

Effects of Low-Energy EM Radiation on Chronic Fatigue
The Effects of Low-Energy Electromagnetic Radiation (Rifetech®Plasma) in Patients with Fatigue An Observational Study
Harald Walach1,2, Viviane Ruof2, Ulrike Kukuk3
OPEN ACCESS
PUBLISHED: 31 October 2025
CITATION: Walach, H., et al., 2025. The Effects of Low-Energy Electromagnetic Radiation (Rifetech®Plasma) in Patients with Fatigue An Observational Study. Medical Research Archives, [online] 13(10). https://doi.org/10.18103/mra.v13i9.7024
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i9.7024
ISSN 2375-1924
ABSTRACT
Fatigue is a debilitating condition, often consequent on infections that persist. There are few treatment options, and patients frequently seek complementary medical treatment. One such treatment, a low-energy electromagnetic radiation emitted by RIFETECH®-Plasma, was used in this observational study. The device emits low frequency, low energy radiation modulated onto cold plasma. The frequency can be adapted according to therapeutic specifications. One hundred and thirteen patients with chronic fatigue were enrolled by 11 practitioners and treated for four weeks, with, on average, two sessions per week which lasted for two hours (median). Outcome was measured with the German version of the Fatigue Severity Scale (FSS) and the World Health Organization 5 Item Quality of Life Questionnaire (WHO-Quol-5) before and after treatment. Since this was a pilot-observational study, the protocol stipulated mainly a descriptive analysis reporting standardized mean differences, with orienting significance testing by robust non-parametric methods. The patients were initially severely fatigued (duration of fatigue 20.9 months on average; FFS sum: 50.05 ± 11.4 standard deviation (SD); mean: 5.57 ± 1,27 SD [healthy controls: 3.0; multiple sclerosis patients: 4.66]) and improved after treatment significantly. Improvement was 13.8 points (SD ±13.0) on the FSS and 8.57 (SD ± 8.4) on the WHO-Quol-5 scale (standardized mean difference 1.0). We conclude that treatment with individually adapted low-energy, low-frequency EM radiation using RIFETECH-Plasma® is a promising treatment option which should be studied further in controlled trials.
Keywords
Fatigue, Low-Energy Electromagnetic Radiation, RIFETECH®-Plasma, Chronic Fatigue, Complementary Medicine
0. Introduction
Fatigue is a common condition, accompanying depression and inflammatory diseases like rheumatoid diseases. It is seen as a long-term sequelae of infections. Long-COVID and other viral infections are often associated with fatigue. About 90% of all cancer patients report fatigue, either as a symptom of the disease or as a consequence of treatment. A review of epidemiological studies found that non-cancer related fatigue was reported in 25% to 35% of the populations studied. In addition, an unknown number of people without any known disease suffer from fatigue, perhaps due to generic stress of modern conditions of life under the permanent threat of crises. Most patients with chronic conditions, like multiple sclerosis, chronic pain or sleep disturbances, also report fatigue. A recent longitudinal observation study in 78,000 persons in the Netherlands documented severe fatigue in 18% and chronic fatigue in 13% of the surveyed persons. The more chronic conditions patients had, the more severe the fatigue was: the odds ratio for fatigue was 1.61 in one chronic condition and 5.50 with four conditions. Thus, fatigue is a pervasive problem, affecting many persons with and without a medical diagnosis.
Common wisdom attributes psychological diagnoses to fatigued patients, such as a psychosomatic conversion syndrome. A recent meta-analysis, which found that the personality trait of neuroticism is indeed associated with fatigue, seems to support such a classification. However, we find that the association (OR = 1.38 for fatigue and neuroticism) is too small to warrant such generalizations. We saw in a large clinical trial with 409 chronic fatigue patients that these patients feel frequently misclassified as psychological, when they themselves usually attribute their suffering to physical causes such as infections. A recent meta-analysis shows that fatigue is associated with autonomic dysregulation, which in itself is likely the consequence of a complex mal-adaptation process.
The common misclassification of fatigue as psychologically caused might also be due to the fact that treatment options are limited. Apart from support and cognitive behavior therapy there is little on offer for patients with fatigue. Hence, such patients are often searching in the field of complementary medicine. One treatment option are so called energy medicine interventions. One class of such techniques uses variable types of low-energy electromagnetic signals. Sometimes such signals are transferred to the body via electrodes and modulated onto very weak AC-currents, often also coupled with a feedback system, where the device records some kind of electromagnetic coupling, such as resistance, or capacitance. We showed in controlled trials and in a meta-analysis that such an intervention can be beneficial in increasing well-being and quality of life.
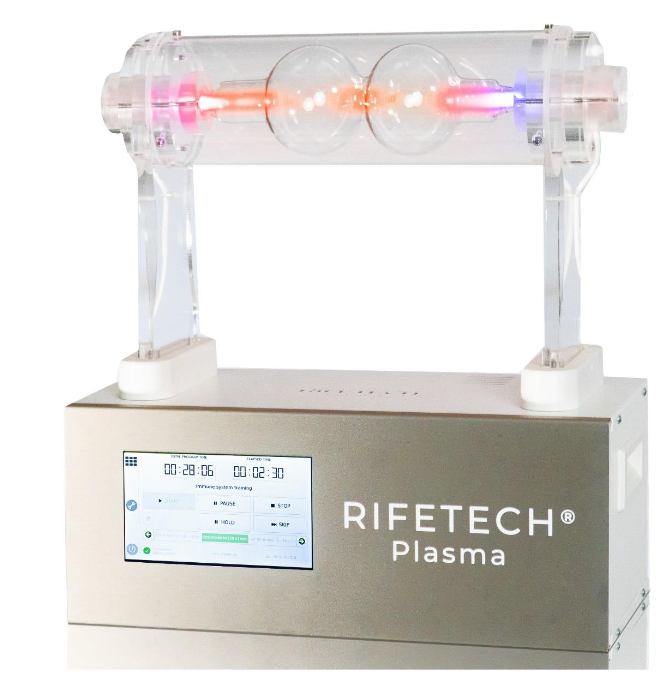
Another treatment option is offered by the novel energy medicine Rifetech Plasma (Figure 1). This is a device which generates a cold plasma, similar to a neon-light tube, which is slightly visible as light of reddish hue. Such a cold plasma is generated, when a gas in a vacuum tube is ignited using a high initial voltage. In the case of this device, the cold plasma radiates a low intensity red light which is barely visible under normal lighting conditions but can be clearly seen when it is dark. Electromagnetic radiations are modulated onto that plasma (potential range 10 µHz to 900 kHz; accurately adjustable to 2 decimals; insecurity ± 5 * 10-6). This is similar to long-range radio waves with a wavelength of several meters to some 100 meters, and thus they can easily penetrate fabric and bodily tissue of patients situated near the device. The original idea was developed by the engineer Royal Raymond Rife (1888-1971). He was the first to develop a light-microscope that could breach the Rayleigh-length, before the advent of electron-microscopy. With his microscope he could make visible small structures such as small bacteria and even viruses. He developed a treatment system, whereby he adapted electromagnetic radiations to the size of the microstructures he saw, such that the wavelength of the radiation would be in resonance as a multiple or fraction of the size of the structure. He seemingly was quite successful. However, as he treated cancer, even though successfully, without a medical license, he was put in prison and his work was confiscated by the FBI due to charges of the FDA. A recent reconstruction of his microscope showed that it indeed worked (project funded by the Fetzer-Franklin Fund; personal communication by Dr. Jan Walleczek, who was in charge of the project).
RIFETECH®-Plasma is a novel development adapting the original ideas of Rife. It was developed with the help of a EU-funded project (Projekt No CZ.01.1.02/0.0/0.0/20_319/0023173) during which the length of the RNA of the SARS-CoV-2 virus genome was measured. The device has a registration as a device for self-treatment in the area of wellness and fulfills the European safety standards (2014/30/EU and 2014/35/EU). It also has been registered as a medical device of risk class 1 in the German medicinal product information database (registration no DE/CA73/99 297351).
The device uses the fraction between the speed of light divided by the precise length of the DNA/RNA of a known pathogen (virus, bacteria, fungus, parasite) to determine a therapeutic wavelength, as well as the size of other structures, such as the diameter. Following the principle of coherent excitation, electromagnetic frequencies that are in direct resonance with biological structures, because their wavelengths are either a multiple or direct ratio of the size of the biological structure can elicit standing waves that can lead to a resonance catastrophe, destroying the pathogen, or important parts of it.
The principle can be experienced in a geometric building such as in a domed crypt, or an octagonal church. If one stands exactly in the center of the building and starts humming softly notes on a sliding scale up and down, there will be one frequency, where the soft note will suddenly reverberate and become amplified. This is the frequency, where the wavelength is in resonance with the height of the building, and thereby the sound is amplified by the resonant frequency. This same principle is applied by the device, only with electromagnetic waves and not with sound waves.
While this generic idea is geared towards targeting pathogens, there are also other frequencies implemented, derived from experience of practitioners and from other devices, that serve other purposes, like regulation or supporting harmonization, such as the well-known Schumann frequency, or the Solfeggio frequencies which are derived from sequences in Gregorianic chants and correspond to the scale originally devised by the Benedictine monk Guido d’Arezzo (10th century). Here, they are not used as sound, but as frequencies modulated onto the plasma. In the same sense there are various other sequences of frequencies, apart from the ones corresponding to pathogens, that stem from experiences of practitioners with other types of bioenergy apparatuses.
While in conventional medicine standardization is an important principle, complementary medical approaches normally use individualization as a therapeutic option. This means: there is no standard protocol, but the treatment protocol is adapted according to patients’ concrete diagnostics, as well as to the severity of the symptoms and the patients’ regulatory capacity. Also, since there is not much experience with this device available, a fixed and standardized protocol for treatment could not be formulated. Rather, practitioners were instructed to document their treatment protocols carefully and use the protocol that would suggest itself as the most suitable after careful diagnosis and revision of the patients’ symptom and severity of the situation. For instance, if the patient came in with a known immunological diagnosis and documented serology of a past infection with a certain infectious agent, such as SARS-CoV-2, meningitis, or Lyme-Borreliosis, the frequencies corresponding to these according pathogens were chosen. After several treatments targeting these pathogens, normally generic frequencies for harmonization or detoxification were used. The protocols have been documented in the statistical report on the study and are available on request.
This device has never been studied before. Thus, no data were available and we decided to start the research program with an open label observational study. As the patients had all been suffering for two years without remission (see below, Results), a spontaneous improvement was quite unlikely and a design, where patients served as their own control seemed sufficient to find out, whether there would be any effect at all, and if so, what size it would have. Observational studies are generally considered sufficient as a first step, if patients are seriously suffering from a disease, where spontaneous remission is unlikely. Such a study was deemed necessary as a first step for designing further studies and conduct power calculations for controlled studies.
1. Method
DESIGN
Eleven practitioners who were familiar with using the device recruited patients with fatigue (ICD Code G93.3) into the study. The design of the study was an open-label, prospective documentation study of four weeks duration. The study protocol was formulated in advance, and registered with the German clinical trials register (DRKS00031476; https://drks.de/register/de/trial/DRKS00031476/preview), after the ethics committee of the Diploma Technical University/Natura Akademie had cleared it (EB 1048/2023). The study was conducted between 11th April 2023 and 3rd August 2023.
PATIENTS
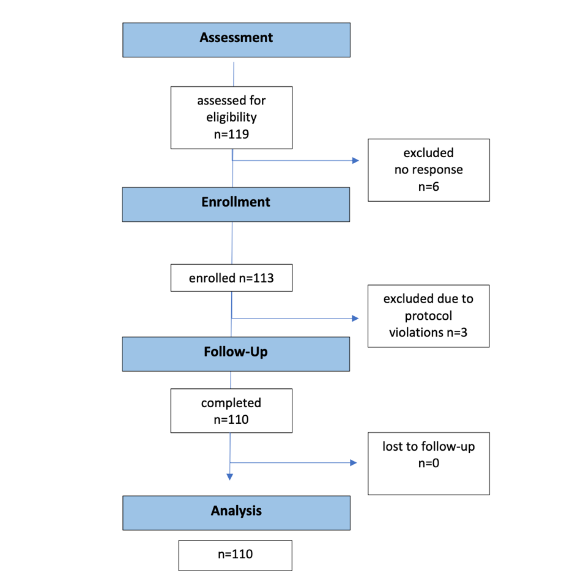
The protocol called for the enrollment of 100 patients with a potential over-recruitment of 10% to account for potential drop-outs. It was anticipated that 10 practitioners should recruit 10 patients each. In the end, 11 practitioners recruited 113 patients from which 110 valid cases were analyzed (see figure 2). Non-valid cases were the ones excluded due to a lack of response after the first assessment and protocol violations.
The single inclusion criterion was the presence of fatigue, ICD Code G93.3. This is the overall category that is present in many diseases and is prevalent in general practice; according to informal reports of our practitioners about 50% to 75% of all patients suffer from fatigue. We applied the following exclusion criteria:
- Age < 18 years without parental consent
- Lack of German knowledge that precludes understanding written information and filling in questionnaires
- no email-address
- Life-threatening condition
- Condition immediately after surgery, i.e. up to 4 weeks after surgery
- Systemic treatment that can induce fatigue (e.g. cytostatic drugs or anti-histaminics)
- Beginning of parallel treatment with another therapist that is intended to treat fatigue
- Characteristics of patient or disease that make it unlikely that changes could be observed during the first four weeks of treatment
OUTCOME MEASURES
As outcome measures we defined the Fatigue Severity Scale (FSS) in its validated German version as the primary outcome and the German version of the World Health Organization-Quality of Life Questionnaire in its 5-item version (WHO-Quol-5). The FSS is a 9-item self-report measure whose items are answered in a 7-point Likert format, with three negative, three positive and one neutral answering options. It assesses fatigue in various dimensions. The validation study was conducted with 454 healthy participants, 188 patients with multiple sclerosis, 235 patients with recent stroke, 429 patients with sleep-wake-disorders. Its internal consistency is high (Cronbach’s α = 0.93) and re-test-reliability analysis showed that the measure is stable over time for at least three weeks. The WHO-Quol-5 is a short 5-item questionnaire that assesses general well-being, energy, positive mood, lack of anxiety, and refreshment through sleep. It is well validated in many languages and used often.
PROCEDURES
The questionnaires were mounted on an internet-based survey platform (Social Science Survey https://www.soscisurvey.de/en/index). We instructed patients to create unique identifiers that did not breach anonymity. After the practitioners had ascertained inclusion and exclusion criteria, patients were invited to participate and, if willing, gave written, informed consent. Practitioners filled in Case Report Forms, and they then notified the study center, by sending the email address of the participating patient. Within a few days the patient received a unique link to the questionnaire form via email. If no response was registered, patients received up to three reminders within a couple of days, and if still no response occurred, patients were phoned by the clinic and reminded to fill in the questionnaires. Four weeks after the first questionnaire had been registered, patients received another mail with a link to the follow-up questionnaire. Practitioners also received a link to a post-treatment questionnaire, in which the assessment of the success of the treatment, potential adverse events, and the treatment regimen were documented. Through close monitoring we were able to avoid any losses to follow-up (see Figure 2, Trial Flow).
2. Results
Eleven practitioners recruited 119 patients. Six patients could never be reached and did not fill in any questionnaires. These were assessed as having withdrawn their consent. Another three patients were withdrawn by the doctors immediately after enrollment as protocol violations. We report initial data for all 113 patients and outcome data for the final sample of 110 patients. Table 1 shows the demographic data.
| Variable | Mean (Standard Deviation) | Frequency (Percent) |
|---|---|---|
| Age | 49.5 (13.7) | |
| Gender | female 95 (84%) | |
| Education | Basic 10 (8.8%) | |
| GCSE 54 (47.8%) | ||
| A-Level 49 (43.4%) | ||
| Training | none 9 (8%) | |
| Professional 64 (56.6%) | ||
| University 40 (35.4%) | ||
| Income | < 15,000 23 (20.3%) | |
| 15-25,000 20 (17.7%) | ||
| 25-40,000 31 (27.4%) | ||
| 40-60,000 24 (21.2%) | ||
| >60,000 15 (13.3%) | ||
| Duration of fatigue in months | 20.9 (31.9) | |
| Fatigue Severity Scale | Sum 50.05 (11.4) | |
| Mean 5.57 (1.27) | ||
| WHO-Quol5 | Sum 7.73 (4.3) |
Patients in this study had been fatigued for nearly two years before entering this study and their FFS mean score was clearly more severe than that of any other patient group documented in the validation study, as documented by the 95%-confidence intervals that do not overlap. This comparison is shown in Table 2.
| Means (Standard Deviations) and [95% Confidence Intervals] | This Study | Healthy | Multiple Sclerosis Patients | Stroke Patients | Sleep-Wake Disturbance |
|---|---|---|---|---|---|
| n = 113 | 5.57 (1.27) [5.33 5.80] | 3.0 (1.08) [2.9 – 3.1] | 4.66 (1.64) [4.42 – 4.89] | 3.90 (1.85) [3.66 4.14] | 4.34 (1.64) [4.19 4.50] |
In 109 out of the 110 patients with full data doctors indicated that other diagnoses were present, and in 77 cases these were mentioned specifically. The supplement of the original report describes these (available on request). Fifty-seven of the patients came with some medication already prescribed, and 53 were unmedicated. Nineteen of those with medication took some naturopathic product or supplement. Cortisone or psychoactive drugs had been prescribed for six patients.
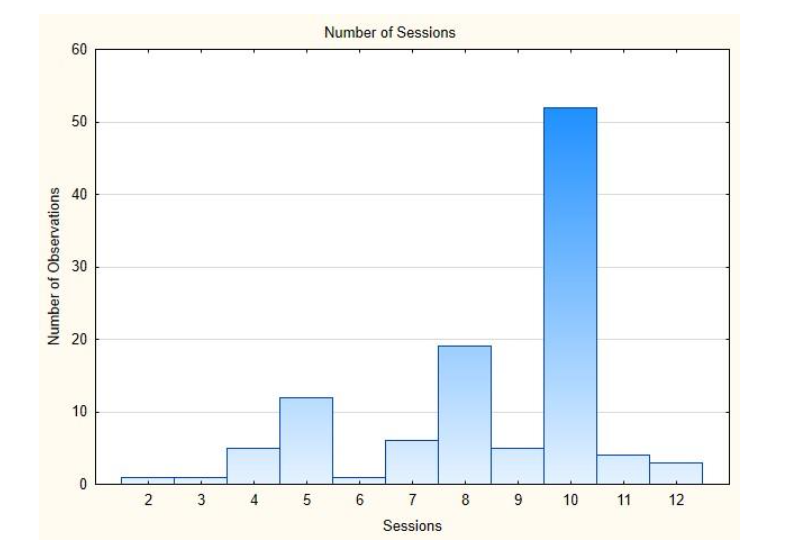
Most of the clinics treated between 8 and 14 patients. Only one clinic treated only one patient, one four patients, and one 19 patients. Table 3 describes the number and length of treatments. Figure 3 shows a histogram of the number of sessions used.
| Mean, Standard Deviation (SD), Median, Minimum and Maximum | |
|---|---|
| No. of treatments | 8.5 2.2 10 2 12 |
| Duration in Minutes | 107.9 27.8 120 30 215 |
Doctors were free to choose individual programs. Except in two cases, doctors described the program sequences they used; they are documented in an Appendix which is available on request. The most frequent programs used were combinations of harmonizing and detoxifying programs, in addition to individual programs which were meant to target specific pathogens, depending on the individual situation or diagnostic.
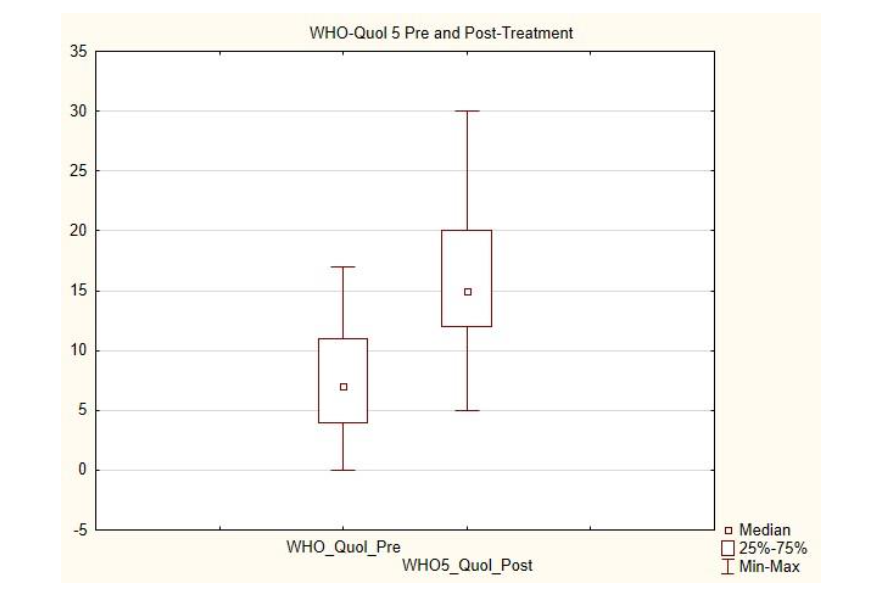
In order to assess improvement, we calculated pre-post differences of the main outcome, the FSS, and the secondary outcome, the WHO-Quol-5. Orienting statistical tests (Wilcoxon tests) were also conducted. The differences were large (standardized mean difference 1.0) and highly significant (p < 0.0001). These data are presented in Table 4. Figures 4 and 5 show box plots of these data with median, interquartile range and the range of data.
| 110 Patients | Wilcoxon Test |
|---|---|
| FSS 13.8 (13.0) | Z = 9.09; p < 10-6 |
| WHO Quol 8.57 (8.4) | Z = 7.8; p < 10-6 |

Independently of patients, doctors assessed the success of the treatment. The results are given in Table 5.
| Frequency | Percent |
|---|---|
| Successful | 71 64.5 |
| Partially successful | 31 28.2 |
| Little success | 6 5.5 |
| Aggravated | 1 1 |
| Missing | 1 1 |
In 50 patients, doctors did not use any additional treatment, but only the Rifetech-treatment. In all other cases, some form of other treatment was deemed useful by the practitioner. Most frequently, these were vitamins and minerals (40%), other treatments (32%), other supplements (19%), homeopathy (6.4%), psychotherapy (2%), acupuncture (1%). Most frequently vitamin D and B-vitamins were prescribed in addition. A complete list of additional treatments is available on request.
An analysis of the patients with additional treatment compared with those without additional treatment shows that the patients with additional treatment had better results than those without. Although the effect size is diminished in patients without additional treatment, it is still sizeable and significant. A comparison of those patient groups is shown in Table 6.
| Mean (SDs) [Effect Size d], Wilcoxon Test of Significance of the change (z-score, p-value) | Only Rifetech (n= 50) | Additional Treatments (n = 59) | Wilcoxon Test Only Rifetech; Z, p-value | Wilcoxon test Additional Treatment, z, p |
|---|---|---|---|---|
| Fatigue Severity Scale Difference | 9.62 (11.0) [0.87] | 17.4 (13.7) [1.27] | 4.9; p = 1*10-5 | 6.3; p < 1*10-5 |
| WHO5-Quol Difference | 6.43 (8.45) [0.76] | 10.19 (8.45) [1.2] | 4.6 p = 4*10-5 | 6.7 p < 1*10-5 |
Fifty-seven patients came into the study with some medication. These patients were more severely ill (FFS Sum 51.88 (SD 10.6) than those without (FFS Sum 48.6 (SD 12.4), but the difference was not significant. Those who were more severely ill profited more (difference 15.0 [SD 13.7]), compared with those without medication who were less severely compromised (difference 12.4 [SD 12.3]). But these differences were not significant.
We intended to separate adverse reactions from aggravations, as the phenomenon of transitory aggravations of existing symptoms is quite common in any complementary treatment that induces regulatory self-control. Adverse reactions were meant to be novel symptoms that the doctor attributes causally to the treatment. However, we suspect that this semantic separation was neither understood nor handled consistently by the doctors. Table 7 shows how these categories were reported.
| Yes | No | |
|---|---|---|
| Aggravation | 26 (23.6%) | 82 (74.5%) |
| Adverse Events | 26 (23.6%) | 83 (75.4%) |
| Healing of Other Symptoms | 74 (67.3%) | 35 (31.8%) |
We can see: A quarter of the patients reported aggravation and/or adverse events, and two third of the patients experienced a generalization of healing, where other symptoms had been healed as well. Aggravations and Adverse Events are positively associated (Spearman’s rank correlation coefficient ρ = .39; p < 0.05). Aggravation is also associated with a larger difference in WHO-Quol-5 (ρ = -.22; p > 0.05). This seems to indicate that an initial aggravation is a positive predictor for improvement.
In a regression analysis, predicting therapeutic success (difference score in primary outcome), we saw that three variables can explain 21% of the variance. Patients with a higher baseline severity of fatigue (beta = .27) and longer duration of treatment (beta = 0.16) improve more. Also, patients treated by one particular doctor improved more. When inspecting the patients of this doctor, we saw that they were mainly less severely ill and had all some additional treatment, mostly vitamins.
3. Discussion
This observational study in 110 patients who had been severely fatigued since nearly 2 years showed that on average 8 sessions of an energy medicine treatment with a new energy medicine device (RIFETECH®-Plasma) which lasted roughly 2 hours each could improve those patients markedly. The improvement in the Fatigue Severity Scale, measured at the beginning and after four weeks was more than a standard deviation and was highly significant. Patients who received additional complementary treatment, mainly vitamin D and B-vitamins, improved more than those without additional treatment, who also improved clearly and significantly.
The decisive question is of course: Is this treatment causally due to the treatment itself or the consequence of some non-specific treatment factors such as the long time spent in silence with a novel device that looks fascinating and promising, and thus is likely to engender a large placebo effect? This question can decisively only be answered by a placebo-controlled study using an inactivated device as a control. Our present study was meant to inform such a controlled study and gives a few interesting hints. The fact that the patients had been ill for nearly two years and were severely fatigued, judging from the comparison with other patient groups, speaks at least against a measurement artifact and against spontaneous improvement. It is quite acceptable, especially as a first step in a research program, to determine potential effects using an observational pre-post-design, in which patients are their own controls. This is especially so, when the condition is long-standing and severe and therefore unlikely to change by accident or through spontaneous remission. This situation was given here, and therefore we are confident that we can exclude artifacts or spontaneous remission as explanation for our data.
Placebo effects cannot be ruled out, of course, as they are quite powerful, work also when given openly, and explain the largest amount of variance in clinical trials. But for patients this question might be irrelevant. They want to be healed, and the means of healing are quite irrelevant, as long as they are reliable, safe and come at manageable costs. For patients it is relevant, how large the full effect of a treatment will be, because this determines whether they have a chance of relieving their symptoms.
For scientific purposes it is certainly important to know, whether such a device and its rationale can deploy therapeutic effects independent of expectation and hope installed by convinced practitioners. To study this, basic research set-ups with defined experiments using only pathogens and controls might be best suited. However, currently it is unclear whether the purported effect of inducing a resonance catastrophe in defined pathogens is sufficient to explain therapeutic effects of such an energy device. Perhaps it is the complex interaction with a living system that is decisive. Currently, we do not know, since to our knowledge this was the first formal study of such a device in patients.
The effects we observed were short term and visible after 4 weeks. We do not know how long-lived they are. For that, follow-up observations would be necessary. However, we think that a time investment of roughly 8 hours distributed over 4 weeks would seem parsimonious considering the fact that otherwise there was little that has helped the patients so far. Our patients have been suffering from fatigue for nearly two years, hence were quite ill. Compared with this, a short 4 week-treatment period, with about 2 time investment per week seems a comparatively cost-effective investment, which would amount to about 3.200 treatment costs if we monetarize an hour with 200. As we did not see any severe side-effects and initial aggravations are usually associated with improvement, we would also deem this treatment as safe.
Future studies should use controls in well-defined patient groups to study whether the effects observed by us are explainable by spontaneous improvements, by placebo-effects, and whether they are specific. Also, it might be interesting to learn, whether other patient groups would also benefit. Informal observations report good effects in other chronic conditions such as headaches and migraines and chronic pain conditions. An interesting field seems to us the treatment of infectious diseases. As the therapeutic principle is expressly geared towards addressing bacterial, viral or parasitic pathogens, as well as fungi, this might be an option for the treatment of infections where antibiotics are either not indicated or ineffective due to resistance. This could then also foster a method of mitigating antimicrobial resistance, which has grown into a major problem.
4. Conclusion
We conclude: A low-energy and low-frequency electromagnetic treatment as delivered by RIFETECH®-Plasma can improve severely fatigued patients in 8 sessions at 2 hours each over 4 weeks to a considerable degree. Improvements were sizeable (SMD = 1.0) and statistically significant. Further research to determine whether these are placebo effects and also how sustainable these effects are is warranted.
Declaration of Authorship: HW conceived the study, developed the design, organized the study and secured funding. He analyzed the data and wrote the first draft. VR helped with study organization and logistics. She programmed the data capture database and helped with editing the text and interpretation of the study. UK ran the study logistics and collected the data. She helped with interpreting the results and contributed to writing.
Conflict of Interest Statement: HW receives consultant fees from the company that sells the device in Germany and another company active in the energy medicine field. The other authors have no conflict of interest.
Funding Statement: The study was funded by Holistic Medicine GmbH, Berlin.
References
- van Praag HM, de Kloet R, van Os J. Stress, the Brain, and Depression. Cambridge: Cambridge University Press; 2004.
- Davies K, Dures E, Ng W-F. Fatigue in inflammatory rheumatic diseases: current knowledge and areas for future research. Nature Reviews Rheumatology. 2021;17(11):651-664.
- Smith AP. Twenty-five years of research on the behavioural malaise associated with influenza and the common cold. Psychoneuroendocrinology. 2013;38(6):744-751.
- Petersen I, Thomas JM, Hamilton WT, White PD. Risk and predictors of fatigue after infectious mononucleosis in a large primary-care cohort. Quarterly Journal of Medicine. 2006;99(1):49-55.
- Lopez-Leon S, Wegman-Ostrosky T, Perelman C, et al. More than 50 long-term effects of COVID-19: a systematic review and meta-analysis. Scientific Reports. 2021;11(1):16144.
- David A, Hausner D, Frenkel M. Cancer-Related Fatigue Is There a Role for Complementary and Integrative Medicine? Current Oncology Reports. 2021;23(12):145.
- Billones R, Liwang JK, Butler K, Graves L, Saligan LN. Dissecting the fatigue experience: A scoping review of fatigue definitions, dimensions, and measures in non-oncologic medical conditions. Brain, Behavior, & Immunity – Health. 2021;15:100266.
- Kuppuswamy A. The Neurobiology of Pathological Fatigue: New Models, New Questions. The Neuroscientist. 2022;28(3):238-253.
- Goërtz YMJ, Braamse AMJ, Spruit MA, et al. Fatigue in patients with chronic disease: results from the population-based Lifelines Cohort Study. Scientific Reports. 2021;11(1):20977.
- Stephan Y, Sutin AR, Luchetti M, Canada B, Terracciano A. Personality and fatigue: meta-analysis of seven prospective studies. Scientific Reports. 2022;12(1):9156.
- Walach H, Bösch H, Lewith G, et al. Efficacy of distant healing in patients with chronic fatigue syndrome: A randomised controlled partially blinded trial (EUHEALS) Psychotherapy and Psychosomatics. 2008;77:158-166.
- Güthlin C, Anton A, Kruse J, Walach H. Subjective concepts of chronically ill patients using distant healing. Qualitative Health Research. 2012; 22:320-331.
- Nelson MJ, Bahl JS, Buckley JD, Thomson RL, Davison K. Evidence of altered cardiac autonomic regulation in myalgic encephalomyelitis/chronic fatigue syndrome: A systematic review and meta-analysis. Medicine. 2019;98(43).
- Hyland ME. Extended network learning error: A new way of conceptualising chronic fatigue syndrome. Psychology and Health. 2001;16:273-287.
- Hyland ME. The Origins of Health and Disease. Cambridge: Cambridge University Press; 2011.
- Bazelmans E, Prins J, Lulofs R, van der Meer J, Bleijenberg G. Cognitive Behaviour Group Therapy for Chronic Fatigue Syndrome: A Non-Randomised Waiting List Controlled Study. Psychotherapy and Psychosomatics. 2005;74(4):218-224.
- Greeson JM, Rosenzweig S, Halbert SC, Cantor IS, Keener MT, Brainard GC. Integrative Medicine Research at an Academic Medical Center: Patient Characteristics and Health-Related Quality-of-Life Outcomes. The Journal of Alternative and Complementary Medicine. 2008;14(6):763-767.
- Schmieke M. Quantum entangled Frequencies to promote Coherence in Bioenergetic Systems. Dev Sanskriti Interdisciplinary International Journal. 2021;18:10-33.
- Walach H, Marmann P. Bioenergy Treatment for Improving Well-Being A Meta-Analysis. Complementary Medical Research. 2023;30(3):258-269.
- Walach H, Marmann P. Self-treatment to improve mental and physical health using two bioenergetic devices: A randomized controlled trial. Journal of Psychiatry and Psychiatric Disorders. 2021;5(4):107-119.
- Lynes B. The Cancer Cure That Worked! Fifty Years of Suppression. Lake Tahoe: Biomed Publishing; 2011, orig. 1987.
- Fröhlich H, Kremer F. Coherent Excitation in Biological Systems. Berlin: Springer; 1983.
- Black N. Why we need observational studies to evaluate the effectiveness of health care. British Medical Journal. 1996;312:1215-1218.
- Valko PO, Bassetti CL, Bloch KE, Held U, Baumann CR. Validation of the Fatigue Severity Scale in a Swiss Cohort. Sleep. 2008;31(11):1601-1607.
- Sischka PE, Costa AP, Steffgen G, Schmidt AF. The WHO-5 well-being index validation based on item response theory and the analysis of measurement invariance across 35 countries. Journal of Affective Disorders Reports. 2020;1:100020.
- Topp CW, Østergaard SD, Søndergaard S, Bech P. The WHO-5 Well-Being Index: A Systematic Review of the Literature. Psychotherapy and Psychosomatics. 2015;84(3):167-176.
- World Health Organisation. Mental health – a state of well-being Geneva: World Health Organization; 2014.
- Lewith G, Jonas WB, Walach H, eds. Clinical Research in Complementary Medicine: Principles, Problems Solutions. 2nd revised edition ed. Edinburgh, London: Churchill Livingstone; 2010.
- Walach H. Placebo effects in Complementary and Alternative Medicine: The selfhealing response. In: Colloca L, Flaten MA, Meissner K, eds. Placebo and Pain: From Bench to Bedside. Amsterdam: Elsevier-Academic Press; 2013:189-202.
- von Wernsdorff M, Loef M, Tuschen-Caffier B, Schmidt S. Effects of open-label placebos in clinical trials: a systematic review and meta-analysis. Scientific Reports. 2021;11(1):3855.
- Walach H, Sadaghiani C, Dehm C, Bierman DJ. The therapeutic effect of clinical trials: understanding placebo response rates in clinical trials – A secondary analysis. BMC Medical Research Methodology. 2005;5:26.
- Walach H, Loef M. Using a matrix-analytical approach to synthesizing evidence solved incompatibility problem in the hierarchy of evidence. Journal of Clinical Epidemiology. 2015;68:1251-1260.
- European Centre for Disease Prevention and Control. Antimicrobial Resistance Surveillance in Europe 2016. Annual Report of the European Antimicrobial Resistance Surveillance Network (EARS-Net). Stockholm: ECDC;2017.
- Hansen G. Antibiotic resistance. In: Halabi SF, Gostin LO, Crowley JS, eds. Global Management of Infectious Disease after Ebola. Oxford: Oxford UP; 2017:87-97.
- Walach H. Complementary Medicine: A Serious Option as We Are Facing the Problem of Bacterial Antibiotic Resistance. Complementary Medicine Research. 2017;24(3):132-134.