





Distraction Osteogenesis: Techniques and Implications in Orthodontics
Distraction Osteogenesis and It’s Orthodontic Implications: A Review
Dr. Sahil Kambale¹, Dr. Amit Handa², Dr. Nikita Bhagwan¹, Dr. Himanshu Srivastava³, Dr. Siddeek Saudagar¹, Dr. Aditi Sarda⁴*
- PG student, Department of Orthodontics and Dentofacial Orthopaedics, Aditya Dental College & Hospital, Beed, Maharashtra, India.
- Professor, Department of Orthodontics and Dentofacial Orthopaedics, Aditya Dental College & Hospital, Beed, Maharashtra, India.
- Associate Professor, Department of Oral & Maxillofacial Pathology and Microbiology, Aditya Dental College & Hospital, Beed, Maharashtra, India.
- Associate Professor, Department of Conservative Dentistry and Endodontics, Aditya Dental College & Hospital, Beed, Maharashtra, India.
OPEN ACCESS
PUBLISHED: 31 October 2024
CITATION: Kambale, S., Handa, A., et al., 2024. TITLE HERE. Medical Research Archives, [online] 12(10). https://doi.org/10.18103/mra.v12i10.5601
DOI https://doi.org/10.18103/mra.v12i10.5601
ISSN 2375-1924
ABSTRACT
Distraction osteogenesis is used synonymously with “Osteo-distraction”, “Trans osseous synthesis” or “bone lengthening”. With the advent of newer techniques in field of orthodontics and oral and maxillofacial surgery, Distraction osteogenesis is ever evolving entity. The methods and approaches used in craniofacial distraction are always changing. We now have a better grasp of the histological and biochemical reaction at the site of distraction. Distraction osteogenesis involves a different series of events from normal fracture healing, and a better understanding of these differences has allowed us to select patients who are good candidates for distraction osteogenesis. The availability of distractors in a variety of forms and styles has also been made easier by recent advancements in manufacturing techniques, which are currently altering the treatment of numerous craniofacial deformities. These days, patients are willing to endure the pangs essential for their perfect esthetics. Treatment outcomes have become more predictable due to innovative approaches to care, the simultaneous correction of several craniofacial abnormalities at many osteotomy sites, and improved surgical accuracy made possible by digital imaging. The purpose of this review article is to summarize distraction osteogenesis under various headings. Conclusion: Distraction Osteogenesis, opens a new plethora of treatment and outcomes. Although the need for conventional mandibular and maxillary osteotomies will always persist, distraction osteogenesis tends to pave way for newer treatment approach for craniofacial abnormalities for orthodontist and oral surgeons as well.
Keywords:
Distraction osteogenesis, Orthodontics, Osteodistraction, Bone lengthening, Treatment.
Introduction
Distraction Osteogenesis is described as “A biological process of formation of new bone between the surfaces of bone segments sequentially separated by incremental traction” by Samchukov M.L., Cherkashin A.N., and Cope J.B. Another definition was given by Aranson who stated, “Distraction Osteogenesis is defined as a gradual, dynamically induced, intramembranous process of ossification between two active bone surfaces that are temporarily separated by minimal energy techniques”. The term distraction osteogenesis is synonymous with “Trans osseous synthesis” or “Osteo-distraction” or in simpler term, “Bone lengthening”. Among the relatively common anomalies of the craniofacial complex are congenital micrognathia, facial asymmetry, and maxillomandibular hypoplasia.
In the past, osteotomies, acute orthopaedic motions, skeletal fixation, and/or inter-positional bone grafts have been used to treat these skeletal abnormalities in nongrowing patients. Recent methods have focused on controlling de novo bone development through osteo-conduction and/or osteo-induction in light of these constraints. Distraction osteogenesis, a callus distraction technique, is an alternate strategy. It involves the production of new bone between the surfaces of bone segments that are progressively separated by incremental force. Since the treatment outcomes have become more predictable due to innovative approaches to care, the simultaneous correction of several craniofacial abnormalities at many osteotomy sites along with improved surgical accuracy made possible by digital imaging.
Distraction osteogenesis has emerged as an effective treatment modality for the correction of bone anomalies and abnormalities which are either pathological or developmental in origin. Earlier it was predominantly used in orthopaedics for the correction of axial skeleton. Its use in the field of dentistry began in the late twentieth century. Successful results from the initial clinical trials prompted more and more researchers to explore this field. Its use in dentistry involves the correction of craniofacial anomalies, alveolar ridge for the prosthetic rehabilitation and recently for the regeneration of lost periodontium. The aim of this review article is to summarize distraction osteogenesis under various headings and its application as well as treatment outcomes in orthodontics and dentofacial orthopaedics. The credit for invention of this technique goes to Gavril Abramovich Illizarov, a Russian orthopaedic surgeon, who, in 1950 accidently discovered this technique. Guerrero first described mandibular symphysis Osteo-distraction in 1990, and other people have since utilized it infrequently. The timeline of significant events related to distraction osteogenesis have been highlighted in Table 1.
| Year | Surgeon | Advancement |
|---|---|---|
| 1798 | Pierre Fouchard | Used Dentofacial expansion and described ‘Bandalette’ |
| 1893 | Goddard | Standardized the palatal expansion protocol by a stabilization period after activation to allow deposition of ‘Osseous Material’ in the created gap |
| 1992 | McCarthy | Distraction osteogenesis for lengthening mandible that is congenitally hypoplastic |
| 1993 | Rachmiel & Blocks et al | Distraction of maxillary segment |
| 1995 | Polley et al | Distraction of midface with a cranial halo frame fixed externally |
| 1996 | Chin & Toth | Alveolar distraction in mandible to increase the alveolar height |
Sequential Periods in Distraction Osteogenesis
The phases of distraction osteogenesis are broadly categorized into 5 groups- Surgical phase, latency phase, distraction phase, consolidation phase and remodelling phase. Planning and initial orthodontics precedes these phases and careful monitoring is the last step of evaluation. Callotasis, a soft callus formation, facilitates the healing of fractures in a natural healing process. According to this theory, distraction osteogenesis entails manipulating the callus in the distraction chamber in order to extend it structurally before calcification takes place.
Getting started with distraction osteogenesis procedure is all about getting ready and organizing. Identifying the aberrant structure and its most likely cause is crucial for effective therapy. Distraction osteogenesis is utilized to make up for the overdevelopment of contralateral structures by correcting the underdevelopment linked to hypoplastic or missing structures. The process of determining which structures need to be addressed is essential to organizing the kind, course, and intensity of distraction. Combination of diagnostic techniques are used like photographs, OPG, lateral cephalograms along with 3D imaging CBCT and stereolithographic models.
Initial or pre-surgical orthodontics seeks to create an occlusion that will stabilize the occlusion and aid in skeletal distraction guidance.
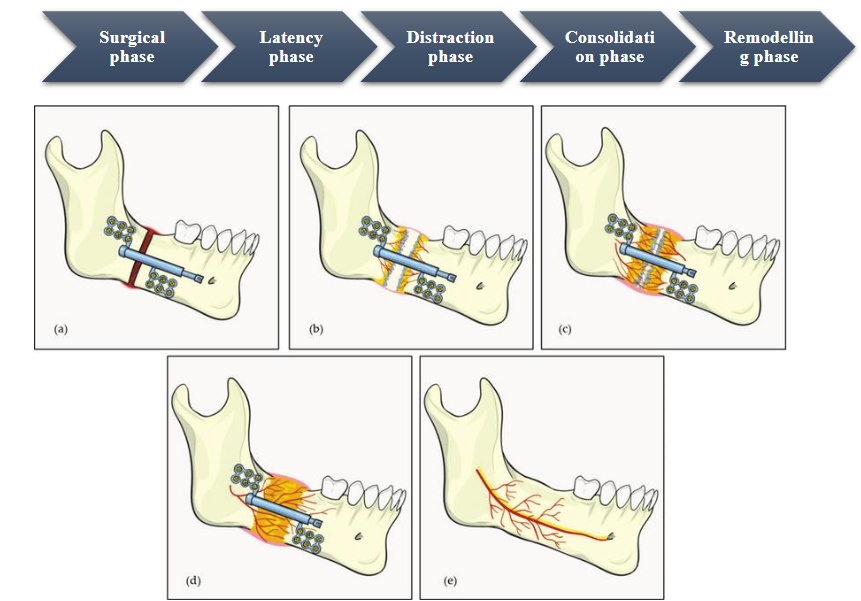
• Surgical phase- In order to separate the segments while maintaining the medulla and periosteum’s blood supply to the bone, a procedure known as a corticotomy involves performing an osteotomy to the cortical layer of the bone. The distraction rhythm in distraction osteogenesis indicates the frequency of the device activated each day, whereas the distraction rate reflects the daily displacement of the bone in millimetres (mm).
• Latency phase-It is the duration necessary for the development of callus. The duration of 5–7 days, as recommended by Ilizarov, is contingent upon the microvasculature and the physiological condition of bone development over the distraction site. Cellular hypoxia over the newly formed bone structure triggers an angiogenic response and mesenchymal cell migration, which aid in the manufacture of collagen. The latency period need to be sufficient for callus development and sufficiently lengthy to avoid calcification.
• Distraction phase-The stiff distraction device must be used in accordance with recommended protocol in order to achieve desired bone growth. By rotating an axial screw, which moves between 0.25 and 0.5 mm each turn (depending on the mechanism being utilized), the device is turned on. The soft callus may be stressed if the rate of distraction is too high, which could lead to thinning of all dimensions in the middle section of the regeneration and the formation of a “Hour Glass” at the distraction point. This has to distraction osteogenesis with how “Pulling Taffy Apart” works. On the other hand, lower rate and frequency can result in early ossification, which would complicate the distraction inadvertently. Clinicians around the world often aim for a daily distraction rate of 1.0–1.5 mm and limit activation frequency to 2-4 times.
• Consolidation phase-This phase comprises an extended period of immobility during which the stretched callus is supported by the device as it matures, maintaining the callus’s stretched and stable posture and avoiding cartilaginous intermediate. The first step in remodelling is to provide lamella bone with elements of bone marrow time to develop. The consolidation period lasts between four and twelve weeks, on average eight weeks. According to clinical recommendations, the consolidation phase should last twice as long as the activation phase. The distraction site’s location and the rate of bone metabolism determine when the consolidation period begins.
• Remodelling phase-This phase primarily consists of formation of lamellar bone. It is in this stage the distractor is removed after establishment of continuity bone & alveolar canal. The need for further intervention should be identified at earliest and also relapse should be checked in follow up visits which will ensure good prognosis.
INDICATIONS
Indications in Mid face (Maxilla & Orbit) abnormalities include need for midfacial and maxillary advancement in treatment of LeFort III and LeFort I respectively. In this region other indications include alveolar gap closure in cleft lip and palate patients, Fronto-orbital advancements, remodelling of the cerebral vault through a slow separation across removed stenotic structures, etc.
In Lower face (Mandible) abnormalities include hemifacial microsomia conditions requiring unilateral distraction of mandible body, angle or ramus. Also, most common indication is infants and children with severe micrognathia and airway obstruction attributed to Pierre Robin syndrome which requires bilateral mandibular distraction. Alveolar segment is distracted vertically for implant facilitation or correction of occlusal plane whereas midline distracted horizontally to correct crossbite or for the improvement of arch form.
Craniofacial distraction osteogenesis for congenital abnormalities includes Cleft lip and palate patients, Hemifacial microsomia, Syndromic or Non syndromic Craniofacial Syndrome (Pierre Robin syndrome, Treacher Collins syndrome, Apert syndrome, Crouzon syndrome), Facial asymmetry, Mandibular hypoplasia due to ankylosis or trauma, Retrognathia, Bimaxillary crowding or deficiencies etc. In acquired abnormalities for reconstruction post oncologic jaw defects, Post traumatic reconstruction, Alveolar insufficiency in horizontal or vertical plane, Failed attempts at bone graft, etc.
CONTRAINDICATIONS
There are no absolute contraindications for mandibular distraction. However, relative contraindications can be stated as poor nutritional status and lack of healthy soft tissue; inadequate bone height and width; old age patients due to drastic fall in count of mesenchymal cells; osteoporotic, irradiated or necrotic bone; systemic disease which has general anaesthesia as a contraindication, etc.
ADVANTAGES
There are numerous advantages of Distraction osteogenesis. It is considered very safe as well as effective procedure and can be performed in a wide age group of patients, ranging from children above 2 years up to adults. Also, it can be performed on OPD basis thus reducing the time of hospitalization. Distraction osteogenesis eliminates use of bone grafts and associated risks thus there is no risk of negative effect on TMJ. Multiplanar & multidirectional distraction is possible along with nil or negligible nerve damage compared to conventional techniques. Treatment results after distraction osteogenesis are very stable. Relapse of soft tissue or skeletal origin is minimal which leads to high patient acceptance is very high. Also, the duration of treatment lesser that that required for BSSO. There is no need for extraction and thus it has a better prognosis.
DISADVANTAGES
Transcutaneous fixation pins can lead to facial scarring. This can be minimized by calculated placement of the incisions in minimal tension lines. To overcome this drawback, osteotomy and pin insertion incision is given intra orally. Incorrect displacement of vector can lead to unsatisfactory results. Only skeletal deformities are corrected and growth disturbance is left untouched. Sometimes a repeat procedure may be needed due to relapse. Newly formed tissue is less in mineral content and density. Use of distractor can be uncomfortable as they are bulky. Treatment cost is high and equipment as well as technique sensitive procedure.
COMPLICATIONS
The complications concerning distraction osteogenesis can be divided into three sections namely:
i. Intra operative- General hazards such as bleeding or pain, injury to the nascent tooth bud by a pin, partial fracture of the bone, nerve injury, instability or device breakage, etc.
ii. Intra distraction- Early bone calcification, discomfort, patient cooperation when using the distraction device, incapacity to eat, infection surrounding pins, etc.
iii. Post distraction- malunion or inability of the callus to heal, soft tissue pressure-induced recurrence, chronic nerve injury, external distractors causing facial scars, issues related to the TMJ, and altered speech.
FACTORS AFFECTING DISTRACTION OSTEOGENESIS
The factors affecting distraction osteogenesis were summarized by Imola MJ et al (2008) as follows:
A. Local factors- These factors include blood supply to the operated region, presence or absence of infection, whether the soft tissue is scarred, bone density at the site, irradiation history & osteoprogenitor supply.
B. Systemic factors- These are overall bodily factors affecting distraction osteogenesis like age, presence of any metabolic disease, deficiency of vitamin D or calcium, patient with a history of steroid intake & connective tissue defects.
C. Distraction factors- These are factors related to the procedure of distraction osteogenesis. These include rate of distraction & its frequency, period of latency and consolidation, rigidity of fixation & regenerative span.
Devices in Distraction Osteogenesis
The devices used in distraction osteogenesis are referred to as distractors. The craniofacial distractors can be divided into internal and external distractors.
1) External distractors
a. Unidirectional- Hoffman Mini Lengthener; Unidirectional mandibular Distractor
b. Bidirectional- Molina’s Bi-directional Distractor
c. Multidirectional- Multi-directional Distractor
2) Internal distractors
a. Tooth borne
b. Bone borne
c. Hybrid distractors
Unidirectional- The Hoffman Mini Lengthener device was introduced by McCarthy in 1989. It was used for mandibular lengthening and was fixed externally. It consisted of two double pin fixation clamps, a telescopic rod and screw. Device is adapted by rotation of clamp and sliding the other along the telescope distractor shaft. Unidirectional Mandibular Distractor developed for mandibular lengthening by Bitter and Klein along with Normed Medizin, Germany. Has two clamps, one for rotation and another for sliding. Both clamps are connected to geared distractor. Distraction is activated by advancement screw present on the sliding clamp.
Bidirectional- Molinas Extraoral Distractor useful in cases with severe hypoplasia of mandible. Indication is post single or double osteotomy, distraction can be done both horizontally or vertically. It has two geared arms and a middle screw for changing angulation. Extraoral Multi-Directional Distractor indicated in cases with midface development defects. In order to bridge the gap between the patient’s diagnosis and the age at which they can have bimaxillary repositioning osteotomies, orthodontic preparation is required. Costochondral grafts are implanted in damaged mandibular locations in children. Guerrero – Intraoral Device for Mandibular Widening first introduced in 1987, this was first device of its kind for widening mandible. A vertical symphyseal osteotomy is required prior and custom-made hyrax is placed. Activated 48 hours post-surgery and upon completion of distraction, acrylic is flowed around appliance to maintain expansion and stabilize it.
Distractor Orientation
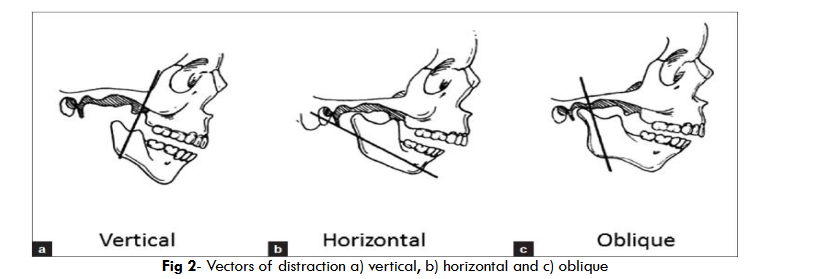
The distraction device orientation is along the three vectors for distraction, namely, vertical, horizontal and oblique. According to various planes in which distraction is carried out, they are subdivided into multiple models as follows:
• Model I- Transverse plane- Distractor oriented parallel to lateral mandibular surface
• Model II- Transverse plane- Distractor oriented parallel to midsagittal axis and to each other as well
• Model III- Transverse plane- Distractor parallel to lateral mandibular surface
• Model IV- Transverse plane- Distractor parallel to each other
• Model V- Sagittal plane- Distractor at an angle to occlusal plane
• Model VI- Sagittal plane- Distractor parallel to occlusal plane
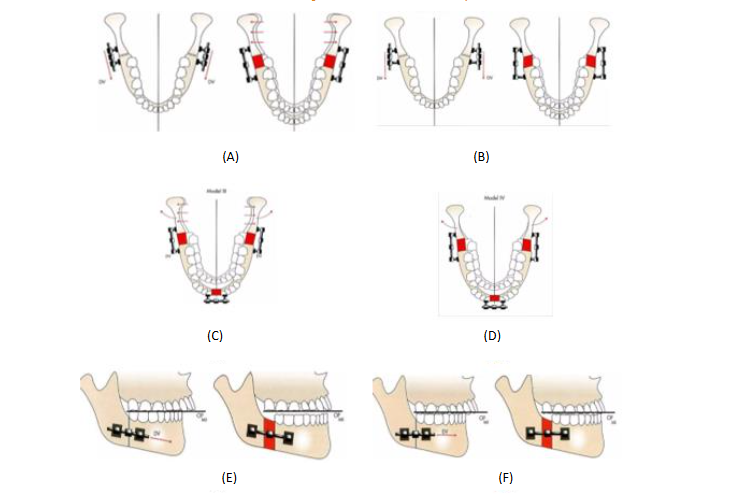
• Model I – Transverse plane – Distractor oriented parallel to lateral mandibular surface {fig 3. (A)}
• Model II – Transverse plane – Distractor oriented parallel to midsagittal axis and to each other as well {fig 3. (B)}
• Model III – Transverse plane – Distractor parallel to lateral mandibular surface {fig 3. (C)}
• Model IV – Transverse plane – Distractor parallel to each other {fig 3. (D)}
• Model V – Sagittal plane – Distractor at an angle to occlusal plane {fig 3. (E)}
• Model VI – Sagittal plane – Distractor parallel to occlusal plane {fig 3. (F)}
Orthodontic Considerations
An orthodontist plays a very crucial role in distraction osteogenesis from start till the end of procedure. This can be divided into three temporal stages:
i. Pre distraction orthodontics- After the mandibular distraction treatment plan has been developed, the dentition’s pre-surgical orthodontic preparation is initiated. A carefully considered pre-surgical orthodontic treatment is necessary for the best possible functional and cosmetic outcomes. In order to prevent the maxillomandibular skeleton relationship from being hampered by the current dental malocclusion, the teeth should be ideally positioned in respect to the basal bone. Designing a distraction stabilizing appliance is a crucial part of pre-distraction orthodontics. Before surgery, distraction appliances are typically placed in patients undergoing distraction osteogenesis.
ii. During distraction orthodontics- The surgical operation is carried out once the pre-surgical orthodontics is finished. Bands, brackets, headgears, elastics, distraction stabilization appliances, maxillary expansion appliances, functional appliances, etc., may be used in this phase of treatment. Utilizing these appliances helps the tooth-bearing segment move toward its intended post-distraction position, which enhances the quality of the surgical and orthodontic outcome.
iii. Post distraction orthodontics- Following consolidation, the distraction device is eliminated, and the newly produced bone across the distraction gap provides support for the mandibular tooth-bearing section. Whether the distraction of mandibular segment was unilateral or bilateral will determine the specific post-distraction orthodontic needs.
Conclusion
Distraction Osteogenesis, opens a new plethora of treatment and outcomes. Although the need for conventional mandibular and maxillary osteotomies will always persist, distraction osteogenesis tends to pave way for newer treatment approach for craniofacial abnormalities for orthodontist and oral surgeons as well. Recent developments have helped in the management of challenging clinical issues such as maxillary and mandibular abnormalities or cleft lip and palate.
Future Scope
It is likely that a more thorough understanding of the biomechanics of new bone formation under the effect of progressive traction will be established by the development of Osteo-distraction in the future for craniofacial applications.
References
- Cherackal G, Thomas N. Distraction Osteogenesis: Evolution and Contemporary Applications in Orthodontics. Journal of Research and Practice in Dentistry. Published online February 3, 2014;1-20.
- Chin M, Toth BA. Distraction osteogenesis in maxillofacial surgery using internal devices: Review of five cases. Journal of Oral and Maxillofacial Surgery. 1996;54(1):45-53.
- Barber S, Carter L, Mannion C, Bates C. Distraction osteogenesis part 2: technical aspects. Orthodontic Update. 2018;11(2):46-54.
- McCarthy JG. Craniofacial Distraction. Springer; 2017.
- Dr. Neharika Awode, Dr. Archana Jatania, Dr. Shruti Jangwad. Distraction Osteogenesis. Mahi Publication; 2024.
- Hatefi K, Hatefi S, Etemadi M. Distraction Osteogenesis in Oral and Maxillofacial Reconstruction Applications: Feasibility Study of Design and Development of an Automatic Continuous Distractor. Majlesi Journal of Electrical Engineering. 2018;12(3):69-75.
- Karacay S, Yildirim E, Bengi O, Okcu K. Treatment of midline shift by asymmetric premaxillary distraction: a case report. Gulhane Medical Journal. 2014;56(2):119.
- Uçkan S, Nurhan. Güler, Arman A, Mutlu N. Mandibular midline distraction using a simple device. Oral Surgery Oral Medicine Oral Pathology Oral Radiology and Endodontology. 2006;101(6):711-717.
- Tevlin R, Griffin M, Chen K, et al. Denervation during mandibular distraction osteogenesis results in impaired bone formation. Scientific Reports. 2023;13(1).
- Tevlin R, Januszyk M, Griffin M, et al. Denervation During Mandibular Distraction Osteogenesis Results in Impaired Osteogenesis. Journal of the American College of Surgeons. 2021;233(5); S196-S197.
- Kochhar R, Modi V, Neranjan de Silva, et al. Polysomnography-guided mandibular distraction osteogenesis in Pierre Robin sequence patients. Journal of Clinical Sleep Medicine. 2022;18(7):1749-1755.
- Hatefi S, Javad Alizargar, Yimesker Yihun, Milad Etemadi Sh, Hsieh NC, Khaled Abou-El-Hossein. Hybrid Distractor for Continuous Mandibular Distraction Osteogenesis. Bioengineering. 2022;9(12):732-732.
- Hatefi S, Etemadi Sh M, Yihun Y, Mansouri R, Akhlaghi A. Continuous distraction osteogenesis device with MAAC controller for mandibular reconstruction applications. BioMedical Engineering OnLine. 2019;18(1).
- Iwai T, Sugiyama S, Hirota M, Kenji Mitsudo. Horizontal alveolar transport distraction osteogenesis to stabilize removable prosthesis after mandibular reconstruction. Journal of Dental Sciences. 2023;18(4):1895-1896.
- Wang A, Wang S, Zhou Y, Wen Y, Jin Z, Chen X. Distraction osteogenesis promotes temporomandibular joint self-remodeling in the treatment of mandibular deviation caused by condylar ankylosis. Heliyon. 2023;9(12):e23055-e23055.
- Aditya Mohan Alwal, G Rajasekhar, Nandagopal Vura, M V S Sudhir, Srikanth Damera. Evaluation of use of distraction osteogenesis in mandibular retrognathia and its effect on soft and hard tissues and airway. National Journal of Maxillofacial Surgery. 2019;10(2):153-153.
- Chattopadhyay D, Vathulya M, Jayaprakash PA, Kapoor A. Outcome analysis of biplanar mandibular distraction in adults. Archives of Craniofacial Surgery. 2021;22(1):45-51.
- Laue K, Pogoda HM, Daniel Philip B, et al. Craniosynostosis and Multiple Skeletal Anomalies in Humans and Zebrafish Result from a Defect in the Localized Degradation of Retinoic Acid. The American Journal of Human Genetics. 2011;89(5):595-606.
- Ishihara Y, Arakawa H, Nishiyama A, Kamioka H. Occlusal reconstruction of a patient with ameloblastoma ablation using alveolar distraction osteogenesis: a case report. Head & Face Medicine. 2020;16(1).
- Gorrela H, Alwala AM, Ramesh K, Tunkimetla S, Prakash R, Zainuddinelyaskhan Y. Arthroplasty Followed by Distraction Osteogenesis Versus Distraction Osteogenesis Followed by Arthroplasty in the Management of TMJ Ankylosis: A Comparative Study. Journal of Maxillofacial and Oral Surgery. Published online October 7, 2020.
- Hatefi S, Milad Etemadi Sh, Javad Alizargar, Venous Behdadipour, Khaled Abou-El-Hossein. Two-Axis Continuous Distractor for Mandibular Reconstruction. Bioengineering. 2022;9(8):371-371.
- Li Z, Jiang D, Yao Y. Experimental Design of Vertical Distraction Osteogenesis Using Simple 3 Screws. Journal of Craniofacial Surgery. 2023;34(5):1599-1604.
- Wolford LM, Reiche-Fischel O, Mehra P. Changes in temporomandibular joint dysfunction after orthognathic surgery. Journal of Oral and Maxillofacial Surgery. 2003;61(6):655-660.
- Gül A, Pieter de Gijt J, Wolvius EB, Koudstaal MJ. Patient experience and satisfaction of surgically assisted rapid maxillary expansion and mandibular midline distraction. Journal of Cranio-Maxillofacial Surgery. 2021;49(8):649-654.
- Hasserius R, Karlsson MK, Jónsson B, Redlund-Johnell I, Johnell O. Long-Term Morbidity and Mortality After a Clinically Diagnosed Vertebral Fracture in the Elderly—a 12- and 22-Year Follow-up of 257 Patients. Calcified Tissue International. 2005;76(4):235-242.
- Monasterio FO, Drucker M, Molina F, Ysunza A. Distraction Osteogenesis in Pierre Robin Sequence and Related Respiratory Problems in Children. Journal of Craniofacial Surgery. 2002;13(1):79-83.
- Hopper RA, Kapadia H, Susarla S, Bly R, Johnson K. Counterclockwise Craniofacial Distraction Osteogenesis for Tracheostomy-Dependent Children with Treacher Collins Syndrome. Plastic and Reconstructive Surgery. 2018;142(2):447-457.
- Thompson SH, Quinn M, Helman JI, Baur DA. Maxillomandibular Distraction Osteogenesis Advancement for the Treatment of Obstructive Sleep Apnea. Journal of Oral and Maxillofacial Surgery. 2007;65(7):1427-1429.
- Garcia AG, Martin MS, Vila PG, Maceiras JL. Minor complications arising in alveolar distraction osteogenesis. Journal of Oral and Maxillofacial Surgery. 2002;60(5):496-.
- Polley JW, Figueroa AA, Girotto JA, Dietze-Fiedler ML. Monobloc Differential Distraction Osteogenesis. Journal of Craniofacial Surgery. 2021;33(1):270-.
- Guerrero C, Bell WR, G. Contasti, A. Brea Rodriguez. Mandibular widening by intraoral distraction osteogenesis. British Journal of Oral & Maxillofacial Surgery. 1997;35(6):383-392.
- Heller JB, Gabbay JS, Daniel, et al. Genioplasty Distraction Osteogenesis and Hyoid Advancement for Correction of Upper Airway Obstruction in Patients with Treacher Collins and Nager Syndromes. 2005;117(7):2389-2398.
- Ekizer A, Uysal T, Güray E, Akkuş D. Effect of LED-mediated-photobiomodulation therapy on orthodontic tooth movement and root resorption in rats. Lasers in Medical Science. 2013;30(2):779-785.