





Detection and Elimination of Air Embolism in Cardiac Surgery
Detection and elimination of potentially pathologic air embolization in cardiac surgery with the use of multi-modal neuromonitoring: a case report
Introduction
Neurological complications associated with cardiac surgeries can be devastating and life altering to patients. Injuries can range from mild postoperative delirium to more severe complications such as focal neurological deficits, seizures, strokes, and catastrophic brain damage¹.¹ Below adverse cerebral outcomes after surgery result in longer hospitalization, prolonged time in the intensive care unit, higher rates of discharge to facilities, and increased in-hospital mortality². Mechanisms of injury include prolonged hypoperfusion, embolism, inflammation, and improper patient positioning and padding. Rates of neurological injury during isolated cardiac surgery have been reported at between 2-3%, with thoracic aortic surgery having higher rates reported at closer to 10%.²˒³ Multimodal, intraoperative neuromonitoring provides a range of information to the cardiac surgery team that would otherwise be unavailable. Within our armamentarium of multimodal monitoring, we have for example, somatosensory evoked potentials (SSEP), which affords us the ability to assess peripheral nerve function in real time. This is useful in cardiac cases as well as complex thoracic and abdominal aortic cases as it is a direct measurement of spinal cord protection, an often cause of neurological injury. Implementation of multimodal, neuromonitoring strategies can potentially identify neurologic insults in real time that would otherwise be missed resulting in lower-than-expected rates of adverse neurological outcomes⁴˒⁵˒⁶. Early identification of potential injury may allow for intraoperative surgical or perfusionist adjustments to minimize the risk of permanent neurologic deficits.
In this article we report an example of the application of multiple intraoperative neuromonitoring modalities that we use during complex cardiac surgery procedures. We were able to catch extensive air emboli early, employ the appropriate intervention and thereby most likely prevented neurological injury.
Case Report:
HISTORY
A 77-year-old male with a history of Barrett’s esophagus, recurrent pericarditis, and a 4.5 cm ascending aortic aneurysm presented to the hospital with acute chest pain. He was found to have a non-ST elevation myocardial infarction (NSTEMI) and was taken for catheterization of the left heart. Coronary angiogram identified three vessel disease involving the left anterior descending artery (LAD), the first branch obtuse marginal branch (OM1), and the posterior descending artery (PDA). The patient was discussed at our multi-disciplinary cardiac team conference. As a group, we felt that 3 vessel bypass, radical pericardiectomy and an ascending aortic replacement would be too much of a physiologic insult. Thereby, we sought to mitigate the risk of surgery, by decreasing both the cardiopulmonary bypass and aortic cross clamp time by having a hybrid approach to his revascularization and performing the pericardiectomy prior to going on pump. The lesions on OM1 and PDA were short, focal, and amendable to percutaneous intervention. The patient would have surgical revascularization of the LAD with a LIMA and coronary stent to the OM1 and PDA branches post-operatively. At the time of surgery, we would perform a radical pericardiectomy and an ascending aortic replacement.
NEUROMONITORING
Multimodality intraoperative neuromonitoring relied on 8 channel electroencephalogram (EEG), bilateral ulnar and posterior tibial somatosensory evoked potentials (SSEP) and brainstem auditory evoked potentials (BAEP) (Cadwell laboratories, Cascade Pro), two channel transcranial Doppler (TCD) ultrasonography (Compumedics DWL Doppler BoxX system), and two channel frontal cerebral oximetry INVOS 5100A near-infrared spectroscopy (Medtronic INVOS). EEG was obtained with gold cup reusable electrodes in the International 10-20 System configuration. SSEPs were recorded to stimulation of the left and right ulnar and posterior tibial nerves. BAEPs were recorded to stimulation of the bilateral auditory click stimuli. Cerebral hemodynamics and the presence of emboli were monitored by recording the left and right middle cerebral artery flow velocity spectra continuously by transtemporal insonation with 2-MHz probe to a depth of 50mm. For near-infrared spectroscopy, a self-adhesive patch containing infra-red source, and 2 detectors was applied to the forehead to measure rCVOS (Image 1).
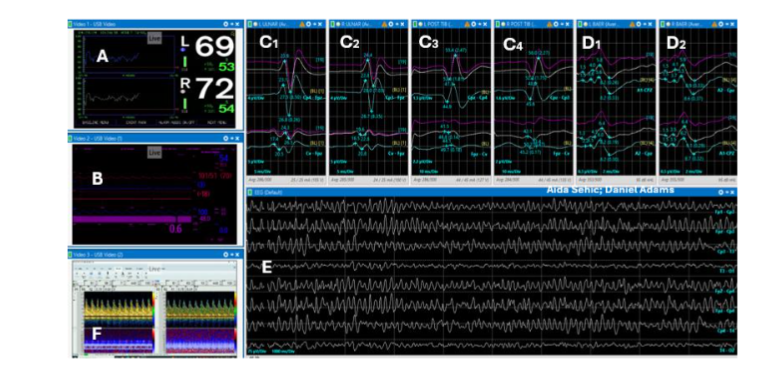
Image 1. Illustrates pre-incision normal baselines. (A) Two channel near infrared spectroscopy (NIRS), (B) video imported from anesthesia monitor vital sign values: blood pressure, heart rate, respiratory rate, CVP, expired CO2, body temperature, inhalation anesthetic gas %. (C1) left upper SSEP, (C2) right upper SSEP, (C3) left lower SSEP, (C4) right lower SSEP, (D1) left BAEP, (D2) right BAEP, (E) eight channel EEG, (F) two channel TCD pulsatile flow velocities for left and right middle cerebral arteries.
SURGERY
General anesthesia was induced with Thiopental and was maintained with Isoflurane and low dose of Propofol. Neuromuscular blockade was obtained with a bolus dose of pancuronium of 0.1 mg/kg. Standard anesthetic monitoring consisted of expired anesthetic gas concentration, arterial blood pressure, capnometry, inspired oxygen concentration, heart rate, nasopharyngeal temperature and electrocardiography.
The chest was opened via a median sternotomy. A Rultract® Skyhook Retractor was then used to harvest the left internal mammary artery as a thin pedicle. The pericardium was noted to be completely adherent to the heart. We therefore proceeded to dissect the parietal pericardium off the heart without the use of cardiopulmonary bypass. We first freed the left ventricle in entirety. Once that was completed, we proceeded to dissecting the pericardium off the right ventricle, right atrium and vena cavae. A radical pericardiectomy was then performed. We excised the pericardium from phrenic nerve to phrenic nerve laterally, involving the thymus superiorly and diaphragm inferiorly. We then took great care to dissect the epicardial surface of the heart, again starting with the left side before going to the right side.
The patient was noted to have a fusiform aneurysm of the ascending aorta, above the sinotubular junction to about 2 cm proximal to the base of the innominate artery. I proceeded to dissect the aortic arch. I then used the Seldinger technique and trans esophageal echocardiogram guidance, to cannulate a 20 Fr cannula in zone 1 of the aortic arch (between the innominate and left carotid arteries). The right atrium was then cannulated for venous drainage. Cardiopulmonary bypass was initiated. Thereafter, an antegrade cardioplegia cannula was then placed above the aortic root followed by a retrograde cardioplegia cannula into the coronary sinus of the right atrium. Shortly after placing the retrograde cardioplegia cannula the sudden appearance of emboli, high-intensity transient ultrasonic signals was noted on transcranial doppler concerning bilaterally for bubble detection (Image 2).
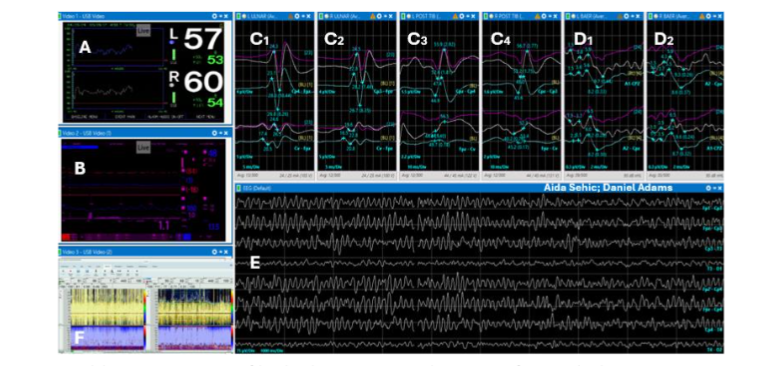
Image 2. Illustrates sudden appearance of high ultrasonic signals (HITS) of air emboli on (F) TCD. Non-pulsatile signal typical for bypass after aortic cross clamp application seen bilaterally on middle cerebral arteries. Other neuromonitoring modalities remain unchanged: (A) NIRS, (B) Vital signs, (C1,2,3,4) SSEPs, (D1,2) BAEP and (E) EEG.
We confirmed with an intra-operative, trans esophageal echocardiogram the presence of large air emboli in the left atrium and ventricle, going into the aortic root. We first checked the aortic cannula as well as the antegrade cardioplegia cannula to ensure that their connections were tight, and that air was not coming from the pump. We were assured that they were not the source of the air emboli. We proceeded with de-airing maneuvers by placing the patient in a Trendelenburg position while turning on the aortic root vent on high suction. I first placed an aortic cross clamp and began to administer cardioplegia in the antegrade fashion to arrest the heart. We noticed that emboli to the brain persisted bilaterally in the left and right middle cerebral arteries in addition to air in the left atrium. I then checked the connection to the retrograde cannula and noticed that connection was not tight. Moreover, even though I had no reason to believe that there was an anatomical anomaly to create a right to left shunt, I still decided to remove the retrograde cardioplegia cannula. This led to immediate resolution of the air emboli to the brain (Image 3).
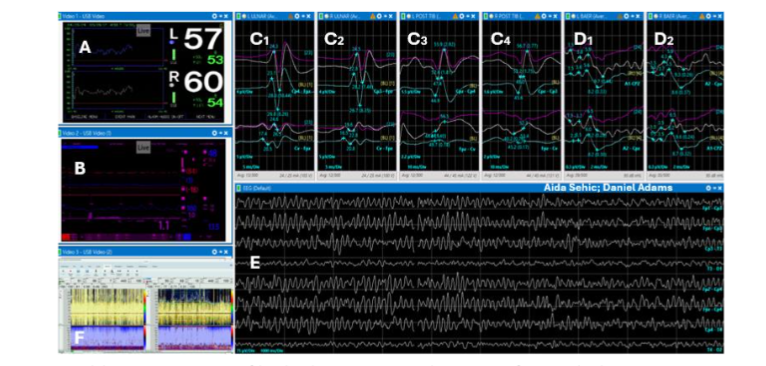
Image 3. Illustrates alert resolution: (F) TCD signal free of air emboli after surgical intervention of removal of retrograde cardioplegia cannula as timely surgical intervention and elimination of air emboli were performed. Other neuromonitoring modalities remain unchanged: (A) NIRS, (B) Vital signs, (C1,2,3,4) SSEPs, (D1,2) BAEP and (E) EEG.
I realized that in placing the aortic cross clamp in haste, it had not completely occluded the aorta, and the heart was still pumping. I re-positioned the aortic cross clamp at the base of the innominate artery. The heart was arrested using Del Nido cardioplegia in the antegrade fashion. At that point, the patient had return of normal parameters on the TCD recordings while all other neuromonitoring modalities were unchanged. This remained to be the case through the end of the case (Image 4).
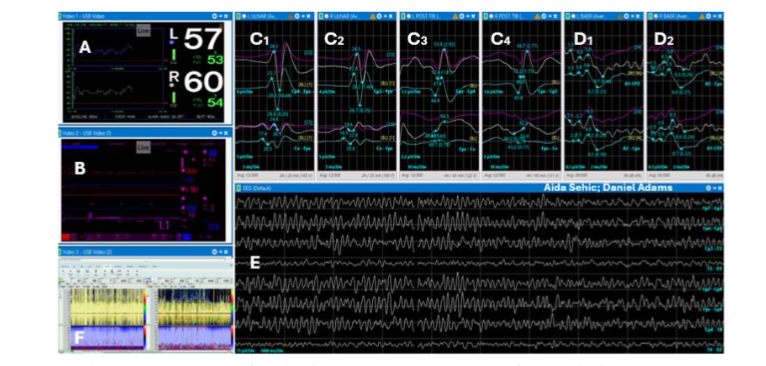
Image 4. Illustrates normal closing signals, same as pre-incision baseline signals. (A) NIRS, (B) Vital signs, (C1,2,3,4) SSEPs, (D1,2) BAEP and (E) EEG. (F) TCD signal becomes pulsatile off bypass and remains free of air emboli.
The LIMA to LAD anastomosis was then performed. Afterwards, attention was turned to the fusiform aneurysm of the ascending aorta. The aorta was resected from the Sino tubular junction to 1cm proximal of the aortic cross clamp. A 30mm gel-weave interposition graft was then sutured in to place first distally and then proximally to complete the aortic reconstruction. The heart was deaired and the patient was taken off bypass. At the completion of neuromonitoring the EEG, evoked potentials, cerebral blood flow velocity, and oxygenation were noted to retain their pre-incision characteristics. Surgical drains were placed, the chest was closed in the standard fashion, and the patient was taken to the ICU intubated. As sedation was weaned in the ICU the patient was noted to be able to follow commands without difficulty. He was extubated later that evening and was noted to have no neurological deficits. The patient was discharged home on post-operative day six. He had successful percutaneous coronary intervention to his PDA and OM1 6 weeks later.
Discussion:
Neurological injury after cardiac surgery is a significant cause of morbidity and mortality. According to a systematic review by Gaudino et al³, pooled rates of operative mortality after perioperative stroke can be as high as 21.3%, compared to only 2.4% in patients without stroke. Multimodal neurocognitive monitoring aims to minimize rates of postoperative cognitive decline and postoperative stroke that may be missed or misdiagnosed by limitations of single modality monitoring.
EEG or NIRS or less frequently TCD are commonly used for single modality neuromonitoring techniques. One of the major benefits of TCD is the high sensitivity for detecting both macro and micro-embolism and the ability to detect reduction of flow velocity⁷. There is some concern that in isolation, TCD may identify many non-physiologically significant micro embolic events⁸˒⁹. This in turn could result in hemodynamic or surgical alterations that would not be beneficial to the patient and could expose the patient to unnecessary risk. NIRS monitors cerebral oxygenation can help identify global desaturation or incorrect cannula positioning. Decreased oxygenation values in NIRS can be due to hypoperfusion secondary to low flow state or due to embolization¹⁰. Without additional information, the decreased oxygenation values noted on isolated NIRS may encourage the perfusionist to increase flows. This could be harmful if the case of decreased oxygenation is in-fact due to embolization phenomena. It is hypothesized that this may be one of reasons why isolated NIRS has not been shown in systematic review to prevent strokes¹⁰. TCD or NIRS alone may drastically underestimate neurological events. Our institution previously showed that multimodal neuromonitoring can help identify events in adults that isolated TCD would have a false negative rate of 55% and isolated NIRS would have had a false negative rate of 43%¹¹.
Zanatta et. al⁶ showed significant benefit of neurophysiological multimodal monitoring with zero major neurological outcomes in the multimodal group of 166 patients, compared to a rate of 4.06% in the control group of 1,555. Multimodal monitoring included EEG, SSEP, TCD, jugular bulb oxygen saturation. Interestingly, 91% of patients who underwent multimodal monitoring had at least one intraoperative event with 83% of patients having isolated micro embolic signals. An additional benefit of neuromonitoring may be in decreasing the amount of postoperative delirium. In a small sample of 82 patients, Kunst et al.¹² showed that anesthetic adjustments based off BIS and NIRS monitoring resulted in significantly less post-operative delirium 2.4% vs. 20% (p=0.01).
In our case, the patient’s NIRS were stable while there was active air embolization taking place. The use of single modality monitoring would have missed this event and we would have continued with the surgery, all while unknowingly, causing potential damming neurological insult to the patient. The patient had several, pre-operative, cardiac specific studies that did not show any anatomical anomalies that would have caused us to suspect that air emboli to the left side would occur from placement of a retrograde cardioplegia cannula through the coronary sinus. He had a cardiac MRI seven months before the surgery, multiple surveillance chest cat scan angiograms for his ascending aortic aneurysm, pre-operative trans thoracic echocardiogram as well an intra-operative echocardiogram. It is likely that he either had small fenestrated unroofed coronary sinus or possibly an iatrogenic injury to the roof of coronary sinus at the time of the placement of the retrograde cannula. The fact that we had not fully excluded the heart with our cross clamp, the heart was continuously being perfused, thus continued to beat and pushing air out of the left ventricle towards the brain. While we are not certain of the exact anatomical reason for why we had a right to left shunt leading to this air entrainment, it is most certain that neurological insult was averted through early detection and timely intervention to mitigate the further emboli.
Previous arguments against neurophysiological monitoring have suggested there is limited utility to identify these alarms, as they cannot be modified intraoperatively. From our own institution, we reviewed 365 alarms in 115 surgeries. We found that 26% of the causes for the alarms were able to be resolved within two attempts of adjustment by either the surgeon, perfusionist, or anesthesiologist¹³. Demonds noted previously that during coronary artery bypass grafting (CABG), an alarm event was noted in 58% of cases and all but 2% were able to be eliminated with adjustments¹⁴. Yet et al.¹⁴ previously reported a case of clinically significant air embolism on multimodal neuromonitoring which resolved after deep Trendelenburg, rapid cooling, brief circulatory arrest, and initiation of retrograde cerebral perfusion for gas evacuation from the aortic vent with no neurological deficits. In a small case series of six patients undergoing aortic arch repair for aortic dissection with multimodal monitoring, three patients (50%) underwent changes to cardiopulmonary bypass flow or cannula positioning based on monitoring¹⁵. Two out of three patients were able to have significant improvement noted on monitoring with adjustments. One of these patients went on to have full recovery without neurological deficit and the other did not survive surgery given the severity of his dissection. In the paper by Zanatta et al.⁶ they discuss the different strategies used to correct or adjust multimodal findings, showing that most of the findings have a potential intervention. Interestingly, after intervention they noted a reversible change in SSEP signals in 3% of the multimodal monitored patients. This rate approximates the 4% rate of major neurologic complications seen in the unmonitored group.
Conclusion:
Using multimodal neurophysiologic monitoring, we were able to identify a concern for an embolic event and make operative changes resulting in good neurologic outcome with resolution of the alarm. Rapid detection of parameter changes on multimodal neurophysiological monitoring allows for more accurate identification of neurological events than single modality neuromonitoring. Posterior tibial somatosensory evoked potentials (SSEP) have a growing role and should likely be included in multimodal intraoperative monitoring. Further randomized control trials are needed to support the ideal multimodal monitoring strategy in cardiac surgery.
Conflict of Interest:
None
Funding Statement:
None.
Acknowledgements:
None.
References
1. Milne B, Gilbey T, Gautel L, Kunst G. Neuromonitoring and Neurocognitive Outcomes in Cardiac Surgery: A Narrative Review. J Cardiothorac Vasc Anesth. 2022 Jul;36(7):2098-2113.
2. Roach GW, Kanchuger M, Mangano CM, Newman M, Nussmeier N, Wolman R, Aggarwal A, Marschall K, Graham SH, Ley C. Adverse cerebral outcomes after coronary bypass surgery. Multicenter Study of Perioperative Ischemia Research Group and the Ischemia Research and Education Foundation Investigators. N Engl J Med. 1996 Dec 19;335(25):1857-63.
3. Gaudino M, Rahouma M, Di Mauro M, Yanagawa B, Abouarab A, Demetres M, Di Franco A, Arisha MJ, Ibrahim DA, Baudo M, Girardi LN, Fremes S. Early Versus Delayed Stroke After Cardiac Surgery: A Systematic Review and Meta-Analysis. J Am Heart Assoc. 2019 Jul 2;8(13).
4. Austin EH 3rd, Edmonds HL Jr, Auden SM, Seremet V, Niznik G, Sehic A, Sowell MK, Cheppo CD, Corlett KM. Benefit of neurophysiologic monitoring for pediatric cardiac surgery. J Thorac Cardiovasc Surg. 1997 Nov;114(5):707-15, 717; discussion 715-6.
5. Edmonds HL Jr. Protective effect of neuromonitoring during cardiac surgery. Ann N Y Acad Sci. 2005 Aug; 1053:12-9.
6. Zanatta P, Messerotti Benvenuti S, Bosco E, Baldanzi F, Palomba D, Valfrè C. Multimodal brain monitoring reduces major neurologic complications in cardiac surgery. J Cardiothorac Vasc Anesth. 2011 Dec;25(6):1076-85.
7. Edmonds H.L, Monitoring of cerebral Perfusion with Transcranial Doppler Ultrasound Intraoperative Monitoring of Neural Function, handbook of Clinical Neurophysiology, Vol. 8 M.R. Nuwer (Ed.) Elsevier B.V. Chapter 67, 2008; 959-974.
8. Kruis RW, Vlasveld FA, Van Dijk D. The (un)importance of cerebral microemboli. Semin Cardiothorac Vasc Anesth. 2010 Jun;14(2):111-8.
9. Patel N, Minhas JS, Chung EM. Intraoperative Embolization and Cognitive Decline After Cardiac Surgery: A Systematic Review. Semin Cardiothorac Vasc Anesth. 2016 Sep;20(3):225-31.
10. Serraino GF, Murphy GJ. Effects of cerebral near-infrared spectroscopy on the outcome of patients undergoing cardiac surgery: a systematic review of randomised trials. BMJ Open. 2017 Sep 7;7(9).
11. Yeh T, Millan D, Calaritis C, Miller J, Adams D, Sehic A, EEG-based Neuromonitoring Improves Identification Of Neural Threats During Cardiac Surgery, Congenital Heart Surgeons Society, CHSS Meeting, Chicago IL, 2021.
12. Kunst G, Gauge N, Salaunkey K, Spazzapan M, Amoako D, Ferreira N, Green DW, Ballard C. Intraoperative Optimization of Both Depth of Anesthesia and Cerebral Oxygenation in Elderly Patients Undergoing Coronary Artery Bypass Graft Surgery-A Randomized Controlled Pilot Trial. J Cardiothorac Vasc Anesth. 2020 May;34(5):1172-1181.
13. Yeh T, Millan D, Calaritis C, Miller J, Adams D, Sehic A, A Coordinated Team Can Extinguish 95% Of Neural Threats Identified By EEG-Based Multimodality Neuromonitoring In Cardiac Surgery. Congenital Heart Surgeons Society, CHSS Meeting, Chicago IL, 2022.
14. Yeh T Jr, Austin EH 3rd, Sehic A, Edmonds HL Jr. Rapid recognition and treatment of cerebral air embolism: the role of neuromonitoring. J Thorac Cardiovasc Surg. 2003 Aug;126(2):589-91.
15. Thudium M, Heinze I, Ellerkmann RK, Hilbert T. Cerebral Function and Perfusion during Cardiopulmonary Bypass: A Plea for a Multimodal Monitoring Approach. Heart Surg Forum. 2018 Jan 31;21(1):E028-E035. doi: 10.1532/hsf.1894. PMID: 29485961.