





Echocardiography in COPD-Related Pulmonary Hypertension
Echocardiographic evaluation for phenotyping pulmonary hypertension in COPD. A review of the literature and a proposal for clinical practice
Rino Frizzelli1, Andralisa Frizzelli2
OPEN ACCESS
PUBLISHED: 28 February 2023
CITATION: FRIZZELLI, Rino; FRIZZELLI, Annalisa. Echocardiographic evaluation for phenotyping pulmonary hypertension in COPD. A review of the literature and a proposal for clinical practice. Medical Research Archives, [S.l.], v. 13, n. 2, feb. 2025. Available at: <https://esmed.org/MRA/mra/article/view/6249>.
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI: https://doi.org/10.18103/mra.v13i2.6249
ISSN 2375-1924
Abstract
Background. Chronic obstructive pulmonary disease (COPD) is a complex and heterogeneous lung condition characterised by chronic respiratory symptoms (dyspnoea, cough, sputum production) due to an inflammatory state affecting the airways, lung parenchyma and pulmonary vasculature. When the inflammatory state is particularly severe, the damage to the lung tissue leads to an imbalance between ventilation and perfusion (V/Q) in the alveoli and to hypoxemia, a factor that increases remodeling of the vascular bed, vascular resistance, worsening hypoxemia and pulmonary hypertension, a common complication that in COPD is usually mild.
Recent cluster analysis within the COPD population has identified a novel phenotyping of patients characterized by moderate airway obstruction, marked reduction in diffusing capacity for carbon monoxide and severe hypoxemia with normal PaCO2 and severe pulmonary hypertension, which is considered “out of proportion” and profound cardiopulmonary impairment.
So, screening for pulmonary hypertension is more necessary than ever in clinical practice, not only to assess pulmonary vascular damage, but also to intercept COPD that may have more vascular than ventilatory damage, or both; or to exclude COPD as a cause due to left ventricular failure.
Methodology:
We reviewed the literature data on the use of echocardiography to screen for pulmonary hypertension in patients with COPD of all severities. Opinions on the reliability of the method vary and are sometimes in contrast to the reliability of the eco-Doppler method for measuring pulmonary pressure in COPD, as the detection of pressure values is often in contrast to the chest conformation resulting from airway pathology. Right heart catheterisation remains the gold standard for the diagnosis of pulmonary hypertension, but the main drawback of the procedure is indeed its invasive nature, which carries some risks and cannot be performed on a large scale, especially in advanced COPD, which is often associated with severe comorbidities. Therefore, based on our experience, we have made a selection within the framework of the entire echocardiographic methodology and suggest a 4-step echocardiographic pathway with multiple parameters, including M-mode, 2D, pulsed-wave (PW) and continuous-wave (CW) colour Doppler, to define the presence of pulmonary hypertension, determine the severity of disease and phenotype of pulmonary vascular COPD or cardiogenic disease that could easily escape clinical observation, and provide support in screening for pulmonary hypertension for those assessing lung pathophysiology function in patients with COPD.
Conclusion:
Considering the limitations, Doppler echocardiography is a useful method for measuring pulmonary pressure and determining the underlying anatomical and functional cardiac abnormalities in patients with COPD. Right heart catheterization is necessary to accurately measure (or rule out) the presence of pulmonary hypertension; however, establishing a good correlation does not mean that one test can accurately replace another, but rather the combination and appropriate use of multiple modalities. Doppler echocardiography is a non-invasive, easily accessible and invaluable screening tool for the assessment and further management of pulmonary hypertension and represents a compromise between accuracy, safety, simplicity and cost. Doppler echocardiography and right heart catheterization, which complement each other, could lead to the highest level of care, especially for the COPD population, which may escape clinical and instrumental assessment of severe pulmonary hypertension. We believe that the clinician today faces the challenge of achieving ever better diagnostic and treatment goals and reducing the invasiveness of procedures to improve diagnostics. Therefore, Doppler echocardiography should be widely used not only in the diagnosis and treatment of heart disease, but also in lung diseases, especially COPD, the most common lung disease. The physician dealing with respiratory diseases must have sufficient knowledge of Doppler echocardiography in daily clinical practice and basic skills to assess or rule out, to prevent or reduce the escape of severe pulmonary hypertension in COPD and to avoid leaving the diagnosis to other specialists who are less involved in respiratory pathology and may pay less attention to the realities of COPD.
Introduction
Chronic obstructive pulmonary disease (COPD) is a heterogeneous lung condition characterised by chronic respiratory symptoms (dyspnea, cough, expectoration and/or exacerbations) due to abnormalities of the airways (bronchitis, bronchiolitis) and/or alveoli (emphysema) that cause persistent, often progressive, airflow obstruction; airflow limitation is poorly reversible.
COPD is a complex disease: an inflammatory condition involves the airways, lung parenchyma, and pulmonary vasculature and perpetuates further on long after patients have quit smoking.
Although we know that the risk of developing COPD is dependent on the amount and duration of cigarette smoking, it is clear that there is a high variation in susceptibility to the disease between individuals. When the inflammatory state is particularly severe, the damage of pulmonary tissue produce a mismatch in the ventilation-perfusion (V/Q) ratio in the alveoli and hypoxemia, a factor leading to increased remodeling of the vascular bed and, over time, structural changes called “remodeling” of the pulmonary vasculature, increased vascular resistance, worsening of hypoxemia and pulmonary hypertension (PH): its presence is associated with reduced survival and greater use of healthcare resources. The symptoms of COPD and of PH can be similar likewise, in severe PH, there may also be a need to distinguish patients with mild COPD from those with severe COPD; therefore, patients with COPD should be tested for PH. Unfortunately, lung functional tests useful for assessment of COPD are not able to measure the pulmonary vascular pressure. Spirometry is mandatory to confirm the presence of persistent airflow limitation but airflow obstruction is not always proportional to hemodynamic vascular compromise; a resting oxygen saturation of less than 90% should prompt measurement of arterial blood gases in all patients with COPD, especially who have Forced Expiratory Volume in the first second (FEV1) less than 40% of predicted, or clinical signs of respiratory failure or right heart failure because hypoxemia is a major cause of PH but not directly related to PH.
The measurement of diffusing capacity for carbon monoxide (DLCO) should not routinely be done, but may be helpful for assessment of patients with severe COPD. Contribution of imaging especially computed tomography (CT) of the chest has revolutionized the approach to assessing patients for COPD although chest CT is not currently considered to be chest radiograph replacement and tool standard of care in the diagnosis and management of COPD but a normal CXR does not exclude PH.
Normal mean pulmonary artery pressure (mPAP) is 14±3 mmHg with an upper limit of 20 mmHg. The 6th World Symposia on Pulmonary Hypertension (WSPH) defined PH in chronic lung diseases as mPAP of 21–24 mmHg with pulmonary vascular resistance (PVR) ≥3 Wood Units (WU) or mPAP 25–34 mmHg alone, and defined severe PH as mPAP ≥35 mmHg, or mPAP ≥25 mmHg with cardiac index <2 L·min⁻¹·m⁻².
Using this definition, most patients with COPD have mild to moderate elevations in mPAP. According to pathological, pathobiological, and therapeutic characteristics PH secondary to COPD is placed into five groups with hemodynamic profile of vascular or precapillary pulmonary hypertension; owing to its frequency COPD is by far the most common cause of PH in this group, more common of mild (mPAP = 25–35 mmHg) and moderate (mPAP = 35–45 mmHg) intensity as in cardiac diseases, whereas severe PH (mean PAP ≥45 mmHg) is generally found in primary PH and in chronic pulmonary thromboembolism. There is still a debate about the most appropriate threshold for Pulmonary Vascular Resistance (PVR), which primarily reflects the functional state of the system coupled to the pulmonary vascular endothelium and smooth muscle cells to characterize PH in a narrow sense, quantify the increase in vascular resistance and determine the haemodynamic profile of vascular or precapillary PH by right heart catheterization (RHC) (table 1).
Table 1. Hemodynamic profiles of pulmonary hypertension by heart catheterization
| Vascular or precapillary pulmonary hypertension | Venous pulmonary hypertension or post-capillary hypertension | Combined pre- and post-capillary hypertension |
|---|---|---|
| mPAP > 20 mmHg | mPAP > 20 mmHg | mPAP > 20 mmHg |
| PCWP ≤ 15 mmHg | PCWP > 15 mmHg | PCWP > 15 mmHg |
| PVR > 2 WU | PVR ≤ 2 WU | PVR > 2 WU |
Legenda: mPAP: mean Pulmonary Artery Pressure.
PCWP: Pulmonary Capillary Wedge Pressure.
PVR: Pulmonary Vascular Resistance.
In natural history of COPD, PH is an important complication not only in the advanced stage but also in patients with mild severity, and the symptoms may be similar. Therefore, patients with COPD should be tested for PH, and RHC is the gold standard for diagnosis.
RHC should be performed when significant PH is suspected and the results are likely to influence the patient’s management, including referral for transplantation, enrolment in clinical trials or registries, treatment of undetected left ventricular dysfunction or use of compassionate therapies. However, clinical practice shows that performing RHC in all COPD patients with suspected PH would be impractical and associated with excessive risk, including morbidity (1.1%) and mortality (0.055%).
Over the last 30 years, Doppler echocardiography (DE) has emerged as one of the most well known tools for assessing the presence or absence of pulmonary hypertension. It is an essential diagnostic step in any COPD patient with suspected PH and allows assessment of the morphological and functional aspects of right ventricular hypertrophy and/or dilatation and ejection flow dynamics and can also provide an estimate of systolic pulmonary artery pressure (sPAP).
On this basis, this study aims to illustrate the use of a non-invasive method such as Doppler echocardiography (DE) for PH screening and severity assessment in patients with COPD. It considers it as a tool that should be included in lung functional tests and fills a gap by characterizing the phenotyping of PH in COPD and providing a basic guide for the clinician dealing with respiratory disease, thus improving the diagnostic, prognostic and therapeutic framework of COPD.
Methodology
We have reviewed the literature data through an electronic search on PubMed and Google Scholar on the use of echocardiography to screen for pulmonary hypertension in patients with COPD of all severities and, based on our experience, we propose a 4-step echocardiographic pathway with multiple parameters, including M-mode, 2D, Pulsed-wave (PW) and Continuous-wave (CW) Colour Doppler, as shown in figures 1–2–3–4–5, to define the presence of PH, determine the severity of the disease, determine the phenotype of pulmonary vascular COPD or cardiogenic disease that could easily escape the clinician, and allow those who have been excluded from learning echocardiography for educational reasons to obtain information leading to diagnostic, therapeutic and prognostic improvements in the patient’s life.
STEP 1 – DE ESTIMATION OF sPAP WITH TRICUSPID REGURGITATION VELOCITY (TRV)
To define PH, sPAP can be used interchangeably with mean pulmonary artery pressure (mPAP). The first step in assessing the echocardiographic probability of the presence of PH is to measure peak TRV using continuous wave Doppler (CW Doppler), which, when substituted into the modified Bernoulli equation (4v²) and added to the estimated right atrial pressure (RAP), provides an estimate of sPAP.
Echocardiographic evaluation for phenotyping pulmonary hypertension in COPD. A review of the literature
The tricuspid regurgitation (TR) jet should be performed from multiple views to obtain the most direct alignment, and the position of the CW cursor should be chosen to obtain the highest velocity (from parasternal short- or long-axis projection, apical and subcostal views). If this signal is of good quality and greater than 3.4 m/s, there is a high probability that PH is present. So,
sPAP = (4 × TRV max² + RAP).
If the TRV peak is less than 3.4 m/s, the probability of PH is assessed in combination with other echocardiographic markers. As a rule, a threshold value of 40 mmHg or higher is compatible with PH. Under optimal conditions, sPAP Doppler estimation correlates well with invasive measures, normal value < 35 mmHg (figure 1). When the TR signal by CW is suboptimal and sPAP is important for clinical decision making, the signal becomes more visible and measurable by injection of moving saline and CW measurement of TR.
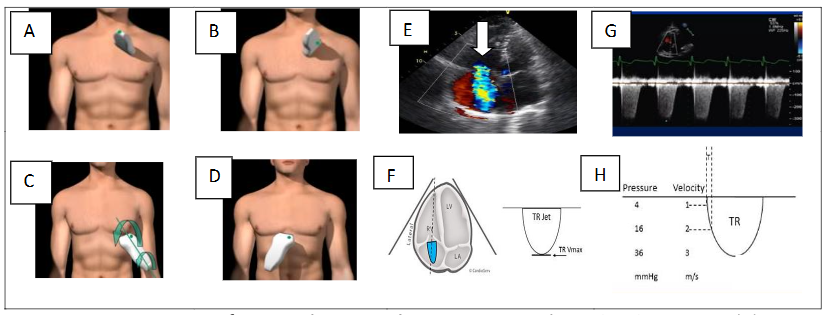
Figure 1. DE estimation of sPAP with Tricuspid Regurgitation Velocity (TRV): parasternal short- or long-axis projection (A–B), apical (C), subcostal (D) views; peak TRV profile (arrow) using CW Doppler (E–F–G–H).
STEP 2 – DE ESTIMATION OF RIGHT ATRIAL PRESSURE (RAP)
An assumed RAP is routinely added to the TR to estimate the sPAP. RAP pressure estimation is based on inferior vena cava (IVC) diameter in the subcostal view during quiet respiration and after “sniff” maneuver. The subcostal view is most useful for imaging the IVC, with the IVC viewed in its long axis.
The measurement of the IVC diameter should be made at end-expiration and just proximal to the junction of the hepatic veins that lie approximately 0.5 to 3.0 cm proximal to the ostium of the right atrium. To accurately assess IVC collapse, the change in diameter of the IVC with a sniff and also with quiet respiration should be measured, ensuring that the change in diameter does not reflect a translation of the IVC into another plane.
The measurements are done at end-diastole (figure 2).
IVC diameter ≤ 2.1 cm that collapses > 50% with a sniff suggests a normal RAP of 3 mmHg (range, 0–5 mmHg).
IVC diameter > 2.1 cm that collapses < 50% with a sniff suggests a high RAP of 15 mmHg (range, 10–20 mmHg).
In indeterminate cases in which the IVC diameter and collapse do not fit this paradigm, an intermediate value of 8 mmHg (range, 5–10 mmHg) may be used.
STEP 3 – DE ESTIMATION OF PULMONARY ACCELERATION TIME (AcT) AND PULMONARY ARTERY DIMENSION
In PH, early pulmonary ejection may be increased, resulting in a short acceleration time. A complementary method for pressure assessment utilizes the AcT of the pulsed wave (PW) Doppler flow velocity in the right ventricular outflow tract (RVOT). This measure is simple, reproducible and correlates inversely with the mPAP. PW Doppler measurement is performed after positioning the sample volume just below the pulmonary cusp on the right ventricle side in the RVOT outflow tract.
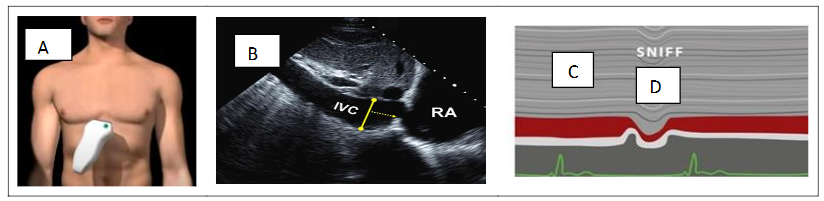
Figure 2. RAP estimation based on inferior vena cava (IVC) diameter in the subcostal view (A–B) during quiet respiration (C) and after “sniff” maneuver (D).
Measure at the end of expiration from the onset of flow to peak flow velocity. As pulmonary artery pressure (PAP) increases, the acceleration time of right ventricular ejection into the pulmonary artery decreases.Use the average of five beats for atrial fibrillation. Heart rates (HR) outside the normal range (< 70 or > 100 bpm) may affect accuracy and a correction for HR may be used (RVOT AT × 75 / HR). Correlations between sPAP and time to maximal pulmonary blood velocity (AcT measured by PW Doppler echocardiography) are strong. In addition, AcT may be a better marker of pulmonary artery impedance or right ventricular afterload than pressure. That is, in two patients with the same mPAP, the patient with a high AcT (i.e., > 100 ms) will have a relatively normal pulmonary vascular resistance (PVR), whereas a patient with an AcT of less than 100 ms is more likely to have an elevated PVR and right ventricular afterload.On PW or CW Doppler examination of the RVOT, a notch can be seen in the centre of the systolic cavity. This notch is thought to be caused by the reflection of the pressure wave reflection at the increased PVR, which temporarily decreases the forward velocity. The presence of a pulmonary systolic notch is considered a marker for an elevated PAP; a pulmonary notch in mid-systole indicates increased PVR and poor vascular compliance, which corresponds to precapillary PH rather than PH due to left heart disease. Pulmonary AcT of less than 90 ms predicts a PVR of mortha3.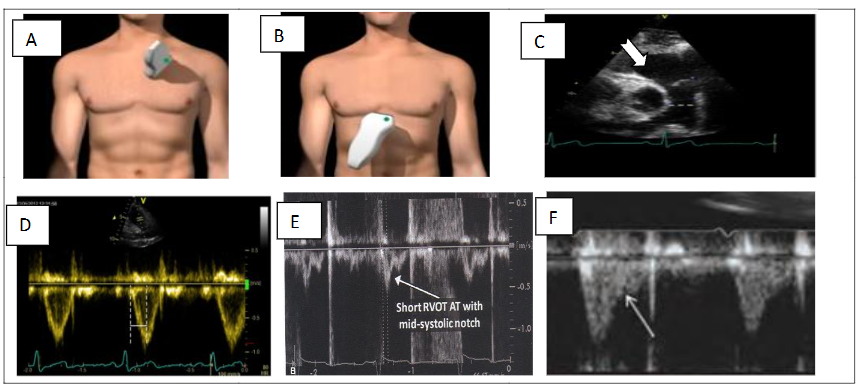
Figure 3. Parasternal (A) and subcostal (B) views. DE estimation of pulmonary artery dimension and pulmonary acceleration time (AcT). PA diameter > 25 mm (arrow) (C). Representative Doppler tracings without evidence of Doppler notching (D). Examples in the mid-systolic notch (arrows), characterized by a distinct notch or nadir in its mid portion, dividing the flow profile into 2 distinct peaks (E); Doppler tracings with a late systolic notch (F).
STEP 4 – DE ESTIMATION OF TRICUSPID ANNULAR PLANE SYSTOLIC EXCURSION (TAPSE), RIGHT ATRIAL (RA) SIZE AND QUALITATIVE ASSESSMENT OF RIGHT VENTRICULAR STRUCTURE AND FUNCTION
a. Tricuspid Annular Plane Systolic Excursion (TAPSE)
TAPSE is an angle-dependent measurement. Therefore, it is important to align the M-mode cursor along the direction of the lateral tricuspid annulus. Select a fast sweep speed. The excursion of the lateral tricuspid annulus is measured in M-mode between the end of diastole and the peak of systole and is a measure of the longitudinal systolic function of the RV in the apical four-chamber view. TAPSE < 1.7 cm is highly suggestive of systolic dysfunction of the RV.
b. Right atrial (RA) dimensions
Area is measured in the apical four-chamber view at end-systole (normal values ≤ 18 cm²), on the frame just prior to tricuspid valve opening, by tracing the RA blood-tissue interface, excluding the area under the tricuspid valve annulus. RA dilatation usually indicates exposure to chronic elevations in RA pressure due to tricuspid valve disease or increased right ventricular filling pressure.
c. Right ventricular (RV) dimensions, right to left ventricular ratio and pericardial effusion
Due to the increasing preload and afterload, there is progressive right ventricular dilatation with worsening PH. All measurements are taken at the end of diastole in the right ventricular-focused view. When performing the methods to quantify right atrial and ventricular size, it is important to pay attention to the correct timing of the cardiac cycle.
Measure the right ventricular at the end of diastole—when it is at its widest. The volume for the right atrial is measured at the end of systole, when it is at its largest volume. It is also possible to evaluate right ventricular-left ventricular ratio, size, and total left ventricular circumference, which, albeit in a generalized form, allows assessment of contractile efficiency and, in the context of the COPD hypothesis, vascular and cardiopulmonary phenotyping. The measurement is performed in apical view without foreshortening and is taken at the end of diastole. A ratio of >1 at the end of diastole suggests right ventricular dilatation. The presence of a pericardial effusion due to PH is a sign of advanced disease with a poor prognosis.
d. Fractional Area Change (FAC)
Fractional Area Change (FAC) is measured in apical four-chamber manual tracing of the RV endocardial border from the lateral tricuspid annulus along the free wall to the apex and back along the interventricular septum to the medial tricuspid annulus at the end of diastole and at the end of systole. A disadvantage of this measure is that it neglects the contribution of the RV outflow tract to overall systolic function. An RV FAC < 35% indicates systolic dysfunction of the RV (figure 4).
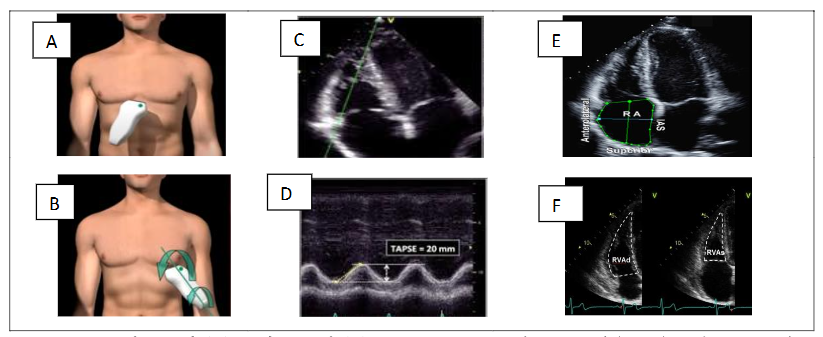
Figure 4. Subcostal (A) and apical (B) views. Decreased tricuspid annular plane systolic excursion (TAPSE) (C–D); end-systolic RA area (E); RV FAC Fractional Area Change (F).
ADDITIONAL DE MEASURES CAN CONTRIBUTE TO CLINICAL DEFINITION AND THERAPEUTIC DECISION, AND INCLUDE ESTIMATION OF DIASTOLIC PAP (dPAP) AND mPAP
Mild pulmonary regurgitation (PR) has been found in 40–78% of patients with morphologically normal pulmonary valves and no other signs of structural heart disease. Pathological regurgitation is infrequent; significant PR occurs in approximately 30% of patients with PH.
With CW and PW Doppler echocardiography, it is possible to estimate the diastolic pressure in the pulmonary artery (dPAP) in PR, especially when significant structural abnormalities of the right heart are present. Colour Doppler flow mapping is the most commonly used method to identify PR. A diastolic jet in the right ventricular outflow tract (RVOT) that starts at the coaptation line of the heart valves and is directed towards the right ventricular is diagnostic for PR.
PR velocities are measured from the parasternal short axis and in the subcostal views using PW in RVOT. However, there is no clinically recognized method for quantifying pulmonary regurgitation using CW Doppler; the density of the CW signal provides a qualitative measure of regurgitation. Although rapid deceleration is associated with more severe regurgitation, it is influenced by several factors, including RV diastolic properties and filling pressures.
dPAP and mPAP can be estimated: PR (pulmonary jet profile using the modified Bernoulli equation as for TRV) and RAP.
dPAP = 4 × (PR end velocity of PR jet velocity)² + RAP (normal value < 15 mmHg)
mPAP = 4 × (PR initial velocity of PR jet)² + RAP, where PR end is the end PR velocity and PR in is the initial PR velocity.
An early PR velocity > 2.2 m/s is considered a marker for increased mPAP. Although this measurement is subject to high inter-observer variability, a jet width that is > 65% of the RVOT width measured in the same frame is indicative of severe PR (figure 5).
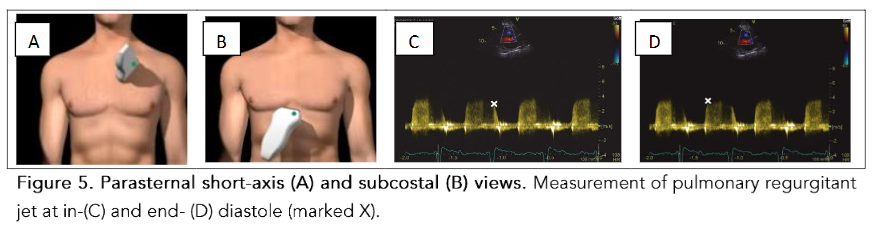
Alternatively, the mPAP can be estimated from the TRV using the formula derived by Chemla et al.:
mPAP = (0.61 × RVSP) + 2.
Discussion
COPD is a complex disease whose clinical presentations and functional characteristics can vary widely, potentially blurring important decisions in clinical practice. The whole concept of COPD as a syndrome with specific entities is constantly evolving. The traditional phenotypic distinction of pink puffers and blue bloaters proposed at the 1959 Ciba Guest Symposium has not proven to be clinically useful. Today, a new concept of clinical phenotype in COPD based on an analytical approach has been proposed; subgrouping patients into phenotypes emphasizes the fact that COPD is not a single disease, but a spectrum of diseases with smoking as a common risk factor.
Pulmonary vascular involvement leading to PH is a typical feature that occurs not only in advanced COPD but also in patients with mild COPD. Recent cluster analysis within the COPD population has identified a novel phenotyping of patients characterized by moderate airway obstruction, marked reduction in diffusing capacity for carbon monoxide (DLCO) and severe hypoxemia. Normal PaCO₂ and severe PH (mPAP ≥ 35 mmHg), which is considered “out of proportion.” These patients may represent a group with exaggerated vascular impairment (pulmonary vascular phenotype) due to factors that trigger PH in COPD, or patients in whom idiopathic pulmonary arterial hypertension (PAH) coexists.
Chaouat et al. retrospectively analysed the hemodynamic investigations of 998 COPD patients. They identified 27 patients with severe PH, defined by mPAP > 40 mmHg and moderate airway obstruction (FEV₁ 50% predicted), severe hypoxemia, hypocapnia, very low DLCO and shorter survival. Thabut et al. confirmed the uncommonness of severe PH in patients with advanced COPD. They used a statistical analysis (“cluster” analysis) to individualize a specific subgroup of “atypical” patients (7.4%) characterized by moderately severe bronchial obstruction (mean FEV₁ 48.5%) as opposed to severe PH (mPAP 39.8 mmHg) and profound hypoxemia (mean PaO₂ 46.2 mmHg), but without hypercapnia (mean PaCO₂ 39.7 mmHg); their PAP was significantly higher and this small subgroup represents a subset of COPD patients in whom pulmonary vascular disease is prevalent.
Based on these observations, at least three COPD phenotypes can be identified with the emerging phenotype of PH:
-
COPD typical phenotype (Global Initiative for Chronic Obstructive Lung Disease – GOLD stage 2–3), which accounts for the majority of the population with COPD. PH is due to the increase in pulmonary vascular resistance (PVR) caused by functional and morphological factors, with chronic alveolar hypoxia being the most important. Pressure values are usually mild to moderate, mPAP is usually ranging between 25 and 35 mmHg in a stable disease state and progresses slowly, with no change in right ventricular function in the majority of cases.
-
COPD pulmonary vascular phenotype (1–7%): this phenotype is characterized by mild airway obstruction (FEV₁ > 60%), diffuse emphysema on high-resolution CT scans, severe precapillary PH (mPAP > 35–40 mmHg), severely reduced DLCO capacity, progressive dyspnea and profound cardiopulmonary limitation. These patients tend to develop progressive right heart failure and, in particular, have features similar to idiopathic PH. In addition, PH may also be complicated by airway obstruction and show clinical overlap with this described phenotype.
-
The cardiopulmonary phenotype of COPD: characterized by hypoxemia, predominantly male, elderly patients with impaired DLCO < 45% of predicted value, a history of smoking, and risk factors for left heart disease.
Therefore, measurement of PH is more necessary than ever in clinical practice, not only to assess pulmonary vascular damage, but also to intercept COPD that may have more vascular than ventilatory damage, or both; or to exclude COPD as a cause of PH due to left ventricular failure. However, it should be emphasized that the assessment of PH and its phenotype is part of the overall clinical assessment.
The exact prevalence of PH in chronic lung disease at large is not known, nor is it accurately reported for individual conditions. Estimates of prevalence vary widely and depend on the definition of PH, the physiological characteristics of the underlying lung disease and the methods used to determine pulmonary pressure.
In patients with severe COPD (FEV₁ < 24% predicted) who were candidates for lung volume reduction surgery or lung transplantation, 50% had PH, although this was usually mild (mPAP < 35 mmHg). In retrospective review of 4,930 patients with COPD evaluable for lung transplantation, PH was present in 30.4% by RHC (mPAP > 25 mmHg and normal PCWP), with a further 17.2% of patients having pulmonary venous hypertension with elevated PCWP.
In another study of 120 patients with severe emphysema (FEV₁ < 27% predicted) undergoing evaluation for lung volume reduction surgery, the incidence of PH, defined as mPAP > 20 mmHg, was 91%. Only 5% of patients had an mPAP > 35 mmHg.
RHC remains the gold standard for the diagnosis of PH and can help to differentiate diastolic left heart failure from precapillary PH in COPD, as it allows measurement of pulmonary vascular resistance (PVR) and capillary wedge pressure (PCWP). Unfortunately, the major drawback of RHC is indeed its invasive nature; the procedure carries some risks and cannot be performed on a large scale in COPD patients. Therefore, RHC cannot be used routinely, especially in advanced COPD, which is often accompanied by severe comorbidities.
Non-invasive tests that offer a compromise between accuracy, safety, simplicity, and cost are a goal of all healthcare professionals. Thus, all patients with mild, moderate, severe, and very severe COPD can be screened with DE, a readily available and non-invasive tool that is crucial to confirm the suspicion of PH. Unfortunately, DE is not in a position to judge PVR, which plays an irreplaceable role in the diagnosis and clinical classification of precapillary PH and in the choice of a specific therapy.
However, there are studies that demonstrate the accuracy of DE for the indirect measurement of PVR. Amr E. Abbas et al. have shown that the Doppler-derived ratio of the tricuspid regurgitant velocity to the velocity time integral of the right ventricular outflow tract (TRV/TVI RVOT) was subsequently correlated with invasive pulmonary vascular resistance (PVR) measurements using regression analysis; an equation was modeled to calculate PVR in Wood Units using DE and the results were compared with invasive measurements using Bland-Altman analysis. Bech-Hanssen et al. found that the effects of pressure reflection in the pulmonary artery tree on the right ventricular pressure waveform can be described by a new DE method. Importantly, these easily determined DE variables can be used to identify patients with increased PVR. Naka Saito et al. distinguished between precapillary and postcapillary PH by adding the atrial volume ratio to the left ventricular ejection fraction.
In addition to estimating sPAP, DE allows assessment of right ventricular morphology and function, right atrial diameter, signs of fluid overload, valves, or other left heart abnormalities that may contribute to the hemodynamic PH profile.
According to our experience, PVR measurement is not necessary for screening and classification of PH in COPD, as a comprehensive assessment of patients with PE relies on the integration of clinical assessment with lung functional tests and imaging. RHC should be performed in suspected severe PH (systolic pressure > 50–60 mm Hg), evaluation for lung transplantation, clinical deterioration, and progressive exercise limitation.
As the poor agreement between DE estimates of sPAP and values measured at RHC has been increasingly recognized in clinical practice, there has been a strong impetus for two separate positions on the accuracy of DE estimates of sPAP: those who support it and those who oppose it.
Hatle et al. were the first to demonstrate that the gradient across a regurgitant tricuspid valve could be estimated from the peak velocity of the tricuspid jet recorded by Doppler ultrasound. Yock and Popp reported that quantification of the regurgitant tricuspid jet from DE measurements to estimate sPAP correlated significantly with RHC measured in 20 patients. Subsequently, several similar observations were published, leading to the view that DE provides an accurate, non-invasive measurement of sPAP.
In the diagnosis of PH, DE is initially at a disadvantage because PH is defined in RHC as an mPAP greater than 20 mmHg. Although it is possible to measure mPAP by transthoracic echocardiography, sPAP is usually reported. The challenge for DE is to determine the upper limit of normal for sPAP. If mPAP is two-thirds of the diastolic pressure plus one-third of the systolic pressure, and assuming an mPAP of 20 mmHg and a pulmonary artery diastolic pressure of 15 mmHg, this would correlate with an sPAP of about 40 mmHg. Many use an upper limit for sPAP of >30 to 35 mmHg; DE is therefore more sensitive than specific. To make matters worse, sPAP measured with DE increases with both age and body surface area.
Body surface area. In order to avoid contradictions with the current guidelines, the American Society of Echocardiography guidelines reflect the prevailing recommendations by including both a numerical range (35–40 mm Hg systolic) and the presence of symptoms for consideration of further investigation.
Those who argue against this are essentially arguing that estimation of PAP by DE does not necessarily correlate with direct measurement of PAP by RHC, as in COPD patients an overinflated chest may alter sound wave transmission. Furthermore, patients with COPD are less likely to have measurable TRV than patients with more severe forms of PH. Even when a TR jet is observed, echocardiographic estimates of PAP are often inaccurate, leading to both false positive and false negative PH diagnoses, and the chance of obtaining tricuspid regurgitation signals of sufficient quality is generally low. In the large series (n = 374) of candidates for lung transplantation (most of them being COPD) investigated by Arcasoy et al., the estimation of sPAP was possible in only 44% of the patients, and 52% of pressure estimations were found to be inaccurate when compared with pressures measured during RHC (>10 mmHg difference). Sensitivity, specificity, and positive and negative predictive values of estimation for diagnosis of PH were 85%, 55%, 52%, and 87%, respectively. Despite a statistically significant correlation with directly measured values, estimation of sPAP by DE was frequently inaccurate in patients with advanced lung disease and leads to considerable overdiagnosis of PH.
Surinder Janda et al. performed a systematic review and quantitative meta-analysis to determine the correlation of pulmonary pressures obtained by DE versus RHC and to determine the diagnostic accuracy of echocardiography for PH. Within 29 studies evaluating patients with lung disease, 4 studies were composed of COPD patients. The summary correlation coefficient between sPAP estimated from DE versus measured by RHC was 0.70 (95% CI 0.67 to 0.73; n = 27). DE sensitivity and specificity for diagnosing PH was 83% (95% CI 73 to 90) and 72% (95% CI 53 to 85; n = 12), respectively. The summary diagnostic OR was 13 (95% CI 5 to 31).
The modest correlation of DE-sPAP versus RHC-sPAP and the modest diagnostic accuracy of DE for PH can be explained by several potential limitations such as misalignment of the ultrasound beam to the tricuspid regurgitant jet. One way of overcoming this is through the use of contrast agents that enhance the velocity signal. From meta-analysis, authors found that approximately 41% of patients did not have an optimal TR jet to allow the measurement of sPAP. The majority of these patients had COPD and thus this method may not be reliable in this population unless contrast is used. When the tricuspid regurgitant jet was adequately visualized, there was no difference in the correlation of sPAP by DE versus RHC and no difference in the diagnostic accuracy of echocardiography for PH.
The diagnostic accuracy for DE for PH with an sPAP threshold of 40 mm Hg was relatively modest. Potential limitations include the possibility of weak correlation and diagnostic accuracy in patients with high pulmonary pressures, inability to acquire an estimate of sPAP in COPD patients, and underestimation when the tricuspid regurgitant jet is not of good quality. So, when measuring pulmonary pressures by DE, clinical context, the prevalence of PH in the patient population, and other echocardiographic parameters of the right ventricle should be taken into consideration to improve the overall diagnostic accuracy. Authors concluded that considering the limitations, DE is a useful and non-invasive modality for measuring pulmonary pressure and for determining underlying anatomical and functional cardiac abnormalities in patients with suspected PH.
Conclusion
Patients with COPD are not all the same. Research into novel COPD phenotypes shows the complexity of the disease, which is not limited to damage to the bronchial and alveolar walls, but also involves vascular structures. Under certain conditions, vascular damage may predominate, leading to the identification of a new phenotype, the so-called vascular phenotype.
Vascular COPD phenotype, characterized by mild bronchial obstruction, severe hypoxemia, and severe PH. Despite advances in other techniques and disputes about the reliability of the data, non-invasive estimation of PH can currently be based on DE with good reliability. A good approach allows a satisfactory diagnosis including a more comprehensive functional evaluation of COPD, which is not limited to determining the phenotype of PH but also assesses right ventricular size and function that are the key to determining disease severity and prognosis. Although RHC is necessary to accurately measure PAP to diagnose (or rule out) the presence of PH, it is ultimately the status of the right ventricular that usually determines therapy and provides important prognostic information. This is an area where DE could allow for better determination of COPD stage, identification of the vascular and cardiopulmonary PH phenotype, and application of appropriate therapies to improve quality of life and prognosis.
In conclusion, we believe that clinicians today face the challenge of achieving ever better diagnostic and treatment goals and reducing the invasiveness of procedures to improve diagnostics. The use of DE remains an invaluable screening tool for the evaluation and further management of PH. However, establishing good correlation does not imply that one test is an accurate substitute for another; the combination and appropriate use of multiple modalities (DE with RHC) that complement each other could lead to the highest level of care, especially for the COPD population that may escape clinical and instrumental assessment of mild and severe PH. So, DE should be widely adopted by healthcare providers involved in the diagnosis and treatment of not only heart disease but also lung disease, especially COPD, the most common lung disease.
Financial disclosures:
The authors have no relevant financial interest in this article.
Authors’ contributions:
All authors contributed equally to and read and approved the final version of the manuscript.
Declaration of competing interest:
The authors report no conflict of interest.
References
1. Agustí A, Celli BR, Criner GJ, et al. Global Initiative for Chronic Obstructive Lung Disease 2023 Report: GOLD Executive Summary. Eur Respir J 2023; 61: 2300239 doi:10.1183/13993003.00239-2023.
2. Boers E, Barrett M, Su JG, Benjafield AV, Sinha S, et al . Pulmonary Disease Through 2050. Global Burden of Chronic Obstructive.JAMA Netw Open. 2023 Dec; 6(12): e2346598. Published online 2023 Dec 7.
doi: 10.1001/jamanetworkopen.2023.46598.
3. Barbera JA, Peinado VI, Santos S. Pulmonary hypertension in chronic obstructive pulmonary disease. Eur Respir J 2003; 21: 892–905 doi: 10.1183/09031936.03.00115402.
4. Kent BD, Mitchell PD, McNicholas WT. Hypoxemia in patients with COPD: cause, effects, and disease progression. Int J Chron Obstruct Pulmon Dis. 2011:6:199-208. doi:10.2147/COPD. S10611. Epub 2011 Mar 14.
5. Weitzenblum E, Hirth C, Ducolone A, Mirhom R, Rasaholinjanahary J, Ehrhart M. Prognostic value of pulmonary artery pressure in chronic obstructive pulmonary disease Thorax 1981 Oct;36(10):752-758. doi: 10.1136/thx.36.10.752. PMID: 7330793 PMCID: PMC471749
6. Lange P, Halpin D M, O’Donnell D., MacNee W. Diagnosis, assessment, and phenotyping of COPD: beyond FEV1 Int J Chron Obstruct Pulmon Dis. 2016 Feb 19;11(Spec Iss):3–12. doi: 10.2147/COPD.S85976.
7. Nathan SD, Barbera JA, Gaine SP, et al. Pulmonary hypertension in chronic lung disease and hypoxia. Eur Respir J 2019; 53: 1801914. https://doi.org/10.1183/13993003.01914-2018.
8. Labaki WW, Martinez CH, Martinez FJ, Galbán CJ, et al. The Role of Chest Computed Tomography in the Evaluation and Management of the Patient with Chronic Obstructive Pulmonary Disease. Am J Respir Crit Care Med.. 2017 Dec 1;196(11):1372–1379. doi: 10.1164/rccm.201703-0451PP.
9. Pistolesi M, Camiciottoli G, Paoletti M, et al. Identification of a predominant COPD phenotype in clinical practice Respiratory Medicine (2008) 102, 367–376. 2008 Mar;102(3):367-76.
doi: 10.1016/j.rmed.2007.10.019. Epub 2008 Jan 8.
10. Zhu Z. Advancements in automated classification of chronic obstructive pulmonary disease based on computed tomography imaging features through deep learning approaches Respir Med . 2024 Sep 18:234:107809. doi: 10.1016/j.rmed.2024.107809.
11. Keller CA, Shepard JW, Chun DS, Vasquez P, Dolan GF. Pulmonary hypertension in chronic pulmonary disease. Multivariate analysis. Chest 1986 Aug;90(2):185-192. doi: 10.1378/chest.90.2.185.
12. Galiè N, Vallerie V, Laughlin M, Rubin LJ, Simonneau G. EDITORIAL WORLD SYMPOSIUM ON PULMONARY HYPERTENSION An overview of the 6th World Symposium on Pulmonary Hypertension Eur Respir J 2019; 53: 1802148 doi.org/10.1183/13993003.02148-2018.
13. Kovacs G, Berghold A, Scheidl S, Olschewski H. Pulmonary arterial pressure during rest and exercise in healthy subjects: a systematic review .Eur Respir J 2009; 34: 888–894 doi: 10.1183/09031936.00145608 .
14. Humbert M, et Al. 2022 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension Developed by the task force for the diagnosis and treatment of pulmonary hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS). Endorsed by the International Society for Heart and Lung Transplantation (ISHLT) and the European Reference Network on rare respiratory diseases (ERN-LUNG). Authors/Task Force Members: (France),European Heart Journal (2022) 43, 3618–3731
https://doi.org/10.1093/eurheartj/ehac237
15. Chemla D, Castelain V, Hervé P. Haemodynamic evaluation of pulmonary hypertension European Respiratory Journal 2002; 20(5): 1314-1331; doi.org/10.1183/09031936.02.00068002
16. Hoeper MM , Lee SH, Voswinckel R, Palazzini M, Jais X, Marinelli A, et al. Complications of right heart catheterization procedures in patients with pulmonary hypertension in experienced centers. Multicenter Study. J Am Coll Cardiol. 2006 Dec 19;48(12):2546-52. doi: 10.1016/j.jacc.2006.07.061. Epub 2006 Nov 28. PMID: 17174196.
17. Nathan SD, Barbera JA, Gaine SP, et al. Pulmonary hypertension in chronic lung disease and hypoxia. Eur Respir J 2019; 53: 1801914 https://doi.org/10.1183/13993003.01914-2018
18. Otto CM. Pulmonary Hypertension in “The Practice of Clinical Echocardiography” Publisher Elsevier 6th Edition August 5, 2021:774-798.
19. Rudski LG, Lai WW, Afilalo J, Handschumacher MD, et al..Guidelines for the Echocardiographic Assessment of the Right Heart in Adults: A Report from the American Society of Echocardiography.Endorsed by the European Association of Echocardiography, a registered branch of the European Society of Cardiology, and the Canadian Society of Echocardiography.J Am Soc Echocardiogr 2010;23:685-713.) doi:10.1016/j.echo. 2010.05.010.
20. Forfia PR, Vachiéry JL. Echocardiography in pulmonary arterial hypertension Am J Cardiol. 2012 Sep 15;110 (6 Suppl):16S-24S. doi: 10.1016/j.amjcard.2012.06.012.PMID: 22921027.
21. Habib G, Torbicki A. The role of echocardiography in the diagnosis and management of patients with pulmonary hypertension. European Respiratory Review 2010; 19(118): 288-299;
doi: https://doi.org/10.1183/09059180.00008110.
22. Augustine DX, Coates-Bradshaw LD, Willis J, et al. Echocardiographic assessment of pulmonary hypertension: a guideline protocol from the British Society of Echocardiography .Echo Res Pract. 2018 Sep;5(3):G11-G24. doi: 10.1530/ERP-17-0071.PMID: 30012832 PMCID: PMC6055509 .
23. Vaidya A, Golbus JR, Vedage NA, Mazurek J, Raza F, Forfia PR. Virtual echocardiography screening tool to differentiate hemodynamic profiles in pulmonary hypertension Pulm Circ. 2020 Sep 17;10(3):2045894020950225. doi: 10.1177/ 2045894020950225. eCollection 2020 Jul-Sep. PMID: 32994924 PMCID: PMC7504864 .
24. Chemla D, Castelain V, Humbert M, Jean-Louis Hebert JL, Simonneau G, Lecarpentier Y, Herve´ P. New Formula for Predicting Mean Pulmonary Artery Pressure Using Systolic Pulmonary Artery Pressure CHEST 2004; Oct;126(4):1313-7. doi: 10.1378/chest.126.4.1313.
25. Fletcher CM, Gilson JG, Hugh-Jones P, Scadding JG. Terminology, Definitions, and Classification of Chronic Pulmonary Emphysema and Related Conditions. A Report of the Conclusions of a Ciba Guest Symposium. Thorax 1959 Dec;14 (4):286–299.
26. Leopoldo N, Segal MD, Martinez FJ. Chronic obstructive pulmonary disease subpopulations and phenotyping. Clinical reviews in allergy and immunology. 2018 American Academy of Allergy, Asthma & Immunology. https://doi.org/10.1016/j.jaci.2018.02.035.
27. Barnes PJ, Vestbo J, Calverley PM. The Pressing Need to Redefine “COPD” Chronic Obstr Pulm Dis. 2019 Nov;6(5):380-383. doi: 10.15326/jcopdf.6.5.2019.0173. PMID: 31710794 PMCID: PMC7020851
28. Vestbo J. COPD: definition and phenotypes. Clin Chest Med. 2014 Mar;35(1):1-6. doi: 10.1016/j.c cm.2013.10.010. Epub 2013 Dec 12. PMID: 24507832.
29. Mirza S, Benzo R. COPD Phenotypes – implications for care Mayo Clin Proc. Author manuscript; available in PMC: 2018 Jul 1.Published in final edited form as: Mayo Clin Proc. 2017 Jul; 92(7):1104–1112. doi: 10.1016/j.mayocp.2017.03.020 PMCID: PMC5587116 NIHMSID: NIHMS883486 PMID: 28688465.
30. Kovacs G, Agusti A, Joan Albert Barbera’ JA, Celli B, Criner G, Humbert M, et al. Pulmonary Vascular Involvement in Chronic Obstructive Pulmonary Disease Is There a Pulmonary Vascular Phenotype? Am J Respir Crit Care Med. 2018 Oct 15;198(8):1000-1011 doi: 10.1164/rccm.201801-0095PP.
31. Dweik RA, Sharon Rounds S, Erzurum SC, et al. An Official American Thoracic Society Statement: Pulmonary Hypertension Phenotypes .Am J Respir Crit Care Med. 2014 Feb 1; 189(3): 345–355. Published online 2014 Feb 1 PMCID: PMC4291177 PMID: 24484330 doi: 10.1164/rccm.201311-1954ST.
32. Chaouat A, Bugnet AS, Kadaoui N, Schott R, Enache I, Ducoloné A, Ehrhart M, Kessler R, Weitzenblum E. Severe pulmonary hypertension and chronic obstructive pulmonary disease . Am J Respir Crit Care Med. 2005 Jul 15;172(2):189-194. doi: 10.1164/rccm.200401-006OC. Epub 2005 Apr 14.
33. Thabut G, Dauriat G, Stern JB, et al. Pulmonary hemodynamics in advanced COPD candidates for lung volume reduction surgery or lung transplantation. Chest. 2005 May;127(5):1531-1536. doi: 10.1378/chest.127.5.1531.
34. Blanco I, Tura-Ceide O, Peinado VI, Barberà JA. Updated Perspectives on Pulmonary Hypertension in COPD. Int J Chron Obstruct Pulmon Dis. 2020 Jun 9:15:1315-1324. PMID: 32606641 PMCID: PMC7293405 doi: 10.2147/COPD.S211841 .
35. Agustín R G, Piccari L. Emerging phenotypes of pulmonary hypertension associated with COPD: a field guide. Pneumonologia i Alergologia Polska 2013, tom 81, nr 4, strony 390–398 Curr Opin Pulm Med. 2022 Sep; 28(5): 343–351. Published online 2022 Jul 16. doi: 10.1097/ MCP.0000000000000890 PMCID: PMC9451611 PMID: 35838373.
36. Krompa A, Marino P. Diagnosis and management of pulmonary hypertension related to chronic respiratory disease. Breathe 2022; 18: 220205 doi: 10.1183/20734735.0205-2022.
37. Humbert M, Kovacs G, Hoeper MM, et al. 2022 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Respir J 2023 Jan 6;61(1):2200879. doi: 10.1183/1399300 3.00879-2022. Print 2023 Jan.
38. Kularatne M, Gerges C, Jevnikar M, Humbert M, Montani D. Updated Clinical Classification and Hemodynamic Definitions of Pulmonary Hypertension and Its Clinical Implications. J. Cardiovasc. Dev. Dis. 2024, 11, 78. https://doi.org/10.3390/jcdd11030078.
39. Cuttica MJ, Kalhan R, Shlobin OA, Ahmad S, Gladwin M, Machado RF, et al. Categorization and impact of pulmonary hypertension in patients with advanced COPD. Respir Med. 2010; Dec;104 (12):1877-82. doi: 10.1016/j.rmed.2010.05.009. Epub 2010 Jun 14.
40. Scharf SM, Iqbal M, Keller C, Criner G, Lee S, Fessler HE, et al. Hemodynamic characterization of patients with severe emphysema. Am J Respir Crit Care Med. 2002 Aug 1;166(3):314-22. doi: 10.1164/rccm.2107027.
41. Abbas AE, Fortuin FD, Schiller NB, et al. A Simple Method for Noninvasive Estimation of Pulmonary Vascular Resistance. JACC Vol. 41, No. 6, 2003 Doppler Evaluation of PVR. 2003 Mar 19; 41(6):1021-7. doi: 10.1016/s0735-1097(02)02973-x.
42. Bech-Hanssen O, Lindgren F, Selimovic N, Rundqvist B. Echocardiography Can Identify Patients With Increased Pulmonary Vascular Resistance by Assessing Pressure Reflection in the Pulmonary Circulation. Circulation: Cardiovascular Imaging Volume 3, Number 4 https://doi.org/10.1161/CIRCIMAGING.109.913467.
43. Saito N, Kato S, Noritaka Saito N, NakachI T, et al. Distinction Between Precapillary and Postcapillary Pulmonary Hypertension by the Atrial Volume Ratio on Transthoracic Echocardiography. J Ultrasound Med.. 2018 Apr;37(4):891-896. doi: 10.1002/jum.14424. Epub 2017 Sep 29. PMID: 28960484.
44. Hatle L, Angelsen BA, Tromsdal A. Non-invasive estimation of pulmonary artery systolic pressure with Doppler ultrasound. Br Heart J 1981;45:157-165. doi: 10.1136/hrt.45.2.157.
45. Yock PG, Popp RL. Noninvasive estimation of right ventricular systolic pressure by Doppler ultrasound in patients with tricuspid regurgitation. Circulation 1984;Oct 70:657-662. doi: 10.1161/01.cir.70.4.657
46. Torbicki A, Skwarski K, Hawrylkiewicz I, et al. Attempts at measuring pulmonary arterial pressure by means of Doppler echocardiography in patients with chronic lung disease. Eur Respir J 1989; 2(9): 856–60. PMID: 2806512.
47. Naeije R, Torbicki A. More on the noninvasive diagnosis of pulmonary hypertension: Doppler echocardiography revisited. Eur Respir J 1995; 8(9): 1445–1449. PMID: 8575567.
48. Fisher MR, Forfia PR, Chamera E, et al. Accuracy of Doppler echocardiography in the hemodynamic assessment of pulmonary hypertension. Am J Respir Crit Care Med . 2009; Apr 1;179(7):615-621. doi: 10.1164/rccm.200811-1691OC. Epub 2009 Jan 22.
49. Rich JD, Shah SJ, Swamy RS, Kamp A, Rich S. Inaccuracy of Doppler echocardiographic estimates of pulmonary artery pressures in patients with pulmonary hypertension: implications for clinical practice Chest. 2011 May;139(5):988-993. doi: 10.1378/chest.10-1269. Epub 2010 Sep 23
50. Arcasoy SM, Christie JD, Ferrari VA, et al. Echocardiographic assessment of pulmonary hypertension in patients with advanced lung disease. Am J Respir Crit Care Med 2003; 167(5): 735–740. doi: 10.1164/rccm.200210-1130OC. Epub 2002 Dec 12.
51. Surinder J, et al. Diagnostic accuracy of echocardiography for pulmonary hypertension: a systematic review and meta-analysis. Heart 2011; 97:612e622. doi:10.1136/hrt.2010.212084.