficial optimism.
- Reframing trauma through Yazidi historical narratives of endurance and survival.
- Strengthening identity through spiritual values, family roles, and collective pride.
- Encouraging generational dialogue, where resilience as well as trauma is transmitted.
Complementary methods like Narrative Exposure Therapy adapted to Yazidi oral traditions can further support survivors in reconstructing coherent life stories, while embedding their trauma within a culturally meaningful context. In parallel, transitional justice mechanisms even when symbolic may enhance psychological healing. Survivors not only require therapy, but also recognition, validation, and justice. The absence of legal accountability for ISIS crimes contributes to collective demoralization and distrust. Evidence from other conflict regions (e.g., Rwanda, the Balkans, Ukraine) demonstrates that perceived injustice strongly predicts post-conflict distress. Grassroots justice efforts such as community dialogues or religiously led recognition rituals can serve reparative functions. When these spaces provide acknowledgement and restore dignity, they reduce self-blame, foster social reintegration, and promote psychological closure.
Ultimately, culturally grounded psychosocial interventions must move beyond symptom reduction toward restoring meaning, dignity, and belonging. Integrating spiritual leaders, communal practices, and justice narratives into therapeutic models is not a luxury it is essential for engaging survivors and facilitating deep, sustainable healing.
4.4. SYNTHESIS AND POLICY RECOMMENDATIONS
Recovery among Yazidi survivors is shaped by the interplay of structural precarity, historical trauma, and culturally grounded resilience. While spiritual practices, communal support, and personal belief remain primary coping resources, these alone cannot offset the psychological toll of genocide, displacement, and injustice. To foster effective recovery:
- Mental health services must be scaled and localized. Culturally adapted interventions delivered in community settings and aligned with Yazidi traditions are essential to overcome stigma and reach the most vulnerable.
- Spiritual and communal mechanisms should not be replaced but integrated into care. Approaches like second-wave positive psychotherapy and Narrative Exposure Therapy can link trauma processing with cultural identity and resilience.
- Justice is psychological care. The absence of legal accountability deepens trauma. Reparative mechanisms and symbolic recognition especially community-led truth-telling and acknowledgment rituals can restore dignity and support healing.
- Structural insecurity perpetuates distress. Safe housing, food access, and legal documentation are not secondary to mental health they are prerequisites.
- Programs must be co-created. Survivors must shape interventions to ensure cultural relevance, trust, and long-term engagement.
Effective support must bridge evidence-based care with cultural meaning-making, address both trauma and injustice, and prioritize survivor agency. Without this, recovery remains partial and justice, incomplete.
4.5. LIMITATIONS
Several limitations should be acknowledged. First, the empirical data presented in this review stem from a cross-sectional survey conducted under complex field conditions in northern Iraq. While the findings offer valuable correlational insights into coping mechanisms and psychosocial challenges, they do not permit causal conclusions. Self-report measures may also be subject to cultural response biases, social desirability effects, or trauma-related distortions. Furthermore, the sample though diverse in age, gender, and living conditions was geographically limited to the Dohuk region and may not fully represent Yazidi survivors living in more remote areas or diaspora contexts. Ongoing insecurity and infrastructural barriers in northern Iraq likely introduced selection bias, particularly excluding those with the highest levels of isolation or impairment. Beyond the scope of this specific study, most existing research on Yazidi mental health remains cross-sectional or based on small-scale qualitative designs. Large-scale randomized controlled trials or longitudinal studies are rare, and systematic follow-up is difficult to maintain due to displacement, safety concerns, and logistical constraints. These broader research gaps continue to limit generalizability and the ability to evaluate long-term intervention outcomes.
5. CONCLUSION
This study highlights the enduring impact of psychological wounds among Yazidi survivors and underscores the need for culturally grounded, structurally informed interventions. Spiritual and communal coping remain central to recovery but are insufficient in the absence of accessible mental health care, legal recognition, and material security. Effective support must bridge trauma-informed therapy with local traditions, integrating psychological care with cultural meaning-making. Only then can healing become both possible and sustainable.
Conflict of Interest Statement: None.
Funding Statement: None.
Acknowledgements: None.
References
- Tekin A, Karadağ H, Süleymanoğlu M, et al. Prevalence and gender differences in symptomatology of posttraumatic stress disorder and depression among Iraqi Yazidis displaced into Turkey. European Journal of Psychotraumatology. 2016;7(1):28556.
- Kreyenbroek PG, Jindī K. God and Sheikh Adi are perfect: sacred poems and religious narratives from the Yezidi tradition. vol 9. Otto Harrassowitz Verlag; 2005.
- Six-Hohenbalken M. May I be a sacrifice for my grandchildren Transgenerational transmission narratives of the Yezidi ferman. Dialectical anthropology. 2019;43(2):161-183. doi:10.1007/s10624-018-9506-9.
- Omarkhali K. Transformations in the Yezidi tradition after the ISIS attacks. An interview with Ilhan Kizilhan. Kurdish Studies. 2016;4(2):148-154.
- Jäger P. Stress and health of internally displaced female Yezidis in Northern Iraq. Journal of immigrant and minority health. 2019;21(2):257-263.
- UN News. UN human rights panel concludes ISIL is committing genocide against Yazidis. UN News. Updated 16.06.2016. Accessed 06.02.2025, 2025. https://news.un.org/en/story/2016/06/532312
- Cluster C, Initiative R. Intentions Survey; IDP Areas of Origin; August 2018. 2018. 08.2018. Accessed 06.02.2025. https://www.ecoi.net/en/file/local/2001462/reach_irq_factsheet_intentions_area_of_origin_august_2018.pdf
- Taha PH, Sijbrandij M. Gender Differences in Traumatic Experiences, PTSD, and Relevant Symptoms among the Iraqi Internally Displaced Persons. International Journal of Environmental Research and Public Health. 2021;18(18):9779.
- Goodman A, Bergbower H, Perrotte V, Chaudhary A. Survival after sexual violence and genocide: Trauma and healing for Yazidi women in Northern Iraq. Health. 2020;12(06):612.
- Al Shawi AF, Hassen SM. Traumatic events, post-traumatic stress disorders, and gender among Yazidi population after ISIS invasion: A post conflict study in Kurdistan Iraq. International Journal of Social Psychiatry. 2022;68(3):656-661.
- Ahmed DR, Mesbah SM, Al Diab Al Azzawi M, Heun R. Trauma and mental health problems among Iraqi IDPs following the 2014 ISIS Invasion: a systematic review. Medicine, Conflict and Survival. 2024;40(4):366-387.
- Schouler-Ocak M, Laban CJ, Bäärnhielm S, Kastrup MC, Dein S, Wintrob R. Transcultural psychiatry: Refugee, asylum seeker and immigrant patients over the globe. Advances in Psychiatry. 2019:637-655.
- Hassan G, Ventevogel P, Jefee-Bahloul H, Barkil-Oteo A, Kirmayer LJ. Mental health and psychosocial wellbeing of Syrians affected by armed conflict. Epidemiology and Psychiatric Sciences. 2016;25(2):129-141.
- Kizilhan JI, Friedl N, Neumann J, Traub L. Potential trauma events and the psychological consequences for Yazidi women after ISIS captivity. BMC Psychiatry. 2020/05/24 2020;20(1):256. doi:10.1186/s12888-020-02671-4.
- UN Habitat. Iraq Risk Reduction and Rehabilitation. UN Habitat. Accessed 10.08.24, 2024. https://unhabitat.org/iraq-risk-reduction-and-rehabilitation
- Pham PN, Fozouni L, Al-Saiedi A, Coughlin K, Vinck P. Association between distress and displacement settings: a cross-sectional survey among displaced Yazidis in northern Iraq. BMC Public Health. 2021;21:1-11.
- Al Shawi AF, Hassen SM. Traumatic events, post-traumatic stress disorders, and gender among Yazidi population after ISIS invasion: A post conflict study in Kurdistan Iraq. International Journal of Social Psychiatry. 2022;68(3):656-661. doi:10.1177/0020764021994145.
- Wörmer N, Lamberty L. Scattered Dreams: The Independence Referendum, the Fall of Kirkuk and the Effect on Kurdish and Iraqi Politics. 2018:78-91. https://www.kas.de/documents/252038/253252/7_dokument_dok_pdf_52122_2.pdf/0a606c42-1abd-1641-9b4d-44d6cd25eca8?version=1.0&t=1539647624437