





Cyanoacrylate Adhesive in Laparoscopic Hernia Repair
Use of cyanoacrylate adhesive for fixation of mesh and peritoneum in transabdominal preperitoneal laparoscopic inguinal hernia repair
Radenko Koprivica, MD, PhD¹, Sanjanin Perišić, MD¹, Jernej Šadl MD¹*
- General Hospital Murska Sobota, Slovenia.
Email: [email protected]
Mobile: +386 64 180 665
OPEN ACCESS
PUBLISHED: 30 April 2025
CITATION: Koprivica, R., Perišić, S., et al., 2025. Use of cyanoacrylate adhesive for fixation of mesh and peritoneum in transabdominal preperitoneal laparoscopic inguinal hernia repair. Medical Research Archives, [online] 13(4). https://doi.org/10.18103/mra.v13i4.6340
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i4.6340
ISSN 2375-1924
ABSTRACT
Introduction: Inguinal hernia surgery is among the most commonly performed operations in general surgery. Standard surgical approaches include open or laparoscopic techniques with various mesh fixation methods: tissue-perforating fixation devices, adhesives, or non-fixation techniques. The European Hernia Society (EHS) guidelines indicate that adhesives for mesh fixation and peritoneal closure can reduce both acute and chronic postoperative pain compared to tissue-perforating fixation methods.
Material and method: Between February 1, 2023, and August 31, 2023, we prospectively monitored 20 male patients divided into two equal groups: Group I (GI) underwent transabdominal preperitoneal (TAPP) procedure with mesh and peritoneum closure using absorbable tacks, while Group II (GII) underwent TAPP procedure with mesh and peritoneum closure using n-butyl-2-cyanoacrylate (NBCA) adhesive. Both groups received light polypropylene titanium mesh (10×15 cm). Postoperative analgesia protocols were identical for all patients. We evaluated the technical success of mesh and peritoneum fixation, postoperative pain using a visual analog scale (VAS), and early complications including hematomas, wound infections, and hernia recurrence. Follow-up assessments were performed on postoperative days 1, 6, and 30. Statistical analysis employed standard descriptive statistics, one and two-factor analysis of variance, multiple range tests, median Mood test, and Tukey test.
Results: The average patient age was 53.7 years with no significant differences between groups. During the 30-day follow-up period, no recurrent hernias, wound infections, or hematomas were observed in either group. Mesh fixation and peritoneal closure were successfully achieved in all cases across both groups. Two-factor analysis of variance showed no statistically significant difference in overall pain scores between the groups. However, Group II (adhesive) demonstrated significantly faster pain reduction over time. By postoperative day 6, patients in Group II reported pain levels equivalent to those reported by Group I patients at day 30 (VAS 0.8). Multiple range tests confirmed that the adhesive technique resulted in significantly more rapid pain reduction compared to the tack fixation method.
Conclusion: The n-butyl-2-cyanoacrylate adhesive technique represents a safe, effective method for mesh fixation and peritoneal closure in TAPP hernia repair. This approach provides superior results in preventing and reducing postoperative pain compared to tissue-perforating fixation techniques, potentially leading to faster recovery and improved patient outcomes.
Keywords: Transabdominal preperitoneal repair, mesh fixation, adhesive technique, cyanoacrylate, peritoneal closure, postoperative pain.
INTRODUCTION
Inguinal hernia surgery represents the most commonly performed general surgical procedure in both Europe and the United States, with over 20 million operations performed annually worldwide. The evolution of surgical techniques for inguinal hernia repair has led to several standardized approaches, including open repair (with or without mesh) and minimally invasive laparoscopic techniques. Within the laparoscopic approaches, different methods of mesh fixation have emerged: tissue-perforating techniques (tacks, staples, sutures), adhesive fixation (fibrin glue, cyanoacrylate), and non-fixation techniques.
Non-fixation mesh methods offer advantages of simplicity and reduced postoperative pain. However, they carry potential disadvantages including excessive mesh mobility, lower tensile strength, and potentially higher recurrence rates. Meta-analyses comparing fixation versus non-fixation methods in laparoscopic hernia repair have shown no statistically significant differences in hernia recurrence rates, suggesting that both approaches may be viable in selected patients.
The International Endohernia Society (IEHS) currently recommends considering non-fixation techniques in transabdominal preperitoneal hernia repair (TAPP) for types LI, LII, MI, and MII inguinal hernias according to the European Hernia Society (EHS) classification system. This guidance reflects the ongoing evolution toward less invasive, less painful approaches that maintain excellent outcomes.
For cases where mesh fixation is indicated, adhesive fixation techniques have gained popularity. The adhesives used for mesh fixation can be categorized into three main groups: synthetic adhesives (cyanoacrylates), biological adhesives (fibrin glue), and genetically engineered polymeric adhesives. Numerous studies have demonstrated that adhesive fixation of mesh may decrease postoperative complications compared to traditional tissue-perforating fixation methods.
Importantly, the EHS guidelines emphasize that adhesive fixation of mesh and peritoneal closure reduces both acute and chronic postoperative pain compared to tissue-perforating fixation methods. This pain reduction represents a significant advantage, as chronic postoperative pain remains one of the most troublesome long-term complications following inguinal hernia repair.
Our study aims to prospectively compare traditional absorbable tack fixation with n-butyl-2-cyanoacrylate (NBCA) adhesive for both mesh fixation and peritoneal closure in TAPP repair, with a focus on technical success, postoperative pain, and early complications.
MATERIAL AND METHOD
Between February 1, 2023, and August 31, 2023, we conducted a prospective comparative study of 20 male patients undergoing laparoscopic inguinal hernia repair. Patients were divided into two equal groups:
- Group I (GI): Patients undergoing TAPP procedure with mesh and peritoneum closure using absorbable tacks
- Group II (GII): Patients undergoing TAPP procedure with mesh and peritoneum closure using NBCA adhesive
INCLUSION AND EXCLUSION CRITERIA
Inclusion criteria for the study were:
- Male gender
- Adult patients (>18 years)
- American Society of Anesthesiologists (ASA) classification I-III
- Direct, indirect, or bilateral inguinal hernia classified as LI-III or MI-III according to the EHS classification
Exclusion criteria were:
- Female gender
- Large inguinoscrotal hernia
- Severe comorbidity
- Use of anticoagulant therapy
- Corticosteroid therapy
- Immunosuppressive therapy
- Psychiatric medication
SURGICAL TECHNIQUE
All patients were operated on by the same surgeon to minimize technical variability. In Group I, mesh fixation and peritoneal closure were performed using absorbable tacks (SecureStrap, absorbable strap fixation device, Ethicon, Johnson & Johnson). An average of 5-7 tacks were used for mesh fixation, and 7-8 tacks for peritoneal closure.
In Group II, mesh and peritoneum were fixed using a laparoscopic instrument with n-butyl-2-cyanoacrylate adhesive (Liquiband Fix 8 by Advanced Medical Solution, Plymouth, UK). Adhesive was applied at approximately the same number of focal points as tacks in Group I. For peritoneal closure in Group II, intra-abdominal pressure was reduced from 14 mmHg to 6-8 mmHg before adhesive application. After adhesive application and complete desufflation, a 5-minute waiting period was observed to allow proper adhesive curing. The abdomen was then re-insufflated to 8 mmHg to inspect the integrity of peritoneal closure.
For both groups, we used identical light polypropylene titanium mesh measuring 10×15 cm (TilenBlue, pfm medical, Germany).
POSTOPERATIVE CARE AND FOLLOW-UP
Postoperative analgesia was standardized for all patients: intravenous paracetamol 1 gram four times daily on the first postoperative day, followed by oral paracetamol 500 mg three times daily for an additional three days. All patients were discharged on the first postoperative day per protocol.
We recorded the technical success of mesh fixation and peritoneal closure, postoperative pain (measured using a visual analog scale), and early postoperative complications including hematomas, wound infections, and hernia recurrence. Follow-up evaluations were performed on postoperative days 1, 6, and 30.
STATISTICAL ANALYSIS
Statistical analysis employed standard descriptive statistics, one and two-factor analysis of variance, multiple range tests, median Mood test, and Tukey test. A p-value <0.05 was considered statistically significant.
RESULTS
The average age of patients was 53.7 years without significant differences between groups. The distribution of hernia characteristics was similar between groups, with 4 patients (20%) presenting with bilateral inguinal hernias, 9 patients (45%) with right-sided hernias, and 7 patients (35%) with left-sided hernias.
According to the EHS classification, hernia size distribution was comparable between groups: 50% of cases were LII or MII, 30% were LI or MI, and 20% were LIII or MIII. The demographic and clinical characteristics of both groups are summarized in Table 1.
| Characteristic | Group I (Tacks) | Group II (Adhesive) |
|---|---|---|
| Bilateral inguinal hernia | 2 (20%) | 2 (20%) |
| Right inguinal hernia | 4 (40%) | 5 (50%) |
| Left inguinal hernia | 4 (40%) | 3 (30%) |
| LI, MI (<1.5cm) EHS classification | 3 (30%) | 3 (30%) |
| LII, MII (1.5-3cm) EHS classification | 5 (50%) | 5 (50%) |
| LIII, MIII (>3cm) EHS classification | 2 (20%) | 2 (20%) |
| Hematoma | 0 (0%) | 0 (0%) |
| Wound infection | 0 (0%) | 0 (0%) |
| Recurrent inguinal hernia | 0 (0%) | 0 (0%) |
| Successful mesh fixation | 10 (100%) | 10 (100%) |
| Successful peritoneum closure | 10 (100%) | 10 (100%) |
The average operative time was 45 minutes in Group I and 51 minutes in Group II. During the 30-day follow-up period, no recurrent hernias, wound infections, or hematomas were observed in either group. Both mesh fixation and peritoneal closure were successfully achieved in all cases across both groups.
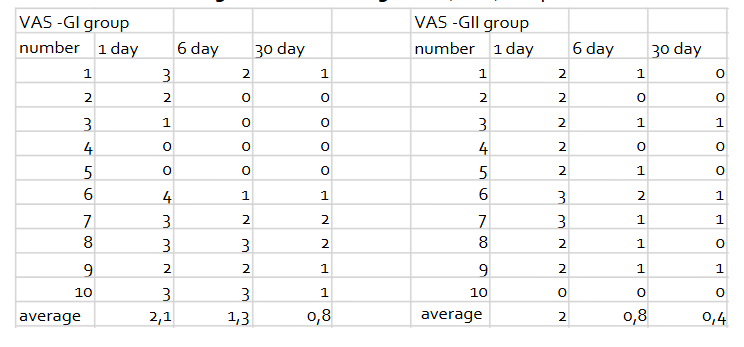
Postoperative pain scores measured using the visual analog scale (VAS) are presented in Table 2.
| Time point | Group I (Tacks) | Group II (Adhesive) |
|---|---|---|
| Day 1 | 2.1 | 2.0 |
| Day 6 | 1.3 | 0.8 |
| Day 30 | 0.8 | 0.4 |
A two-factor analysis of variance showed no statistically significant difference between the two groups overall (p=0.1732). However, the difference between time points within groups was statistically significant (p<0.0001), indicating significant pain reduction over time in both groups.
Analysis of Variance
| Source | Sum of Squares | Df | Mean Square | F-Ratio | P-Value |
|---|---|---|---|---|---|
| MAIN EFFECTS | 1.66667 | 1 | 1.66667 | 1.90 | 0.1732 |
| B:days | 22.0333 | 2 | 11.0167 | 12.58 | 0.0000 |
| RESIDUAL | 49.0333 | 56 | 0.875595 | ||
| TOTAL (CORRECTED) | 72.7333 | 59 |
For Group I, a single-factor analysis of variance showed that the difference between the three time points was not statistically significant (p>0.05). However, the multiple range test (LSD) indicated that the difference between day 1 and day 30 in Group I was statistically significant.
For Group II, a single-factor analysis of variance demonstrated that the difference between the three time points was statistically significant (p<0.0001, F-ratio 15.6). The difference between day 1 and day 6, as well as between day 1 and day 30, was statistically significant. The difference between day 6 and day 30 was not statistically significant. The Mood Median test confirmed that the difference between all three time points in Group II was statistically significant (p<0.0001).
Multiple range tests comparing all six samples (three time points for each of the two groups) showed that of fifteen possible comparisons, the difference was statistically significant in seven comparisons and not significant in eight comparisons. Notably, the pain intensity in Group I at day 30 was equivalent to the pain intensity in Group II at day 6, indicating that patients treated with adhesive achieved pain relief significantly faster than those treated with tacks.
| Method: 95.0 percent LSD | Count | Mean | Homogeneous Groups |
|---|---|---|---|
| GII 30 day | 10 | 0.4 | X |
| GI 30 day | 10 | 0.8 | XX |
| GII 6 day | 10 | 0.8 | XX |
| GI 6 day | 10 | 1.3 | XX |
| GII 1 day | 10 | 2.0 | X |
| GI 1 day | 10 | 2.1 | X |
Contrast Sig. Difference +/- Limits
GI 1day-GI 6 day 0.8 0.8506
GI 1 day – GI 30 day * 1.3 0.8506
GI 1 day – GII 1day 0.1 0.8506
GI 1 day – GII 6 day * 1.3 0.8506
GI 1 day – GII 30day * 1.7 0.8506
GI 6 day – GI 30 day 0.5 0.8506
DISCUSSION
The choice of fixation method during laparoscopic inguinal hernia repair represents a key technical decision with significant implications for patient outcomes. Current evidence suggests that penetrating fixation agents for mesh in hernioplasty should be used judiciously, if at all, to avoid potential nerve injury, vascular damage, and intra-abdominal adhesions. This recommendation is reflected in the IEHS guidelines, which suggest that fibrin glue should be the preferred method for mesh fixation in TAPP hernioplasty.
N-butyl-2-cyanoacrylate (NBCA) offers several advantages over fibrin glue, including stronger mesh fixation, the ability to effectively seal peritoneal flaps, and potential utility for skin incision closure. The primary disadvantage of NBCA is that it is not bioresorbable. However, our experience demonstrated excellent technical success with NBCA, achieving complete mesh fixation and peritoneal closure in all cases, with no incidence of hernia recurrence, wound infection, or hematoma formation during the 30-day follow-up period.
The mechanisms underlying the efficacy of tissue adhesives in surgical applications are multifaceted. These agents elicit a minimal inflammatory response while simultaneously improving wound healing and exerting bacteriostatic effects. These properties contribute to both the technical success and favorable safety profile observed with adhesive fixation techniques.
A significant finding in our study was the accelerated reduction in postoperative pain in patients treated with adhesive fixation compared to those treated with tacks. Our analysis demonstrated that patients undergoing TAPP repair with adhesive fixation achieved by postoperative day 6 the same level of pain relief that patients with tack fixation experienced at postoperative day 30. This represents a significant advantage in terms of recovery trajectory.
Pain reduction is a critical determinant of convalescence duration following inguinal hernia repair. The faster pain reduction observed with adhesive fixation techniques may translate to earlier return to normal activities and work, addressing an important socioeconomic aspect of hernia surgery. Considering that inguinal hernioplasty represents one of the most commonly performed general surgical procedures worldwide, improvements in recovery times and reductions in chronic postoperative pain carry substantial public health implications.
The excellent results in reducing chronic postoperative pain and the low recurrence rates associated with NBCA adhesive fixation have contributed to its increasing adoption in clinical practice, reflected in the growing body of literature on this topic. Our findings align with this trend, supporting the use of NBCA as an effective alternative to traditional fixation methods.
Peritoneal closure represents another critical technical aspect of TAPP repair, as inadequate closure may lead to complications such as early postoperative ileus. Our study demonstrated that peritoneal closure using NBCA is a safe and reliable method, achieving successful closure in 100% of cases. This is consistent with previous research showing that NBCA can provide durable peritoneal closure without serious complications at 12-month follow-up. However, it should be noted that while Dauser and colleagues achieved peritoneal adhesion using LiquiBandFIX8 adhesive in 90% of cases, we achieved closure in all cases in our series.
The success of peritoneal closure with adhesive may be influenced by anatomical considerations, with certain conditions potentially limiting its effectiveness (such as adhesions of the sigmoid colon with strong traction to the distal peritoneal flap). Based on the current evidence, there are no recommendations for the exclusive use of NBCA for peritoneal closure, but our results suggest it is a viable and effective option in appropriately selected patients.
CONCLUSION
The n-butyl-2-cyanoacrylate adhesive represents an excellent method for both mesh fixation and peritoneal closure in TAPP inguinal hernia repair. The technique is simple, safe, and readily implementable in clinical practice. Most importantly, adhesive fixation techniques offer superior results compared to tissue-perforating fixation methods in terms of prevention and reduction of postoperative pain. The significantly faster pain reduction observed with adhesive fixation may translate to shorter convalescence periods and improved quality of life for patients undergoing laparoscopic inguinal hernia repair.
Conflict of Interest:
None.
Funding Statement:
None.
Acknowledgements:
None.
REFERENCES
- Matthews RD, Neumayer L. Inguinal hernia in the 21st century: an evidence-based review. Curr Probl Surg. 2008;45:261-312.
- Primatesta P, Goldacre MJ. Inguinal hernia repair: incidence of elective and emergency surgery, readmission and mortality. Int J Epidemiol. 1996;25:835-9.
- Fortelny RH, Petter-Puchner AH, Glaser KS, et al. Use of fibrin sealant (Tisseel/Tissucol) in hernia repair: a systematic review. Surg Endosc. 2012;26:1803-12.
- Petter-Puchner AH, Brunner W, Gruber-Blum S, et al. A systematic review of hernia surgery in SIL (single-incision laparoscopy) technique. Eur Surg. 2014;46:113-4.
- Fischer S, Zechmeister-Koss I. Is day surgery safe? A systematic literature review. Eur Surg. 2014;46:103-12.
- Katkhouda N, Mavor E, Friedlander MH, et al. Use of fibrin sealant for prosthetic mesh fixation in laparoscopic extraperitoneal inguinal hernia repair. Ann Surg. 2001;233:18-25.
- Sajid MS, Ladwa N, Kalra L, et al. A meta-analysis examining the use of tacker fixation versus no-fixation of mesh in laparoscopic inguinal hernia repair. Int J Surg. 2012;10:224-31.
- Bittner R, Montgomery MA, Arregui ME, et al. Update of guidelines on laparoscopic (TAPP) and endoscopic (TEP) treatment of inguinal hernia (International Endohernia Society). Surg Endosc. 2015;29:289-321.
- Fortelny RH, Petter-Puchner AH, Walder N, et al. Cyanoacrylate tissue sealant impairs tissue integration of macroporous mesh in experimental hernia repair. Surg Endosc. 2007;21:1781-5.
- Fortelny RH, Petter-Puchner AH, May C, et al. The impact of atraumatic fibrin sealant vs. staple mesh fixation in TAPP hernia repair on chronic pain and quality of life: Results of a randomized controlled study. Surg Endosc. 2012;26:249-54.
- Kukleta JF, Freytag C, Weber M, et al. Efficiency and safety of mesh fixation in laparoscopic inguinal hernia repair using n-butyl-cyanoacrylate: long-term biocompatibility in over 1300 mesh fixations. Hernia. 2012;16:153-62.
- Dauser B, Szyszkowitz A, Seitinger G, et al. A novel glue device for fixation of mesh and peritoneal closure during laparoscopic inguinal hernia repair: short and medium-term results. Eur Surg. 2017;49:27-31.
- Lee MGM, Jones D. Applications of fibrin sealant in surgery. Surg Innov. 2005;12:203-13.
- Ryou M, Thompson CC. Tissue adhesives: a review. Tech Gastrointest Endosc. 2006;8:33-7.
- ASGE Technology Committee, Bhat YM, Banerjee S, et al. Tissue adhesives: cyanoacrylate glue and fibrin sealant. Gastrointest Endosc. 2013;78:209-15.
- Bay-Nielsen M, Thomsen H, Andersen FH, et al. Convalescence after inguinal herniorrhaphy. Br J Surg. 2004;91:362-7.
- Callesen T, Klarskov B, Bech K, Kehlet H. Short convalescence after inguinal herniorrhaphy with standardized recommendations: duration and reasons for delayed return to work. Eur J Surg. 1999;165:236-41.
- Kehlet H, Jensen TS, Woolf CJ. Persistent postsurgical pain: risk factors and prevention. Lancet. 2006;367:1618-25.
- McCormack K, Wake B, Perez J, et al. Laparoscopic surgery for inguinal hernia repair: systematic review of effectiveness and economic evaluation. Health Technol Assess. 2005;9:1-203.
- Helvind NM, Andersen K, Rosenberg J. Lower reoperation rates with the use of fibrin sealant versus tacks for mesh fixation. Surg Endosc. 2013;27:4184-91.
- Matthews RD, Neumayer L. Inguinal hernia in the 21st century: an evidence-based review. Curr Probl Surg. 2008;45:261-312.