





Cultural Competence in Nursing: Ray’s Caring Dynamics
Cultural Competence: Ray’s Theory of Transcultural Caring Dynamics in Nursing and Health Care to Guide Reflective Analysis for Self-Awareness
OPEN ACCESS
PUBLISHED: 31 May 2026
CITATION: Martin, M.B., Ray, M.A., 2026. Cultural Competence: Ray’s Theory of Transcultural Caring Dynamics in Nursing and Health Care to Guide Reflective Analysis for Self-Awareness. Medical Research Archives, [online] 14(5). https://doi.org/10.18103/mra.v14i5.7387
DOI https://doi.org/10.18103/mra.v14i5.7387
ISSN 2375-1924
ABSTRACT
Introduction: The aim of this article is to present the theoretical model with a description of Ray’s Theory of Transcultural Caring Dynamics in Nursing and Health Care with supporting transcultural nursing phenomena and global health care data.
Methods: The theory was developed from knowledge of nursing, transcultural nursing, complexity science, and cultural anthropology.
Results: The theory and model are significant resources to address contemporary issues of culture, human-environment integrality, cultural diversity, migration patterns in the global community, minority health, the social determinants of health, and the need for increasing cultural awareness, communitarian ethics, reflective analysis, and competency of health care professionals in the delivery of competent cultural health care for improved health, healing, and a peaceful death. The paper points out that the central emphasis of the theory and model, essence of caring, transcultural ethics, transcultural context, and universal sources (spirituality) highlight the opportunity for transcultural awareness, seeking understanding and cultural choice. This multidimensional aspect of the model illuminates both patient’s/family’s and provider’s cultures and values, and the environment, and acknowledges the criticality through reflection of the cultural impact on mutual choices for health care outcomes and quality of life.
Conclusion: This theory and contemporary knowledge about the changing world community, migration patterns, social determinants of health (SDOH), transcultural caring science and its dynamics provide opportunities for nurses and physicians to enact effective transcultural health care aligned with the unique cultural needs of each patient and their family.
Keywords: transcultural caring dynamics, communitarian ethics, organizations, spirituality, migration, cultural awareness, reflective analysis, transcultural inter-professional competency.
INTRODUCTION
Anthropologist and nurse researcher Madeline Leininger, foretold that by 2015 healthcare systems should be transculturally based to meet the care needs of diverse global populations. Transcultural health care thus refers to the “ability of health care systems to provide care to patients from diverse cultural backgrounds in a manner that respects and accommodates their unique values, beliefs, and practices.” As of the numbers of health care workers globally included 29.1 million nurses, 12.7 million medical doctors, 3.7 million pharmacists, 2.5 million dentists, 2.2 million midwives, 14.9 million additional occupations, totaling 65.1 million health care workers, plus 3 million social workers, each faced with the challenges and rewards of globalization in practice. The time is now for healthcare workers to gain knowledge, skills, and attitudes that best prepare them to practice in a patient centered culturally informed manner. Ongoing socio-political conflicts, human rights violations, social injustice, poverty, food insecurity, drug abuse, and violence complicate the needs of patients. Providers will benefit by guidance from a dynamic framework which illuminates significant cultural influences of patients with a central focus on choice.
The purpose of this paper is to present factors influencing the need for cultural competency, introduce transcultural nursing and Ray’s Theory of Transcultural Caring Dynamics in Nursing and Health Care and describe the value of reflective analysis for self-awareness of providers guided by Ray’s theory, highlighting individual patient’s cultural needs.
FACTORS INFLUENCING THE NEED FOR CULTURAL COMPETENCY
Health care providers across the world must be vigilant about the increasing migration of populations, minority health, health disparities, and the need for culturally congruent care in practice; these matters have relevance both locally and globally.
MIGRATION
For centuries migrating people have sought opportunities for better quality of life internationally. Migration is a significant influence in global development. Nations must contend with and understand political conflicts, terrorism, religious extremism, poverty, and disease, while addressing humanitarian needs through understanding and peaceful solutions. In the year 2020, 281 million people (less than 4% of the world’s population) worldwide were immigrants compared to approximately 154 million in 1990. Europe has the largest number of migrants at 87 million, Asia has 85.6 million, North America has 59 million, Africa has 25.4 million. This trend of increasing migration conveys the need for healthcare providers globally to optimize their ability to care for diverse populations within practice.
MINORITY HEALTH
Increasing migration results in minority groups within destination countries. Minority health denotes unique health traits of racial/ethnic groups, commonly underserved due to racism and discrimination; intentional research is needed about minority populations to optimize health care outcomes. Minority health research is the empirical inquiry of factors including behavioral, biological, environmental, and societal, that impact the health of racial/ethnic minorities with the goal of optimal health outcomes and disease prevention. In Europe stakeholders from academia, the health care community, and NGOs have voiced a call for action about health inequalities; there is a need for improved data collection and analyses and collaborative research to achieve understanding and political will on the subject.
HEALTH INEQUITY AND HEALTH DISPARITY
In 2008 the World Health Organization (WHO) Commission on Social Determinants of Health (SDOH) published data about sources of global health inequities that called attention to the SDOH which include economics, education, environment, and social and political systems. Pacquiao et al. attest that SDOH may impact up to half of health outcomes and that health disparities are the differences in health outcomes of populations related to these societal disadvantages which are best addressed at systems’ levels. The WHO published the Operational Framework for Monitoring Social Determinants of Health Equity in 2024 to guide national governments to track SDOH, take needed action, and use data to effect policy that supports health equity. Longstanding and present social environments, prejudice, and bias also impact differences in care by influencing discriminatory behaviors among providers. Healthcare providers across the world are well positioned to advocate for equity in healthcare and patient rights, whether institutionally (i.e., hospital patient bill of rights), nationally (i.e. civil rights), or globally (i.e. human rights), as cited in the UN Universal Declaration of Human Rights that member states are expected to follow.
NEED FOR CULTURALLY CONGRUENT CARE
Migration, minority health, health inequity and health disparity elucidate the need for culturally congruent care, not only for optimal patient care outcomes, but also to promote patient satisfaction. The impact of SDOH on health outcomes calls for inclusivity and support for environments that support diversity, equity (fairness), and social justice (equal economic, political, and social rights). Transcultural caring competence (accountability and responsibility) requires cultural knowledge and skill and comprehension of the complexity of human relationships and the influence of the environmental context. Fortunately, academic educators for physicians and nurses are increasingly supporting SDOH education in curricula. Transculturally astute healthcare providers are compelled to access resources about SDOH in practice and professional settings, as well as credentialing bodies. The WHO generates annual reports of sustainable development goal progress with country specific information. These data include valuable population health information that inform practice. Culturally congruent care requires healthcare provides to have knowledge of the ethnicity, caring and curing practices, educational levels, and communication norms of often encountered cultural groups. Knowledge of culturally congruent care may be gained from ethnographic research and taking time to inquire what matters most to patients to foster understanding. Cultural influences of health, wellbeing, death and dying are complex; “respect for persons, cultivating humanity through a commitment to peace, power, justice, and caring are uncompromising.” Science, now complexity science conveys the interconnectedness of all things (human-environment integrality), choice-making within networks of relationships, and transcultural caring dynamics. These phenomena are enunciated within the concept of culture and recognized differently in culture theories and international organizations, thus highlighting what is necessary for student learning now and in the future.
TRANSCULTURAL NURSING AND RAY’S THEORY OF TRANSCULTURAL CARING DYNAMICS IN NURSING AND HEALTHCARE
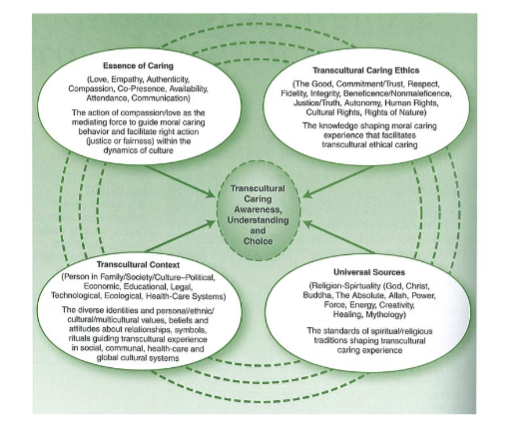
Ray’s transcultural caring dynamics in nursing health care model serves as a framework to determine culturally based patient care in light of its five components: essence of caring, transcultural caring ethics, transcultural context, and universal sources, with the central theme of transcultural caring awareness, understanding, and choice. Transcultural caring is central to this model and is described as the connections between being generous and engaging in appropriate actions; between love as empathy for another’s suffering; and fairness within the cultural issues in nursing, organizations, and society. Ray purports that culture is dynamic and complex, has different meanings, and that influences on health are multi-dimensional and interconnected between nursing, person, and culture with a central premise of transcultural caring awareness, understanding, and choice.
ESSENCE OF CARING
Ray originally presented the concept of caring, inclusive of co-presence and love, as a knowledge base for nursing responsibilities expressed as transcultural caring. Aspects of this component of the theory include love, empathy, authenticity, compassion, co-presence, availability, and communication with compassion, all needed to guide caring behavior and to uphold justice and fairness within cultural dynamics. Ray views caring as a moral imperative, a complex human characteristic, that is communicative and contextual with the environment, organizations, and the universe. The legacy of caring within nursing is acknowledged by Ray, validating respect for nursing’s past, contemporary advancements, and futuristic concerns. The image of the framework provides a visual means to appreciate the classifications of caring and interconnectedness of factors within the practice of spiritual-ethical caring which comprises compassion and love, genuine presence and availability to the patient, and enacting justice.
The essence of caring component of Ray’s theory interconnectedness among all theoretical components and underscores observance of ethical standards (transcultural caring ethics), religious and spiritual influences, (universal sources), and the contextual implications (transcultural context) of the human-environment relationship. For example, caring is a cultural resource that is incorporated by all cultures and all religions to facilitate the improvement of health and well-being of diverse individuals, families, communities, and complex systems. From a human-environmental point of view, in a study published in 2026. Ray’s theory of bureaucratic caring was used as underpinning the analysis of health outcomes, especially respiratory and dermatological health regarding exposure to harmful Algal in the marine environment. Ray attests that the central emphasis of the theory requires being aware of the multidimensional aspect of both patient’s and provider’s cultures, acknowledging the cultural impact on health, and providing choices in care aligned with cultural values and environmental concerns. These behaviors provide opportunities for nurses to enact effective transcultural nursing care aligned with the unique cultural needs of each patient.
TRANSCULTURAL CARING ETHICS
Transcultural caring ethics refers to the knowledge that informs the provision of care from an ethical perspective. Dimensions of transcultural caring ethics comprise “the good, commitment/trust, respect, fidelity, integrity, beneficence/non-maleficence, justice/truth, autonomy, human rights, cultural rights, and rights of nature.” Transcultural caring ethics require respect for individual human rights, cultural rights, and cultural needs, and validates respect for individual differences. Cultural beliefs and behaviors are directed by values. Ethical principles including autonomy, beneficence, non-maleficence, and justice, are influenced by cultural values. Ray described ethics as a “code of conduct developed and reinforced in terms of what is good and right (or moral) in character and behavior.” Ray’s model considers the dynamics facing health care professionals today and provides a structure within which caring may take place. The rapid changes in health care, technology, and socio-political dynamics taking place in the world today necessitate thoughtful decision making about ethical questions related to doing no harm. Today, the position of Artificial Intelligence (AI) and its potential negative effect on all cultures is so concerning to the point that the “godfather” of AI and Nobel Laureate, Dr. Geoffrey Hinton states that technologists must embrace “maternal” characteristics, such as empathy, compassion, patience, and attentiveness in the process of creating and promulgating the science/technology of AI, especially as it relates to what it means to be human. Also, for example, ethical principles may be considered at a culture specific level; for example, as in the religion of Islam, or at an institutional level, or as in the work of an ethics committee. Awareness among nurses and patients of how ethical principles are related to cultural values allows for engagement in meaningful mutual decision making. The many levels wherein professional ethics, cultural rights, and justice are considered, rethought, and reinterpreted call for what Ray described as communitarian ethics, or reasonable discourse, with the goal of gaining mutual understanding. Ray’s theoretical framework highlights the importance of an ethical imperative for the care of patients that is aligned with their cultural backgrounds.
TRANSCULTURAL CONTEXT
Ray describes transcultural context as the interrelationships between the person and environment, person and nature, person and society, and person and spirituality. As previously stated, this description validates the connections to humans to dynamic communication, automation, and technology present in the global environment. This “mutual human-environment process” supports the use of reflection to comprehend the individual, family, their community, and the world. Transcultural context considers the person within several systems: familial, cultural, political, economic, educational, legal, technological, ecological and health care.
In transcultural nursing what is familiar, physically, mentally, and emotionally extends beyond the familiar; Ray emphasized in her theory that transcultural caring in nursing necessitates examining universal socio-political effects on cultural identity, ethnicity, and multiculturalism. The understanding of complex cultural systems and influences, such as any religion for example, is attainable using this theory, which meticulously contemplates culture-specific dynamics at every level of society: globally, nationally, and locally. The inter-relational nature of Ray’s theory to both person-to-person dynamics as well as to conceptual dynamics is emphasized in this model. For example, a non-Sikh nurse may encounter a Sikh patient who faced discrimination in their country of origin, as well as in United States or Canada, who may be at risk for further offenses in the healthcare environment. The concept of transcultural context considers all characteristics of the human-environment relationship including the healthcare setting. Structures and processes within healthcare institutions, including its workforce and leadership, are influences by the prevalent sociocultural context that impacts how cultural groups are understood. While nurses, as care providers may be affected by socio-political occurrences personally, professionally they are expected objectively to meet diverse patient care needs through self-reflection and cultural knowledge.
UNIVERSAL SOURCES
Dimensions of the universal sources include spiritual/religious beliefs of individuals and groups in reference to God, Christ, Buddha, The Absolute, Allah, Power, Force, Energy, Creativity, Healing, and Mythology as expressions of faith and religious tradition. Contemporary and traditional scientific analyses of belonging portray the holistic views of spirituality, theology, and connections to the universe. Universal sources or religions of the world such as Judaism, Christianity, Islam, Hinduism, Buddhism, Confucianism, and Shintoism offer meaning to their devotees. For example, a non-Jehovah’s Witness nurse may encounter a Jehovah’s Witness patient who has an aversion to blood transfusions; this nurse must collaborate with the team to offer alternatives such as volume expansion techniques. The role of the transcultural nurse is to recognize the needs of a patient’s religious values and rituals and endorse choice therein for well-being.
TRANSCULTURAL CARING INQUIRY: AWARENESS, UNDERSTANDING, AND CHOICE
Ray defined inquiry as knowledge discovery and development to comprehend another’s culture, as inherent in transcultural caring nursing practice. Cultural competence of healthcare staff is founded in mindfulness of the relationships and connections of health beliefs of varied populations. Ray’s theory underscores the need for cultural awareness, cultural understanding, and the provision of culturally applicable choices for diverse populations through recurring themes of caring, ethics, contextual considerations, and competence. Consideration of religious and cultural care needs, which, when accommodated, upholds mutual understanding and choices in care. Krogstie recently highlighted the importance of allowing choice expressed in Ray’s theory for marginalized populations potentially engaged in research in an unstable political culture. The concept, choice in this theoretical model showed the researcher a path forward that illuminated when research was not timely or beneficial to marginalized populations in a given political culture and environment.
THE VALUE OF REFLECTIVE ANALYSIS FOR SELF-AWARENESS OF PROVIDERS GUIDED BY RAY’S THEORY HIGHLIGHTING INDIVIDUAL PATIENT NEEDS
Reflective analysis is a dynamic, transformative educational process that enriches practice through in-depth identification of areas of accomplishment and needed improvement. As such, Johns, a scholar of reflective practice iterated “reflexive narrative is a journey of self-inquiry towards self-realization.” Critical reflection is used in nursing education to enhance competency of all key nursing skills to ensure patient comfort and safety across the lifespan; its promising outcomes include personal growth, self-awareness, problem solving, critical thinking, and empathy. Originally nursing knowledge was informed by other disciplines such as medicine and the social sciences; now nursing, as a discipline in its own right, informs other disciplines. Thus these authors declare that reflective analysis be used not only in nursing education, but also in medical education and practice to support optimal outcomes in the existing diverse patient populations encountered.
In health care, cultural competency has transpired as a crucial aspect of care delivery which takes into account a patient’s beliefs and preferences in societies wherein cultural and linguistic diversity abound. Cultural competency comprises accountability and responsibility for one’s action in the acquisition of knowledge, skills, and attitudes that enable a workforce to be effective in cross cultural work environments. In a scoping review of best practices for increasing cultural competency, findings included several educational strategies including lectures, discussions, simulations, and reflections to develop knowledge, awareness, attitudes and skills.
Caring is the essence of nursing. It is a crucial competency evaluated in nursing education. In the nursing profession, Ray defines caring as an empathic relationship with patients in which the principles of charity and the right action, compassion and love for others, and justice and equality are enacted in consideration of organizational and cultural contexts. A comprehensive scoping review about cultural competence initiatives in Europe identified several cultural models used in health care, including, of whom Ray was a student. Ray’s Transcultural Caring Dynamics in Nursing and Health Care Theory endorses the attainment of cultural competency through transcultural spiritual-ethical caring, i.e., accountability and responsibility in terms of empathy, compassion and justice for right action in practice with sensitivity to cultural needs of patients ever so relevant to healthcare professionals today including medical professionals.
In a Taiwanese qualitative study guided by Ray’s theoretical dimensions of caring, transcultural ethics, transcultural context, and universal sources written patient reflections about patient centered caring from 32 undergraduate nursing students were analyzed. Four themes were identified: 1) creating a caring experience to meet patient physical and psychological needs, 2) learning caring ethics by recognizing individual’s integrity and rights, 3) acknowledging influence of family, school peers, and communities influencing the caring experience, and 4) investigating teaching and learning approaches to enrich the caring experience, which all indicated the value of reflective analysis to support culturally suitable patient centered care.
Similar findings were revealed in a systematic review conducted in the Netherlands of 15 studies wherein three themes were identified: building and maintaining relationships, sense of belonging, and personal development, and eight subthemes of recognizing many perspectives, empathy, two way communication, patient centered care, processing thoughts and emotions, self-care, interaction positively with peers, and developing trust and community highlighting the universal advantages of reflective learning.
Johns described a concept advanced by Casement of a continuous dialogue the practitioner has with themselves in response to the unfolding situation about what is happening, how to respond, and what to achieve in clinical situations. In nursing and medical practices, Ray and Locsin explain this as a dynamic form of reflection-in-action, phenomenological hermeneutics (descriptive and intuitive interpretation). This awareness or openness to the unknown also leaves room for the patient to contribute to any subsequent knowing, and what is jointly discovered by professionals and patients. These ideas correspond with and highlight the concept of cultural competency (accountability and responsibility of the provision of spiritual-ethical caring); that is, the practitioner does not act by power-over the cultural other, but is mindful of how significant the patient (and family) of diverse cultures is as a part of the health care encounter since patients are whom we serve and they provide the foundational and holistic essence of their ethnicities–what means most to them in terms of their care.
There are many issues that must be taken into consideration to avoid potential culture value conflict in the provision of mutual culturally competent care, such as, communication itself in terms of linguistic differences, national/international legislative beliefs about health care delivery and the economics of health care, embracement of different health belief models and caring practices (complimentary, alternative, western, eastern, indigenous, middle eastern, tribal and so forth), diverse religious practices, and potential stereotyping, prejudice, ethnocentrism, class distinction on the part of the practitioner, and for patients, fear, gender characteristics or sexual diversity, cultural rituals and symbols, and overall, misunderstandings or potential conflict must be taken into consideration. As a consequence, spiritual ethical reflective inquiry is critical for transcultural caring based teaching and learning for the purpose of understanding patterns—the pattern of seeing, mapping (functioning), recognizing, and transforming. In summary, critical reflection-in-action is self-inquiry, that is, spiritual-ethical caring thought and action including understanding of how crucial self-inquiry of the patient and family is toward the self-realization of health. Summarily, the process involves respecting others through compassion and justice, seeking knowledge and understanding of the holistic nature of people to improve cultural awareness and decision making, understanding migration patterns, sustaining inter-professional collaboration, seeking knowledge of the influence of media cultures all to continually build local, civic, and inter-organizational/international communities that facilitate the choices for health, caring, healing, well-being and a peaceful death.
CONCLUSION
Contemporary knowledge about the changing world community, migration patterns, complex local and global health issues with identifiable social determinants of health (SDOH) highlight the need for developing awareness of the diversity of cultures and cultural competence. In this paper, Ray’s theory of transcultural caring science and its ethical, contextual, and spiritual dynamics, and reflection-in-action gives rise to understanding the meaning of cultural competence as accountability and responsibility in the provision of care for the ‘cultural other’ by healthcare professionals. Thus, as a cultural resource, the knowledge and theory provide opportunities for nurses and physicians to effectively practice transcultural health care which aligns with the unique cultural needs of each patient and their family.
Conflict of Interest Statement: The authors state that there are no conflicts of interest to declare.
Funding Statement: None.
Acknowledgements: None.
REFERENCES
- Leininger MM. Transcultural nursing and globalization of healthcare: Importance, focus and historical aspects. In Leininger MM and McFarland MR, eds, Transcultural Nursing: Concepts, Theories, Research & Practice (ed., pp. 3–44). McGraw Hill; 2002.
- Wehbe-Alamah H, McFarland M. Leininger’s Transcultural Healthcare: Concepts, Theories, Research & Practice. McGraw Hill; 2026.
- Boniol M, Kunjumen T, Nair TS, Siyam A, Campbell J, Diallo K. The global health workforce stock and distribution in 2020 and 2030: a threat to equity and ‘universal’ health coverage? BMJ Global Health. 2022;7(6):e009316. doi:10.1136/bmjgh-009316.
- Social Work Action. International Federation of Social Workers. Accessed April 30, 2026. https://www.ifsw.org/social-work-action/
- Krogstie R. Facing failure: Lessons from research on marginalized populations in an unstable political culture. Published November 17, 2025. Accessed April 30, 2026. https://nursology.net/2025/11/17/facing-failure-lessons-from-research-on-marginalized-populations-in-an-unstable-political-culture/
- Ray M. Transcultural Caring Dynamics in Nursing and Health Care (1st ed.). F. A. Davis; 2010.
- Ray M. Transcultural Caring Dynamics in Nursing and Health Care (2nd ed.). F. A. Davis; 2016.
- Ray M. Ray’s theory of transcultural caring dynamics in nursing and health care: A significant cultural resource. International Journal for Human Caring. 2024; 28(3): 61-68. http://dx.doi.org/10.20467/IJHC:2022-0048
- Ray M. (2021). Evolution of Ray’s theory of bureaucratic caring. International Journal for Human Caring. 25(3), 159-175. https://doi.org/10.20467/HumanCaring-D20-00043
- World Migration Report 2024. International Organization for Migration. Accessed April 30, 2026. https://worldmigrationreport.iom.int/msite/wmr2024-interactive/
- What are Health Disparities? National Institutes of Health. Published February 25, 2026. Accessed April 30, 2026. https://www.nimhd.nih.gov/about/what-are-health-disparities
- Scholz N. Addressing Health Inequalities in the European Union – Concepts, Action, State of Play. In-Depth Analysis. Brussels, Belgium: Parliamentary Research Service. Published February 2020. Accessed April 30, 2026. PE 646.18 URL: https://www.europarl.europa.eu/thinktank/en/document/EPRS_IDA(2020)646182
- Operational framework for monitoring social determinants of health equity. World Health Organization. who.int. Published January 18, 2024. Accessed April 30, 2026. https://www.who.int/publications/i/item/9789240088320
- Pacquiao DF, Maxwell JB, Ludwig-Beymer P, Stievano A, Sagar P, Purnell L, Daub K. Integration of population health, social determinants, and social justice in transcultural nursing and culturally competent care: White paper by the Scholars Education Interest Group. Journal of Transcultural Nursing. 2023; 34(3): 75-177. doi:10.1177/104365962231163878.
- The Universal Declaration of Human Rights. United Nations. un.org. Accessed April 30, 2026.
- Tang C, Tian B, Zhang X, Zhang K, Xiao X, Simoni JM, Wang H. The influence of cultural competence of nurses on patient satisfaction and the mediating effect of patient trust. Journal of Advances in Nursing. 2019; 75(4):749-759. doi:10.1111/jan.13854.
- Social Determinants of Health. AACN Essentials Tool Kit: Domains & Concepts. Accessed April 30, 2026. https://www.aacnnursing.org/essentials/toolkit/domains-concepts/social-determinants-of-health
- Nour N, Stuckler D, Ajayi O, Abdellah M. Effectiveness of alternative approaches to integrating SDOH into medical education: A scoping review. BMC Medical Education. 2023; 23: 18. https://doi.org/10.1186/s12909-022-03899-2
- Rosa WE, Dossey BM, Koithan M, Kreitzer MJ, Manjrekar P., Meleis A, Mukamana D, Ray M, Watson, J. Nursing theory in the quest for the Sustainable Development Goals. Nursing Science Quarterly. 2020; 33(2):178-182. doi:10.1177/0894318420903495.
- Wehbe-Alamah H. The Ethnonursing Research Method: Major features and enablers. In McFarland M, Wehbe-Alamah H. eds, Transcultural Nursing Concepts, Theories, Research and Practice. McGraw-Hill Education; 2018; 57-84.
- Wehbe-Alamah H, McFarland M. Leininger’s Ethnonursing Research Method: Historical retrospective and overview. Journal of Transcultural Nursing. 2020; 31(4): 337–349. https://doi.org/10.1177/1043659620912308.
- Boykin A, Schoenhofer S. Nursing as Caring: A Model for Transforming Practice. Jones & Bartlett Learning; 2001: 40.
- Parse RR. Human becoming: Parse’s theory of nursing. Nursing Science Quarterly. 1992; 5(1): 35–42. https://doi.org/10.1177/089431849200500109.
- Ray M, Turkel M. Caring as emancipatory nursing praxis: The theory of relational caring complexity. Advances in Nursing Science. 2014; 37(2), 132-146. https://doi.org/10.1097/ans.0000000000000024.
- Davidson AW, Ray MA, Turkel MC. Nursing, caring, and complexity science: for human-environment well-being.; 2011. http://lghttp.48653.nexcesscdn.net/80223CF/springer-static/media/samplechapters/9780826125873/9780826125873_chapter.pdf.
- Ray M. A study of caring within an institutional culture. [Dissertation], University of Utah, College of Nursing, Salt Lake City, Utah. Dissertation Abstracts International (University Microfilms, No. 81-27-787); 1981.
- Koszalinski R, Wilson C, Schaefer AM. Underpinning human health outcomes of harmful algal bloom Exposure Research: An analysis of the relationship and Applicability of the Bureaucratic Caring Theory. Scandinavian Journal of Caring Sciences. 2026; 40(1):e70199. doi:10.1111/scs.70199.
- Egan M. The ‘godfather’ of AI reveals the only way humanity can survive super intelligent AI. CNN Business. Published August 13, 2025. Accessed April 30, 2026. https://www.cnn.com/2025/08/13/tech/ai-geoffrey-hinton.
- Coyoca G, Ray M. A Nursing Research review of the application of the Phenomenological Caring Inquiry Methodology. Medical Research Archives. 2025;13(10). doi:10.18103/mra.v13i10.6963.
- Martin MB. Perceived discrimination of Muslims in health care. Journal of Muslim Mental Health. 2015;9(2):41-69.
- Johns C. Becoming a Reflective Practitioner (7th ed.). Wiley; 2025.
- Tseng T-J. Ray M. Wu CJ. Examining nursing students’ learning through reflective analysis using Ray’s transcultural caring dynamics in nursing and health care theory. British Medical Education. 2025; 25(559): 3-8. https://doi.org/10.1186/s12909-23-07123-9.
- Martin MB, Ray M. Enhancing the role of the transcultural healthcare provider in the global environment. In Wehbe-Alamah H, McFarland M, eds. Leininger’s Transcultural Healthcare: Concepts, Theories, Research & Practice. McGraw Hill; 2026.
- Leininger M. Leininger’s acculturation health care assessment tool for cultural patterns in traditional and non-traditional life ways. Journal of Transcultural Nursing. 1991; 2(2):40-42. www.ncbi.nlm.nih.gov/pubmed/20432395.
- Coyoca GS, Tuppal C, Ray M. Eliciting the Theory of Meaning on Self-Care for Nurses: Application of Ray’s Caring Inquiry. The Technician. 2025; 37(1). doi:10.62071/apjsi.v37i1.760.
- Poudel B. Ray M. Consciousness: Humanoid robots and caring in nursing from multicultural perspectives. International Journal for Human Caring. 2019; 23(2): 185-195. https://dx.doi.org/10.20467/1091-5710.23.2.185.
- Ray M. Illuminating the meaning of caring: Unfolding the sacred art of divine love. In M. Roach, ed. Caring from the heart: The Convergence of Caring and Spirituality. Paulist Press;163-178.
- Betancourt JR. Cultural competence and medical education: many names, many perspectives, one goal. Academic Medicine. 2006;81(6):499-501. doi:10.1097/01.acm.0000225211.77088.cb.
- Adeani IS, Febriani RB, Syafryadin S. Using Gibbs Reflective Cycle in making reflections of literary analysis. Indonesian EFL Journal. 2020;6(2):139. doi:10.25134/ieflj.v6i2.3382.
- Newman M, Smith M, Dexheimer Pharris M, Jones D. The focus of the discipline revisited. Advances in Nursing Science. 2008; 31(1): E16-E27. doi:10.1097/01.ANS.0000311533.65941.f1.
- Brottman MR, Char DM, Hattori RA, Heeb R, Taff SD. Toward cultural competency in health care: A scoping review of the diversity and inclusion education literature. Academic Medicine. 2019;95(5):803-813. doi:10.1097/acm.0000000000002995.
- Leininger M. The phenomenon of caring. Part V. Caring: the essence and central focus of nursing. Nurs Res Rep. 1977;12(1):2-14.