

Creative Methods in Psychotherapy: Developing Healthy Modes
How Creative Methods Can be Used to Develop a Healthy Adult Mode in Psychotherapy: A Case Study
Christina Löwenborg1
- Licensed psychotherapist, certified supervisor and trainer, Stockholm, Sweden Christina holds an MSc in social work and is trained in Child Oriented Family Therapy. She is also a recognized psychodrama guide and a mindfulness instructor.
Email: [email protected]
OPEN ACCESS
PUBLISHED: 31 August 2025
CITATION: Löwenborg, C., 2025. How Creative Methods Can be Used to Develop a Healthy Adult Mode in Psychotherapy: A Case Study. Medical Research Archives, [online] 13(8). https://doi.org/10.18103/mra.v13i8.6844
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI: https://doi.org/10.18103/mra.v13i8.6844
ISSN 2375-1924
ABSTRACT
The purpose of the case description is to describe a crucial element of a psychotherapeutic process, where patient and therapist work to enact the patient´s perceptions and experiences via tangible, visual and representative methodology, and to explain, in context, relevant starting points in taping, psychodrama and the mode concept in schema therapy.
The case study is built on qualitative design and comprises a presentation of a psychotherapeutic process, as well as a description of theoretical and methodical starting points in the methodology. The case study consists of a selection of material from a session in a psychotherapy process with a patient during the period 2022–24. The purpose is to describe an element of that process.
The outcome is presented in text and images on the basis of a described change process.
The principal conclusions in the case study demonstrate that the combination of taping, psychodramatic techniques and the mode model from schema therapy share several common denominators. The theoretical and methodical starting points can be combined and can contribute to identifying the following factors as significant parts of the therapeutic process described: visualization of vulnerabilities, identification of unsatisfied needs, mentalization, change in behavior and development of a healthy mode.
The case description is relevant given that the combined methodology is still an innovative area, and the case description has a contribution to make to development of the methodology within the area.
This article describes how tangible, visual and creative methodologies can be applied in psychotherapy. The method combines techniques from taping and psychodrama, and uses schema therapeutic points of origin.
Keywords: Schema therapy, taping and psychodrama.
1. Introduction
Psychotherapy, a treatment method in psychology, has been studied for over a century. Key milestones in research began with a 1924 assessment, followed by two influential articles—Rosenzweig (1936), who suggested different therapies yield similar outcomes, and Eysenck (1952), who controversially argued psychotherapy was no more effective than no treatment.
In the 1970s and especially the 1980s, research expanded, with studies by Smith, Glass, and Miller confirming psychotherapy’s effectiveness compared to placebo or no treatment. Psychotherapy research later divided into two main areas: effect research (evaluating outcomes) and process research (examining therapeutic mechanisms and interactions).
During the 1990s, randomized controlled trials (RCTs) gained prominence, especially in evaluating CBT due to its manualized approach. Later focus shifted toward understanding what makes therapy effective, not just whether it works—aligning with process research.
This article introduces a case study using creative, tangible, and visual methods in therapy, combining taping, psychodrama, and schema therapy. Central to this approach is the concept of head, heart, and hands-on:
- Head: Cognitive understanding
- Heart: Emotional experience
- Hands-on: Active engagement
The article continues with methodology, a review of the three therapeutic methods, and a detailed case study, ending with a discussion on integrating these creative methods in psychotherapy.
2. Purpose
The purpose of this case study is, from a user perspective, to describe a patient’s experience and perception of a methodology consisting of tangible, visual and representative methodology in psychotherapy.
The case study is built on a qualitative design and comprises a presentation of a psychotherapeutic process, as well as a description of theoretical and methodical starting points in the methodology. The case study consists of a selection of material from a psychotherapy process with a patient during the period 2022-2024.
The outcome is presented in text and images on the basis of a described change process.
The principal conclusions in the case study demonstrate that the combination of taping, psychodramatic techniques and the mode model from schema therapy share several common denominators. The theoretical and methodical starting points can be combined and can contribute to identifying the following factors a significant part of the therapeutic process described: visualization of vulnerabilities, identification of unsatisfied needs, mentalization, change in behavior and development of a healthy mode.
The purpose of the case description is to describe an element of a psychotherapeutic process, where patient and therapist work to enact the patient´s perceptions and experiences via tangible, visual and representative methodology, and to explain in context, relevant starting points in taping, psychodrama and the mode concept in schema-therapy.
The case description is relevant given that the combined methodology is still an innovative area, and the case description has a contribution to make to development of the methodology within the areas.
In part, the purpose of the article is, on the basis of case description, to describe some of the patient´s perceptions and experiences through/ enacting them with tangible, visual and representative methodology. The qualitative approach consists of describing the work process in text and images.
The second purpose is to describe the theoretical and methodological starting points applied in the psychotherapy process.
Based on database searches performed, the literature has been selected on the basis of its association with the field of taping, psychodrama and schema therapy.
A qualitative design was selected in order to achieve a deeper understanding of how the patient describes and perceives her own experiences. It centers on soft data, non-quantifiable data accessing the patient´s description and, through a case description, establishing a perspective viewed from the inside. The case study description aims to “perform a deep dive” and study subjective experiences.
The patient in the case description has been anonymized. In the presentation of the findings, fictive names and places have been used and personal expressions have been deleted. Anonymizing the patient makes it impossible to attribute the description to a specific individual.
Photography of set-ups via a mobile phone was used during the psychotherapy process in order to collect the empirical material.
In this article, the concepts of patient, narrator and protagonist are equated.
3. Taping
Taping is a visual and action-based method for storytelling and therapeutic conversation. It allows a narrator to represent their internal and external experiences using symbols and figures, thereby making abstract ideas tangible. Developed by Norwegian psychologist Martin Soltvedt, taping forms part of Child-Oriented Family Therapy and helps individuals express complex scenarios such as conflicts, visions, or life narratives.
The method transforms the interaction between therapist and patient into an active co-creation. This participatory approach allows the therapist to be more curious and challenging without appearing intrusive. A unique feature of taping is its capacity to represent both internal emotional states (“inside-out”) and external circumstances (“outside-in”) simultaneously.
Taping is often integrated with psychodramatic techniques and schema theory, particularly the concept of schema modes, making it a versatile tool for therapeutic work.
4. Schema Therapy
Schema Therapy, created by Jeffrey Young in the 1980s, emerged as a response to the limitations of traditional therapies when dealing with deep-rooted psychological problems. It is grounded in Cognitive Behavioral Therapy (CBT), attachment theory, and Gestalt therapy, and integrates emotional, cognitive, behavioral, and relational techniques.
At its core, schema therapy assumes that all humans are born with basic emotional needs—such as safety, autonomy, emotional validation, playfulness, and boundaries. When these needs are not met, individuals develop maladaptive patterns or schemas. These schemas arise from a combination of temperament and life experiences and manifest as dysfunctional thoughts, emotions, bodily reactions, and behaviors.
Common emotional wounds include:
- Abandonment due to lack of consistent attachment
- Emotional neglect resulting from insufficient empathy or guidance
Schema therapy categorizes modes (emotional states or coping responses) into four key groups:
- Vulnerable Child – Feelings like fear, anger, and shame.
- Internal Critic/Demanding Side – Harsh internal voices inherited from critical figures.
- Detached Protector – Avoidant behaviors that numb emotions, such as distraction or overeating.
- Healthy Adult – A compassionate and balanced mode that supports healing and autonomy.
The goal of schema therapy is to weaken dysfunctional schemas and empower the “Healthy Adult” to fulfill unmet emotional needs and lead a fulfilling life.
5. Psychodrama
Psychodrama is a therapeutic and developmental method founded by Jacob Moreno in the 1920s. It is widely used for personal therapy, crisis intervention, group supervision, and leadership development. The technique explores subjective truths through dramatization and structured creativity, bringing a person’s internal images and experiences to life on stage.
Key psychodramatic techniques include:
- Role Reversal – The patient (protagonist) switches roles with another character to gain empathy and new perspectives.
- Doubling – Another participant acts as the inner voice of the protagonist, expressing unspoken feelings or thoughts.
- Mirroring – The protagonist watches their own scene being acted out, providing distance and clarity.
- Concretization – Abstract concepts or physical symptoms (e.g., anxiety or a tree) are personified on stage to enable dialogue.
Psychodrama blends emotional release with cognitive insight. Change occurs not just through expression but through embodied learning and reflection. The method facilitates what is known as “action insight,” consisting of:
- A personally meaningful learning experience,
- Learning through doing, and
- Learning at a physical (bodily) level.
Following the dramatization, a sharing phase allows integration of emotional expression and cognitive understanding—blending “head and heart” to facilitate sustainable change.
6. The key concepts
Head, heart and hands-on are the key concepts that this action methodology comprises. The Head stands for the cognitive component that allows an outside-in perspective and intelligibility of the context. The Heart represents an inside-out perspective, an emotional experience of the situation that can contribute to understanding, while Hands-on corresponds to action in the situation in question, on the basis of intelligibility and understanding. Emotional learning is accorded a prioritized position as regards interactive processes that psychotherapeutic and psychosocial conversations with patients/clients entail and is termed the most effective component.
In taping, the stage is variable. The narration can move through and between past, present and future. It can depict parallel happenings, and it can present an external and an internal reality at one and the same time. Figures can be moved back and forwards. All this facilitates the generation of reflections and the exploration of thoughts and ideas.
The method involves the use of Playmobil® figures, and the ones available represent people of different ages, genders and ethnicities. As they have moving parts, it is possible to highlight their expressions and attitudes by, for example, turning their heads, arms and legs, thus clarifying the relationship between those involved. They can stand close to one another, or far apart. They can turn to face one another or to face away from each other, depending on what is being played out on the stage.
In conjunction with the Playmobil® figures, symbols are used to make the narrative more finely shaded and illustrative. These include tangled balls of cotton that can be placed between figures to illustrate entangled, conflicted relations. There is also a stone, which can be used to represent a weight – possibly a mood of grief or depression. A heart can be used to symbolize a warm relationship. A transparent cube can illustrate a feeling of isolation or exclusion. A telephone can symbolize that the parties are communicating, while a fence can be used to indicate the opposite. The symbols are selected by the narrator, who applies their subjective interpretation to them. In taping, the technique of externalization can be applied through concretizing the externalized problem. For example, a stone can be used to illustrate someone’s depression, thus separating the problem from the person so as to clarify that the person is not the depression. This also allows a dialogue between the person and the depression. Symbols for animals – such as a horse, dog, cat and bird – can be used to aid descriptions in the narrative. The figures need a delimited space – a stage where the action can take place. Tape and the fence symbol serve as external and internal boundaries in the narratives that take shape. An alter-ego figure functions as the narrator’s representation of himself/herself in a certain situation. Wild and tame animal figures are used to express feelings and forces that find expression between those involved. For example, a bull can express powerfulness, while a little rabbit can be used to represent trepidation. A tortoise can be used to indicate how a person withdraws into their shell for protection, while a snake can be used to depict unreliability. The narrator chooses the symbols that express the emotions that need to be represented on the stage. The narrative receives support and emotional charge from tangible symbols. The actual image narrative presents a perception of a reality and the picture created remains clear in the memory.
7. Taping with modes. A case study.
Taping can be used to help express a mode through the medium of symbols. When a mode is concretized with the assistance of a symbol, the act visualizes the dominant and overarching state or mind in which the patient finds him/herself at that moment in time. As the patient is also asked to stage how the other person is perceived, the exercise also reveals the patient’s perception of the other person’s mode. The table is thus the stage for the components that are perceived as strong influencers for the issue or the problem. The image presented now comprises information about the current status, which can then be examined and understood. The patient is given the opportunity to express emotions and cognitions on the basis of his/her current mode/status, and, if appropriate, to use symbols to try other modes and see how that might change the issue/the problem.
The following section presents a case study drawn from a psychotherapy process. The illustrations depict the different emotional statuses that emerge during the narration.
The case study described above illustrates how the concept of modes can be used in taping. Concretizing dysfunctional modes – negative voices – and discovering more positive modes – voices that can converse with the negative voice – can help change the internal emotions and the external dialogue.
Healing factors also encompass changes in behavior as the individual learns to replace dysfunctional coping styles with more functional ones.
Common mode constellations in taping are the vulnerable child and the demanding parent, the critical parent and the healthy adult and the vulnerable child and the detached protector.
Taping allows an opportunity to externalize modes, and externalization, in turn, supports mentalization.
Having or developing a healthy adult mode entails being integrated in thought, emotion and action, as well as moving towards mutual satisfaction of needs in relationships.
In the upcoming illustration, the case of Martha, taping is combined with psychodrama techniques and the modes concept in schema therapy. The illustration has been anonymized, names have been changed, and events have been modified to protect the parties involved.
The case description shows that the narrative and representation can take place in parallel during the therapeutic conversation.
Martha has sought therapy to learn how to express her feelings and needs, to be able to stand up for herself in relationships with others. She has a history of adapting to relationships, which has resulted in her suppressing her own needs and feelings.
At this point, she finds herself in a situation filled with strong emotions that overwhelm her. She cries as she begins recounting her story.

Martha is asked to demonstrate the situation that she wants the therapist to understand. Martha says that she was invited to a party, and felt excited and happy. The therapist asks Martha to show how she felt, using affect symbols. Martha chooses powerful female figures. On the table now is her alter-ego figure and her positive emotions.

During the evening, Martha makes a new acquaintance, Philip. They discover that they have a lot in common and Martha becomes attracted to Philip.
“Bring Philip up to the table stage,” says the therapist. It is important that the scene on the table matches the location of the narrative. If the representation stops and the narrative continues, the link between words and images ceases.
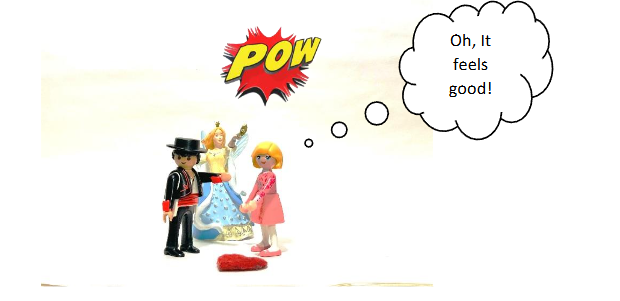
After a fun, intense and passionate evening and night together, contact stops. Martha doesn’t hear from Philip.
“He hasn’t been in touch!” says Martha.
“How does it feel for you?” asks the therapist. “Show me.”
The encouragement to “Show me” is an important instruction in taping work. The client is asked to both tell and show. The scene on the table between client and therapist needs to be consistent with the narrative. Otherwise, the image loses its relevance. The image reinforces and illuminates the core of the narrative. Emotions are captured and clarified.
Martha turns Philip’s figure so that he now stands with his back to Martha. Martha rearranges the stage. She removes the powerful, positive affect symbols, because they are no longer relevant. The scene has changed.
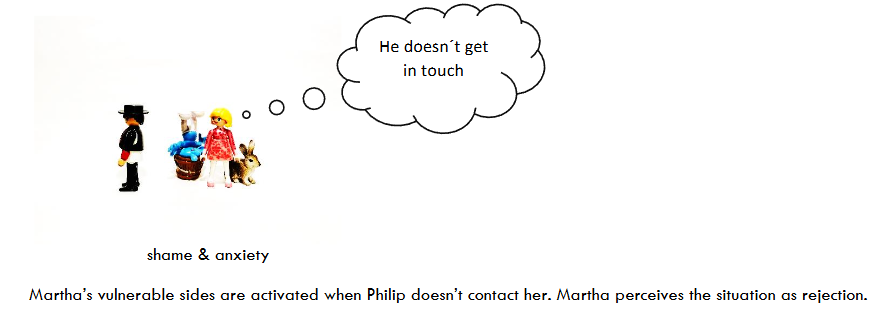
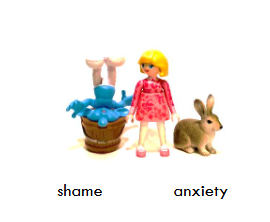
“I feel ashamed and worried,” says Martha, choosing symbols she thinks express those feelings. Martha places the affect symbols behind her alter-ego.
The mood has changed dramatically, from excitement and happiness to shame and anxiety.
Martha’s vulnerable sides are activated when Philip doesn’t contact her. Martha perceives the situation as rejection.
In this situation, Martha is asked to verbally express what is going on inside her.
“How does that side of you sound? Put a finger on the rabbit, which is the symbol of this anxiety.”
In taping, the affect symbols can be animated. Placing a finger on the emotion being symbolized concretely expresses the feeling in the present. By expressing the feeling in the present, the link between thought and feeling is strengthened.
“Philip is angry with me!” says Martha, while placing a figure of a roaring tiger behind Philip. Martha’s subjective view of how she sees the situation is now made visible.

Martha thinks and believes that Philip is angry with her. The therapist wants to explore what other emotions Martha may have, and suggests that she place her finger on the second symbol, which represents shame, and express what that side of her sounds like.
“Philip doesn’t think I’m good enough in his eyes. He doesn’t want to carry on being with me,” says Martha.
Martha places the figure of a scorpion behind Philip.
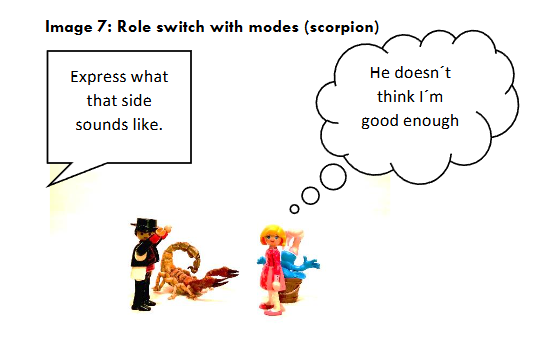
On the table now stands Philip, who Martha assumes is critical and rejecting, and herself – ashamed, self-accusing, and worried that Philip does not want to see her again. Martha’s subjective inner world, her inner working hypothesis, is now made visible on the table.
How has it come to be that Martha’s inner world looks like this? Philip has not expressed any criticism to Martha. The statements are based on a very limited time together. And Martha has not tried to contact Philip either.
This raises the question: What was Martha’s relationship with David like? The therapist asks Martha whether they should explore together how past experiences may be affecting the situation Martha finds herself in. Martha thinks that would be helpful.
“Would you like to show me what your previous relationship with David was like?” says the therapist.
Martha changes the scene. She puts a figure representing David on the table and places a powerful affect symbol – a gorilla – behind him.
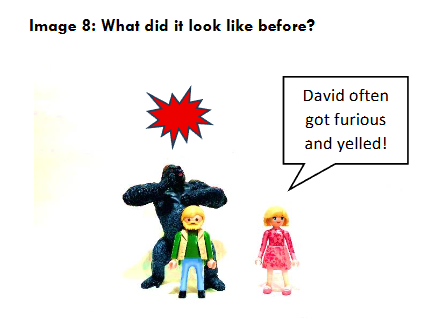
“David often got furious and yelled at me. He might get annoyed with a colleague at work who he didn’t think was doing enough, but then he would direct his anger at me when he got home,” says Martha.
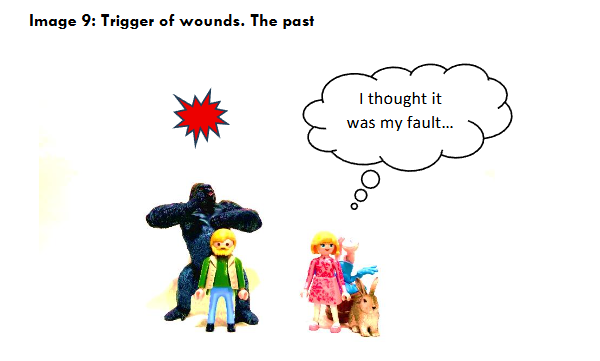
“What happened to you then? What was going on inside you?” asks the therapist.
“I thought it was my fault, that I wasn’t doing well enough or being good enough. I thought if I adapted or improved, it would calm David down,” says Martha, placing her finger on the symbol of vulnerability – the rabbit.
Martha says that she often felt judged in her relationship with David – about what she looked like or what she did. Martha often worried that her actions and choices would be questioned and criticized by David.
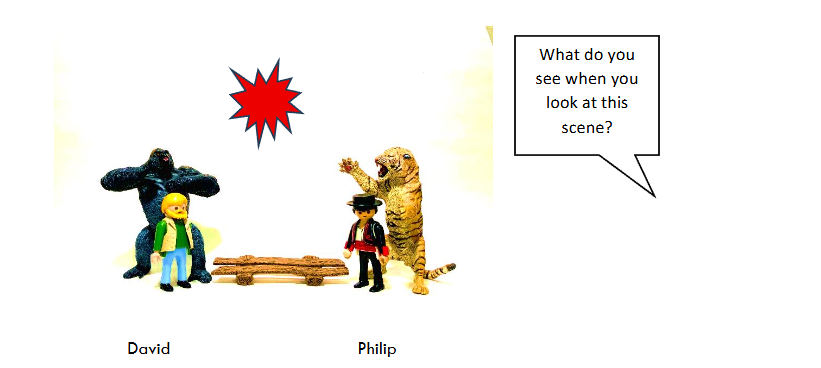
On the table there is now a figure representing David, who is irritated and critical, and another figure representing Philip, who is angry and critical.
“What do you see when you look at this scene?” asks the therapist.
“Oh my goodness!” exclaims Martha. She leans back and looks exhausted.
The therapist asks for permission to enter Martha’s scene and change the positions of the characters, creating an affect bridge between the past and the present, i.e. between David and Philip.
Now there is an affect bridge – between David’s anger and critical temperament and Philip’s supposed anger and critical temperament on one side, and Martha’s vulnerabilities in the form of fear and shame on the other.
After studying the change made to the scene, Martha says: “Yes, this is exactly what it’s like. It can be so hard.”
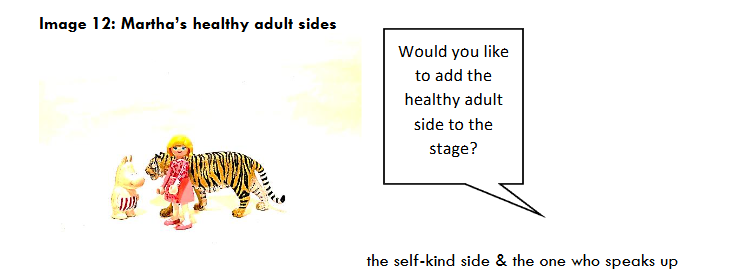
“Would you like to add the healthy adult side to the stage?” asks the therapist.
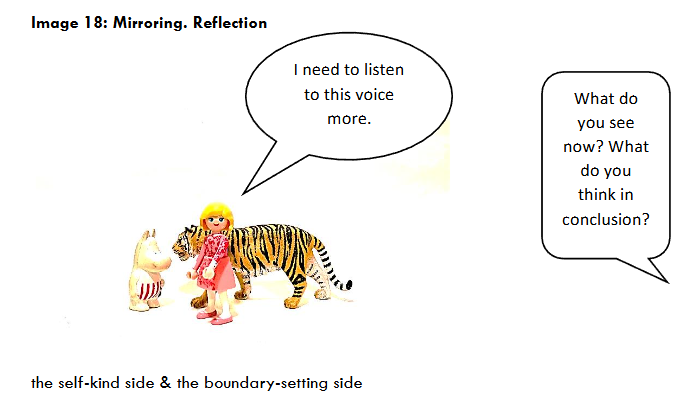
Martha picks up a symbol she calls “self-kind” and another for “the person who speaks up”. For the self-kind side, she chooses a symbol representing a mother, and for the boundary-setting side of herself, Martha chooses a powerful wild animal, a tiger.

What do you see when you look at this scene?
“Would you like to add the healthy adult side to the stage?”
The therapist asks Martha to place her finger on one of her symbols. “What does the healthy adult side tell you?”
Martha places her finger on the self-kind side, turns it towards her alter-ego figure and says out loud: “This anxiety you feel is an old ghost from your previous relationship, when you felt constantly judged and questioned.”
“It’s not that surprising that the pattern we develop repeats itself in a new relationship,” adds the therapist. Martha looks pleased.
“Is there something you need to say to David?”
Martha places her finger on the boundary-setting side, the tiger, and says: “You should know that from now on I will set a limit for you, David. I don’t think you have any right to judge me, how I look or what I do.”
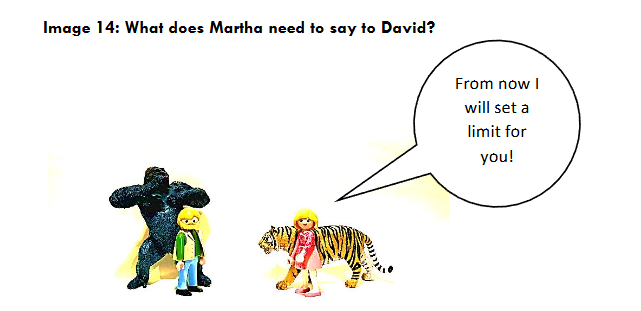
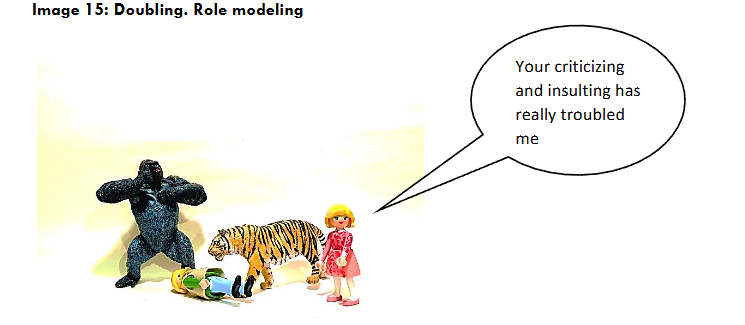
The therapist asks if she can come in and double Martha’s boundary-setting side, which she is keen to do. Doubling means that the therapist acts on behalf of the client. It requires prior permission from the client and verification afterwards. The purpose of doubling is to add important information for the client, or to express something that the client needs to express but has difficulty expressing.
The therapist puts her finger on the tiger and says, “This has caused me a lot of trouble.”
Martha is asked to repeat what is correct in her own words. The doubling needs to be verified or adjusted, so that the statement is consistent with the client’s perception.
“What you have done, criticizing and insulting me, has really troubled me. My self-esteem has taken a real hit,” Martha says firmly, pushing over David’s alter-ego figure.
“How does that feel?” asks the therapist.
“It feels very good!” Martha replies.
“Would you like to update the stage, so that it matches how it feels now?” asks the therapist, looking at Martha.
It is vital that the stage is continuously updated as the narrative progresses and changes.
“I understand why I feel useless and bad, and why I worry about what the other person will think of me. I see that my negative experiences have affected me in a way that has hurt me,” says Martha, putting up a fence between the vulnerable sides and the healthy adult sides.
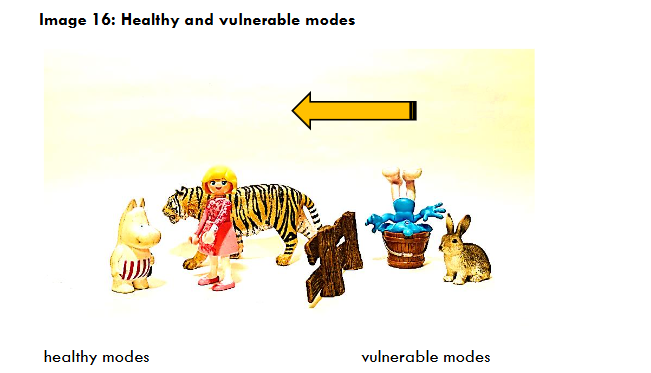
“Now I can see you standing together with your healthy adult sides, which symbolize self-care in different ways. Does the healthy side want to tell you anything else?” asks the therapist.
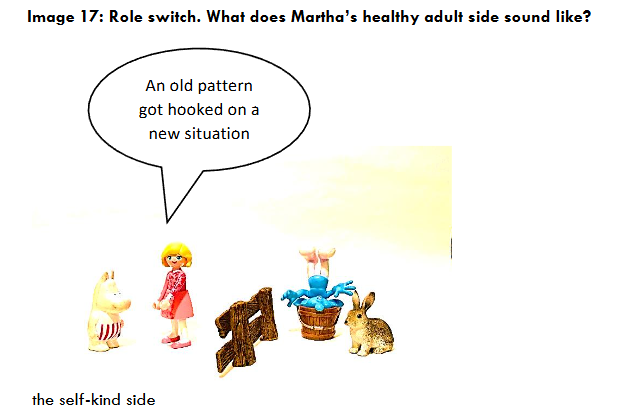
Martha puts her finger on the side she calls “self-kind” and says:
“What happened to you after Philip didn’t get in touch was an old pattern from the past that got hooked on a new situation. You have no idea why Philip hasn’t been in touch. You could just call him.”
When Martha is not as affected by shame and fear, she can access more resources within herself. She is in touch with a healthy sense of self-worth and can consider contacting Philip herself.
An old pattern got hooked on a new situation
“What do you see now? What do you think in conclusion?” the therapist asks.
Martha has identified important strategies for her life, and to remind herself of them, the therapist suggests that she take photos of them with her cell phone.
“Would you like to take a photo of the healthy adult sides, i.e. self-care and self-assertion, so you can remind yourself of that voice when you need to hear it?”
Martha gets out her cell phone and takes a photo of the scene.
“I’ll bring that picture up and look at it when I need to,” says Martha.
The image is emotionally charged, and research shows that we remember better with images – known by researchers as the superiority effect.
In this case description, affect theory is combined with schema therapeutic modes, psychodramatic techniques and taping methodology. During the session, Martha switches roles with her inner sides on the taping stage – at times the vulnerable side (fear and shame) and at times the healthy adult side (self-care and self-assertion).
There are several aspects of the healthy adult mode, including being able to raise yourself up and get an overview of your situation (a metaperspective). Another aspect revolves around maintaining inner emotional contact, i.e. being with yourself and your feelings. A further aspect is taking care of yourself and wishing yourself well. A final important aspect is taking responsibility for your actions and standing up for yourself.
During the therapy session, Martha sees how patterns from the past are making it difficult for her in the present. Martha’s attention to her healthy adult sides is strengthened. Finally, Martha takes a photo of the scene of her healthy adult sides to remind her of them.
Schema therapy, which has provided an important basis for the treatment, has to do with understanding the vulnerability, focusing on the vulnerable side so as to decrease the vulnerability and increase the healthy, adult side of the person.
Having or developing a healthy adult mode entails being integrated in thought, emotion and action, as well as moving towards mutual satisfaction of needs in important relationships to others. Playfulness and spontaneity having the opportunity to explore, to be curious and to tread new paths – as being one of our fundamental core needs. This core need has to be covered in relationships with others so as to allow healthy development and maturity to occur.
8. Discussion
In the concept head, heart and hands-on, emphasis is placed on the specific and unique aspects of the methods taping, psychodrama and schema model, and on how the methods integrate the functions of cognitive analysis with the immediate emotional experience and active participation. Briefly put: head, heart and hands-on become one. There are many similarities between taping and psychodrama, but there are several differences as well. The fact that both methods integrate head, heart and hands-on, and that they are tangible, visual and creative methods, has made it possible to use the methods alternately in psychotherapy sessions and to exploit their respective potentials. Both feature strong elements of non-verbal communication, which is an asset when the exploration of the problem is sensitive in nature, and when the exploration itself risks becoming over-intellectualizing.
The mode concept from schema theory is a usable model in combination with taping and psychodrama, and which brings sharpness and distinction to the work method with its clean-cut forms of dominant states of mind in the moment. In the methods of taping and psychodrama, the actor in the narrative act; speaks and express emotions. In taping, the drama takes place on a table-top stage using acting figures, while in psychodrama, the protagonist – physically acts together with their co-actors directly on the stage itself. In addition to the setting of a stage, taping and psychodrama share a number of significant component parts. Both have a leading figure – a narrator/ protagonist – who tells a story. There is a conversation guide, or a “director”, who helps drive the narrative forward. In both cases, the relationship between the narrator/the protagonist and the conversation guide (the director) becomes more co-creative, which allows the player to become more challenging and wondering, without becoming more directly inquisitive.
The schema therapeutic perspective encompasses emotional, cognitive, behavioral and relation-related interventions, which makes the theory suitable for integration with taping and psychodrama. Schema healing factors include changes in behavior as the individual learns to replace dysfunctional coping styles with more functional ones. When a wound (a schema) heals, it is no longer triggered as readily as it was before. The concept of modes opens the door to internal dialogue between different sides of the person. Having or developing a healthy adult mode entails not only the integration of thoughts, emotions and actions, but also a mutual satisfaction of needs in relations with others.
There is much to be gained by combining the methods. Role reversal is to be found in both taping and psychodrama. Role reversal is a technique whereby the narrator/the protagonist swaps roles with another actor in the drama, and it is one of the principal techniques for reinforcing mentalization capacity. Role reversal makes it possible to view the world from the other person’s perspective. The same technique is to be found in taping, when the narrator places their finger on another person’s figure and answers their alter-ego. Roll reversal, which boosts mentalization capacity, has to do with looking at oneself from the outside, and understanding the other person from the inside. Mentalization capacity is supported in taping through the narrator animating their figures by moving them around the stage and speaking, thus taking on the perspectives, thoughts, emotions and needs of another person. Role reversal is also found in methodologies stemming from the schema model, with starting points drawn from gestalt therapy. Switching from taping to psychodrama in role exchange reinforces the narrator’s/protagonist’s experiences and actions even further.
Concretization is to be found in both taping and psychodrama. Both methods can concretize the external as well as the internal representation within the narrator/protagonist, both separately and simultaneously. Taping allows inner images to be concretized – for example, the feeling that the person encompasses both a large, capable persona and a small, frightened one, which can be represented through the use of two different figures/animals/symbols. In psychodrama, an auxiliary ego can be cast as the large, capable persona, while another auxiliary takes on the role of the small, frightened one. In both cases, concretization allows the narrator/protagonist to engage in internal dialogue. The concept of modes, which covers a variety of states of mind in which the individual may find himself/herself, is one way to conceptualize and concretize the different sides the individual displays in a given situation.
Externalization is also to be found in both taping and psychodrama, and the concept of modes, in and of itself, is one way to externalize different sides of oneself and of others who are active in the situation. Externalization is a concept that is closely aligned with concretization. The technique is intended to separate the problem from the person so as to clarify that the person has a relationship to the problem—but is not the problem itself. Externalization of “partial selves” occurs when the narrator chooses different figures as representations of him/herself, which clarifies how the narrator views their internal world, and those of others. When externalization takes place in psychodrama, the role of “partial self” is played by an auxiliary ego. The concept of modes in the schema model corresponds to the “partial selves” concept in psychodrama.
Doubling is a psychodramatic technique that it is beneficial to use in taping. In psychodrama, the group members have the opportunity to assist the protagonist in expressing messages and emotions that their finds difficult to bring out, by physically stepping onto the stage and expressing their emotions through the protagonist. In taping, in psychotherapy, the therapist can double the narrator during the reflection phase by placing their finger on the clients alter-ego figure and suggesting messages. In the same way as in psychodrama, the protagonist always has the option of declining the suggestions put forward. Doubling can take place through the narrator’s alter-ego figure, and through externalized modes.
Mirroring is a technique that appears in both psychodrama and taping but takes different forms in the two methods. In psychodrama, the protagonist steps off the stage while an auxiliary ego takes on the role of protagonist. The intention is for the protagonist to take advantage of the distance to gain a better overview of the happening and thus to come up with thoughts and ideas about what their should do in the situation. In taping, an overview is always available through the physical distance between the narrator and the figures on the stage. The conversation guide can switch between the narration playing out on the stage, and reflections derived from the overview that the scene provides. In the case study, mirroring is used to allow the patient to gain distance from the situation, and to think about what needs to be done. There are also similarities in how the process is concluded in taping and psychodrama. In taping, the activity is concluded by looking up from the scene playing out on the tabletop and reflecting on what has happened; how the narrative that has played out becomes useful to the narrator. It is in the conclusion phase that links are established between what happened on the stage and reality. What was created on the stage need, in one way or another, be applied in reality. Following the dramatization, a sharing phase allows integration of emotional expression and cognitive understanding. The miniature format of taping makes it possible to establish multiple stages at the same time; this creates structure and a broad overview of the happening. Presence in multiple settings can be built up simultaneously; different perspectives on one and the same issue can be illustrated in this smaller format, while the large format of psychodrama does not present the same opportunities. The taping stage can be used to visualize a helicopter perspective and keep the complexity alive. Both methods are action methods and encourage people to express themselves in action. The actors – regardless of whether they are representative figures or actual people on a stage – can look at one another, look away, raise and lower their voices; the dialogue plays out in front of everyone’s eyes. In the same way, different modes can enter into dialogue with each other. The methods can move through different time perspectives: past, present and future. When characters address one another, they do so in the present tense; this augments both the sense of reality and the emotional temperature. In both methods, new dialogues can be tested between the characters. If the narrator/protagonist needs to find other ways to act, their can experiment with bringing new approaches to old situations. The originators of taping, psychodrama and schema therapy all emphasize the importance of play and creativity in the therapeutic work. Martin Soltvedt describes his desire to turn the conventional relationship between play and conversation upside down, with the purpose of tapping more strongly into the desire to play in the adult person in the change process.
9. Conclusion
This case study demonstrates the therapeutic potential of integrating creative, visual, and action-oriented methods—taping, psychodrama, and schema therapy—to facilitate the development of a healthy adult mode. Through the case of Martha, it becomes clear that such a combined approach allows patients to externalize and explore complex inner experiences in a tangible and emotionally safe format. By visualizing internal states, embodying roles, and dialoguing with different sides of the self, patients can access deeper emotional insights and enact meaningful behavioral change.
One of the most powerful aspects of this methodology is its capacity to make abstract inner processes visible and concrete. When emotional pain, cognitive distortions, and unmet needs are expressed through figures, symbols, and dramatic techniques, the therapeutic process becomes not only more engaging but also more accessible for the patient. The methods used support metacognition, strengthen mentalization, and foster an integration of thought, feeling, and action—hallmarks of the healthy adult mode.
This integrated approach taps into core human needs: the need for connection, understanding, expression, spontaneity, and play. It empowers patients to recognize and revise dysfunctional patterns rooted in past experiences, enabling them to respond more adaptively in the present. Martha’s journey illustrates how the activation of earlier schemas can be transformed through the embodied experience of her healthy adult self—an inner voice that is kind, assertive, and protective.
While further research is needed to assess the broader applicability of these methods, this case suggests that combining schema therapy with taping and psychodrama offers a promising path for fostering emotional healing and personal growth. By engaging the head, heart, and hands-on in a unified process, therapists can co-create therapeutic spaces where patients feel both safe and empowered to reconstruct their inner worlds—and, ultimately, to live fuller and more authentic lives.
References
- Ainsworth MDS, Bowlby J. An ethological approach to personality development. Am Psychol. 1991.
- Bieling PJ, McCabe RE, Antony MM. Kognitiv beteendeterapi grupp. Stockholm: Liber; 2008.
- Boterhoven De Haan KL. Therapists’ thoughts on therapy: Clinicians’ perception of the therapy processes that distinguish schema, cognitive behavioural and psychodynamic approaches [thesis]. Murdoch, Australia: Murdoch University; 2014.
- Bowlby J. A secure base: Parent-child attachment and healthy human development. New York: Basic Books; 1988.
- Burlingame GM, MacKenzie RK, Strauss B. Small-group treatment: Evidence for effectiveness and mechanisms of change. In: Lambert MJ, ed. Bergin and Garfield’s Handbook of Psychotherapy and Behavior Change. Oxford: Oxford Press; 2004.
- Cullberg Weston M. En dörr till ditt inre. Visualisering i terapi. Hungary: Studentlitteratur; 2010.
- de Poy E, Gitlin LN. Introduction to Research: Understanding and Applying Multiple Strategies. St. Louis, MO: Mosby; 1999.
- Eysenck HJ. The effects of psychotherapy: An evaluation. J Consult Psychol. 1952;16(5):319–324. doi:10.1037/h006363
- Fitzsimmons K, Gallagher S, Blayone S, Chan B, Leaitch W, Veals N, Wilkinson N. The Young Schema Questionnaire in Group Therapy: A Client-Focused Approach. London: Routledge; 2009.
- Gyllenhammar C, Perris P. En klinikers handbok & en terapiberättelse. Stockholm: Natur & Kultur; 2016.
- Josefsson D, Linge E. Hemligheten. Från ögonkast till varaktig relation. Finland: Natur & Kultur; 2008.
- Lockwood G, Perris P. A new look at core emotional needs. In: Vreeswijk M, Broersen J, Nadort M, eds. The Wiley-Blackwell Handbook of Schema Therapy: Research and Practice. Chichester: John Wiley & Sons, Ltd; 2012.
- Lockwood G. International Society of Schematherapy; 2008.
- Löwenborg C. Värdefulla tankegångar från Kanadas urinvånare. Socionomen. 2000;(2).
- Löwenborg C. Reflekterande processer. Socionomen. 2001;(8).
- Löwenborg C. Inspiration across cultures: reflecting teams among the métis in Canada. Aust N Z J Fam Ther. 2001;22(1).
- Löwenborg C, Nilsson L. Vad är verksamt i handledning – en kvalitativ undersökning. Sundbyberg: Bomastryck; 2002. FoU-rapport 2002:2. ISBN: 91-89681-00-0.
- Löwenborg C, Nilsson L. Vitryska utsiktsplatser. Sundbyberg: Alfaprint; 2005. ISBN: 91-631-7596-7.
- Löwenborg C, Kamsvåg K. Med andra ögon – brukarens syn på familjebehandling. Forskningsrapport 2006:1.
- Löwenborg C. Psykodrama i annat ljus – förändringens fyra rum. Stockholm: Stockholms institut för psykodrama, sociometri och gruppsykoterapi; 2008.
- Löwenborg C, Sjöblom Y. Föräldrars och ungdomars erfarenheter av familjebehandling inom socialtjänsten. Socialvetenskaplig tidskrift. 2009;1.
- Löwenborg C. Huvud, hjärta och handling – Om konkreta, visuella och gestaltande metoder i handledning. 2013, 2016, 2017.
- Löwenborg C. Head, heart and hands on – Concerning, concrete, visual and creative methods in supervision. Glob J Hum Soc Sci A. 2019;19(13):1.0.
- Nilsson J. Tejping och trauma. Lithuania: JNPK; 2027.
- Pakzad F. Emotionell inlärning som en väg till ny kunskap i handledning. Psykoterapi. 2019;1. Laholm: Trydells tryckeri AB.
- Perls FS. Det gestaltterapeutiska arbetssättet; Ögonvittne till psykoterapi. Stockholm: Wahlström & Widstrand; 1977.
- Philips B, Holmqvist R. Vad är verksamt i psykoterapi? Stockholm: Liber; 2008.
- Rosenzweig S. Some implicit common factors in diverse methods of psychotherapy: Am J Orthopsychiatry. 1936;6.
- Rydén G, Wallroth P. Mentalisering. Att leka med verkligheten. Finland: Natur & Kultur; 2008.
- Smith ML, Glass GV, Miller TI. The Benefits of Psychotherapy. Baltimore: Johns Hopkins University Press; 1980.
- Soltvedt M. BOF – Barnorienterad familjeterapi. Falun: Mareld; 2005.
- Tschacher W, Zorn P, Ramseyer P. Change Mechanisms of Schema-Centered Group Psychotherapy with Personality Disorder Patients. Rome: Catholic University of Sacred Heart; 2012.
- van Wreeswijk M, Broersen J, Nadort M. Handbook of Schema Therapy: Theory, Research and Practice. Chichester: Wiley Blackwell; 2012.
- Yalom ID. The Theory and Practice of Group Psychotherapy. New York: Basic Books; 2005.
- Young J, Klosko J, Weishaar M. Schema Therapy: A Practitioner’s Guide. New York: Guilford Publications; 2003.
- Young J, Klosko J. Lev som du vill och inte som du lärt dig. Reinventing your life. Stockholm: Natur och Kultur; 2010.