





Coronary Calcifications as Prognostic Factors in COVID-19
Coronary Calcifications are a More Relevant Prognostic Factor for Lethality in Patients with COVID-19
M. F. V. V. Aragao 1,2,3,4, M. B. d. Albuquerque 5, J. S. d. Santana 5, D. S. Marques 5, D. C. Perrelli 5, L. C. Nascimento MD 6, J. C. F. Reinaux 2,6, M. M. P. M. L. d. Lima 6, T. R. d. Costa 6, J. E. F. d. Fonte 6, M. C. Leite 6, M. M. Valença 2, M. Marques 5, L. V. Aragao 3,7, J. P. V. Aragao 3,8, F. A. C. Sarmento Neto 6, C. M. S. Campos 2,9, G. N. Leandro 5, P. M. Parizel 10
Abstract
Background: The objective is to evaluate the prognostic factor of lethality of coronary calcifications by the scoring method of overall visual assessment in patients with COVID-19 who underwent chest computed tomography and also evaluate other clinical comorbidities.
Methods: This is a retrospective study that evaluated coronary calcifications scoring by qualitative overall visual inspection of 201 patients with COVID-19 who required Chest computed tomography to evaluate lung complications. The coronary calcifications scoring was analyzed by qualitative evaluation of chest computed tomography scans by radiologists who gave a rating on a scale of 0 to 4 (0= no coronary calcifications CACs; 1= discrete coronary calcifications; 2= moderate coronary calcifications; 3= marked coronary calcifications; 4= stent).
Results: The average age of patients who died from COVID-19 was 59 years (SD = 19) with a significant difference for those who did not die (47.3 years (SD 11.9). The lethality of the sample was 9.0%, being 35.3% in the group with coronary calcifications (scale of 2; 3 and 4), while in the group without coronary calcifications (scale of 0 and 1) it was 6.5% (p= 0.001). It is observed that patients with comorbidities have a statistically significant association with the outcome of death when compared to groups without these comorbidities: systemic arterial hypertension (18.3% vs 5.9% p= 0.009), diabetes mellitus (29% vs 6.2% p= 0.001), dyspnea (15.2% vs 4.7% p=0.025) and chronic renal failure (28% vs 7.2% p=0.06). In the multivariate analysis, coronary calcifications stood out as the main risk factor for the death of patients with COVID-19 (p = 0.030; OR 5.13) followed by diabetes mellitus (p = 0.010; OR 4.71) and chronic kidney failure (p = 0.029; OR 3.98).
Conclusion: Moderate, severe coronary calcifications and stent are the more relevant prognostic factor, being a major risk factor for lethality in patients with COVID-19 in our study.
Keywords
Coronary calcifications, COVID-19, lethality, prognostic factor, comorbidities
1. Introduction
A new pandemic of coronavirus infection called coronavirus disease 2019 (COVID-19) was first detected in December 2019 in the city of Wuhan, China caused by the novel coronavirus SARS-CoV2 virus. It is suggested that this is probably a disease of zoonotic origin, acquired from animals, because of the large number of infected people who were exposed in a public market in that city. The main target of COVID-19 is the human respiratory tract and person-to-person transmission occurs mainly through direct contact via droplets spread by the cough or sneeze of an infected individual. Consequently, COVID-19 spread quickly to all continents, affecting the populations of 240 countries, areas or territories around the world. Despite COVID-19 primarily affects the human respiratory system, it also has been shown that it can involve multiple organ systems, with severe cases resulting in significant morbidity and mortality.
After the fifth year of the onset of this new disease, there is a cumulative total of 777,074,803 confirmed cases of COVID-19 that have determined 7,079,142 deaths around the world. (WHO 15/December/2024). Symptoms related to COVID-19 infection usually appear after an incubation period of about five days. The most common symptoms of COVID-19 are fever, cough and fatigue; other symptoms include headache, haemoptysis and dyspnoea, among others. In more severe cases, patients may develop pneumonia, acute respiratory distress syndrome, acute cardiac complications and death.
Identifying higher-risk groups through clinical, radiological, laboratory and epidemiological factors that may be more closely related to the severe form of COVID-19 and the death of these patients can help prevent complications and fatalities. Thus, the prognosis of these high-risk patients could be improved if, upon initial diagnosis of COVID-19, more intensive medical care were established with earlier and more appropriate treatment for the infection and its complications, seeking to minimize sequelae and fatal cases.
To prevent COVID-19, vaccination was developed and expanded around the world through vaccination campaigns, starting in December 2020. With the development of vaccination, there was a significant reduction in cases of the disease. Furthermore, it was observed that the effect of vaccination mainly protects against the most severe cases of the disease.
From the scientific literature, we were able to identify studies that relate coronary artery calcifications (CACs) and complications in patients with COVID-19. In an article, the authors performed a visual semi-quantitative assessment of chest CT, where they found an association between a higher level of CACs and increased risk of intubation and use of assisted ventilation in patients hospitalised due to COVID-19. Meanwhile, Gupta et al reinforced the importance of qualitative analysis of CAC on non-contrast CT for the prognosis of patients with COVID-19 by finding a correlation between the presence of CAC and a higher risk of intubation and death. Studies in general population before COVID-19 have evaluated risk factors for cardiovascular disease, such as age of patient, hypertension, diabetes, chronic kidney failure and dyslipidaemia. Considering that these comorbidities are factors that predispose to coronary atheromatous disease and consequently to CACs, more studies that evaluate if CACs and/or comorbidity predisposes to an unfavorable outcome in patients with COVID-19 are necessary.
The aim of this retrospective study was to evaluate the risk of lethality in patients with COVID-19 who underwent chest computed tomography (CT) to assess pulmonary complications, analyzing: a) levels of coronary artery calcifications (CACs) on CT scans by the scoring method of overall visual assessment and b) other clinical comorbidities.
2. Materials and Methods
The Institutional Review Board of the Ethics Committee of the “Universidade Federal de Pernambuco” approved this observational, retrospective, cross-sectional study. The Informed Consent was waived.
A survey of the cases was carried out to identify patients with confirmed COVID-19 who had undergone chest Computed Tomography (CT) scan in a radiology department. The radiological and clinical data were retrospectively collected from 01 May 2021 to 23 May 2021. The origin of the data is from a radiological unit in Recife, Pernambuco, Brazil: “Real Hospital Português de Beneficência em Pernambuco” which is a quaternary hospital, and which has become a regional reference regarding the care of COVID-19 patients.
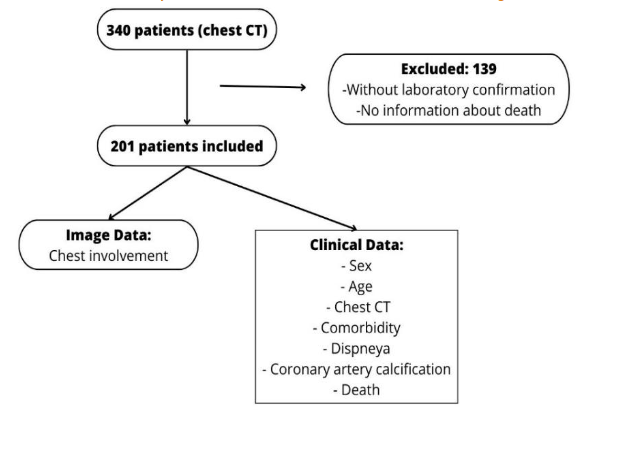
We used a convenience sample of 201 cases from a radiology department, who had undergone chest CT to investigate for COVID-19 complication. The inclusion criteria were laboratory confirmation of COVID-19 disease by reverse transcription polymerase chain reaction real time (RT-PCR) or swab nasal antigen (Figure 1).
The clinical and radiological variables data were retrospectively collected from the medical records. For comparison the patients were divided into two groups: (a) death or (b) not death, evaluating for both selected variables: sex, age, systemic arterial hypertension, diabetes mellitus, dyslipidaemia, chronic kidney failure, dyspnoea, CACs scoring found in the chest CT and the percentual extent of pulmonary lesions found in the chest CT.
In this retrospective study, the radiologists used a qualitative scoring method of overall visual assessment of the CACs in the COVID-19 patients who had undergone chest CT scans due to pulmonary complications. By using chest CT scans performed for evaluation of COVID-19 lung complication, a simple visual assessment of CACs scoring was generated for risk assessment of death. The severity of CACs was assessed by visual inspection in a double-blind study independently by three residents of radiology in third year (JCFR, TRC and MCL) and one radiologist with 28 years of experience (MMPMLL). When there was a discrepancy between the analyses, a fifth radiologist (specialist in thoracic radiology) with 6 years of experience (FACSN), reevaluated the exam and reported the final calcification score.
CACs was defined as hyperdensity at coronary arteries by visual inspection, using the mediastinal window. A qualitative scoring of overall visual assessment of CACs was classified in a scale of 0-4 (0= no calcification; 1= discrete calcification; 2= moderate calcification; 3= severe calcification; 4= stent). Discrete calcification was considered when there were only isolated foci of calcification. Severe calcification was considered when there was a continuous segment of vascular calcification and moderate calcification when it was more than mild, but without criteria for severe.
After retrospective evaluation of chest computed tomography (CT) scans, using qualitative overall visual CAC scoring method (none, mild, moderate and severe CACs and stent), for statistical analysis COVID-19 patients were grouped into two groups called: 1) without CACs (those patients classified as none and mild CACs); 2) with CACs (those patients with moderate and severe CACs and stent).
The institution’s radiologists analysed all chest exams, and the qualitative score of pulmonary opacities of COVID-19 patterns (viral pneumonia) was performed independently, classifying the findings into: (a) less than 25%, (b) between 25% and 50% or (c) equal to or greater than 50%. Our study considered only the evaluation of chest CT reports by radiologists at the Institution.
2.1. STATISTICAL ANALYSIS
Softwares SPSS 21.0 (Statistical Package for the Social Sciences) for Windows and Excel 2010 were used. All tests were applied with a 95% confidence. The results are presented in Table 1 with their absolute and relative frequencies respectively. The numerical variables are represented by measures of central tendency and measures of dispersion. To verify the existence of an association, Fisher’s Exact Test for categorical variables was applied. T-student test was used for the analysis of patient age when comparing the mean between the groups (deaths and non-deaths). The p < 0.05 was considered statistical significance. A multivariate logistic regression model considering death as the dependent variable was constructed using the independent variables that presented a p-value < 0.10 in the univariate analysis and presented in the Table 2.
3. Results
We analysed the profiles of the 201 COVID-19 patients included in this study which are shown on Table 1. For comparison, the patients were divided into two groups: (a) death or (b) not death. Patients who died with COVID-19 were statistically significantly older.
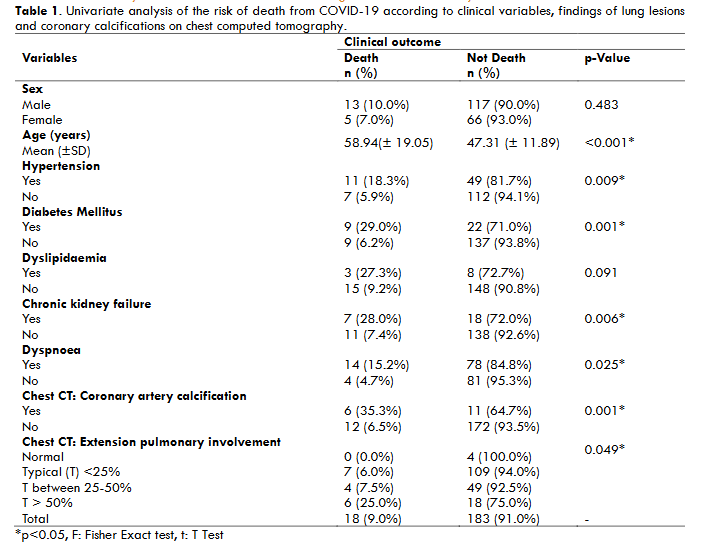
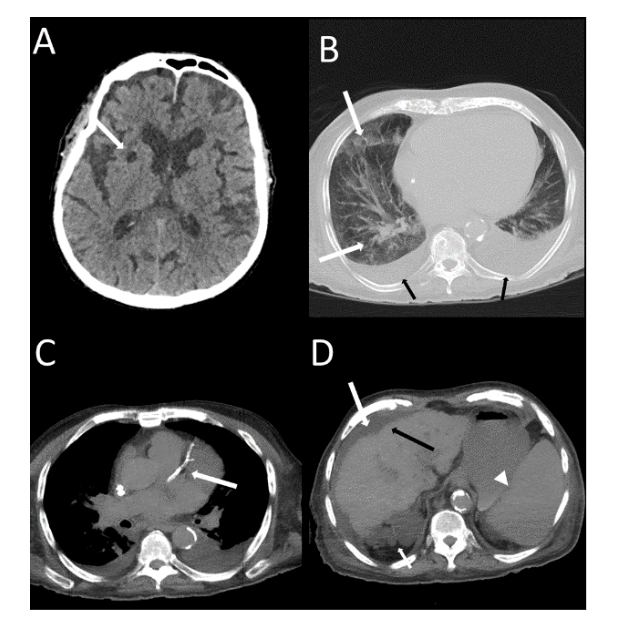
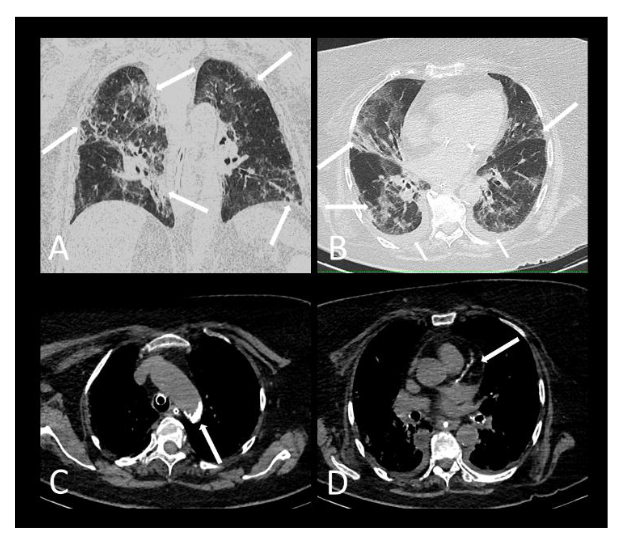
A greater frequency of deaths was found in males compared to females without statistical significance. However, the patients who died (Figure 2 and 3) with statistical significance were older and more frequently presented systemic arterial hypertension, diabetes mellitus, chronic kidney failure, dyspnoea, more than 50% extension pulmonary involvement and moderate-severe CACs or coronary arterial stent.
Based on logistic regression using multivariate analysis, it was found that patients with diabetes were approximately 4.7 times more likely to die from COVID-19 than patients without diabetes mellitus. While patients with chronic kidney disease are approximately 4 times more likely to die than patients without chronic kidney failure. In the analysis, CACs highlighted as the main risk factor for the death of patients with COVID-19, in which patients who had severe, moderate CACs or stents were 5 times more likely to die than patients without CACs or with discreet CACs.

4. Discussion
In this retrospective study, by using chest CT scans performed for evaluation of COVID-19 lung complication, a simple visual overall assessment of CACs scoring could be generated for risk assessment of death. We observed an association between the group denominated with presence of CACs (moderate and severe CACs and stent) and patient lethality. Patients who died due to COVID-19 were older and more frequently presented with systemic arterial hypertension, diabetes mellitus, chronic renal failure, dyspnoea and more than 50% extensive lung involvement on chest CT.
We also found that patients with CACs (moderate, severe or stent) are approximately 5 times more likely to die than patients without CACs. Patients with diabetes are approximately 4.7 times more likely to die from COVID-19 than patients without diabetes mellitus. While patients with chronic kidney disease are approximately 4 times more likely to die than patients without chronic kidney failure.
It is known that the SARS-Cov-2 can cause respiratory infections and it can lead to viral pneumonia and acute respiratory distress. Currently, COVID-19 is associated with a high inflammatory burden that can induce vascular inflammation, myocarditis, and cardiac arrhythmias. Nevertheless, the role of presence of atherosclerosis and vascular calcification in the prognosis of COVID-19 patients it is not well defined in the literature. Few studies have described the correlation between coronary calcification and the bad prognosis in COVID-19 patients. Our findings are in accordance with what was described by Colombi and collaborators that coronary artery calcification is associated with a greater probability of fatal incidents and that CT metrics were better predictors of death in comparison to clinical model.
The group with presence of moderate and severe CACs and stent was statistically significant on the risk of death from COVID-19, regardless of age and/or history of comorbidities such as hypertension, diabetes, dyslipidaemia and chronic kidney failure. Although the patients who died were older with significance in the univariate analysis (the age is also a factor in the development of coronary heart disease), in our study, the multivariate logistic regression analysis excluded age as a statistically significant variable for the death outcome.
Our findings agree with Gupta et al. who found in CT scans of the chest of patients with COVID-19 a greater probability of the individuals with coronary calcification needing intubation and dying, when compared to the group without calcification. These authors also highlighted that the increase in the degree of calcification was related to a higher risk of intubation. However, they found that the presence of stent, as a separated group, did not demonstrate statistical significance on the risk of intubation or death from COVID-19.
These findings are in line with the literature report in which older patients and/or with a history of hypertension, diabetes, obesity, chronic kidney disease or lung diseases had a worse prognosis and greater chance of death. Kotlo et al reported that the presence of CACs is associated with an increase in hospital admission to an Intensive Care Unit and/or use of mechanical ventilation in patients with COVID-19. Furthermore, the authors found that patients with severe CACs, regardless of previous heart disease, were at high risk of morbidity and mortality from COVID-19. Dillinger et al. also demonstrated an association between the presence of coronary calcifications and a worse prognosis for patients hospitalised with COVID-19. The authors further highlight that this may be due to the potential of COVID-19 to exacerbate the severity of immune response, endothelial dysfunction, and myocardial stress in patients with a previous history of subclinical coronary atherosclerosis.
The presence of the dyspnoea symptom was also associated with the lethality of patients with COVID-19. Qiu et al also reported that patients with dyspnoea were more vulnerable to death. The authors associated this with the fact that dyspnoea is a sign of reduced lung function and hypoxia, which places them in a greater need for surveillance to prevent a worse prognosis.
As our study is retrospective, information was collected from patients’ medical records that did not contain any information about the virus strain. However, in May 2021 the strains in circulation in Brazil were, Alpha (B.1.1.7), Beta (B.1.351), Gamma (P.1) and Delta (B.1.617.2). The limitation of our study is that it is retrospective. The variables analysed were not always noted down in the medical records of all patients.
Regarding mortality, Magro and collaborators found that age, sex and C-reactive protein at day 1 are predictors as possible risk factors but, transaminases were not predictors for mortality in COVID-19 patients. Another interesting study supported the existing data that high load of inflammatory markers is associated with more severe COVID-19 lung disease and indirectly high mortality. This study found that three markers (interleukin 6, serum ferritin and lactate dehydrogenase) have significant relation with chest CT severity of pulmonar lesions. However, our study did not aim to evaluate inflammatory markers.
A limitation of our study was that the coronary arteries were evaluated on chest CT using the protocol for evaluating lung parenchyma. A major concern here it’s that chest CT is not intended for the evaluation of coronary artery disease but coronary angiotomography, therefore, lacking of a comparison against a gold standard, results might lead to erroneous conclusions.
On the other hand, our study suggests that in addition to evaluation of pulmonary lesion involvement, the identification of moderate, severe CACs or stent on the same non-contrast chest CT scan will help to estimate the patient’s higher risk in the acute phase of COVID-19, alerting for greater medical care. It can also serve as an indicator for the need to continue the investigation, when possible, with an adequate coronary evaluation through a calcium scoring protocol, coronary CT angiography or coronary arteriography.
So, an initial qualitative evaluation of coronary arteries through chest CT can serve as a screening for CACs, which will also serve as another imaging marker of the patient’s prognosis in addition to the quantification of pulmonary lesions, in COVID-19 patients who are worsening and being investigated. Chest TC scan can be easily reproduced anywhere in the world without the need for advanced software.
In this sense, our work contributes by reinforcing the existence of an association between the presence of moderate and severe CACs and stent and the greater risk of lethality in patients with COVID-19. These patients have about a 5 times greater chance of death. We also found a higher risk of death in diabetic patients or chronic renal failure in logistic regression.
In this way, we hope that our findings can be used as a scientific basis for the use of antivirals, early hospitalisations and other more intensive treatments in patients positive for COVID-19 and who are at greater risk of developing a severe form of the disease to avoid serious sequelae and death.
We recommend prospective studies have a larger sample of COVID-19 patients. More people with without CACs and with CACS are needed to confirm our findings about the risk factors which lead to the development of a severe form of the COVID-19 disease in the with CACs group.
5. Conclusion
In this retrospective study, by using chest CT scans without contrast performed for evaluation of COVID-19 lung complication, a simple visual overall assessment of CACs scoring could be generated for risk assessment of death. We observed that the presence of moderate and severe CACs and the presence of stent are the more relevant prognostic factor. A stronger association was observed between the group denominated with presence of CACs (moderate, severe CACs and stent) and patient lethality. Patients who died due to COVID-19 were older and more frequently presented with systemic arterial hypertension, diabetes mellitus, chronic renal failure, dyspnoea and more than 50% extensive lung involvement on chest CT. The group of patients with CACs (moderate, severe CACs or stent) are approximately 5 times more likely to die than patients without calcification. Patients with diabetes are approximately 4.7 times more likely to die from COVID-19 than patients without diabetes mellitus. While patients with chronic kidney disease are approximately 4 times more likely to die than patients without chronic kidney failure.
Funding for this study
The medicine student Matheus Barros de Albuquerque received scholarship from Institutional Scientific Initiation Scholarship Programme (PIBIC) and Institutional Scientific Initiation Scholarship Programme (PROPESQI). The research advisor of this PIBIC is Prof. Dr. Maria de Fátima Viana Vasco Aragão, who, however, did not receive any funding.
Conflicts of interest
The authors wish to confirm that there are no known conflicts of interest associated with this publication and there has been no financial support for this work that could have influenced its outcome.
Ethical statement
This research was submitted and approved by the Ethics Committee for Research on Human Beings of the Center for Health Sciences, Federal University of Pernambuco – Brazil, under Opinion 5,708,786 on October 19, 2022.
6. References
- Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395(10223):497-506.
- World Health Organization. WHO COVID-19 dashboard. WHO. Published December 15, 2024. Accessed January 2, 2025. https://data.who.int/dashboards/covid19/cases?n=o
- Kelso JM. Anaphylactic reactions to novel mRNA SARS-CoV-2/COVID-19 vaccines. Vaccine. 2021;39:865-867.
- Ramos AM, Almeida A, Silva P, et al. Modeling the impact of SARS-CoV-2 variants and vaccines on the spread of COVID-19. Commun Nonlinear Sci Numer Simul. 2021;102:105937.
- Lopez Bernal J, Andrews N, Gower C, et al. Effectiveness of the Pfizer-BioNTech and Oxford-AstraZeneca vaccines on COVID-19 related symptoms, hospital admissions, and mortality in older adults in England: test negative case-control study. BMJ. 2021;373:n1088.
- Zhang JJ, Dong X, Cao YY, et al. Risk and protective factors for COVID-19 morbidity, severity, and mortality. Clin Rev Allergy Immunol. 2023;64(1):90-107.
- Colombi D, Bodini FC, Petrini M, et al. Qualitative and quantitative chest CT parameters as predictors of specific mortality in COVID-19 patients. Emerg Radiol. 2020;27:701-710.
- Nair AV, Kumar D, Yadav SK, et al. Utility of visual coronary artery calcification on non-cardiac gated thoracic CT in predicting clinical severity and outcome in COVID-19. Clin Imaging. 2021;74:123-130. doi:10.1016/j.clinimag.2021.01.015
- Gupta YS, Finkelstein M, Manna S, et al. Coronary artery calcification in COVID-19 patients: an imaging biomarker for adverse clinical outcomes. Clin Imaging. 2021;77:1-8. doi:10.1016/j.clinimag.2021.02.016
- Munzel T, Sorensen M, Gori T, et al. Environmental risk factors and cardiovascular diseases: a comprehensive expert review. Cardiovasc Res. 2022;118(14):2880-2902.
- Adedinsewo DA, Carter RE, Attia ZI, et al. Racial and ethnic disparities in cardiovascular disease risk among patients with chronic kidney disease. Curr Cardiovasc Risk Rep. 2022;16(11):145-157.
- Chiles C, Duan F, Gladish G et al Association of Coronary Artery Calcification and Mortality in the National Lung Screening Trial: A Comparison of Three Scoring Methods Radiology 2015 276:1, 82-90
- Zhou P, Yang XL, Wang XG, et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature. 2020;579(7798):270-273. doi:10.1038/s41586-020-2012-7
- Madjid M, Safavi-Naeini P, Solomon SD, Vardeny O. Potential effects of coronaviruses on the cardiovascular system: a review. JAMA Cardiol. 2020;5(7):831-840. doi:10.1001/jamacardio.2020.1286
- Sanyaolu A, Okorie C, Marinkovic A, et al. Comorbidity and its impact on patients with COVID-19. SN Compr Clin Med. 2020;2:1069-1076.
- Aragao MdFVV, Leal MdC, Andrade PHP, et al. Clinical and radiological profiles of COVID-19 patients with neurological symptomatology: a comparative study. Viruses. 2021;13(5):845. doi:10.3390/v13050845
- Kotlo S, Thorgerson A, Kulinski J. Coronary artery calcification as a predictor of adverse outcomes in patients hospitalized with COVID-19. Am Heart J Plus. 2023;28:100288.
- Dillinger JG, Dubreuil O, Hober C, et al. Coronary artery calcification and complications in patients with COVID-19. Cardiovasc Imaging. 2020;13(11):2468-2470.
- Qiu P, Zhou Y, Wang F, et al. Clinical characteristics, laboratory outcome characteristics, comorbidities, and complications of related COVID-19 deceased: a systematic review and meta-analysis. Aging Clin Exp Res. 2020;32:1869-1878.
- Imai M, Halfmann PJ, Yamayoshi S, et al. Characterization of a new SARS-CoV-2 variant that emerged in Brazil. Proc Natl Acad Sci USA. 2021;118:e2106535118.
- Marquitti FMD, Covas DT, Dias C, et al. Brazil in the face of new SARS-CoV-2 variants: emergencies and challenges in public health. Rev Bras Epidemiol. 2021;24:e210022. doi:10.1590/1980-549720210022
- Magro B, Tacelli M, Pasulo L, et al. Role of transaminases, CRP, and LDH in COVID-19 patients with and without respiratory failure during the disease outbreak. Med Res Arch. 2021;9(12). doi:10.18103/mra.v9i12.2593
- Parrey A, Ahangar AG, Wani AH, et al. COVID-19 severity correlation between inflammatory markers and high-resolution computerised tomography. Med Res Arch. 2021;9(12). Accessed February 17, 2025. https://doi.org/10.18103/mra.v9i12.2619