





Dynamic Leg Length Discrepancy in Hip Arthroplasty Patients
Dynamic Leg Length Discrepancy in Hip Arthroplasty Patients: What is the Amount a Patient Can Accept Without a Limp? How to Avoid Medical-Legal Issues
Abstract
Introduction: Leg length discrepancy (LLD) following total hip arthroplasty (THA) is a common occurrence that can spoil an otherwise excellent clinical outcome as well as have medical-legal ramifications. Scientifically, the amount of LLD that is clinically significant in THA patients is not well established. The purpose of this study was to determine the relationship between static leg length discrepancy (SLLD) and dynamic leg length discrepancy (DLLD) in total hip arthroplasty patients. We also investigated the correlation between various methods of static leg length discrepancy measurement.
Methods: Static leg length was measured by three methods: tape measure from anterior superior iliac spine to medial malleolus, inclinometer (spirit level) measured with the sacrum for flexion of lumbar spine with the knees extended, ortho-roentgenogram. Participants were assessed for dynamic leg length discrepancy during walking using an inertial measurement unit (IMU). The IMU consisted of three tri-axially arranged accelerometers applied to the lumbar region of the spine in order to measure the centre of mass excursion in three dimensions. Data are recorded at 200 Hz for a maximum of 20 seconds. Each participant completed nine gait tests: four walks with modified shoe lifts applied in random order to the operative or non-operative sides of the THA group or alternate sides on controls, and a normal walk with no lift applied to either side. Lift heights were 0.2 cm, 1.2 cm, 2.2 cm, and 3.2 cm.
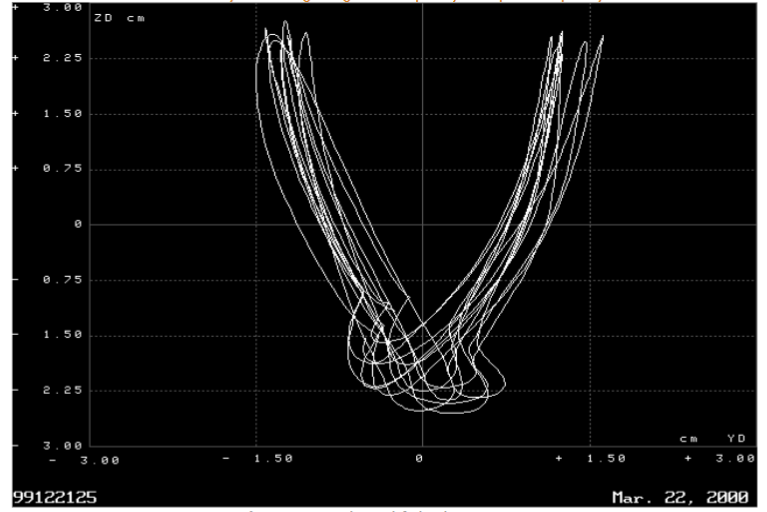
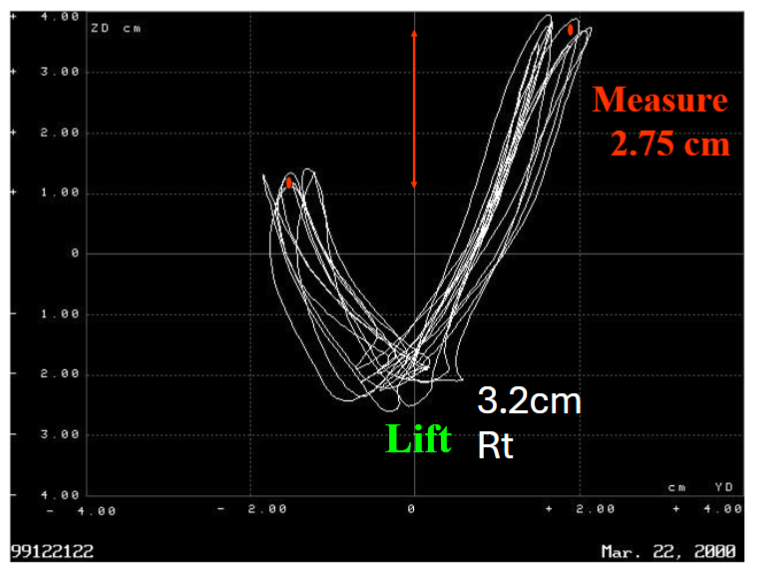
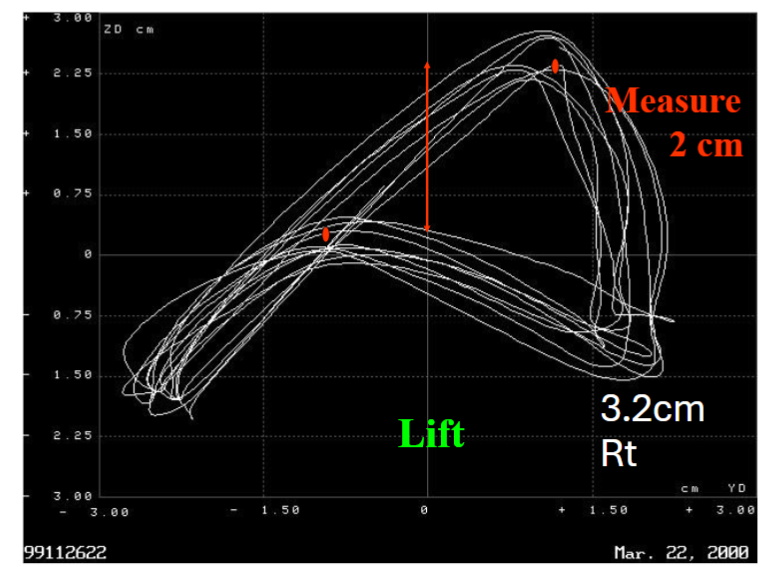
Results: Data from the inertial measurement unit was plotted in two dimensions to illustrate dynamic leg length discrepancy. A control with no lift and basically equal leg lengths showing a nice shift and equal heights of the Anterior Superior Iliac Crest (ASIS). A patient with a 1.2 cm lift on the right side, indicates a dynamic leg length discrepancy of 1 cm. A patient with 3.2 cm of lift on the right side, measures a 2.75 cm leg length discrepancy dynamically.
Conclusion: Dynamic leg length discrepancy of less than one centimeter is rarely detected by the patient and is quite easily adapted to with a small lift in the other shoe of 80% of the inequality. Dynamic leg length discrepancy of greater than one centimeter (static leg length discrepancy greater than 1.2 cm) usually provides a patient with enough discrepancy that a limp is perceptible. This study emphasizes the need to do careful leg length measurements when performing total hip arthroplasty.
Keywords
- Leg length discrepancy
- Total hip arthroplasty
- Dynamic leg length discrepancy
- Static leg length discrepancy
- Inertial measurement unit
Introduction
Leg length discrepancy (LLD) is one of the most common complications of total hip arthroplasty with a reported incidence anywhere from 1 – 27 % of patients. Symptomatic LLD can cause pain, altered gait patterns, and instability, all leading to patient dissatisfaction and making it one of the most common reasons for filing a law suit against orthopaedic surgeons.
Leg length discrepancy post-total hip replacement is usually that of overlengthening of the operative side to achieve improved stability. The incidence, of course, has been significantly decreased with better offsets of the stem and of the cup, more gradual neck lengths (and more sizes) that are able to improve the offset without establishing a significant leg length discrepancy and a better head size to improve stability without lengthening the patient.
A number of authors have reported on LLD over the years and the amount that is clinically acceptable. These views should be considered historical and really should have very little influence on how we view our patients. In 1978 Gross reported no functional or clinical significance in adults, and therefore no treatment required, for LLD less than two centimeters. In a 2019 survey of the United Kingdom surgeons 89% of surgeons agreed that 15 mm of LLD after primary uncomplicated THR was always acceptable; 90% of surgeons felt that LLD more than 22.74 mm was never acceptable. Edeen et al reported that 32% of patients were aware of LLD, with an average LLD of 15 mm, and more than half were bothered by this inequality. Others have reported that LLD greater than 10 mm results in clinical significance, with 15 – 27% requiring a shoe lift on the opposite side and altered gait dynamics.
The methods previously used to assess leg lengths were the Charnley Schuck method, preoperative templating plus intraoperative leg lengths, ASIS to medial malleolus, with palpation of the medial malleolus through the drapes. Another common option is a caliper or a fixed device to measure leg length.
A number of authors have studied the impact of LLD on gait with more recent studies using simple and inexpensive inertial measurement units instead of optoelectronic motion capture systems. An inertial measurement unit (IMU) is a device that measures acceleration vectors along orthogonal orientations in the Cartesian-coordinate plane. Despite the recognition that LLD affects gait parameters, most treatment has always been based on statically measured leg length discrepancy. How does static leg length discrepancy relate to dynamic leg length discrepancy, i.e. the leg length discrepancy while ambulating?
Our current study measured static leg length discrepancy in a select group of total hip arthroplasty patients using a tape measure, orthoroentogram, and a GPS accelerometer with a 5-20 Hz sampling rate. We also measured dynamic leg length discrepancy using an inertial measurement unit to derive biomechanical parameters. The purpose of this study was to determine the relationship between static leg length discrepancy (SLLD) and dynamic leg length discrepancy (DLLD) in total hip arthroplasty patients. We also investigated the correlation between various methods of static leg length discrepancy measurement.
Materials and Methods
Participants
The study population consisted of 20 subjects with a unilateral total hip arthroplasty (THA group) and 10 healthy age-matched controls (Control group). The THA group were selected from a local hip arthroplasty database. Inclusion criteria included: unilateral total hip arthroplasty, at least 12 months post hip replacement, no perceived or clinically observed limp, no hip or knee contractures, Harris Hip score of 80 or greater, and no significant associated medical conditions. Healthy age-matched volunteers were recruited and screened via telephone. All participants signed informed consent prior to study participation.
Static Leg Length Discrepancy (SLLD) Measurement
Static leg length was measured by three different methods. One was a tape measure from anterior superior iliac spine to medial malleolus: an average of three measurements was made for each patient. The second was inclinometer (spirit level) measured with the sacrum for flexion of lumbar spine with the knees extended, as per the literature: four degrees of inclinometer equaled one centimeter of leg length discrepancy; three measurements were taken and averaged. The third was ortho-roentgenogram: two independent observers with two readings each and an average of the two values.
Dynamic Leg Length Discrepancy (DLLD) Measurement
All participants were assessed for dynamic leg length discrepancy during walking using an inertial measurement unit (GPS accelerometer). The accelerometer consisted of three, tri-axially arranged, accelerometers applied to the lumbar region of the spine in order to measure the centre of mass excursion in three dimensions. Data were recorded at 200 Hz for a maximum of 20 seconds. For each gait test, participants were instructed to walk at a self-selected pace down a straight, unobstructed 20 meter hallway for 20 seconds. The test was repeated if the participant did not take a minimum of seven strides per side during the test. Each participant completed nine gait tests: four walks with modified shoe lifts applied in random order to the operative or non-operative sides of the THA group or alternate sides on controls, and a normal walk with no lift applied to either side. Lift heights were 0.2 cm, 1.2 cm, 2.2 cm, and 3.2 cm.
Participants in the THA group were also asked to subjectively assess which side was more difficult with the lifted walks, either operative or non-operative.
Statistical Analysis
Measurements were compared using analysis of variance (ANOVA) and Pearson’s correlation coefficient. Significance level was set at p=0.05.
Results
There were 13 males and seven females recruited in the THA group. The control group was evenly divided with five males and five females. Age, height, and weight were comparable between groups (Table 1). In the THA group, the time since surgery was 12 months to 107 months and clinical examination indicated no perceptible limp. The average Harris Hip score was 97.8 with a range from 92-100.
| THA Group | Control Group | |||||
|---|---|---|---|---|---|---|
| Range | Mean | Standard Deviation | Range | Mean | Standard Deviation | |
| Age (years) | 51-82 | 68.65 | 10.65 | 52-80 | 67.98 | 9.9 |
| Height (cm) | 155-181 | 169.10 | 7.13 | 153-191 | 170.2 | 11.14 |
| Weight (kg) | 56.3-142 | 80.68 | 20.97 | 61-103 | 80.82 | 13.58 |
Static leg length measurements are shown in Table 2. The maximum postoperative DLLD that was tolerated by the THA patients without causing a limp was 9.1 mm. Correlation between measurement methods in the unlifted state are shown in Table 3. When you look at the correlation and P value the only two that really matched up were that of the tape measure versus dynamic leg length discrepancy. Tape versus x-ray, x-ray versus inclinometer and tape versus inclinometer did not show much correlation. There was very reasonable and good correlation, which achieved statistical significance, in the tape versus dynamic leg length discrepancy, which is reassuring to all of us in clinical practice.
| Mean (cm) | SD (cm) | Range (cm) | |
|---|---|---|---|
| Tape | 0.35 | 0.33 | 0 – 1.0 |
| X-Ray | 0.46 | 0.47 | 0.02 – 1.48 |
| Inclinometer | 0.41 | 0.30 | 0 – 1.25 |
| DLLD | 0.43 | 0.26 | 0.14 – 0.91 |
| Correlation (R2) | P-value | |
|---|---|---|
| Tape vs. Inclinometer | 0.7147 * | 0.0000 |
| X-ray vs. Inclinometer | 0.4142 * | 0.0013 |
| Tape vs. X-ray | 0.2349 * | 0.0171 |
| Tape vs. DLLD | 0.2029 * | 0.0259 |
| Inclinometer vs. DLLD | 0.1178 | 0.0755 |
| X-ray vs. DLLD | 0.0157 | 0.2680 |
Data from the accelerometer inertial measurement unit (IMU) unit is plotted in 2 and 3 dimensions with a gait view program to illustrate dynamic leg length discrepancy. All participants were assessed for dynamic leg length discrepancy during walking using an accelerometer. The GPS accelerometer consisted of three, tri-axially arranged, accelerometers applied to the lumbar region of the spine in order to measure the centre of mass excursion in three dimensions. Data were recorded at 200 Hz for a maximum of 20 seconds during each walking phase. This is a GPS inertial measurement program.
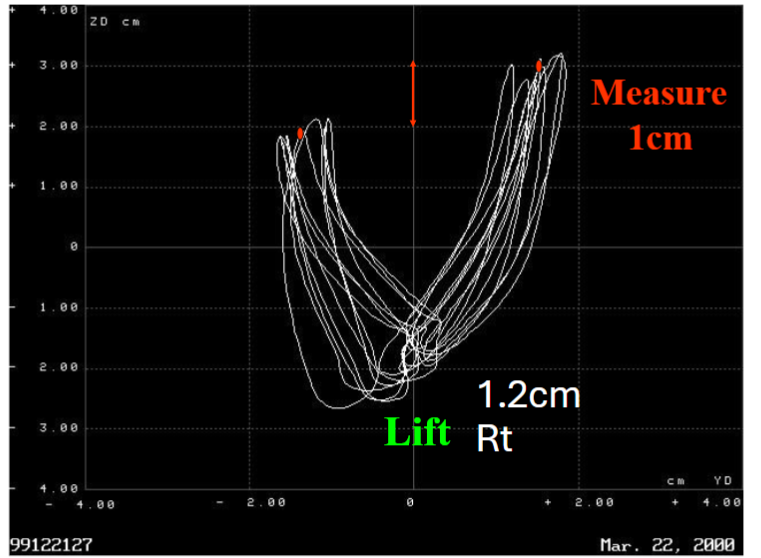
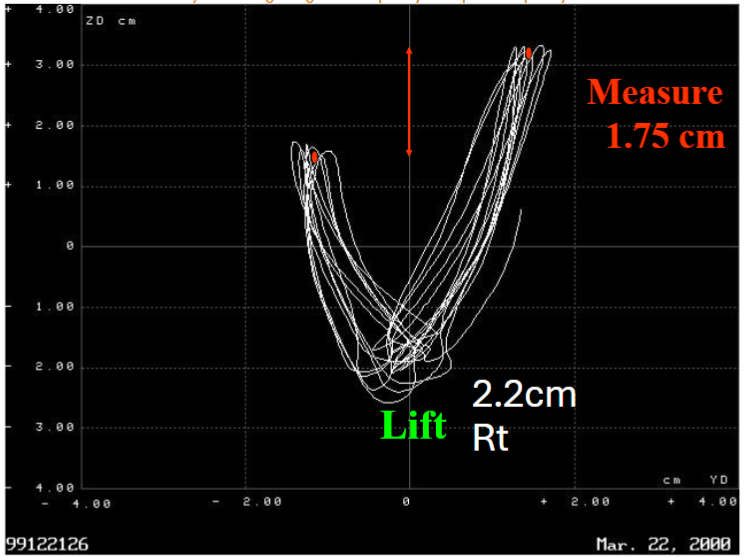
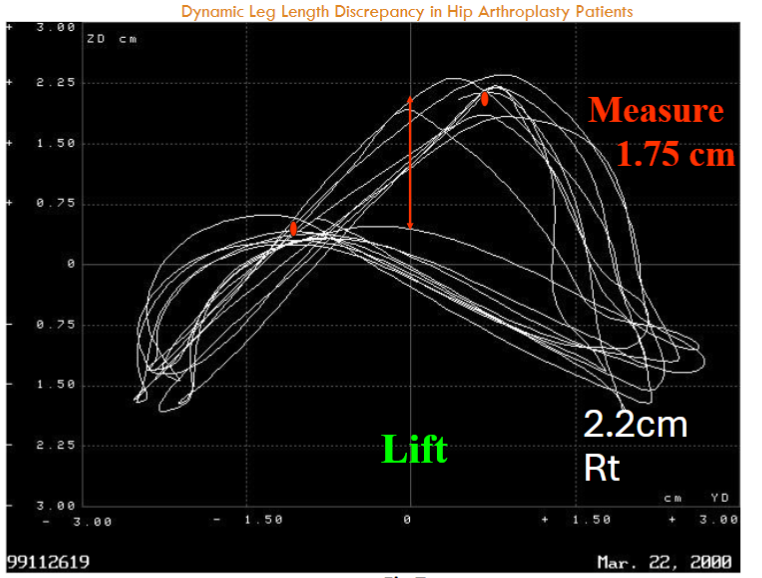
The next figure shows that of a patient with a 1.2 cm lift on the right side, indicating a dynamic leg length discrepancy of 1 cm. The patient was able to compensate by about 80%. Figure three shows a patient with 2.2 cm lift on the right side, measuring a dynamic leg length discrepancy of 1.75 cm.
Using the fore-aft measurement, the next figure of the same patient with no lift shows no major leg length discrepancy with the graph viewed from above the patient. Figure 5 shows a right-sided lift of 1.2 cm and the patient self-adjusts so it measures 8 mm.
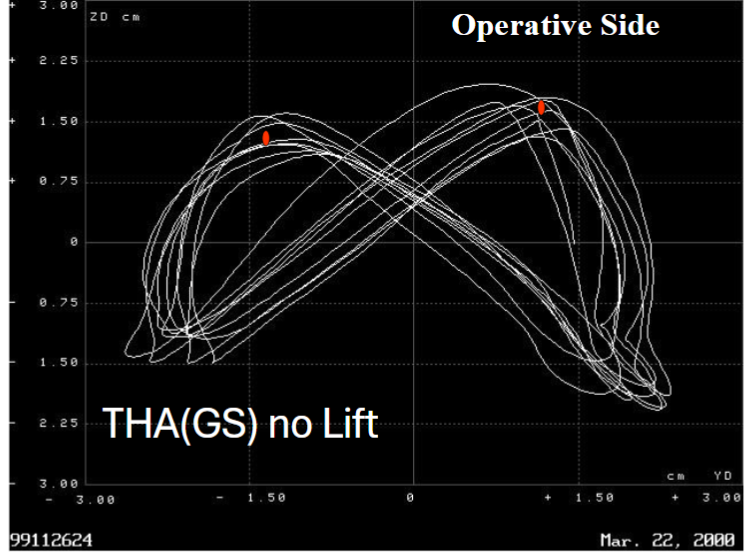
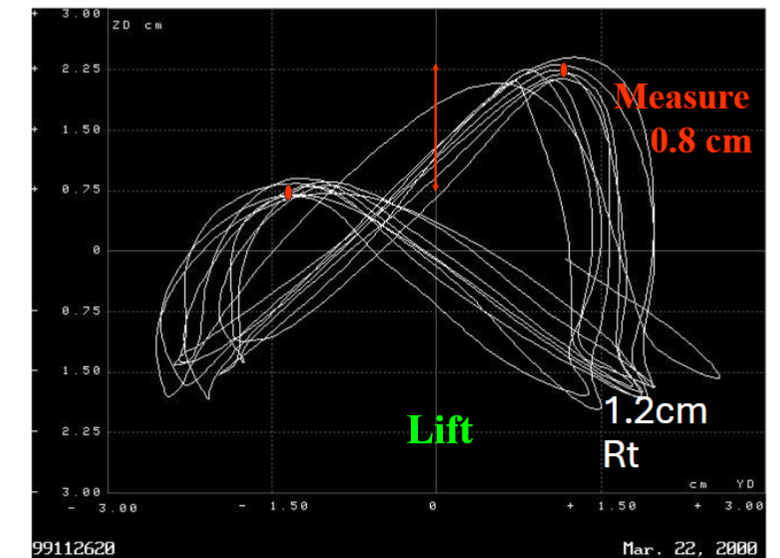
Figure 7 shows the patient has a 2.2 cm lift on the right side. The patient self-adjusts to have a 1.75 cm difference. Inertial measurement is a sensitive measurement of dynamic leg length discrepancy and correlates highly with simulated leg length discrepancy lifts in total hip arthroplasty patients. Figure 8 shows the high correlation between lift height and dynamic leg length discrepancy in the THA group and the control group.
For example, an 8 mm leg lengthening could be corrected with a 6 mm lift on the other leg. This, as indicated above, would mean the patient can accommodate to approximately 20% of the leg length discrepancy, so they require a lift of 80% of the measured difference. If > 20 mm, they may require 85% of the discrepancy in the form of a lift. The ability to compensate decreases with the size of the discrepancy which has never really been detailed prior to this current study.
In a select group of total hip arthroplasty patients with no limp, up to 9 mm of leg length discrepancy could be measured statically and dynamically. If a LLD exists > 9 mm they all limped! There was a high correlation between tape and inclinometer, x-ray and inclinometer for static leg length measurements, weaker correlation between tape and x-ray. Of all static measurements only the tape correlated with dynamic leg length discrepancy in the unlifted state.
Total hip replacement recipients in this study compensated better on the non-operative side, 80%, versus the operative side, 20%. Controls again show high correlation between lifts and dynamic leg length discrepancy, so if there is no difference between sides they can compensate for lifts similar to non-operative side of the patient. Older patients with total hip replacements can only compensate up to 20% of the leg length discrepancy (up to a maximum of 9 mm) versus a young, healthy patient who can compensate up to 50% of the discrepancy. This should be the key message of this paper. THR patients cannot accommodate 50% of any stated LLD, and all patients notice a LLD if the LLD is > 9 mm. Most total hip replacement patients prefer a longer non-operative side while walking versus lengthening of the operative side but 20% actually prefer a longer operative side which is very interesting. We were unable to determine this group as an identifiable subgroup.
Discussion
Discrepancy of leg length (LLD) is common after arthroplasty of the hip, with lengthening being the more noticeable to patients than shortening of the operative limb. There are some suggestions in the literature that the amount of leg length discrepancy is not of clinically significant if it is less than one centimeter. This may be true but not in all cases. Some patients just do not have the ability to accommodate even for relatively small differences in leg length.
This study suggests that a younger patient with a 12 mm leg length inequality would have a dynamic leg length difference of 6 mm versus the older patient with a 12 mm difference would feel a dynamic leg length discrepancy of 10 mm. This is totally different than what we were all taught in the past and illustrates the true dichotomy of a patient’s and a surgeon’s perception of a “successful” surgical outcome. A patient with a seemingly minimal leg length inequality may still be very unhappy until they are lifted up to equal lengths. Many patients will slowly adapt to a minimal discrepancy but should be given a lift first and gradually be allowed to discard it on their own time. This is another key point: a lift should be given early to help the patient adapt “early on” in the rehabilitation process. Do not wait for an unhappy patient by telling them “it will be fine”!
Patient reported function scores and clinical tests demonstrate a few very weak correlations with radiographic outcomes. Under correction of the femoral offset is associated with lower patient reported function scores and with more step irregularity as well as step asymmetry during gait. Postoperative leg length inequality was associated with increased frontal plane tilt angle of the pelvis during the Trendelenburg test and increased sagittal plane motion of the pelvis during gait.
All surgical approaches for total hip arthroplasty, including anterior, lateral and posterior approaches show that leg length discrepancy occurs in about 25% of patients. Nearly nine percent (8.9%) of patients experienced a detrimental increase in leg length in the operative leg after total hip arthroplasty. It is not “approach related” despite many claims to the contrary.
Computer-assisted surgery studies have been done but remain inconclusive to date in determining whether computer-assisted surgery can provide a more accurate reproducible technique to achieve leg length equality in total hip arthroplasty patients. They have compared the clinical outcome with conventional, on-the-table judgement of leg lengths in a THA done through a lateral approach. Results demonstrate that computer-assisted surgery can provide a more accurate reproduction of limb length but the difference, although seeming statistically significant, did not show a clinically significant difference to date. Short to medium term studies have demonstrated no benefit in clinical outcome scores.
The hope is that this improved accuracy will make a long term difference in wear and outcomes but the better ultra-highly-cross-linked poly may make this impossible to measure clinically. Reassuringly, there was a high correlation between measurements from a computer-assisted surgery and the final intraoperative radiographic measurements.
If indeed a significant inequality exists and the patient is very unhappy, surgical correction may be required. Fortunately, there have been good studies looking at the long term results of revision surgery with refractory symptomatic leg length inequality after primary hip replacement. Parvizi et al concluded that a marked postoperative LLD may lead to substantial disability as a result of pain or functional impairment, which warrants revision surgery. In the case of revision surgery for leg length inequality, while it may not resolve all of the pain and symptoms for the patient, it is a successful treatment to equalize leg lengths for patients who do not respond to conservative treatment of their leg length inequality. Clinical assessment, post revision of leg lengths, using a modified D’Aubigne and Postel scoring system reduced the leg length inequality from an average of 16 mm to 2 mm. In a surgical follow-up of twenty-one patients, 20 of 21 patients (95%) were satisfied with the improvement in their leg length discrepancy.
Leg length inequality should be avoided at all costs and there are numerous advantages to present day THA systems to avoid this mostly preventable complication. Systems should have high and low offset femoral necks, large heads, and offset acetabular liners in every surgeon’s set up for a primary and revision THA operation. Trochanteric advancement can be used primarily or as a revision of a leg length inequality to allow for equal leg lengths when instability is an issue.
Conclusion
This paper provides evidence that a leg length inequality of up to 9 mm is rarely detected by the majority of patients and is quite easily adapted to with a small lift of 80% of the inequality in the other shoe. Leg length inequality of greater than 9 mm, or one centimeter for easy memory for most of us, usually provides a patient with enough discrepancy that a limp is very perceptible. The patient will notice this as a leg length inequality or a leg length lengthening of the operative side. Thus, surgeons and patients should be made aware of this and a heel lift or orthotic should be offered early in the rehabilitation phase for any measured or perceived discrepancy (true leg length or perceived).
We, therefore, suggest that leg length inequality of less than 9 mm is very acceptable to the majority of patients in our study and will lead to a happy patient and a satisfied surgeon. Even these patients should be supplied with an early lift (80% of the LLD) and allowed to discard this on their own time. Any more than 9 mm of leg length discrepancy can lead to a disgruntled patient and a dissatisfied surgeon. This is harder to correct with just a lift or orthotic but the earlier the lift is supplied the better the outcome.
Measurement of dynamic leg length discrepancy is an appropriate method to determine lift requirements in post-operative total hip replacements. Inertial measurement units can be useful to assess the patient and determine the dynamic leg length discrepancy that the patient has dynamically as opposed to a static measurement. The main message is, of course, an ounce of prevention is worth a pound of cure so avoid lengthening the operative side intra-operatively if at all possible. This is usually accomplished utilizing all the methods mentioned plus image guided surgery may aid in this as well to preplan your surgery accurately.
References
- Benedetti, M. G., F. Catani, E. Benedetti, L. Berti, A. Di Gioia & S. Giannini (2010) To what extent does leg length discrepancy impair motor activity in patients after total hip arthroplasty? Int Orthop, 34, 1115-21.
- Bolink, S. A. A. N., E. Lenguerrand, L. R. Brunton, N. Hinds, V. Wylde, I. C. Heyligers, A. W. Blom, M. R. Whitehouse & B. Grimm (2019) The association of leg length and offset reconstruction after total hip arthroplasty with clinical outcomes. Clin Biomech (Bristol, Avon), 68, 89-95.
- Desai, A. S., A. Dramis & T. N. Board (2013) Leg length discrepancy after total hip arthroplasty: a review of literature. Curr Rev Musculoskelet Med, 6, 336-41.
- Edeen, J., P. F. Sharkey & A. H. Alexander (1995) Clinical significance of leg-length inequality after total hip arthroplasty. Am J Orthop (Belle Mead NJ), 24, 347-51.
- Gross, R. H. (1978) Leg length discrepancy: how much is too much? Orthopedics, 1, 307-10.
- Hofmann, A. A. & M. C. Skrzynski (2000) Leg-length inequality and nerve palsy in total hip arthroplasty: a lawyer awaits! Orthopedics, 23, 943-4.
- Jasty, M., W. Webster & W. Harris (1996) Management of limb length inequality during total hip replacement. Clin Orthop Relat Res, 165-71.
- Lecoanet, P., M. Vargas, J. Pallaro, T. Thelen, C. Ribes & T. Fabre (2018) Leg length discrepancy after total hip arthroplasty: Can leg length be satisfactorily controlled via anterior approach without a traction table? Evaluation in 56 patients with EOS 3D. Orthop Traumatol Surg Res, 104, 1143-1148.
- Li, J., A. B. McWilliams, Z. Jin, J. Fisher, M. H. Stone, A. C. Redmond & T. D. Stewart (2015) Unilateral total hip replacement patients with symptomatic leg length inequality have abnormal hip biomechanics during walking. Clin Biomech (Bristol, Avon), 30, 513-9.
- Licini, D. J., D. J. Burnikel, R. M. Meneghini & J. L. Ochsner (2013) Comparison of limb-length discrepancy after THA: with and without computer navigation. Orthopedics, 36, e543-7.
- Loughenbury, F. A., A. B. McWilliams, T. D. Stewart, A. C. Redmond & M. H. Stone (2019) Hip surgeons and leg length inequality after primary hip replacement. Hip Int, 29, 102-108.
- Mahar, R. K., R. L. Kirby & D. A. MacLeod (1985) Simulated leg-length discrepancy: its effect on mean center-of-pressure position and postural sway. Arch Phys Med Rehabil, 66, 822-4.
- Manzotti, A., P. Cerveri, E. De Momi, C. Pullen & N. Confalonieri (2011) Does computer-assisted surgery benefit leg length restoration in total hip replacement? Navigation versus conventional freehand. Int Orthop, 35, 19-24.
- McWilliams, A. B., A. Lampropoulos & M. H. Stone (2018) Revision surgery for leg length inequality after primary hip replacement. Hip Int, 28, 554-558.
- Parvizi, J., P. F. Sharkey, G. A. Bissett, R. H. Rothman & W. J. Hozack (2003) Surgical treatment of limb-length discrepancy following total hip arthroplasty. J Bone Joint Surg Am, 85, 2310-7.
- Pyrko, P. & J. Zuckerman (2016) Leg Length Discrepancy in Primary Total Hip Arthroplasty. Bull Hosp Jt Dis (2013), 74, 82-7.
- Rajpaul, J. & M. N. Rasool (2018) Leg length correction in computer assisted primary total hip arthroplasty: A collective review of the literature. J Orthop, 15, 442-446.
- Ranawat, C. S., R. R. Rao, J. A. Rodriguez & H. S. Bhende (2001) Correction of limb-length inequality during total hip arthroplasty. J Arthroplasty, 16, 715-20.
- Ranawat, C. S. & J. A. Rodriguez (1997) Functional leg-length inequality following total hip arthroplasty. J Arthroplasty, 12, 359-64.
- Wylde, V., S. L. Whitehouse, A. H. Taylor, G. T. Pattison, G. C. Bannister & A. W. Blom (2009) Prevalence and functional impact of patient-perceived leg length discrepancy after hip replacement. Int Orthop, 33, 905-9.