






Efficacy of GSPECT Filters on LVEF Evaluation in CAD
Efficacy of 3D GSPECT Reconstruction Filters on LVEF Evaluation in the Presence of Low to Intermediate Perfusion Defects – Correlation with ECHO
Michael Masoomi, PhD, MRCP(Lon) *1,2, Iman Al-Shammeri, MD¹, Latifa Al-Kandari, MD³, Hany Elrahman, MPH¹, Jehan Al-Shammeri, PhD⁴, Osama Raqab, MD¹, Sherif Arafit, MD⁵
- Department of Nuclear Medicine, ADAN Hospital, KUWAIT.
- Department of Research and Innovation, Portsmouth University Hospital, U.K.
- Department of Radiology, ADAN Hospital, KUWAIT.
- Department of NM, Faculty of Medicine, KW University, KUWAIT.
- Dabbous Cardiac Center, ADAN Hospital, KUWAIT.
OPEN ACCESS
PUBLISHED: 31 July 2024
CITATION: Masoomi, M., Al-Shammeri, I., et al., 2024. Efficacy of 3D GSPECT Reconstruction Filters on LVEF Evaluation in the Presence of Low to Intermediate Perfusion Defects – Correlation with ECHO. Medical Research Archives, [online] 12(7).
https://doi.org/10.18103/mra.v12i7.5534
COPYRIGHT: © 2024 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v12i7.5534
ISSN 2375-1924
ABSTRACT
Background: LVEF is a reliable diagnostic and prognostic value in coronary artery disease. Several modalities including ECHO, GSPECT, cMRI and RNV can assess the LVEF. Filtering contributes to the variation of LVEF with influence on spatial resolution and statistical noise in the reconstructed images. The authors investigated the impact of Wiener and Butterworth filters variation for accuracy of LVEFs in CAD pts.
Methods: Scans of 21 patients; 14 males and 7 females, 25–76 years old, with suspected CAD who underwent the 99mTc Myoview GSPECT using QPS and QGS were reconstructed with Wiener filter based on the outcome of an earlier SPECT-CT optimisation of two chest phantoms. The patient results compared to the previous reports using a standard Butterworth filter and the ECHO for comparison.
Results: 47%, 29% and 24% of pts reported normal, equivocal (EV) and having CAD based on LVEF respectively and prior to modified filtering. A good correlation between ECHO and the calculated LVEF with Wiener and Butterworth (r² = 0.876 & r² = 0.847) and for small heart (r² = 0.951 & r² = 0.933) was observed. To achieve less variation in LVEF measurement, we established mean cutoff value for Butterworth (0.26 +/-0.09) and a mean point value for Wiener (4.9 +/-1.19) in correlation to ECHO. Patients with LVEF of <40 showed greater variation in point-setting for Wiener, but less fluctuation in cutoff for Butterworth. No remarkable difference noticed for LVEF between two filter techniques for normal cases after adjusting parameters.
Conclusions: There was a good agreement between LVEF derived from GSPECT and ECHO after adjusting parameters with 10% higher accuracy in equivocal cases at this stage. Mean percentage LVEF error for Wiener and Butterworth against ECHO were 2% and 6% respectively post correction, together with more elevated qualitative acceptable images. The accuracy of intermediate CAD reporting for both rest and stress studies were elevated, though more patients’ images needed to be assessed for equivocal and smaller size hearts to reach a more statistically viable result.
Keywords: LVEF, GSPECT, ECHO, Perfusion defect, Multifunctional filters, Echocardiography.
1. Introduction
Myocardial perfusion imaging (MPI) using single photon emission computerized tomography (SPECT) 99mTc-sestamibi is an accurate noninvasive means of detecting coronary artery disease (CAD) and assessing the severity of perfusion abnormalities in patients with coronary stenosis. Gated SPECT (GSPECT) offers the possibility of obtaining additional functional information from perfusion studies, including wall motion and calculation of left ventricular ejection fraction (LVEF). Feasible, accurate, and reproducible assessment of left ventricular ejection fraction (LVEF) is an important objective of non-invasive cardiac imaging. The calculation of LVEF relies upon the identification of the endocardial surface, which will be affected by the spatial resolution and statistical noise in the reconstructed images. Left ventricular function indicators including left ventricular volumes (LVVs) and ejection fraction (LVEF) are powerful and reliable in terms of their diagnostic and prognostic value, especially in coronary artery disease¹–³. Moreover, current practice guidelines use LVEF thresholds for decision making in different clinical scenarios, such as the recommendation regarding device implantation or pharmacologic therapy in patients with heart failure⁴–⁵ and the recommendation for valve replacement in patients with severe valvular heart disease. Left ventricular ejection fraction is also a common enrolment criterion and/or end point for clinical trials⁶–⁷.
Nowadays, several modalities including echocardiography (ECHO), gated myocardial perfusion single photon emission tomography (GSPECT), cardiac magnetic resonance imaging (cMRI), and radionuclide ventriculography (RNV) are available for the assessment of LVVs and LVEF. Much discrepancy in selection of proper filter and its parameters for individual cases exists and concerns have been raised about the different findings in particular situations, such as in the presence of perfusion defects or in patients with small heart⁸. Low-pass filters smoothen the image, obscure the significance of small lesions, and reduce the sensitivity of the technique⁹–¹⁰. Restoration filters, on the other hand, enhance the image contrast, exaggerate artefacts at certain frequencies, and reduce the specificity of the technique¹¹–¹².
In the State of Kuwait, CHD is the major cause of morbidity and mortality and CVDs are estimated to cause 46.0% of all mortalities¹³–¹⁴. A study conducted by the MOH-KW in cooperation with WHO in 2006 and published by WHO in 2008, showed the incidence of heart diseases among the 2,280 Kuwaiti participants was 2.9%, though it did not exceed 15% among women in Kuwait. The State of Kuwait has witnessed rapid economic and sociodemographic changes during the last four decades. The major transitions in the developing societies have had apparent influences on behavioural, social, and lifestyle patterns¹⁵. As a consequence of these dramatic changes in the State of Kuwait, the prevalence of hypertension is 25.3%, diabetes 23.3%, dyslipidemia 70.3%, obesity 48.2% and smoking 17.8%¹⁶–¹⁷.
The earlier study by the author, Masoomi M et al.¹⁸ of a chest phantom and reanalyzing and re-evaluation of 92 male and female patients (41–77 years old) with suspected CAD, showed that the Wiener and Butterworth filters could produce results with the highest contrast for both cold and hot spheres and for the patient data it produced elevated improvement in diagnostic accuracy. The processed images were consistent with angiography results and correlated well with the CT-Angio and angiography results (r=0.79) and were statistically significant (P<0.001). Sensitivity of the Wiener filter (0.96) suggested a high probability that Wiener filter will correctly diagnose CAD patient in comparison to the Butterworth with a sensitivity of 0.69. In this study, the authors addressed the impact of Wiener and Butterworth filters variation on quantitative accuracy of LVEFs in CAD patients and the correlation between 3D GSPECT and ECHO in the evaluation of left ventricular end-diastolic volume (EDV), end-systolic volume (ESV) and LVEF in the presence of perfusion defect and small hearts was assessed. The ECHO is a routine and widely used noninvasive modality for this purpose.
2. Methods
2.1. STUDY DESIGN
This retrospective study was undertaken during the period of 2022 with selection of 21 adult patients with CAD. Individuals were 25 years old or older, of either sex (male or female), any nationality (Kuwaiti nationals, non-Kuwaiti Arabs, or non-Kuwaiti non-Arabs).
2.2. PHANTOM STUDY
Due to variation of imaging system structure and to acquire statistically reliable and acceptable images, the optimized activity was calculated as follows (Equation 1).
The investigation initiated by performing various SPECT-CT scans of a NEMA body phantom (Figure 1) having hot and cold inserts (9.5–37 mm). Data acquired on GE 670 PRO SPECT/CT: 360°, 64 frames, 60s, 128, IEGP with CT attenuation (120 kV & 170 mA).
Equation (1)
A = (15 Kc/s ÷ 5600 (Kc/s)/mCi) × (1/0.4) = 2250 mCi
The images were reconstructed with FBP and ITERATIVE OSEM utilizing Butterworth, and Wiener filters (Equation 2). The image contrast [C = (RO−R1)/R0 ×100] where R0 and R1 are accumulated counts in a defined ROI over the mid-slice of inserts as well as on the background, was calculated for each set of the reconstructed image of the phantom utilizing the stated filters (Wiener and Butterworth), to assess absolute nearness of the inserts quantitatively and qualitatively. The selected filters were chosen based on the outcome of the previous study¹⁸, for image optimization of various SPECT-CT scans of a NEMA body phantom with hot and cold inserts.
Equation (2)
B(f) = 1 / (1 + (f/fc)²ⁿ)
W(f) = MTF⁻¹ × (MTF² / (MTF² + N/O))
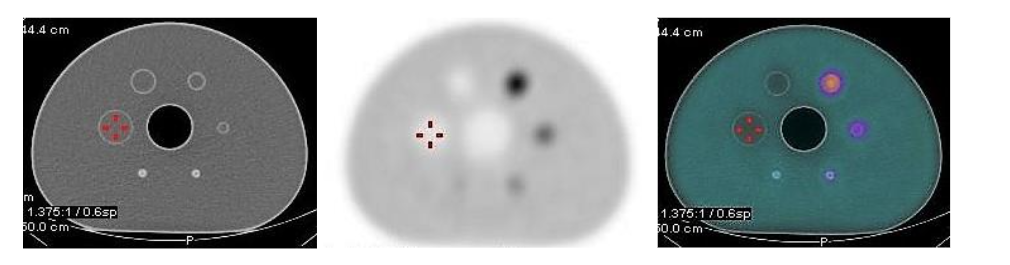
Figure 1: SPECT–CT images (Transaxial) of NEMA phantom for optimization of patient cardiac imaging
2.3. PATIENTS STUDY
In this study, we retrospectively selected 21 patients, 14 males and 7 females, age 25–76 years old, with known or suspected CAD and have had a history of reduced left ventricular EF and sinus rhythm on electrocardiogram. The patients were referred from the specialized Dabbous Center, a local large Cardiovascular Center, for gated SPECT-CT MPI imaging (predominantly 99mTc-Tetrofosmin GSPECT) due to clinical indication. A Consent form had been signed and obtained as part of the routine clinical study, as well as the ethical approval from the institution, though the reprocessing of patient data was approved by the department as part of the optimization. The patient’s ergonomic data had been recorded and their body mass indexes had been calculated.
Patients had either a treadmill or pharmacological stress. Physical stress was undertaken according to Bruce protocols. For pharmacological stress, patients had intravenous infusion of Persantin (14 mgkg⁻¹ min⁻¹) and 99mTc-Tetrofosmin were injected at 6 mins.
α conditionedified patients underwent dobutamine (starting dose of 10 mg·kg⁻¹·min⁻¹, increased at 3-minute intervals to a maximum of 50 mg kg⁻¹ min⁻¹). Regardless (0.4 mg) will be injected rapidly into the IV line over 10 seconds. Patients scheduled for rest imaging had been instructed to refrain from caffeine-containing beverages for at least 24 hours before the test and had received a dose of 99mTc-Myoview (standard, 740 MBq; but 1000 MBq for patients >100 kg). Both stress and rest SPECT images were acquired 45 to 60 minutes after tracer injection with 24-hour time delay between the stress and rest studies.
Images were acquired on GE 670 PRO SPECT/CT; RAO to LPO (180Ø), 64 frames, 25s, 64×64, LEHR with CT attenuation (120 kV & 50 mA) and reproduced utilizing FBP and ITERATIVE OSEM reconstructions with modified Wiener & Butterworth filters. Quantitative and qualitative evaluation was carried out using Cedars Sinai QGS and QPS. The post modified filter implementation was carried out on 2 ways; a): to match the calculated LVEF% for both Butterworth and Wiener filters to the ECHO results and record the filtering parameters, b): to modify the filtering parameter in conjunction with the gated images and the cardiac wall motion for the filters and record the LVEF %. Left ventricular ejection fraction was determined from LV end-diastolic volume and end-systolic volume using the following standard formula:
LVEF = [(end-diastolic volume) – (end-systolic volume)] / [end-diastolic volume] ×100.
The cardiac images were reconstructed and displayed on the short, vertical, and horizontal long axis. Echocardiographic examination had been done in all patients using an echocardiography General Electric Medical System (GE Vivid T8) equipped with 2–5 MHz transducers and automated function imaging (AFI). Measurements had been performed according to the American Society of Echocardiography guidelines¹⁹.
2.4. STATISTICAL ANALYSIS
Statistical analysis was performed with SPSS software (SPSS Statistics for Windows, version 17.0; SPSS Inc., Chicago, IL, USA). Quantitative continuous variables are expressed as mean ± standard deviation (SD), and categorical variables are presented as count (percentage). The correlation of left ventricular EF and volumes (derived using the available software packages) with echocardiography was evaluated by means of Spearman’s correlation analysis. The percentage of cases reported normal or equivocal, before and after reconstruction using the optimized filters, was also reported, and compared.
3. Results
57%, 14% and 29% of the registered patients reported normal, equivocal (EV) and having CAD based on quantitative and qualitative assessment of LVEF respectively, prior to modified filtering. The post modified filter implementation was carried out on 2 ways; a): to match the calculated LVEF% for both Butterworth and Wiener filters to the ECHO results and record the filtering parameters, b): to modify the filtering parameter in conjunction with the gated images and the cardiac wall motion for the filters and record the LVEF %. Although, for the first approach (a) there was an absolute correlation between GSPECT and ECHO after modifying filter parameters, the gated images suffered from over smoothing, and the cardiac wall motion was not diagnostically observable. We established a mean cutoff value for Butterworth (0.26 +/-0.09) and a mean point value for Wiener (4.9 +/-1.19) in correlation to ECHO. For the second approach, filter parameters continuously were adjusted until diagnostically acceptable gated images with observable cardiac wall motion were obtained. LVEFs were then recorded and compared to ECHO (LVEF). A good correlation between ECHO and the calculated LVEF with Wiener and Butterworth for men (r= 0.88 & r=0.84) and for smaller heart (women, r=0.95 & r=0.93) were observed. A cutoff value (0.5) and power (10) for Butterworth and a mean point value (4) and power (0.1) for Wiener were established for both men and women patients. Mean percentage LVEF error for Wiener and Butterworth against ECHO LVEF were 2% and 6% respectively post correction with much elevated qualitative acceptable images.
Figures (2–5) present reprocessed images of a normal, and intermediates (male and smaller heart-woman) perfusion defects using the selected filters. Table (1) also presents quantitative LVEF, EDV, ESV and ECHO evaluation and the comparison before and after filter modifications for combined male and female data.
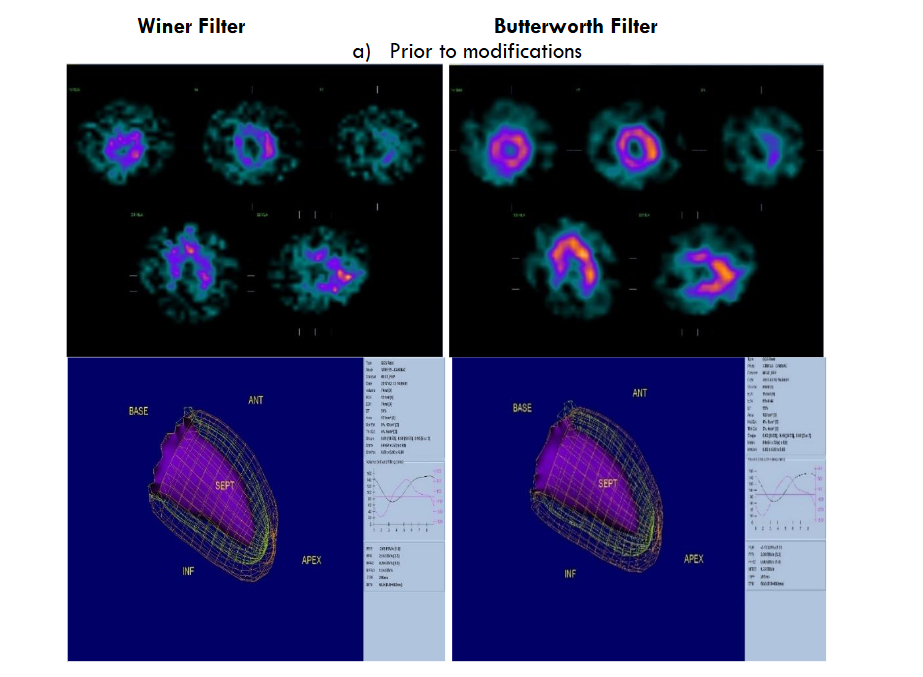
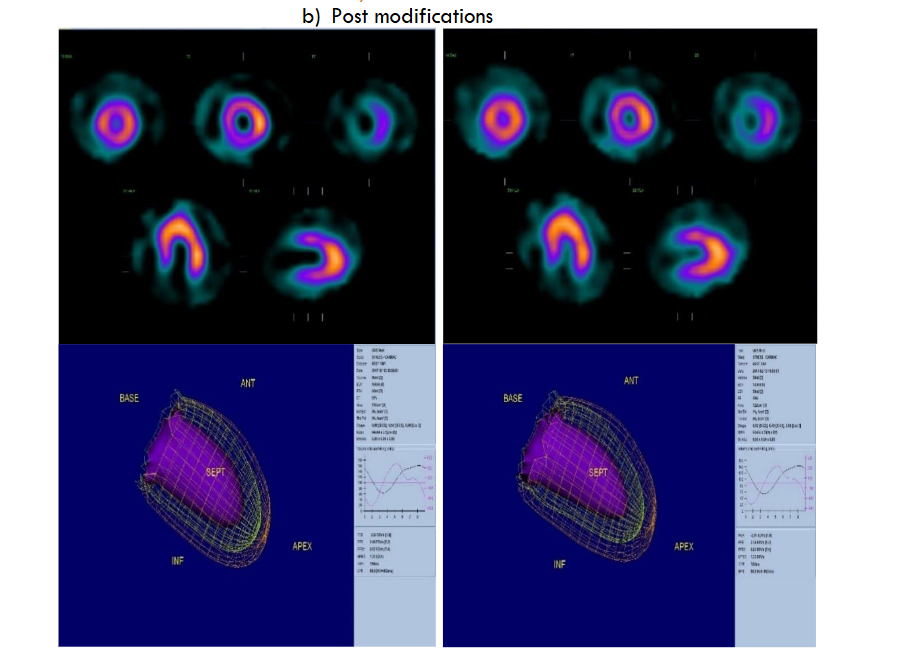
Figure 2 presents an intermediate perfusion defect case – A 24-year-old male smoker with hypertension and having palpitations for evaluation of myocardial perfusion.
a): pre modification filters showing poor observable perfusion and cardiac wall boundary and motion,
b): post correction showing a noticeable cardiac wall delineation together with the elevated observable cardiac muscle contraction (more observable on 3D dynamic). The LVEF was elevated by 10% post correction and was more in line with the ECHO result.
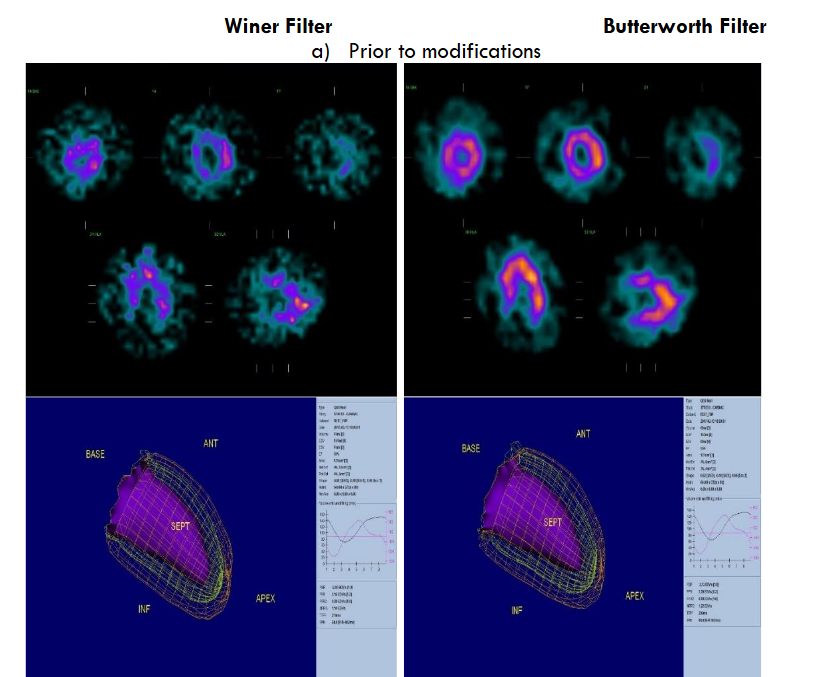
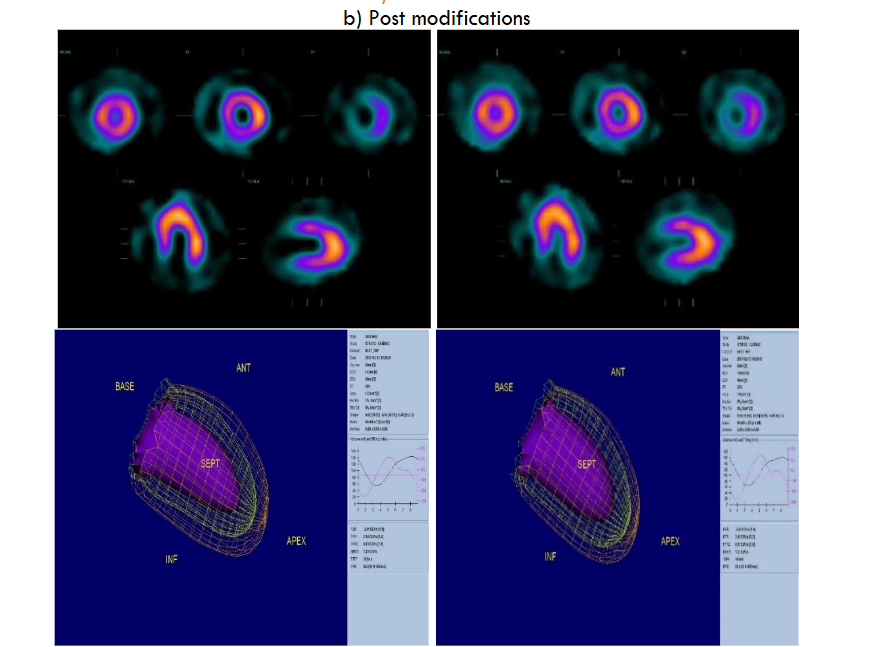
Figure 3 presents a normal cardiac case – A 56 years old male smoker with hypertension, shortness of breast and atypical chest pain for assessment of myocardial perfusion,
a – b): Pre filter correction showing cardiac images with poor to moderate cardiac wall boundary and motion, though LVEF was normal. Post filter correction showing more effectively the cardiac wall boundary and the wall motion for visual motion assessment. LVEF was elevated by 10%. The overall report also suggested normal with higher confidence in diagnostic accuracy.
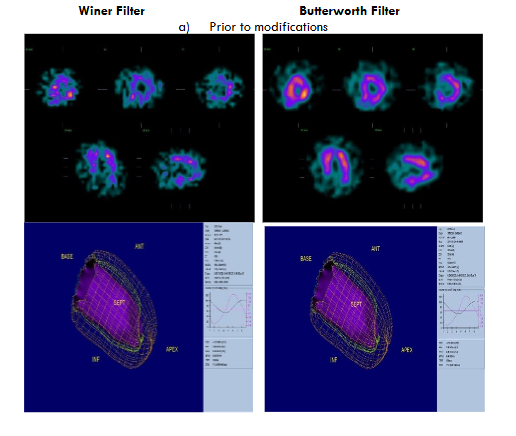
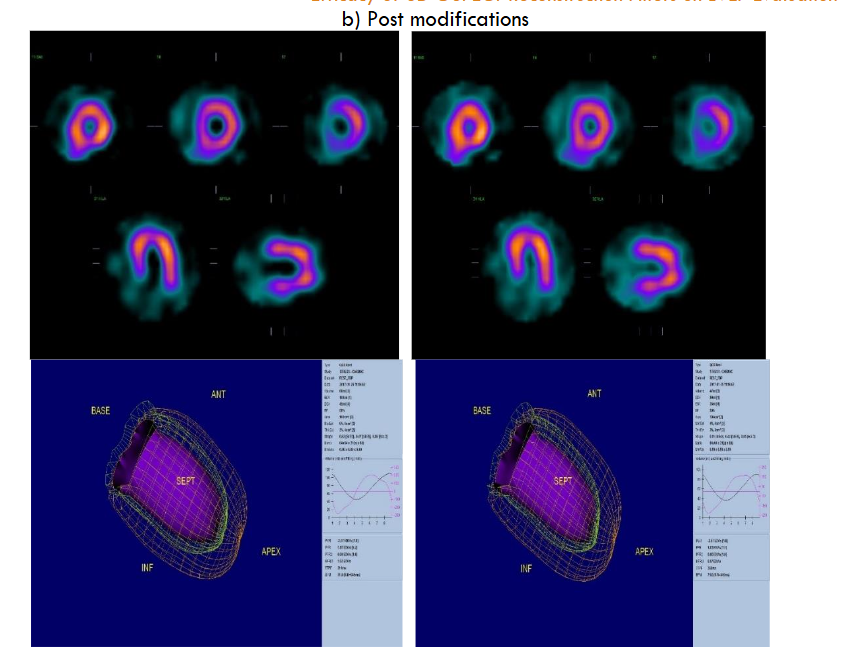 Figure 4 is an intermediate perfusion defect case – A 56 years old diabetes female with hypertension and shortness of breath.
Figure 4 is an intermediate perfusion defect case – A 56 years old diabetes female with hypertension and shortness of breath.
a): images with pre modification filters showing poor cardiac wall boundary and unclear wall motion. LVEF was reported as 45%,
b): post correction showing a noticeable cardiac wall delineation and cardiac muscle contraction (more observable on 3D dynamic). LVEF calculation elevated to 58% vs. ECHO LVEF of 61%.
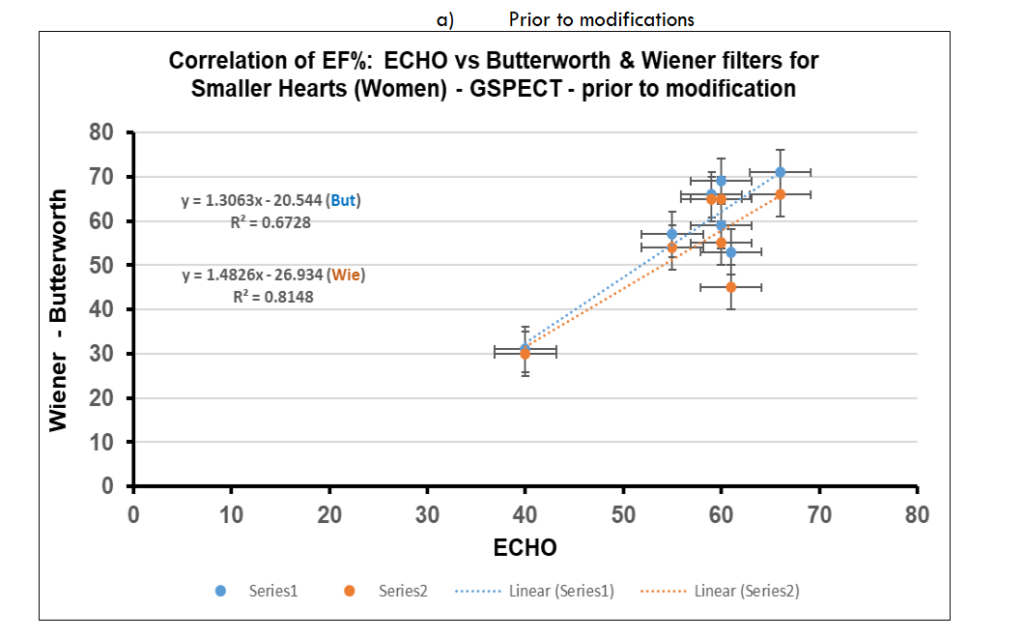
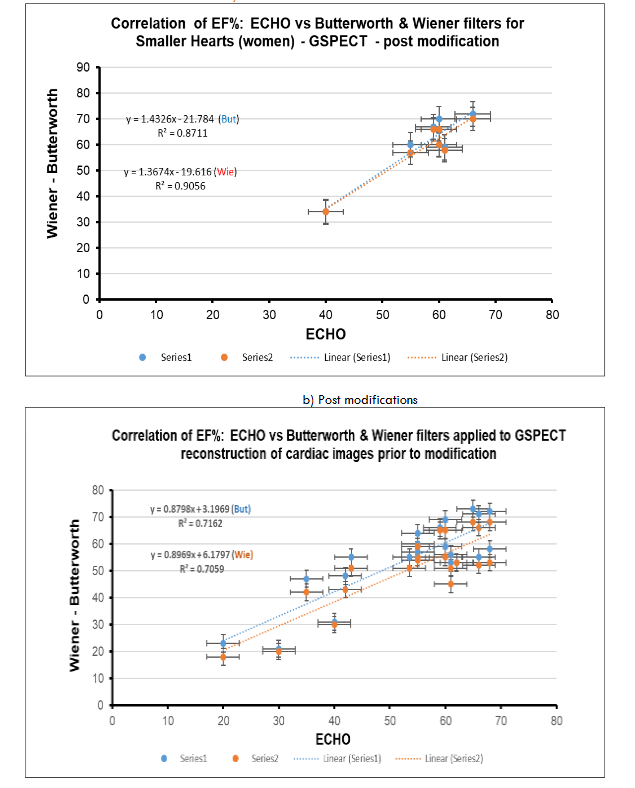
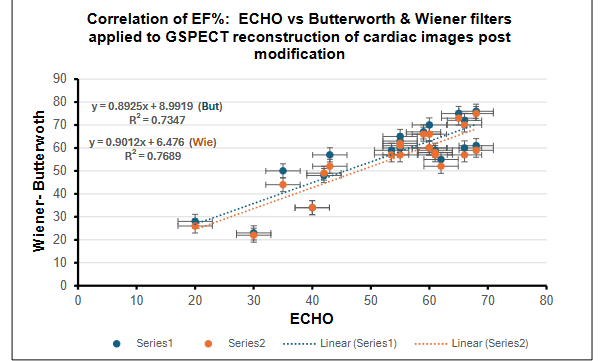
Figure 5: Scatter plot and linear correlation of SPECT Gated LVEF for normal and smaller size hearts vs. ECHO
a) pre modification and implementation of Wiener and Butterworth filters,
b) pre modification and implementation of Wiener and Butterworth filters.
Table 1: Quantitative comparison of EF, EDV, and ESV with ECHO prior and post modifications for combined male and female data.
| Parameters | Butterworth Before Modification | Wiener Before Modification | Butterworth Post Modification | Wiener Post Modification | ECHO |
|---|---|---|---|---|---|
| EF | 54.8 (14.5) | 50.6 (14.1) | 57.1 (14.1) | 55.1 (13.9) | 53.6 (13.4) |
| EDV | 107.7 (32.8) | 109.9 (31.8) | 100.7 (31.2) | 118.5 (30.9) | 131.3 (54.1) |
| ESV | 53.9 (39.6) | 57.9 (35.3) | 46.1 (32.5) | 56.0 (32.5) | 74.8 (52.4) |
EDV, end-diastolic volume; EF, ejection fraction; ESV, end-systolic volume; ECHO, echocardiography.
4. Discussion
Left ventricular ejection fraction refers to the fraction of LV end-diastolic volume ejected during systole. It is the most widely used measure of assessment for LV systolic function and is familiar to patients and clinicians²⁰. Although echocardiography is not a gold standard tool for the evaluation of left ventricular EF and volumes, decision making in the initial evaluation, management, and follow-up of patients with heart failure is largely done based on the widely available echocardiographic approach²¹. A good correlation of functional parameters derived from gated SPECT MPI with echocardiography indicates that gated SPECT MPI can be reliably used for the simultaneous assessment of perfusion and function in patients with heart failure, which can provide better diagnostic and prognostic accuracy for SPECT MPI.
This is the first study in our center assesses the impact of two different filters on GSPECT LVEF compared to echocardiography. The current practice for cardiac imaging in our busy local hospital was based on FBP and Butterworth (But) filter for processing the SPECT/CT images. The selected Wiener filter has characteristics of both the smoothing and blurring compensation. It reduces the high-frequency components of the data (that are supposed to be the noise) and at the same time, some selected medial frequencies are magnified.
During the process of optimization and to select a most suitable filter that provides higher contrast for a range of defects, many phantom images were reconstructed by applying a series of cutoff frequencies, orders, PSF and the noise to signal values for the listed filters¹⁸. SPECT filters can greatly affect the quality of clinical images by their degree of smoothing. Determining the best filter and the proper degree of smoothing can help to ensure the most accurate diagnosis.
We acknowledge that reconstruction filter is not the only parameter that affects the related image quantitatively and qualitatively. Other influencing factors such; scatter, attenuation, partial volume effect, the imaging system calibrations, and choice of collimators are influencing the outcome that is not within the remit of this study. The authors investigated the practical application of the range of filters in previous study¹⁸ that are currently employed for cardiac processing at the imaging centre.
The measurements of EF, EDV, and ESV by using gated SPECT MPI with Cedars Sinai QGS and QPS post filter modification well correlate with echocardiography data. Although echocardiography is not a gold standard tool for the evaluation of left ventricular EF and volumes, decision making in the initial evaluation, management, and follow-up of patients with heart failure is done based
on the widely available echocardiographic approach²². A good correlation of functional parameters derived from gated SPECT MPI with echocardiography indicates that gated SPECT MPI can be reliably used for the simultaneous assessment of perfusion and function in patients with heart failure, which can provide better diagnostic and prognostic accuracy for SPECT MPI.
Previous works by other authors also showed a good correlation between the two methods respectively. Vourvouri et al. reported a good correlation between QGS and two-dimensional echocardiography in 32 patients with severe left ventricular systolic dysfunction (r > 0.8 for EF, and r > 0.9 for EDV and ESV)²³. In a study by Berk et al.²⁴, a good correlation between QGS and echocardiography was also found in 33 patients with dilated cardiomyopathy, and it was noted that eight-frame gated SPECT overestimates the values of EDV and ESV compared with echocardiography; however, it appeared the EF was not statistically significant. Our study revealed slightly higher values of EF than echocardiogram post correction though, differences were not statistically significant. Comparatively EDV, and ESV showed lower values than echocardiography for both sexes using Cedars Sinai QGS and QPS post filter modification (Table 1). In contrast to patients with a small heart, the ESV less than the EDV owing to technical variability and edge detection and might be explained by better count statistics due to partial-volume effect and smaller left ventricular volume in the end-systolic frame.
It has been reported²⁵ that gated SPECT MPI can be most advantageous when the simultaneous evaluation of myocardial function and perfusion are required, even in heart failure patients such as those who are candidates for cardiac resynchronization therapy, when the assessment of myocardial viability, ESV, and left ventricular dyssynchrony are needed for the evaluation of response to cardiac resynchronization therapy. The presented results were based on a retrospective study.
5. Conclusion
The current study, based on the limited number of patients, is suggesting that modification of Wiener and Butterworth filters could produce results that are consistent with ECHO and can help speed image processing time since a proper filter function is often chosen clinically by the tedious and time-consuming process of trial and error. Mean percentage LVEF error for Wiener and Butterworth against ECHO LVEF were 2% and 6% respectively post correction, together with much elevated qualitative acceptable images. The authors are aware of the current limited number of patients, though the outcome is very encouraging and so aiming to gather the larger sample data for further comparison.
Conflicts of Interest Statement
The authors have no conflicts of interest to declare.
Funding Statement
None
Acknowledgments
Authors would like to thank Dr Haytham Ramzy – radiology department in Adan Hospital for his input in provision of clinical expertise and interpretation of images.
References
- Schaefer WM, Lipke CS, Standke D etal. Quantification of left ventricular volumes and ejection fraction from gated 99mTc-MIBI SPECT: MRI validation and comparison of the Emory Cardiac Toolbox with QGS and 4D-MSPECT. J Nucl Med 2005; 46: 1256–1263.
- Demir H, Tan YZ, Kozdag G etal. Comparison of gated SPECT, echocardiography and cardiac magnetic resonance imaging for the assessment of left ventricular ejection fraction and volumes. Ann Saudi Med 2007; 27: 415–420.
- Kakhki VD, Zakavi SR, Sadeghi R, Yousefi A. Importance of gated imaging in both phases of myocardial perfusion SPECT: myocardial stunning after dipyridamole infusion. JNM Technology 2006; 34: 88–91.
- American Cancer Society, “Cancer Facts and Figures for African Americans, 2019-2021 Accessed December 5, 2023, https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/cancer-facts-and-figures-for-African Americans/cancer-facts-and-figures-for-African-Americans-2019-2021.pdf
- National Cancer Institute. Surveillance, Epidemiology, and End Results Program 1975-2020 Cervical cancer incidence and mortality. Long term trends. https://seer.cancer.gov/statistics-network/explorer/.
- Bellinger JD, Millegan W, Abdalla AE. “I’m not ashamed to talk on it!”: African American women’s decisions about cervical cancer prevention and control in South Carolina. Women’s Health Issues. Mar-Apr 2015;25(2): 120-7. doi: 10.1016/j.whi.2014.10.006
- Kakhki VR, Zakavi SR, Sadeghi R. Comparison of two softwares in gated myocardial perfusion single photon emission tomography, for the measurement of left ventricular volumes and ejection fraction, in patients with and without perfusion defects. Hell J Nucl Med 2007; 10: 19–23.
- Kakhki VR, Sadeghi R. Gated myocardial perfusion SPECT in patients with a small heart: effect of zooming and filtering. Clin Nucl Med 2007; 32: 404–406.
- Hull DM, Peskin CS, Rabinowitz AM, et al. The derivation and verification of a non-stationary, optimal smoothing filter for nuclear medicine image data. Phys Med Biol 1990; 35:1641–62.
- Lyra M, Ploussi A. Filtering in SPECT image reconstruction. Int J Biomed Imaging 2011; 2011:1–4.
- King MA, Long DT, Brill BA. SPECT volume quantitation: influence of spatial resolution, source size and shape, and voxel size. Med Phys 1991; 18:1016–23.
- Fakhri GE, Buvat I, Benali H, et al. Relative impact of scatter, collimator response, attenuation, and finite spatial resolution corrections in cardiac SPECT. J Nucl Med 2000; 41:1400–8.
- Zubaid M, Rashed WA, Husain M, Mohammad BA, Ridha M, Basharuthulla M, et al. A registry of acute myocardial infarction in Kuwait: patient characteristics and practice patterns. Can J Cardiol. 2004, 20: 783-787.
- World Health Organization: World Health Statistics – Kuwait: country profiles -noncommunicable diseases. http://www.who.int/gho/countries/kwt/country_profiles/en/index.html
- Awad A and Al-Nafisi H. Public knowledge of cardiovascular disease and its risk factors in Kuwait: a cross-sectional survey. BMC Public Health 2014, 14:1131. http://www.biomedcentral.com/1471-2458/14/1131
- Alarouj M, Bennakhi A, Alnesef Y, Sharifi M, Elkum N: Diabetes and associated cardiovascular risk factors in the State of Kuwait: the first national survey. Int J Clin Pract. 2013, 67: 89-96. 10.1111/ijcp.12064.
- International Diabetes Federation: IDF diabetes atlas: sixth edition. http://www.idf.org/diabetesatlas
- Masoomi AM, Al-Shammeri I, Kalafallah K, Elrahman H, Ragab O, Ahmed E, et.al. Wiener filter improves diagnostic accuracy of CAD SPECT images—comparison to angiography and CT angiography. Medicine (2019) 98:4 (e14207).
- Mitchell C, Rahko PS, Blauwet LA, Finstuen B, Foster MC, Horton K. Guidelines for Performing a Comprehensive Transthoracic Echocardiographic Examination in Adults: Recommendations from the American Society of Echocardiography. Published: VOLUME 32, ISSUE 1, P1-64, JANUARY 2019 September 30, 2018. DOI: https://doi.org/10.1016/j.echo.2018.06.004
- Patricia A. Pellikka, Lilin She, Thomas A. Holly, Grace Lin, Padmini Varadarajan, Ramdas G. Pai, Robert O. Bonow, et.al. Variability in Ejection Fraction Measured by Echocardiography, Gated Single-Photon Emission Computed Tomography, and Cardiac Magnetic Resonance in Patients with Coronary Artery Disease and Left Ventricular Dysfunction. JAMA Network Open. 2018;1(4): e181456. doi:10.1001/jamanetworkopen.2018.1456
- Shojaeifard M, Ghaedian T, Yaghoobi N, Malek H, Firoozabadi H, Bitarafan-Rajabi A, et al. Comparison of Gated SPECT Myocardial Perfusion Imaging with Echocardiography for the Measurement of Left Ventricular Volumes and Ejection Fraction in Patients with Severe Heart Failure. Res Cardiovasc Med. 2016 February; 5(1): e29005.
- Hunt SA, Abraham WT, Chin MH, Feldman AM, Francis GS, et. al. 2009 Focused update incorporated into the ACC/ AHA 2005 Guidelines for the Diagnosis and Management of Heart Failure in Adults A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines Developed in Collaboration with the International Society for Heart and Lung Transplantation. J Am Coll Cardiol. 2009;53(15): e1–e90.
- Vourvouri EC, Poldermans D, Bax JJ, Sianos G, Sozzi FB, Schinkel AF, et al. Evaluation of left ventricular function and volumes in patients with ischaemic cardiomyopathy: gated single-photon emission computed tomography versus two-dimensional echocardiography. Eur J Nucl Med. 2001;28(11):1610–5.
- Berk F, Isgoren S, Demir H, Kozdag G, Ural D, Komsuoglu B. Evaluation of left ventricular function and volume in patients with dilated cardiomyopathy: gated myocardial single-photon emission tomography (SPECT) versus echocardiography. Ann Saudi Med. 2005;25(3):198–204.
- Azizian N, Rastgou F, Ghaedian T, Golabchi A, Bahadorian B, Khanlarzadeh V. LV Dyssynchrony Assessed with Phase Analysis on Gated Myocardial Perfusion SPECT Can Predict Response to CRT in Patients with End-Stage Heart Failure. Res Cardiovasc Med. 2014;3(4): e20720.