

Digital Behavioral Health in Low-Income Communities
Implementing a Digital Child Behavioral Health Prevention Program in Faith-Based Settings in Uganda: A Feasibility Study
Keng-Yen Tsai, Elizabeth Nnanna Kusiak, Hafsa Sentongo, Antoinette Schonfeld, Omar El-Shahawy, Devin Mann
Abstract
Background: The rapid advancement of digital health and evidence-based intervention options, along with the high burden of disease in low-and-middle income countries (LMICs), necessitates innovative approaches to behavioral health interventions.
Objective: To test the feasibility of the SBIRT model in Faith-Based Organizations (FBOs) in SSA families’ religious and cultural contexts.
Methods: We developed a digital toolkit to implement a technology-supported population approach of child mental health promotion in community settings.
Results: The findings demonstrated feasibility and acceptability of the P-BHDT program.
Conclusion: The P-BHDT program has the potential to improve child mental health in LMICs.
Keywords: Digital health, behavioral health, feasibility study, Faith-Based Organizations, child mental health
Introduction
Child mental health is critical to the overall well-being of children and their families. The burden of disease among children, particularly in low-and-middle income countries (LMICs), is significant due to high poverty, violence, health problems, and poor health care systems. Low-cost preventive solutions for reducing burden for LMICs in communities is urgently needed. To address the preventive service and evidence-based intervention gaps, we aimed to implement a technology-supported population approach of child mental health promotion in community settings.
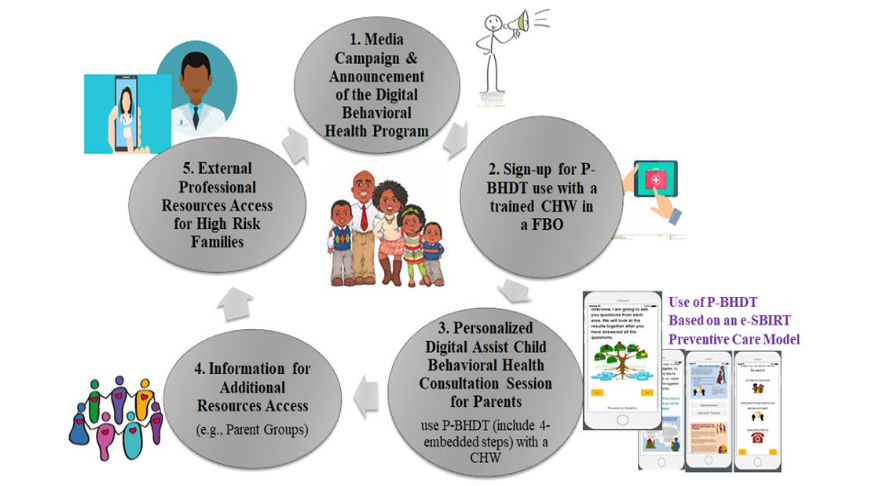
Pediatric Digital Behavioral Health Tool (P-BHDT) Intervention
FBOs in SSA families’ religious and cultural settings. Given that FBO is the center of SSA families’ social and cultural life, we aimed to leverage the existing community structures to deliver the P-BHDT and to identify the SBIRT intervention model.
Methods
The study was initiated on October 10, right before the pandemic. The original trial design and evaluation timeline. To provide a brief overview of the original design here, the study was randomized to control, with CHWs trained to implement P-BHDT program to families with children aged 3-8 years old.
Participants and Procedures
The FBOs were selected based on recommendation from our research staff and Advisory Board members. The FBO leaders who were interested in having their FBO participate in the study were enrolled. Six FBOs (or 3 match-paired similar in size and location with each pair) were recruited. Within each pair, we randomly assigned one to intervention and one to wait-list control.
Results
Table 1 summarizes the demographic characteristics of our recruited FBOs, CHWs, and families.
| FBO | Mean (SD) | Mean (CI) % | Control | p |
|---|---|---|---|---|
| Average # of congregation members | 120.00 (18.12) | 72.6% (289.91) | 0.854 | |
| Age | 0 | 0 | 0 |
Discussion
This study is the first to test the feasibility of the P-BHDT program in the community context. We found that intervention parents significantly improved in their mindfulness parenting and perceived effectiveness in discipline/child-parent relationship.
Conclusion
From October 2019 until November 2021, during the course of this study, Ugandan families faced significant challenges due to prolonged COVID-19 lockdowns, school closures, and economic hardship. Our findings in this context suggest that the P-BHDT program has the potential to improve child mental health in LMICs.
Conflict of Interest
The authors declare that they have no competing interests.
Funding
The National Institutes of Health (R21MH116692) funded this study.
Ethical Approval
The ethics related to this study was approved by the Institutional Review Boards of New York University School of Medicine (IRB No. i18-00728) and Makerere University (IRB No. 594).
References
1. Murray CJL, Vos T, Lozano R, Naghavi M, Flaxman AD, Michaud C. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990-2010: a systematic analysis for the Global Burden of Disease Study. Lancet. 2012;380:2197-223.
2. Omar MA, Green AT, Bird PK, et al. Mental health policy process: a comparative study of Ghana, South Africa, Uganda and Zambia. International journal of mental health systems. 2010;424. doi:10.1186/1752-4458-424.
3. Jamison DT. Disease and mortality in sub-Saharan Africa. 2006.
4. Sanyal R. Mental illness: evidence-based interventions in children and adolescents. 2010;4:1-4.