






COVID-19 Reinfection Risks in Long-Term Opioid Users
Risk of COVID-19 reinfection and its severe complications in adults treated with long-term opioids for chronic non-cancer pain
1. Introduction
Since December 2019, over 770 million cases and over 6.9 million deaths attributed to SARS-CoV-2 infection have been reported globally¹. The pandemic has disproportionately affected populations impacted by chronic health issues, including people with chronic non-cancer pain²˒³. Research has shown the COVID-19 pandemic increased the burden of chronic pain, with worsened social isolation, economic stress, anxiety, and disrupted access to pain management contributing to this distress⁴˒⁵. Pharmacological treatments, including long-term opioid therapy (LTOT), are a part of standard care in chronic non-cancer pain⁶˒⁷, with an increase in opioid medication use for managing chronic pain noted likely in compensation for stopping physical/psychological treatments due to the pandemic⁵˒⁸.
To date, research evaluating the relationship between opioid use and COVID-19 infection outcomes has primarily focused on persons with an opioid use disorder (OUD), showing increased risk of complications due to the COVID-19 infection in this population⁹⁻¹¹. Opioids can cause acute respiratory depression and compromise immune system¹²˒¹³, which has been identified as a risk factor for severe COVID-19 complications¹⁴. As additional SARS-CoV-2 variants emerged that can evade prior immunity, rates of COVID-19 reinfection have increased over the past 3 years¹⁵˒¹⁶. Reinfection with COVID-19 has been associated with greater risk of intensive care unit (ICU) admission, mechanical ventilation, and development of chronic physical and mental health sequelae¹⁷˒¹⁸. Despite recent advancement in vaccines and treatments for COVID-19, concerns remain about waning immunity against SARS-CoV-2 virus and its variants and reinfection, especially among individuals at an already-higher risk of COVID-19 complications, such as adults treated for chronic pain with LTOT.
Moreover, the literature has shown elevated risk of mortality and healthcare utilization after initial COVID-19 infection among people prescribed opioids¹⁹˒²⁰. Many people on opioid treatment also experience medical comorbidities (diabetes, obesity/overweight, cardiovascular disease, chronic kidney disease, chronic liver disease, chronic lung disease, immune problems, sickle cell disease)¹⁹˒²¹, mental health conditions (anxiety, bipolar, dementia, depression)¹⁰, and substance use (alcohol, drugs, tobacco/nicotine) disorders, which have been documented as important moderators for poor COVID-19 outcomes. To better understand the relationship between COVID-19 and opioid-related treatment, this retrospective cohort study leveraged TriNetX, a large existing database of electronic health records (EHRs), to assess the risk of COVID-19 reinfection and its severe complications within 30 days of the reinfection onset among adults treated with LTOT for chronic non-cancer pain in the U.S.
2. Methods
2.1. STUDY DESIGN AND DATA SOURCE
This study utilized a retrospective cohort design using EHRs from the TriNetX database (Cambridge, MA), a global health data network containing de-identified EHRs (e.g., demographic, diagnosis, procedure, medication, and laboratory information) of more than 80 million patients from 57 participating healthcare organizations predominately from the U.S. TriNetX research data have undergone extensive curation and mapping to common clinical entities and terminologies to ensure high usability as well as consistency with the Reporting of Studies Conducted using Observational Routinely collected Data (RECORD) guidelines²². Because the TriNetX database consists of deidentified standard data elements defined and processed in compliance with Sections §164.514(a) and §164.514(b)(1) of the HIPAA Privacy Rule, the Institutional Review Board of the Pennsylvania State University determined that the use of the TriNetX data does not require the IRB approval.
2.2. STUDY POPULATION
Individuals eligible for the analysis were adults ≥18 years old diagnosed with COVID-19 between January 1, 2020 and April 30, 2022 (study enrollment period) and either meeting criteria for being classified to the LTOT or the Control cohorts. The diagnosis of a COVID-19 illness was based on the presence of both COVID-19 diagnosis and a positive laboratory test result documented in the EHR (see Supplemental Table S1 for details)¹⁹˒²³. Eligible patients’ health data were extracted through June 30, 2022, yielding the study assessment period to span January 1, 2020 and June 30, 2022; this approach allowed to capture potential COVID-19 reinfection-related events, defined as occurring with 30 days of the initial infection, in all study participants. Individuals were ineligible if they had diagnoses of opioid use disorder (OUD) or cancer, or lived in nursing homes or palliative care facilities prior to their first COVID-19 infection to exclude those treated with opioids for OUD or cancer or terminal illness related care.
2.3. TREATMENT AND CONTROL COHORTS
The LTOT cohort comprised adults who had been issued at least three outpatient prescriptions for opioid medications, and the Control cohort included adults who were not prescribed any opioids within six months prior to their first COVID-19 infection noted during the study assessment period. Therefore, some of the opioid medications could have been prescribed before January 2020 if study participants experienced the first COVID-19 illness in the first few months of the assessment period.
Prescription opioids included agonists and partial agonists prescribed as monotherapy or a combination medication in a form compatible with outpatient prescribing for chronic non-cancer pain¹⁹˒²⁴. Although buprenorphine and methadone are used to treat OUD, our analysis excluded patients with OUD diagnoses; in addition, methadone prescriptions are assumed to be issued for chronic pain, because only opioid treatment programs are allowed to dispense methadone as treatment for OUD in the outpatient settings. The study identified opioid medications using normalized name and code sets for medications based on the Prescription for Electronic Drug Information Exchange (RxNorm)²⁵. The list of RxNorm codes is provided in Supplemental Table S1.
2.4. OUTCOME MEASURES OF COVID-19 REINFECTION AND ITS SEVERITY
The first COVID-19 infection episode during the study assessment period was considered the “index” infection. A COVID-19 reinfection (i.e., a new infection with SARS-CoV-2) was defined as a COVID-19 infection documented at least 30 days after the index infection date. Severe COVID-19 complications were defined as presence of an emergency department (ED), hospital or intensive care unit (ICU) admission, or death within 30 days of the reinfection. Presence of COVID-19 reinfection and its severe complications were assessed through dichotomous (yes/no) metrics for each of the variables of interest.
2.5. BASELINE CHARACTERISTICS
Demographic and health comorbidity data were extracted at the time of the index COVID-19 infection date for each study participant. The available demographic data included sex (male/female), age group (18-39, 40-64, 65+), ethnicity (Hispanic/non-Hispanic) and race (White/Black/Other). Data on comorbid conditions known to be associated with the increased risk of severe COVID-19 complications included the diagnoses of chronic medical (diabetes, obesity/overweight, cardiovascular disease, chronic kidney disease, chronic liver disease, chronic lung disease, immune problems, sickle cell disease)¹⁹˒²¹, mental health (anxiety, bipolar, dementia, depression)¹⁰, and substance use (alcohol, drugs, tobacco/nicotine) disorders. Presence of the tobacco/nicotine use disorder diagnoses served as the proxy of smoking/tobacco status, which is not a part of available EHR data. Detailed information on the diagnostic codes for the conditions extracted in this study is provided in Supplemental Table S1.
2.6. STATISTICAL ANALYSIS
Summary statistics were computed to describe the baseline characteristics and outcome measures of the study sample and by the cohort status. Between-cohort differences at baseline were compared using the t-test for continuous and chi-square for categorical normally-distributed variables (or equivalent non-parametric tests for non-normally distributed variables). Multiple logistic regression modeling was utilized to assess the risk of COVID-19 reinfection and its severe complications, when controlling for baseline demographic and comorbid condition characteristics. The regression analysis was conducted using the Maximum Likelihood Estimation method to estimate the adjusted odds ratios (aORs), Wald 95% confidence intervals (CIs) for the coefficients, and p-values for each outcome variable to estimate the risk of a given outcome. The significance level was determined based on two-tailed p-value < 0.05. All statistical analyses were performed using PROC LOGISTIC procedure (Version 9.4 SAS Institute Inc., Carey, NC).
3. Results
3.1. STUDY SAMPLE CHARACTERISTICS
The study sample consisted of 2,120,701 adults diagnosed with COVID-19 between January 1, 2020 and June 30, 2022, including 36,265 individuals in the LTOT and 2,084,436 individuals in the Control cohort. Compared to the Control cohort, the LTOT cohort had a statistically significantly greater percentage of individuals who were younger, males, non-Whites, and had a higher burden of chronic medical/mental health conditions and substance use disorders, known risk factors for COVID-19 complications (Table 1).
3.2. RISK OF COVID-19 REINFECTION AND ITS SEVERE COMPLICATIONS
During the study assessment period, approximately 50.1% (18,150) of patients in the LTOT cohort had a documented COVID-19 reinfection compared to 28.6% (596,790) of patients in the Control cohort (p<0.01). Among those with COVID-19 re-infection, adults in the LTOT cohort, compared to the Control cohort, also had a greater frequency (p<0.01) of the ED visits, hospital and ICU admissions, and mortality within 30 days of COVID-19 reinfection (Table 2).
Table 1. Baseline characteristics of the study sample: Adults with COVID-19 infection
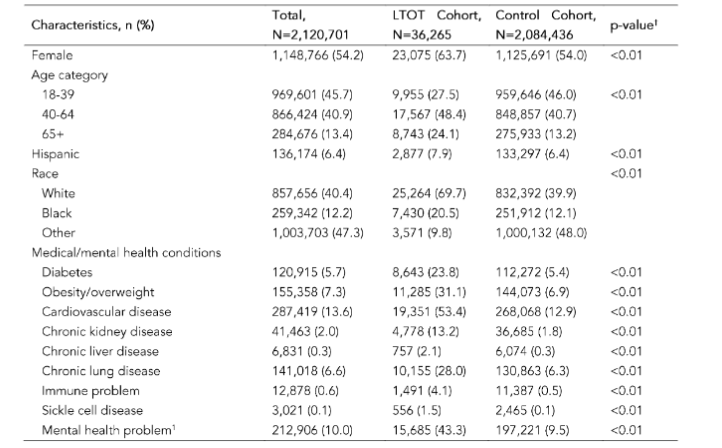

¹Chi-square statistics were computed to evaluate differences in proportions between the cohorts.
¹Mental health problem included anxiety, bipolar disorder, dementia, depression, and ADHD.
²Other drug use disorders included cannabis, sedative, cocaine, stimulant, hallucinogen, inhalant, or psychoactive drug use disorders, and excluded opioid, alcohol, and nicotine/tobacco use disorders.
Table 2. COVID-19 reinfection and its severe complications: frequency within the study sample and by the cohort status
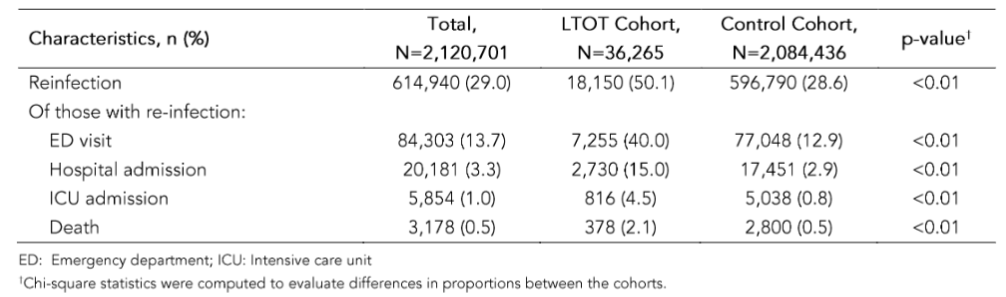
ED: Emergency department; ICU: intensive care unit
¹Chi-square statistics were computed to evaluate differences in proportions between the cohorts.
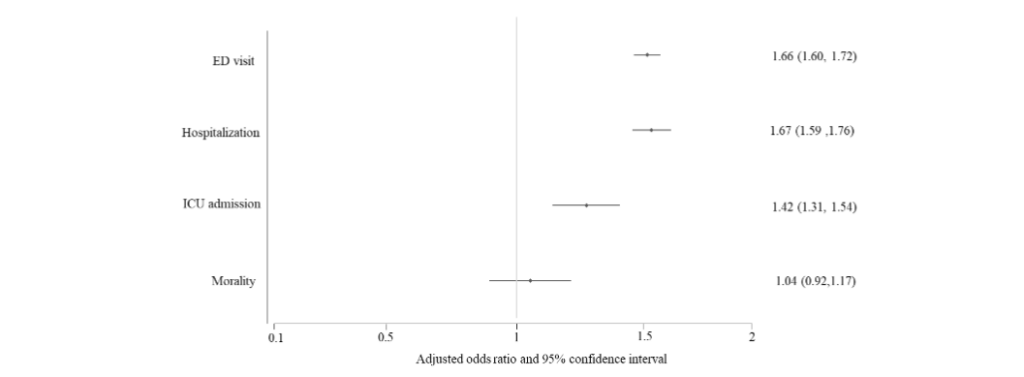
The logistic regression analysis, controlling for baseline characteristics, revealed that, compared to the Control cohort, the LTOT cohort had an increased likelihood of COVID-19 re-infection (aOR=2.75, 95% CI: 2.69, 2.81; p<0.01). After being re-infected, the LTOT cohort, compared to those in the Control cohort, was also more likely to have an ED visit (aOR=1.66, 95% CI: 1.60, 1.72; p<0.01), and be admitted to a hospital (aOR=1.67, 95% CI: 1.59, 1.76; p<0.01) and ICU (aOR=1.42, 95% CI: 1.31, 1.54; p<0.01) within 30 days of reinfection (Figure 1). No statistically significant differences in 30-day mortality rates were noted between the cohorts (aOR=1.04, 95% CI: 0.92, 1.17; p=0.50). The details of the statistical models and their outputs for each outcome measure are provided in Supplemental Table S2.
Figure 1. Logistic regression analysis: the likelihood of severe complications within 30 days of the COVID-19 reinfection among adults treated with long-term opioid therapy versus those not treated with opioid medications.
4. Discussion
This retrospective cohort study, based on a secondary analysis of large EHR research database with over 2.1 million adults with COVID-19 infection in the U.S., revealed that adults with LTOT-treated chronic non-cancer pain are at a greater risk of reinfection with COVID-19 and, once re-infected, were more likely to require ED, hospital, and ICU care. These findings extend the evidence from prior research, which indicated that individuals on LTOT were at increased risk to experience a COVID-19 illness and associated worse outcomes¹⁹˒²⁶. Together, these results suggest that persons on LTOT are more likely to become infected and re-infected, and, once infected by SARS-CoV-2, are more likely to become severely ill. The increased utilization of emergency, hospital and critical care services, caused by these infections and reinfections has imposed additional strain on limited healthcare resources, especially in communities that are already underserved and disproportionately affected by the pandemic.
The COVID-19 pandemic has led to unprecedented public health challenges and harms, with an especially heavy toll among individuals treated with LTOT for refractory, severe chronic pain⁸˒¹⁹. Prior research has shown that individuals on long-term opioid treatment often experience underlying health issues that can compromise their immune system or overall health, making it harder for the body to cope with additional stressors like a severe viral infection. Essentially, the combination of compromised respiratory function, underlying health issues, potential impacts on immune response, and lifestyle factors contribute to the increased risk of severe COVID-19 infection in those prescribed opioid medication¹⁹. Together with the findings of increased risk for both COVID-19 illness and its severe complications among adults with LTOT, this underscores the need to consider LTOT prescribed for chronic pain as a risk factor for worse outcomes when evaluating and managing patients with a COVID-19 infection. Although chronic non-cancer pain treated with LTOT is not currently listed by the Centers for Disease Control and Prevention as one of recognized risk factors for more severe COVID-19 illness²⁷, the finding of the study can be clinically applied when counseling adults with LTOT-treated chronic pain about the importance of COVID-19 prevention strategies.
The strengths of this study include a large sample size and reliance on clinically-relevant, real-life data. Utilizing a large database enabled us to estimate the risk for COVID-19 reinfection and its sequelae in individuals prescribed LTOT while accounting for a range of demographic, medical, and mental health characteristics to strengthen the validity of our findings, and minimize the potential impact of confounding and bias.
Despite its strengths, this study has several important limitations. First, the COVID-19 diagnosis and testing records would not have been captured in the TriNetX database if the diagnosis was established at facilities outside of participating research data network, potentially causing selection bias. Second, the study used retrospective observational data; the lack of prospective, randomized design could have affected the outcome validity. In addition, although the existing social determinants of health are critical for predicting future health outcomes²⁸˒²⁹, the TriNetX-based research data do not contain information on patient socioeconomic contexts (e.g., health insurance, education or income levels) that could be important confounders in the analyses. Future prospective studies and secondary database analyses using advanced data mining techniques or machine learning algorithms, and accounting for social determinants of health information could provide more insight and better account for important confounders.
5. Conclusion
Findings from this retrospective cohort study, leveraging EHRs from a large national research database, indicated that adults treated with LTOT for chronic non-cancer pain are at increased risk for COVID-19 reinfection and its severe complications, requiring ED, hospital, and ICU care. These results can help guide clinical decisions when caring for patients treated with LTOT regarding the prevention as well as monitoring and treatment of COVID-19 re-infection.
Contributors
All authors were involved in revisions, read and approved the final manuscript. WJT contributed to the planning and design of the work, literature review, data analysis, interpretation, and writing the manuscript. MP, CH, GH, KB, AVR contributed to literature review, data analysis, interpretation, and writing the manuscript. AEZ contributed to study design, data analysis, interpretation, and writing the manuscript.
Funding
The author(s) received no funding support for the research, authorship, and/or publication of this article.
Competing interests
None declared.
Ethic approval
All the data queries were performed in the TriNetX online portal managed by the Penn State Clinic and Translational Science Institute. Because there was no protected health information data accessed in the analysis, this research was determined to be exempt from the Institutional Review Board oversight.
Patient and public involvement
Patients and the public were not involved in the design, conduct, reporting, or dissemination of the study.
Provenance and peer review
Not commissioned; externally peer reviewed.
Data availability statement
No data are available
References
1. World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Accessed October 26, 2023. https://covid19.who.int
2. Shanthanna H, Nelson AM, Kissoon N, Narouze S. The COVID-19 pandemic and its consequences for chronic pain: a narrative review. Anaesthesia. 2022;77(9):1039-1050. doi:10.1111/anae.15801
3. Lavin A, LeBlanc F, El Helou A. The impact of COVID-19 on chronic pain. Front Pain Res Lausanne Switz. 2023;4:1234099. doi:10.3389/ fpain.2023.1234099
4. Consonni M, Telesca A, Grazzi L, Cazzato D, Lauria G. Life with chronic pain during COVID-19 lockdown: the case of patients with small fibre neuropathy and chronic migraine. Neurol Sci Off J Ital Neurol Soc Ital Soc Clin Neurophysiol. 2021 ;42(2):389-397. doi:10.1007/s10072-020-04890-9
5. Lacasse A, Pagé MG, Dassieu L, et al. Impact of the COVID-19 pandemic on the pharmacological, physical, and psychological treatments of pain: findings from the Chronic Pain & COVID-19 Pan-Canadian Study. Pain Rep. 2021;6(1):e891. doi:10. 1097/PR9.0000000000000891
6. Turk DC, Wilson HD, Cahana A. Treatment of chronic non-cancer pain. Lancet Lond Engl. 2011; 377(9784):2226-2235. doi:10.1016/S0140-6736(11 )60402-9
7. Boudreau D, Von Korff M, Rutter CM, et al. Trends in long-term opioid therapy for chronic non-cancer pain. Pharmacoepidemiol Drug Saf. 2009;1 8(12):1166-1175. doi:10.1002/pds.1833
8. Zgierska AE, Burzinski CA, Garland EL, et al. Experiences of adults with opioid-treated chronic low back pain during the COVID-19 pandemic: A cross-sectional survey study. Medicine (Baltimore). 2023;102(41):e34885. doi:10.1097/MD.0000000000034885
9. Wang QQ, Kaelber DC, Xu R, Volkow ND. COVID-19 risk and outcomes in patients with substance use disorders: analyses from electronic health records in the United States. Mol Psychiatry. 2021;26(1):30-39. doi:10.1038/s41380-020-00880-7
10. Wang Q, Xu R, Volkow ND. Increased risk of COVID-19 infection and mortality in people with mental disorders: analysis from electronic health records in the United States. World Psychiatry Off J World Psychiatr Assoc WPA. 2021;20(1):124-130. doi:10.1002/wps.20806
11. Jamali Z, Emamian MH, Hashemi H, Fotouhi A. The Association of Opioid Use Disorder and COVID-19, a Longitudinal Study. Int J Prev Med. 2022;13:157. doi:10.4103/ijpvm.ijpvm_68_22
12. Dahan A, Aarts L, Smith TW. Incidence, Reversal, and Prevention of Opioid-induced Respiratory Depression. Anesthesiology. 2010;112 (1):226-238. doi:10.1097/ALN.0b013e3181c38c25
13. Wiese AD, Grijalva CG. The use of prescribed opioid analgesics & the risk of serious infections. Future Microbiol. 2018;13(8):849-852. doi:10.2217 /fmb-2018-0101
14. Schimmel J, Manini AF. Opioid Use Disorder and COVID-19: Biological Plausibility for Worsened Outcomes. Subst Use Misuse. 2020;55(11):1900-1901. doi:10.1080/10826084.2020.1791184
15. Ren X, Zhou J, Guo J, et al. Reinfection in patients with COVID-19: a systematic review. Glob Health Res Policy. 2022;7(1):12. doi:10.1186/s4125 6-022-00245-3
16. SeyedAlinaghi S, Mirzapour P, Dadras O, et al. Characterization of SARS-CoV-2 different variants and related morbidity and mortality: a systematic review. Eur J Med Res. 2021;26(1):51. doi:10.1186 /s40001-021-00524-8
17. Dhillon RA, Qamar MA, Gilani JA, et al. The mystery of COVID-19 reinfections: A global systematic review and meta-analysis. Ann Med Surg 2012. 2021;72:103130. doi:10.1016/j.amsu.2 021.103130
18. Bowe B, Xie Y, Al-Aly Z. Acute and postacute sequelae associated with SARS-CoV-2 reinfection. Nat Med. 2022;28(11):2398-2405. doi:10.1038/s41 591-022-02051-3
19. Tuan WJ, Spotts H, Zgierska AE, Lennon RP. COVID-19 outcomes among adult patients treated with long-term opioid therapy for chronic non-cancer pain in the USA: a retrospective cohort study. BMJ Open. 2021;11(11):e056436. doi:10.11 36/bmjopen-2021-056436
20. Shah R, Kuo YF, Baillargeon J, Raji MA. The impact of long-term opioid use on the risk and severity of COVID-19. J Opioid Manag. 2020;16(6) :401-404. doi:10.5055/jom.2020.0597
21. Yek C, Warner S, Wiltz JL, et al. Risk Factors for Severe COVID-19 Outcomes Among Persons Aged ≥18 Years Who Completed a Primary COVID-19 Vaccination Series – 465 Health Care Facilities, United States, December 2020-October 2021. MMWR Morb Mortal Wkly Rep. 2022;71(1):1 9-25. doi:10.15585/mmwr.mm7101a4
22. Benchimol EI, Smeeth L, Guttmann A, et al. The REporting of studies Conducted using Observational Routinely-collected health Data (RECORD) Statement. PLOS Med. 2015;12(10):e10 01885. doi:10.1371/journal.pmed.1001885
23. Latronica JR, Clegg TJ, Tuan WJ, Bone C. Are Amphetamines Associated with Adverse Cardiovascular Events Among Elderly Individuals? J Am Board Fam Med JABFM. 2021;34(6):1074-1081. doi:10.3122/jabfm.2021.06.210228
24. Tuan WJ, Sehgal N, Zgierska AE. Using electronic health record’s data to assess daily dose of opioids prescribed for outpatients with chronic non-cancer pain. Fam Med Community Health. 2021;9(Suppl 1):e001277. doi:10.1136/fmch-2021-001277
25. Nelson SJ, Zeng K, Kilbourne J, Powell T, Moore R. Normalized names for clinical drugs: RxNorm at 6 years. J Am Med Inform Assoc JAMIA. 2011;18(4):441-448. doi:10.1136/amiajnl-2011-000116
26. Khani S, Tafaroji J, Yaghoubi M, Emami Kazemabad MJ, Hejazi SA. Prevalence of COVID-19 outcomes in patients referred to opioid agonist treatment centers. Front Pharmacol. 2023;14:1105 176. doi:10.3389/fphar.2023.1105176
27. U.S. Centers for Disease Control and Prevention. COVID-19 and Your Health. Centers for Disease Control and Prevention. February 11, 2020. Accessed March 6, 2022. https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/people-with-medical-conditions.html
28. Case A, Deaton A. Rising morbidity and mortality in midlife among white non-Hispanic Americans in the 21st century. Proc Natl Acad Sci U S A. 2015;112(49):15078-15083. doi:10.1073/pn as.1518393112
29. Abrams EM, Szefler SJ. COVID-19 and the impact of social determinants of health. Lancet Respir Med. 2020;8(7):659-661. doi:10.1016/S221 3-2600(20)30234-4