

Cupping of Large Optic Discs: Diagnostic Challenges in Africa
Cupping of large optic discs: a diagnostic challenge in African patients
Dr. D Soma, MBChB, FC Ophth(SA), MMed(Ophth)(SA)¹*, Prof. GD McLaren, MBBCh, FCS(SA)Ophth, FRCOphth(UK)², TR Carmichael MBBCh(Wits), FC Ophth(SA), PhD(Med), MSc(med)³
- Senior Lecturer and Clinical Unit Head of Ophthalmology at Steve Biko Academic Hospital, Division of Ophthalmology, Department of Health Sciences, University of Pretoria, Pretoria, South Africa.
- Emeritus Professor, Division of Ophthalmology, Department of Neurosciences, University of Witwatersrand, Johannesburg, South Africa.
- Professor, Division of Ophthalmology, Department of Neurosciences, University of Witwatersrand, Johannesburg, South Africa.
OPEN ACCESS
PUBLISHED: 30 November 2024
CITATIONSoma, D., McLaren, G.D., et al.2024. Cupping of large optic discs – a diagnostic challenge in African patients. Medical Research Archives, [online] 12(11).https://doi.org/10.18103/mra.v12i11.6107
COPYRIGHT © 2024 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v12i11.6107
ISSN 2375-1924
Abstract
Purpose: To determine in a cohort of African patients with large optic discs the relationship between disc size and central nervous system (CNS) pathology. The aim was to correlate the parameters of physiological cupping with the vertical cup to disc ratio (CDR).
Design: A prospective observational study.
Methods: Patients were identified from a database of patients who were glaucoma suspects, who are diagnosed with primary open angle glaucoma or normal tension glaucoma and attend the glaucoma clinic at St John Eye Hospital. This hospital is situated in Johannesburg, South Africa.
Results: A total of 40 patients with large discs and large cups (516/491) were identified. The mean age of the cohort was 56 years. Visual acuity ranged from a mean of -6.5 to a mean of 0.4.
Conclusion: The findings suggest that large optic discs are more likely to be misdiagnosed as glaucoma and that the parameters of physiological cupping need to be considered.
Keywords
- Optic disc
- Glaucoma
- Cupping
- African patients
Introduction
Glaucoma is an eye condition that results in optic nerve damage. This manifests as increased cupping of the disc. Cupping of the optic disc is a typical feature of glaucomatous optic nerve damage. Thus the vertical cup to disc ratio (CDR) has been used in the evaluation of glaucoma. The cup size is related physiologically to the disc size and pathologically to glaucomatous damage. A glaucomatous optic nerve gives rise to visual field changes. In addition, retinal nerve fibre layer atrophy occurs in glaucoma.
Diagnosing pathological changes based on the vertical cup to disc ratio alone is of limited value. It is important to take into account the disc size¹. There are different methods to measure disc size and each with its own strength and limitations. It is possible to measure the optic nerve head at the slitlamp with different types of lenses². By using a 60 diopter lens and a high magnification fundus lens (volk 60 diopter lens) a vertical slit is placed over the optic disc to measure the vertical disc diameter. Correction factors may be needed depending on the power of the lens used.³ A 60 diopter Volk lens has a correction factor of 0.92³.
Racial differences in optic disc size exists. A number of studies have shown that Africans have larger optic discs compared to Europeans⁴˒⁵.
Healey et al showed in the Blue Mountain Eye Study that there is an increase in the cup to disc ratio with an increase in the vertical disc size⁶. This is significant enough to warrant measurement of the optic disc size. Large optic discs are defined as optic discs measuring 1.8mm or more⁷. The importance of assessing the vertical cup to disc ratio in relation to disc size was extensively studied by Jonas and co-workers⁸ as well as Garway-Heath and associates⁹. They showed that the vertical cup to disc ratio for disc size has the highest diagnostic power compared to other optic disc parameters for separating normal subjects from pre-perimetric glaucoma patients.
It is clinically difficult to distinguish physiologic cupping from glaucomatous changes. Patients with large vertical cup to disc ratios are generally misdiagnosed as glaucomatous. This can be prevented if disc size is measured because we know that large discs generally have large vertical cup to disc ratios⁶˒⁸˒⁹. In this way, the distinction between physiologic cupping and glaucomatous cupping can be made with greater confidence.
There is controversy whether there is a positive correlation between disc size and retinal nerve fibre layer thickness. Cross section study by Budenz et al.¹⁰ showed that for every square millimeter increase in cup disc area, the mean retinal nerve fibre layer increased by 3.3um.
Central corneal thickness (CCT) plays an important role in the diagnosis of glaucoma. And it influences the intraocular pressure. In a cross section study by Brandt et al.¹¹ 1301 patients with ocular hypertension were studied to determine if CCT influences intraocular pressure (IOP) measurements at different pressures. They showed that the mean CCT for Africans was 555.7um and for Europeans was 573um. They showed that Africans had thinner corneas than Europeans and concluded that CCT may influence the accuracy of IOP measurements. Thin corneas underestimate IOP measurements and thick corneas overestimate IOP measurements¹˒¹².
Objectives
The objectives of this study was to determine in a cohort of 69 African patients with large optic discs and large optic cups, that proportion of patients with physiologic cupping misdiagnosed as glaucomatous. Also, to evaluate the possible relationship between optic disc size and central corneal thickness in the African population.
Study design
A case series consisting of 69 African patients with large optic discs and large optic cups, were evaluated, to determine what proportion had physiologic cupping and what proportion were glaucomatous and categorised as normal were further evaluated to determine what proportion was
misdiagnosed and treated as glaucoma. The relationship between disc size and central corneal thickness was also evaluated.
Glaucoma patients in this project is defined as patients who are glaucoma suspects, who are diagnosed with primary open angle glaucoma or normal tension glaucoma and attend the glaucoma clinic at St John Eye Hospital. This hospital is situated in Johannesburg, South Africa.
Method
Prior to this research project being carried out, a protocol was submitted to the human research ethics committee (medical) at the University of the Witwatersrand in Johannesburg. A clearance certificate was issued (M070435).
Large discs are defined as optic discs having a corrected vertical disc height measuring more than 1.8mm. Large cups are defined as cup to disc ratios of 0.6 or more.
This was a convenience sampling of glaucoma patients with large optic discs and large optic cups, attending the glaucoma clinic at St John Eye Hospital. Patients were invited to participate in the study and informed consent was obtained from those patients willing to participate in the study.
-
A glaucoma suspect is defined as a patient with one of the following three features. An optic nerve or retinal nerve fibre layer (RNFL) defect, or visual field abnormality consistent with glaucoma, or a consistently high IOP (>22mmHg)¹³.
-
Primary open angle glaucoma is defined as a triad of increased IOP, optic nerve head changes and changes on the visual field or RNFL analysis¹³.
-
Normal tension glaucoma is defined as IOP<21mmHg with visual field defects and RNFL defects¹³.
-
Ocular hypertension is defined as IOP>21mmHg and no changes on visual fields or the RNFL analysis¹³.
High myopes (myopic more than -8 diopters) and children were excluded from the study. High myopes were excluded because they have markedly different appearances of the optic nerve head, in normal and glaucomatous eyes¹⁴˒¹⁵. Also, the vertical disc height is influenced by axial length (high myopia) and not by the distance of the lens from the cornea or by the refractive errors less than -8 diopters¹⁶.
Clinical examination included history, slit-lamp biomicroscopy findings which included IOP, gonioscopy and fundus examination that concentrated on the qualitative and quantitative measurements of the optic nerve head. Special investigations included refraction, CCT measurements, visual fields and retinal nerve fibre layer analysis.
A Haag Streit biomicroscope was used to examine the eye. A 60 diopter lens was used to examine and measure the optic disc head. A vertical slit-beam was placed over the optic disc and the beam was adjusted to measure the vertical disc diameter. The measurement was read off the calibrated rod of the biomicroscope. A correction factor was needed for the lens (x1.02 for the Nikon 60 D lens)³.
A calibrated Goldmann tonometer was used to measure the intraocular pressure (IOP). This measurement was entered into the Heidelberg engineering IOPac advanced pachymeter to obtain the Adjusted-IOP (A-IOP), taking the central corneal thickness into account.
Gonioscopy was performed using a Volk 3-mirror-lens.The Shaffer-Etienne classification system was used in this study which defines:
Grade 0 – No structures are visible and represents a closed angle.
Grade 1 – Schwalbe line is visible and represents possible angle closure.
Grade 2 – Schwalbe line and trabecular meshwork are visible but scleral spur not visible in a narrow angle.
Grade 3 – Scleral spur is visible and angle closure is impossible.
Grade 4 – All structures are visible from Schwalbe’s line to the ciliary band.
Refraction was carried out with a Nikon handheld autorefractor and refined subjectively. In this way, patients who were more myopic than -8 diopters, or more hyperopic than +4 diopters, were excluded from the study.
Visual fields were performed using the Oculus automotive perimeter. This documented any functional loss or progression of functional loss by the nerve over time. This was followed up for at least 5 years in order to exclude any progression to glaucoma in patients who were classified as having physiologic cupping.
The GDxVCC (Carl Zeiss meditec Inc., Dublin CA, USA), is a retinal nerve fibre layer (RNFL) analyzer that uses scanning laser polarimetry to quantify the nerve fibre layer thickness in order to detect early glaucomatous changes³. A retinal nerve fibre analysis was done with a scanning laser polarimeter to confirm the presence or absence of glaucomatous retinal nerve fibre layer defects. This was based on the nerve fibre index, TSNIT (temporal, superior, nasal, inferior, temporal) graph and parameters and the deviation map¹⁷.
The excel data base was used for data summary. Statistics were performed using the statistical software Stata version 8 (Stata Corporation, College station, Texas, USA).
Results
Hundred and thirty eight eyes of 69 African patients were analysed. Forty seven patients (71%) were female and 28 (41%) were male. Patients ages ranged between 18 to 87 years with a mean age of 56 years. Visual acuity ranged from 6/6 to light perception. Refraction ranged from myopia of -6.5 D to hyperopia of +4 D.
From a cohort of 69 patients with large discs and large cups, 51/69 (74%) had normal eyes and 18/69 (26%) had pathologic cupping. The group of 51 patients with normal eyes was further evaluated and 9/51 (18%) were previously misdiagnosed and treated with anti-glaucoma medications. The main reason for the misdiagnosis was an increased cup to disc ratio in the presence of a large disc.
OUTCOME MEASURES
• central corneal thickness (CCT)
• intraocular pressure (IOP) and adjusted intraocular pressure (A-IOP)
• corrected vertical disc height (VDH)
• vertical cup to disc ratio (CDR)
• relationship between VDH and vertical cup height
• relationship between VDH and central corneal thickness
• retinal nerve fibre layer analysis
• visual fields
CENTRAL CORNEAL THICKNESS
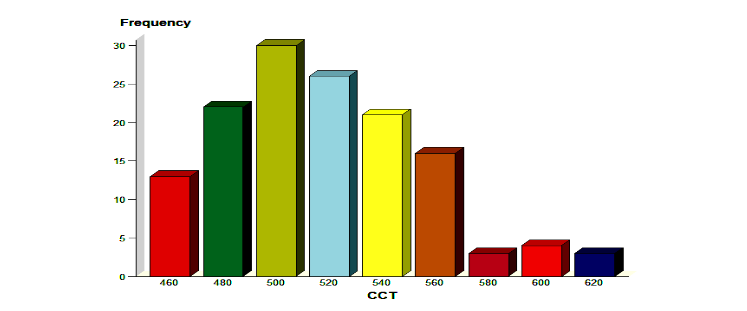
This was measured using the Heidelberg engineering IOPac advanced pachymeter. It ranged between 454μm and 618μm. The mean CCT was 516μm±37.5μm. (Figure 1) In this study, CCT<544μm was regarded as a thin cornea. Out of a total of 138 eyes, 107 eyes (77.5%) had CCT<544μm.
Refraction was carried out with a Nikon handheld autorefractor and refined subjectively. In this way, patients who were more myopic than -8 diopters, or more hyperopic than +4 diopters, were excluded from the study.
Visual fields were performed using the Oculus automated perimeter. This documented any functional loss or progression of functional loss by the retinal nerve fibre layer analysis. This was followed up for at least 5 years in order to exclude any progression to glaucoma in patients who were classified as having normal fields.
The GDxVCC (Carl Zeiss meditec Inc., Dublin CA, USA), is a retinal nerve fibre layer (RNFL) analyzer that uses a scanning laser polarimeter to quantify the retinal nerve fibre layer thickness. The Nerve fibre index (NFI) is the best parameter to differentiate glaucomatous and healthy eyes. The NFI ranges from zero to one hundred. The more advanced the glaucoma, the higher the NFI. Glaucoma eyes have NFI values of 35 and above and healthy eyes have NFI values of 44 and below. An NFI value between 35 and 44 is considered borderline and therefore does not make the diagnosis of glaucoma.
The TSNIT graph (TSNIT) shows RNFL values of the eyes on the expected age related normative data. The RNFL graph made the diagnosis of glaucoma possible.
VERTICAL CUP TO DISC RATIO
The vertical cup to disc ratio was measured relative to VDH. The vertical cup to disc ratio ranged from 0.6 to 1 (mean±SD, 0.7±0.08).
RELATIONSHIP BETWEEN VDH AND VERTICAL CUP HEIGHT
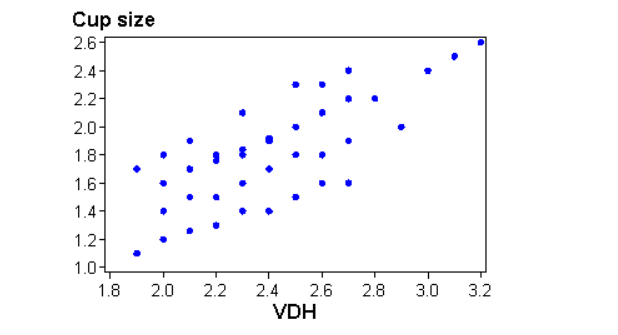
The vertical cup height was calculated by taking the CDR and multiplying it with the VDH. The vertical cup height increased with an increase in VDH. There was a positive linear relationship between the vertical cup height and the VDH. (Figure 3)
Figure 3. The relationship between VDH and vertical cup height
RELATIONSHIP BETWEEN VDH AND CCT
Vertical disc height ranged between 1.9mm and 3.2mm. The central corneal thickness ranged from 454μm to 618μm. There was no linear correlation between VDH and CCT. The Pearson correlation co-efficient was 0.13.
RETINAL NERVE FIBRE LAYER ANALYSIS
This was carried out for each eye. The findings were interpreted as normal, having RNFL changes indicative of glaucoma or as unsuccessful. The parameters that were considered for the above were based on
-
The nerve fibre index (NFI).
This is the best parameter to differentiate glaucomatous and healthy eyes¹⁷. The NFI ranges from zero to one hundred. The more advanced the glaucoma, the higher the NFI. Glaucoma eyes have NFI values of 35 and above and healthy eyes have NFI values of 44 and below. A NFI value between 35 and 44 is considered borderline and therefore other data in the GDxVCC printout may be used to make the diagnosis of glaucoma. -
The TSNIT graph – This shows RNFL values of each of the eyes on the expected age related normal range¹⁷.
-
The deviation map – This map plots the RNFL values that deviate from the normal range. The colour coded p-values indicate the extent of the deviation¹⁷.
In this study the NFI for normal eyes ranged between 3 and 44. The mean NFI for all normal eyes was 38. The NFI for glaucoma eyes ranged between 35 and 98. The mean NFI for glaucoma eyes was 49.6. In eyes that had borderline NFI values i.e. NFI values between 35 and 44, other parameters on the GDxVCC together with the visual fields were used to determine if the eye had glaucoma or not.
The reason for an unsuccessful GDxVCC evaluation, which occurred in 8 eyes, was due to poor visualization of the fundii due to cataract formation.
VISUAL FIELDS
The Oculus automotive perimeter was used to measure and document visual fields in all 138 eyes. Although the study was carried out over 4 months, visual fields done before the 4 months were also assessed and followed up for 5 years to ensure the absence of glaucomatous progression in patients diagnosed with physiologic cupping. The visual fields were compared to ascertain if there were glaucomatous field losses or if there was any progression of field loss. Fields were categorized as having glaucomatous change, normal, unreliable or unsuccessful. In this study, fields with glaucomatous change was defined as one of the following: A glaucoma hemifield test outside normal limits on at least two consecutive occasions or a cluster of three or more non-edge points in a location typical for glaucoma or a corrected pattern standard deviation in less than 5% of normal individuals on two consecutive fields¹³. Normal fields were defined as visual fields with no glaucomatous changes. Unreliable fields were defined as visual fields where glaucomatous changes were difficult to assess. Unsuccessful visual fields were due to profound visual loss.
In this study, there was a total of 138 eyes. 18/138 (13%) visual fields could not be determined as normal or having glaucomatous defects because the visual fields were unreliable or unsuccessful. 51 eyes were correctly diagnosed as having physiologic cupping of the optic discs and had normal visual fields. Out of the 51 eyes that were previously misdiagnosed with glaucoma, 30 eyes showed glaucomatous visual field defects, 5 visual fields were unreliable and 1 visual field was unsuccessful. Glaucoma was diagnosed in the latter two groups with the aid of the GDxVCC.
Discussion
Examination of the optic nerve head in glaucoma commonly involves the evaluation of the optic cup, the neuroretinal rim contour and the retinal nerve fibre layer. An important but overlooked component of the optic nerve head evaluation is measurement of the optic disc size.
In healthy subjects, small discs can have small cups and large discs can have large cups¹⁶. Large discs with large cups can therefore be misdiagnosed as glaucoma. Sometimes the visual fields obtained may be unreliable and therefore the diagnosis of glaucoma becomes a challenge to the ophthalmologist.
This study was limited to African patients. There were several reasons for this. Firstly, there is a increased prevalence of glaucoma in African patients. This was shown in the Baltimore Eye Study which showed that African-Americans have a higher prevalence of glaucoma across all age groups when compared to Europeans in the same city¹⁸˒¹⁹. A study done by Rotchford et al.²⁰ also showed that glaucoma was one of the leading causes of blindness in people of African origin in rural Zululand (South Africa). Secondly, the optic disc head characteristics in African patients differ from their European counterparts⁴˒⁵˒²⁰. African patients have larger optic disc sizes when compared to their European counterparts⁴˒⁵. Thirdly, African patients have thin central corneal thickness when compared to their European counterparts¹¹˒¹²˒²¹˒²². By limiting the data to African patients, it was hoped that consistent results, not confounded by findings from other racial groups, would be achieved.
Optic disc size is influenced by a number of factors. It may be influenced by age and gender. In addition, variation in anatomical structures of the optic nerve head and the retinal nerve fibre layer is associated with variation in disc size. Due to the small number of cases, a limitation of this study is that no comparisons could be drawn about disc size related to age and gender.
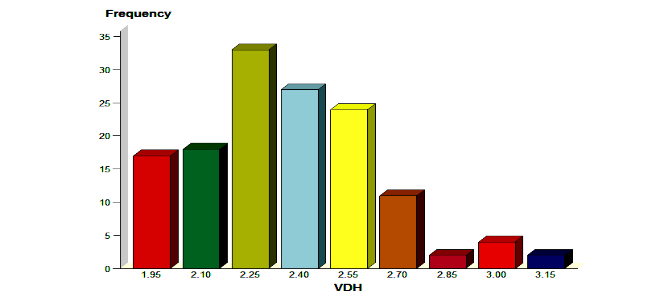
Africans have larger discs when compared to their European counterparts¹²˒¹³. The mean vertical and horizontal disc diameters as measured by Quigley for the disc of a normal human eye is a vertical disc diameter of 1.88mm and a horizontal diameter of 1.77mm²³. In this study, large discs were defined as discs with a vertical height measuring more than 1.8mm. The vertical disc height (VDH) ranged between 1.9 and 3.2mm (mean±SD,2.3±0.26) and the horizontal disc diameter (HDD) ranged between 1.7 to 2.9mm (mean±SD, 2.1±0.22). Studies conducted by Quigley et al (1990) also demonstrated larger vertical disc height in Africans (1.96±0.16) compared to the VDH of Caucasians (1.82±0.15)²³. This study showed much larger disc sizes, possibly due to genetic variation. There was a normal gaussian distribution for VDH (Figure 2).
Large cups were defined as a cup-disc ratio greater than 0.6. The Blue Mountains Eye Study showed that for each 0.1 millimeter increase in disc diameter there was an increase in cup to disc ratio of 0.27⁶˒⁷. Beck et al reported that large discs have proportionately large cup to disc ratios in the normal eyes of African subjects²⁴. The data from our study showed that there was a direct linear relationship between vertical disc height and vertical cup height (Figure 3).
Central corneal thickness influences intraocular pressure measurements. The mean central corneal thickness in the normal human eye is 545μm²². In this study, the CCT ranged from 457μm to 616μm (mean±SD,516±37μm) and 77.5% of patients had thin corneas (CCT<544μm). Thick corneas overestimate actual intraocular pressure measurements and thin corneas underestimate intraocular pressure measurements²². In this study, no conclusion could be found between disc size and thin corneas. The Pearson correlation co-efficient was 0.12657. A study done in the United States showed an inverse relationship between disc size and CCT in African-American patients, but that this was not statistically significant¹².
To diagnose glaucoma, the following criteria was used: an increased intraocular pressure; structural changes of the optic nerve head; visual field changes and corresponding retinal nerve fibre layer damage on the scanning laser polarimeter (GDxVCC). In this study, unreliable visual fields sometimes made it difficult to make a diagnosis of glaucoma and the researchers therefore had to rely on the retinal nerve fibre layer analysis to assist with the diagnosis. It is important to bear in mind that during early glaucoma, there may not be visual field defects and patients therefore needed to be followed up for at least 5 years to ensure that patients in the physiologic cupping group did not progress to glaucoma.
Of the 69 patients studied, 51 patients (74%) had physiologic cupping and 18 patients (26%) had pathologic cupping. Of the 51 patients with physiologic cupping, 9 (18%) were previously
misdiagnosed as glaucoma and had received unnecessary treatment while the other 42 (82%) patients were correctly diagnosed as physiologic cupping.
A significant number of patients in the group of patients with large discs (51/69) had physiological cupping. The researchers concluded that although Africans are more susceptible to glaucoma and have large discs, large discs is not on its own a risk factor for the development of glaucoma. The researchers further concluded that large discs that have proportionately larger cups are more likely to be misdiagnosed as glaucoma than be diagnosed as physiologic cupping. Nine of the 51 patients were erroneously misdiagnosed and treated for glaucoma. The reason for the misdiagnosis was a large cup size in a large disc. Studies conducted by Heijl and Mölder showed that larger discs were more likely to be misdiagnosed with glaucoma than were smaller discs²⁵. It is logical therefore that disc size may affect the diagnosis.
Of the nine patients misdiagnosed and treated for glaucoma, one patient had undergone surgery unnecessarily. The patient who had undergone surgery did not disclose that she had been taking allergy medication (comprising topical steroids). On examination, she was found to have large cups, an increased intraocular pressure and unreliable visual fields. This trend continued for a period of time. At that point in time ophthalmologists at the hospital did not have access to a scanning laser polarimeter such as the GDxVCC. A trabeculectomy was carried out. Post-trabeculectomy, her IOP increased and it was then discovered that she was a steroid responder. She was found to have large discs with large cups. Years later when the scanning laser polarimeter (GDxVCC) became available, the retinal nerve fibre layer of this patient showed no retinal nerve fibre layer defects.
Although the literature reports an increase incidence of glaucoma in African patients, one has to be very careful in diagnosing a patient with glaucoma, because the possibility of physiological cupping in African patients with large discs must be considered. On the other hand a recent article Kim et al mentioned risk factors on fundus photography that can predict the conversion of cupping in large discs to glaucoma. This falls out of the scope of this study²⁶.
Conclusion
Africans have large discs and patients with large discs have corresponding large cups. Large cups do not necessarily imply that the patient has glaucoma. In this study, the majority – 51 of the 69 patients (74%) – with large discs and large cups had physiologic cupping. Nine of the 51 patients were misdiagnosed as having glaucoma. The main reason for misdiagnosis was a large cup in relation to a large disc. Measuring these parameters may aid in preventing the misdiagnosis of glaucoma, unnecessary treatment and morbidity to these patients.
Patients have thin corneas and large discs. The thinner the cornea the lower the measured intraocular pressure, i.e. thin corneas underestimate IOP, and this has to be taken into account in the diagnosis of glaucoma. In this study, 77.5% of patients had thin corneas (CCT<544µm) but the researchers found no inverse correlation between CCT and disc size.
Conflict of Interest:
The authors have no conflict of interest to disclose.
Funding Statement:
The authors received no funding towards this research.
Acknowledgements:
None.
References
1. LaRosa F, Gross R, Orengo-Nania S. Central corneal thickness of Caucasians and African-Americans in glaucomatous and non-glaucomatous populations. Arch Ophthalmol 2001;119:23-7.
2. Ansari-Shahrezaei S, Maar N, Biowski R, et al. Biomicroscopic Measurement of the Optic Disc with a High-Power Positive lens. Invest Ophthalmol Vis Sci 2001;42:153-157.
3. Hitchings RA, Migdal C, Bechetoille A, et al. Terminology and guidelines for glaucoma. 2nd ed. Italy: Editrice DOGMA s.r.l, 2003:1-13,1-19,1-20.
4. Chi T, Ritch R, Stickler D, et al. Racial differences in optic nerve head parameters. Arch Ophthalmol 1989;107:836-9.
5. Varma R, Tielsch JM, Quigley HA, et al. Race, age, gender and refractive error related differences in the normal optic disc. Arch Ophthalmol 1994; 112:1068-76.
6. Healey PR, Mitchell P, Smith W, et al. Relationship between cup-disc ratio and optic disc diameter: The Blue Mountains Eye Study. Aust N Z J Ophthalmol 1997;25:S99-101.
7. Crowston JG, Hopley CR, Healey PR, et al. The effect of optic disc diameter on vertical cup to disc ratio percentiles in a population based cohort: The Blue Mountains Eye Study. Br J Ophthalmol 2004; 88:766-70.
8. Jonas JB, Bergua A, Schmitz-Valckenberg P, et al. Ranking of Optic Disc Cariables for Detection of Glaucomatous Optic Nerve Damage. Invest Ophthalmol Vis Sci 2000;41:1764-1773.
9. Garway-Heath DF, Ruben ST, Viswanathan A, et al. Vertical cup/disc ratio in relation to optic disc size: Its value in the assessment of the glaucoma suspect. Br J Ophthalmol 1998;82:1118-24.
10. Bedenz DL, Anderson DR, Varma R, et al. Determinants of Normal Retinal Nerve Fibre lLayer Thickness Measured by Stratus OCT. Ophthalmology 2007;5:1-5.
11. Brandt JD, Beisser JA, Kass MA, et al. Central corneal thickness in Ocular Hypertension Treatment Study (OHTS). Ophthalmology 2001;108:1779-1788.
12. Pakravan M, Parsa A, Sanagou M, et al. Central corneal thickness and correlation to optic disc size: A potential link for susceptibility to glaucoma. Br J Ophthalmol 2007;91:26-8.
13. Salmon J. Kanski’s Clinical Ophthalmology. A Systematic Approach. 9th Edition. Butterworth-Heinemann. Elsvier. 2021.
14. Jonas JB, Gusek GC, Naumann GOH. Optic disc morphology in high myopia. Graefes Arch Clin Exp Ophthalmol 1988;226:587-90.
15. Jonas JB, Dichtl A. Optic disc morphology in myopic primary open-angle glaucoma. Graefes Arch Clin Exp Ophthalmol 1997;235:627-33.
16. Susanna R Jr, Vessani RM. New findings in the evaluation of the optic disc in glaucoma diagnosis. Curr Opin Ophthalmol 2007;18:122-128.
17. Lester M, Garway-Heath D, Leimj H. Optic nerve head and retinal nerve fiber analysis. Italy: Editrice DOGMA s.r.l, 2003:101-2.
18. Tielsch JM, Sommer A, Katz J, et al. Racial variations in the prevalence of primary open angle glaucoma: Baltimore Eye Survey. JAMA 1991; 266:369-74.
19.Kyari F, Abdull MM, Bastawrous et al. Epidemiology of Glaucoma in Sub-Saharan Africa: Prevalence, Incidence and Risk Factors. Middle East Afr J Ophthalmol 2013;20(2):111-125.
20. Rotchford AP, Johnson GJ. Glaucoma in Zulus: A population-based cross-sectional survey in a rural district in South Africa. Arch Ophthalmol 2002;120:471-8.
21. Doughty MJ, Zaman ML. Human corneal thickness and its impact on intraocular pressure measures: a review and meta-analysis approach. Surv Ophthalmol 2000;44:367-408.
22. Baboolal SO and Smit DP. South African Eye Study (SAES): ethnic differences in central corneal thickness and intraocular pressure. Eye 2018; 32:749-756.
23. Quigley HA, Brown AE, Morrison JD, et al. The size and shape of the optic disc in normal human eyes. Arch Ophthalmol 1990;108:51-7.
24. Beck RW, Messner DK, Musch DC, et al. Is there a racial difference in physiologic cup size? Ophthalmology 1985;92:873-6.
25. Heijl A, Mölder H. Optic disc diameter influences the ability to detect glaucomatous disc damage. Acta Ophthalmol 1993;71:122-9.
26. Kim YW, Yun YI and Choi HJ. Screeningfundus photography predicts and reveals risk factors for glaucoma conversion in eyes with large optic disc cupping. Sci Rep 2023;13:81-92.