





Electrophysiology and Mood Disorders: Insights on Comorbidity
Electrophysiology of Self and Mood Disorder as an Energy Shift: Mitochondrial Dysfunction and Medical Comorbidity, Beyond the Metabolic Syndrome
Sermin Kesebir, MD1
- Professor of Psychiatry, Üsküdar University, NPİstanbul Brain Hospital, İstanbul, Turkey
OPEN ACCESS
PUBLISHED: 31 July 2025
CITATION: Kesebir, S., 2025. Electrophysiology of Self and Mood Disorder as an Energy Shift: Mitochondrial Dysfunction and Medical Comorbidity, Beyond the Metabolic Syndrome. Medical Research Archives, [online] 13(7).
https://doi.org/10.18103/mra.v13i7.6765
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i7.6765
ISSN 2375-1924
Abstract
Depressive and manic episodes of bipolar disorder are characterized by decreased and increased energy. As the duration of the disease increases, psychomotor retardation and anhedonia become dominant. Increased activity in the Default Mode Network and decreased activity in the Salience Network and Central Executive Network have been associated with Glutamate/GABA (Gamma-Aminobutyric Acid) imbalance. Medical comorbidity has an etiological partnership as well as medication burden and lifestyle. According to the entropy change we calculated on EEG (Electroencephalography), we classified mood disorders into three groups. Including family history, which is true comorbidity, was framed by physical illnesses. We showed how the entropy change in chaotic phase transitions in cases diagnosed with bipolar disorder is regulated by lithium. Cross frequency coupling delta/beta appears both as a trait to deal with depressive symptoms and as a state to reveal mixed symptoms. Delta activity is predictive of response to lithium and ECT (Electroconvulsive Therapy), and nonresponse to antidepressants. It is a gabaergic dysfunction. Self pathology has been proposed as a mental projection of bipolar disorder. There is a decrease in glutamic acide decarboxilase enzyme activity, which is responsible for GABA production at the molecular level. GABA is a metabolite of Krebs. Also in immune cells. The GABA shunt plays an important role in preventing the accumulation of reactive oxygen species and cell death. The price for this is disruption in phosphorylation processes, which is reflected in the energy balance. In this article, three planes are tried to be brought together with their projections on each other: Self pathology on the mental plane, mood disorder on the brain plane, medical comorbidity on the body plane.
Keywords
Mood disorder, affective spectrum, medical comorbidity, metabolic syndrome, GABA shunt, self pathology, EEG.
Introduction
Recent brain imaging studies indicate an alternative connectivity and a unique network function in patients with mood disorders. Increased activity in the Default Mode Network, decreased activity in the Salience Network, and Central Executive Network in patients with mood disorders have been associated with Glutamate/GABA (Gamma-Aminobutyric Acid) imbalance. Glutamate/GABA imbalance is associated with regional blood flow irregularities, global intrinsic network activity and connectivity, and declines in global signals. While one group of researchers attribute the primary role to GABA based on the efficacy of brexanolone in postpartum depression, the majority support glutamatergic dysfunction, which is reversed by fast-acting ketamine.
This article attempts to present a physical and mental projection of bipolar disorder based on EEG (Electroencephalography) data. A mental projection is as important as a physical projection in the holistic conceptualization of psychiatric disorders. In this article, three planes are tried to be brought together with their projections on each other: i) Self pathology on the mind plane, ii) Mood disorder on the brain plane, iii) Medical comorbidity on the body plane.
The self may be such a representation for bipolar disorder. The projection of self-pathology on the EEG can be compared with the electrophysiological and pathophysiological features of bipolar disorder. In this partnership, the approach of self psychology will serve to increase our power in psychotherapy.
The life expectancy of cases diagnosed with bipolar disorder is on average ten years shorter than that of healthy controls. The reason for this is not only suicide and decreased quality of life and functionality, but also comorbid medical diseases. A mood spectrum that includes physical illnesses is possible, Kraepelin said (1921). Such an expansion will increase our treatment options, which is also related to preventive medicine.
Our current diagnostic systems ignore neurobiological heterogeneity. Indeed, a DSM (Diagnostic and Statistical Manual of Mental Disorders) diagnosis matches multiple treatment options, and vice versa. Individual-specific treatment is based on biomarkers. Endophenotype is the heritable form of the biomarker. EEG may serve as a biomarker for mood disorders and has also been proposed as an endophenotype. Heritability of some EEG parameters such as alpha peak frequency and alpha spectral power density was shown in twin and family studies. The heritability quotients of these two variables were determined as 81 and 79% respectively. There rates are superior to p300 amplitude and latency values previously determined as 60 and 51% respectively. Temporal resolution of EEG provides an important advantage.
Bipolar Self
Self is the state of feeling and experiencing the existence of the subject called “me”. The grandiose self and the idealized parent image are the two poles of a fragmented self in the newborn. It becomes a formation with continuity and permanence between the two poles, through a real relationship and live processes. Experiences of time and space accumulate and combine to form an integrated self.
The human child achieves this by fulfilling and satisfying its longing for fusion/union with its self-object. The self is a spatiotemporal formation. An integrated self is both the source and organizer of the ego function. Curiosity and enthusiasm, ideals, talents and skills are the third pillar of the self. Self is a resting network activity, and EEG. It is like a fingerprint, it is unique. The ability to produce an alpha wave appropriately is related to the individual’s affective repertoire.
The situations in which we see a decrease in liveliness, self-esteem, curiosity and enthusiasm are situations in which the grandiose self is damaged. Psychomotor retardation dominates the phenomenon. A reactive mood is in a dependent relationship with its self-object. A feeling of guilt sets in because the demands of the idealized parental image are not met. It is a phenomenon of depression.
The trauma in question is emotional and/or physical neglect. It is the most common type of childhood trauma in bipolar disorder. Kohut talks about defensive and compensatory structures: The deficiency in one pole is tried to be completed by strengthening the other, so that the self function can continue. If a trauma occurs due to the weakness of the self-object or the fact that it is strong but does not allow for fusion/idealization and identification, which is related to abuse, the self becomes prone to disintegration. “Depressed child”, “hypochondriac child”, “feeling dead” appear in the absence of empathy, in other words, in the absence of a life-giving energy source. Unintegrated or dissociated aggression, unintegrated or dissociated sexuality, and paranoid position are products of breakdown of the self. It is similar to the phenomenon of the manic period.
In other words, a grandiose self that is not properly and sufficiently mirrored will gravitate towards the idealized parental image. If it is supported sufficiently and sufficiently and identification is allowed, it will evolve to the next level with narcissistic defenses. Otherwise, it will move towards borderline personality organization. This is the basis for the frequency of comorbidity between bipolar disorder and borderline personality disorder. In bipolar disorder type II, depressive type of narcissistic personality disorder is ahead of borderline personality disorder. In the case of bipolar disorder, the stressors and traumas of daily life, unlike childhood trauma, are regressions that occur on an integrated/existing structure and are associated with the dissociation of the self. They are candidates for evolution to mood episode.
Individually specific temperamental factors regulate neurodevelopment in the direction of sensitivity and resilience in early life, which determines our future clinical profile. Temperamental diversity tells us which type and level of severity of environmental factors we may be affected by, it regulates the immune response, and manages disease severity and comorbidities. This is what happened in the Covid-19 pandemic.
The self that begins to form in the human infant is simultaneously attuned to the body. Different neurophysiological variables that differ in different temperament subtypes have been demonstrated, such as heart rate variability, basal cortisol levels, and skin conductance.
At this point, a disruption in the development of the grandiose self, which is an existential anxiety in the early stages, will occur together with a disruption in the adaptive responses in the body. Lactose intolerance can be given as an example of this situation. In the later stages, it will be matched with situational and anticipatory anxiety, autoimmune and allergic diseases. Any disruption in the idealized parental image path is met with disruptions in the stress response in the body. It is caused by oxidative stress. Metabolic syndrome can be given as an example of stress responses mediated by inflammatory effector systems and glucocorticoid-insulin signaling mechanisms. At the point where these two parallel paths intersect and create, at the point of individual-specific abilities and skills, in other words, in identity formation, depersonalization and derealization are reflected in the electrical activity of the brain as epileptic phenomena. It is together with hypothalamopituitary gonadal axis pathologies.
| Self pathology | Mental disorders | Medical comorbidity |
|---|---|---|
| Grandiose self | Anxiety spectrum disorder | Autoimmune and allergic disease |
| Idealized parental image | Affective spectrum disorders | Neuroinflammation/Metabolic syndrome |
| Fragmented/Disintegrated Self | Depersonalisation/Derealisation/Psychotic spectrum disorder | Epileptic phenomenon |
Projective connections between self and body have been examined in detail between mood disorders and medical comorbidity. Schizophrenia and other neurodevelopmental disorders are excluded from this formulation.
In one of our current studies, we showed that there is an inverse relationship between the “Self Inventory” and ‘’Mood Disorder Questionnaire (MDQ)’’ in terms of compensatory dimension scores in healthy individuals. When we compared healthy individuals with cases diagnosed with bipolar disorder, we saw that defensive structures came to the fore in cases diagnosed with bipolar disorder. When I examined the relationship between self-inventory scores and EEG spectral power densities, I found that it was similar to the electrophysiological representation of bipolar disorder. The electrophysiological representation of the self was consistent with brain imaging representations in the literature in terms of its source.
| Reactive Mood and Cyclicity | Comorbid Anxiety | Psychotic symptom |
|---|---|---|
| Metabolic Syndrome: Inflammatory effector systems, glucocorticoid/insulin signaling mechanisms, purinergic dysfunction, thrombotic dysfunction. | Proliferative cancers of the breast, prostate and gastrointestinal tract | Autoimmune and Allergic diseases |
| Epilepsy, epileptic phenomena | Leukemia and lymphomas | PCOS and other diseases of the genitourinary system and Hypothalamopituitary Gonadal axis |
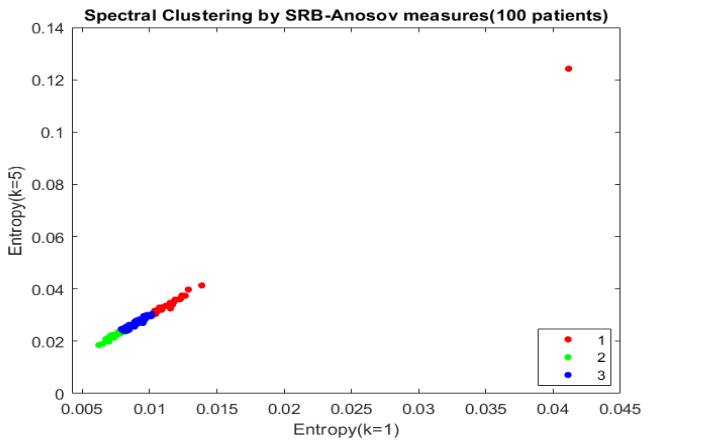
Figure 1: Reclassification of Mood Disorders with Comorbid Medical Diseases based on Sinai-Ruelle-Bowen/ SRB Entropy Measures
The nature of the relationship with the self-object is the source of mental energy. In self-pathology, self-referential rumination at the symptomatic level is ahead of environmental focus, internal awareness is ahead of external awareness, rest network is ahead of the executive network at the network level, and anterior cingulate cortex (ASC) is ahead of the dorsolateral prefrontal cortex (DLPFC) at the regional level. There is a decrease in glutamic acid decarboxylase (GAD) enzyme activity, which is responsible for GABA production at the molecular level of self pathology. With flumazenil PET, response to internal and external stimuli was found to be correlated with a decrease in GABA receptor binding in the PFC. In addition, alpha spectral power density with combined EEG and MRS (Magnetic Resonance Spectroscopy) was found to be associated with perigenual ASC glutamate levels.
GABA Shunt
GABA is a metabolite of Krebs, including immune cells. The alternative physiological pathway called the GABA shunt occurs as a stress response in the mitochondria. It is activated by an increase in ROS (reactive oxygen species) production. The function of the GABA shunt is to prevent ROS-mediated cell death. The increase in ROS production is stimulated by proinflammatory processes.
Increased mitochondrial oxidation of succinate by succinate dehydrogenase (SDH) and increased mitochondrial membrane potential stimulate the production of mitochondrial reactive oxygen species (ROS). RNA (Ribonucleic acid) sequencing has shown that this picture creates a proinflammatory gene expression profile. While increasing succinate levels during the transition from oxidative phosphorylation to glycolysis will activate SDH, an anti-inflammatory process will occur if SDH is blocked with an inhibitor such as dimethyl malonate.
If the function of the GABA shunt is to prevent ROS-mediated cell death, this comes at the cost of some changes in the phosphorylation processes responsible for energy production that occur when the GABA shunt operates. The catabolic products of the GABA shunt support metabolic homeostasis, producing NADH (Nicotinamide adenin dinucleotide) and NADPH (Nicotinamide adenin dinucleotide phosphate). However, when compared to ATP (Adenosine triphosphate) production, we see a deterioration in bioenergetics. Gamma hydroxybutyric acid (GHB), which is formed by the catabolism of GABA, is also a psychoactive neurotransmitter that can enter the Krebs cycle. In addition to its acute neuroprotective effects, it has harmful effects that can lead to cognitive dysfunction in the chronic process.
In the light of the information I have tried to summarize so far, psychomotor retardation, anhedonia, and cognitive impairment, which become more dominant in mood disorders, especially as the duration of the disease increases, seem to be explained by the GABA shunt.
Inflammation and oxidative stress, and allostatic load in the form of mitochondrial gene variations, have a detrimental effect on mitochondrial function in bipolar patients. Different studies have also shown functional polymorphisms in mitochondrial DNA (Deoxyribonucleic acid in some regions of the brain.
For example, in one study, a replication-deficient mutant and a defective herpes simplex virus 1 (HSV-1) vector were developed to help transfer the glutamic acid decarboxylase-67 (GAD67) gene. Infection with these GAD67-expressing amplicon vectors was shown to increase resistance to H2O2, and this protection was associated with increased energy metabolism, as demonstrated by ATP levels. At this point, the decrease in ATP levels in the presence of gamma-vinyl GABA (GVG), a specific GABA-T (transaminase) inhibitor, was interpreted as involving GABA shunt activity.
Normally, the level of glutathione (GSH), which requires ATP for its synthesis, is increased by the GAD67 transgene. The activity of glucose-6-phosphate dehydrogenase, which plays a role in protecting NADPH that can be used to replenish the GSH pool, was also found to be increased by infection with the same vector.
In light of these findings, it was stated that replication-deficient HSV-1 and the GAD67 transgene may have complementary neuroprotective effects, and infection with amplicon vectors expressing GAD67 may protect undifferentiated cortical neurons from oxidative stress-mediated glutamate toxicity.
At this point, I would like to share a case. An untreated and prolonged depression patient, because she has no insight and lives alone, came with catatonia. Brain imaging indicated limbic encephalopathy, and GAD65 antibodies were positive in the neuroinflammatory panel. There was type 2 diabetes in the medical history and a family history of autoimmune disease. She was treated with ECT and gabapentin. At the end of two years, he continues his life with a period of well-being in which functionality is preserved with 300 mg/day lithium. Glucose and oxygen are vital for the brain. When glucose metabolism is disrupted, reactive oxygen species are released increasingly. Hexokinase (HK) is an important enzyme in glucose metabolism and is linked to brain mitochondrial redox modulation by recycling adenosine diphosphate (ADP) for oxidative phosphorylation. Tiagabine and vigabatrin block the effects of the GABA shunt on oxidative phosphorylation-induced HK (Hexokinase) activity. This is evidence that phosphorylation of glucose is related with the GABA shunt.
Projection of the Biphasic State to Medical Comorbidity
Mitochondrial dysfunction i) It is reflected in glucose metabolism. In a thesis study from 2010, we showed that glucose metabolism disorder was present in 64% of first-episode mania cases. In the first quarter of 2022, metformin emerged as a treatment option for treatment-resistant bipolar depression in a four-blind placebo-controlled study. ii) It is reflected in lipid metabolism. Epidemiological studies found that the frequency of depression was lower in cases using statins. On the other hand, studies have been published that found a relationship between statin use and impulsivity and self-harming behavior. It reminds us of the similar properties of antidepressants. iii) It is reflected in purinergic function. It is involved in uric acid metabolism. iv) It is reflected in circadian function. Delayed sleep phase syndrome has been proposed as a compensatory mechanism for an impaired energy metabolism at the cellular level.
Physical exercise has gained momentum as a non-pharmacological treatment intervention. It enables the release of extracellular vesicles into the circulation. Extracellular vesicles, which are cargo signatures containing microRNA, are hypothesized to contribute to the antidepressant effect through their effects in regulating glucocorticoid-mediated inflammation.
While multiple etiologies and pathogenesis by gene-environment interaction, our current treatment targets lie between the symptom and the common pathways leading to the symptom. It is the interactions between stress and neural circuits that cause stress and should be the target of treatment. The mind uses the brain as an interface: That is, psychiatric disorders and physical diseases occur through similar mechanisms and processes.
In a study from 2012, we investigated physical illnesses in more than two thousand outpatients. We found that the duration of illness in cases diagnosed with mood disorders was similar to the duration of physical illness. This is an epidemiological comorbidity. There was no such correlation in cases diagnosed with schizophrenia. In another large sample study, which also included family history, we obtained a trait index as a result of the factor analysis we applied to the research items in cases diagnosed with bipolar disorder.
| 1. | Delayed sleep phase |
|---|---|
| 2. | Addiction |
| 3. | Cardiovascular disease, DM, breast, prostate or gastrointestinal system cancers in Family History |
| 4. | Vagus tenderness |
| 5. | Presence of thyroid pathology or other autoimmune disease |
| 6. | Left-handedness |
| 7. | Presence of febril convulsion or migraine and PCOS, and/or epilepsy, leukemia/lymphoma in Family History |
According to the entropy change we calculated on EEG, we classified mood disorders into three groups. Including family history, which is true comorbidity, was framed by physical illnesses: The first group, which forms the core of the mood disorder with its reactive and cyclic nature, was associated with the metabolic syndrome, together with proliferative cancers of the breast and prostate and the gastrointestinal tract. The second group, comorbid with anxiety disorder, was accompanied by allergic and autoimmune diseases, especially thyroid pathology. The third group with psychotic findings included epilepsy, migraine, polycystic ovary, leukemia and lymphomas. When looking at this distribution, it is also seen that three endocrine axes are separated: i) HPA (Hypothalamic Pituitary Adrenal axis), ii) HPT (Hypothalamic Pituitary Thyroid axis), iii) HPG (Hypothalamic Pituitary Gonadal axis). One might wonder whether it could shed light on stem cell therapies associated with the 3 germ layers.
The anxiety disorders are the most common psychiatric comorbidity for the bipolar disorders. Comorbidity in these rates suggests that the two diseases are inherited together in nature. In this subgroup, personal and familiar history of thyroid pathologies are positive. This is a subgroup that can be elicited by linkage data in the literature and it corresponds to comorbidity for panic disorder in which familial aggregation had been shown.
Cytokines are responsible for innate immunity. Toll-like receptors (TLR) are endosomal pattern recognition receptors related to molecular patterns that promote pathogenesis to cytokines. TLR receptors are expressed primarily in microglia, are found in the thyroid gland, adrenal gland, and intestines. Another place where they are found in the early stages of development is the thymus. At this point, it should be remembered that mood stabilizing agents were first called thymoleptics. The address of adaptive immunity is the HLA (Human Leukocyte Antigen) system. The adaptation in question is immunosuppression. According to our results, comorbid anxiety and neuroleptic sensitivity have a positive correlation in bipolar patients.
The presence of epilepsy in the family history and the current psychotic symptom have a strong correlation in the bipolar patients. According to our results, there is an association between bipolar disorder and leukemia-lymphoma, polycystic ovary syndrome and epilepsy and migraine in the third group. In the postinsemination of embryonic period, vitellus sac derived erythromyeloid progenitors enter the central nervous system. In adult life, somatic mutations of BRAF genes disrupt the continuity of macrophage. This condition can cause highly heritable neurodegenerative diseases in the brain and cerebellum, and various tumors, leukemias and lymphomas in the periphery of body.
In the group that forms the core of mood disorder with its reactive and cyclic nature, there is an association with metabolic syndrome components and proliferative cancers of breast, prostate and gastrointestinal tract in the personal or family history. All of this group meets at least one of the metabolic syndrome criteria according to NCEPATP III (National Cholesterol Education Program-Adult Treatment Panel III). Most of this group are characterized by mixed symptoms and irritability rather than euphoria. There is a relationship between diabetes and seasonality in this group.
Metabolic syndrome is more common in bipolar disorder type II than type I, and predicted by seasonality. Climate and geographical change and in this context migration are risk factors for both mood disorder and metabolic syndrome with temperamental properties. The interface between the mood disorder and metabolic syndrome are inflammatory effector systems and glucocorticoid/insulin signaling mechanisms.
Bipolar EEG
Depression is characterized by slow waves on the EEG, first theta and then the slower delta. Delta activity is predictive of response to lithium and ECT (Electroconvulsive Therapy), and nonresponse to antidepressants, which indicates that the depression in question is bipolar depression. It is a gabaergic dysfunction. The increase in fast wave activity is first reciprocated by beta. This is a response to the increase in slow wave activity, initially like a compensation mechanism. And it can be thought of as a more severe form of depression on the unipolar-bipolar continuum.
Since depressive episodes with mixed features include both poles of bipolar disorder, they are phenomenologically rich and pathophysiologically chaotic periods of illness. It offers very valuable opportunities to consider phenomenology together with physiopathology. Mood dysregulation and compensatory regulation efforts, which are the core symptoms of the disease, are clearly present here.
In this study, we evaluated 8 cases with bipolar disorder type II, depressive episodes, mixed features, using EEG, HDRS (Hamilton Depression Rating Scale) and MDQ at baseline and at the end of the 3rd week of treatment with lamotrigine.
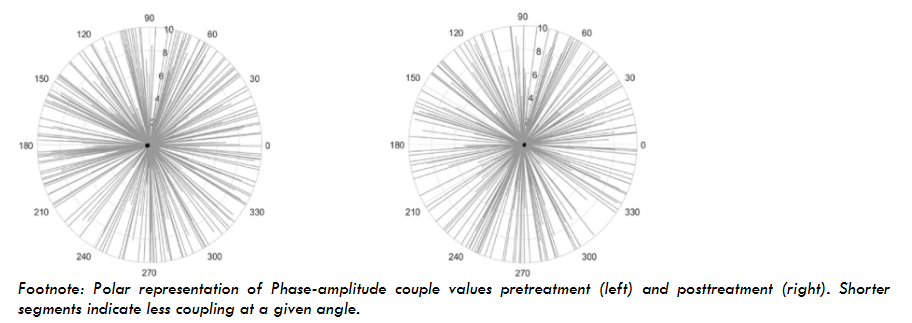
The cross-frequency coupling (CFC) delta/beta can be thought of as a corticosubcortical dialogue, a seesaw. Depressive mood is shaped in alpha, obsessive rumination is shaped in theta, and retardation is shaped in delta activity. At this point, increased attention, physical activity and phase shift in sleep are compensatory changes up to a point. While irritability, reward addiction and decreased inhibitory control are points where balance is challenged, the key word is that the dialogue continues. At the point where the coupling is broken, the mainspring breaks, euphoria fades, hostility and aggression, paranoia and persecution take over. At the breaking point, the alternative path is maximum cognitive loss. 1 Hz is a cycle.
Discussion
CFC appears both as a trait to deal with depressive symptoms and as a state to reveal mixed symptoms. Aretaeus from Cappadocia says “It seems to me that melancholia is the beginning and a part of mania.” As a matter of fact, everything in nature is in a state of continuity. We divide time and space. Temperament and personality, comorbid anxiety and antidepressant use, comorbid ADHD (Attention Deficit and Hyperactivity Disorder) and stimulant use, alcohol and substance use disorder calls the mania.
At this point, the predictive value of CFC delta/beta on bipolarity, impulse control disorders, and alcohol and substance abuse and dependence is very valuable, especially if noradrenergic, dopaminergic and glutamatergic antidepressant use or stimulant somatic treatments are applied. In such a case, there is a risk of creating a mixed episode and cycle acceleration as well as a manic shift, with the risk of increasing impulsivity in all directions.
This study evaluates 363 patients who were diagnosed with affective disorders according to DSM-V. They were referred for the initial application. All were drug-free cases. According to our results, obsession, interpersonal sensitivity, anger, and paranoia are related with bipolarity also with some spectral powers of EEG too.
Risk factors are different. Whereas in the episode, all patients are similar to each other. Each episode changes the course of the disease. Bipolar disorder is a result of various and diverse interaction mechanisms in pathophysiological rewiring of the neuroprogression containing neurobiological factors and epigenetic mechanisms.
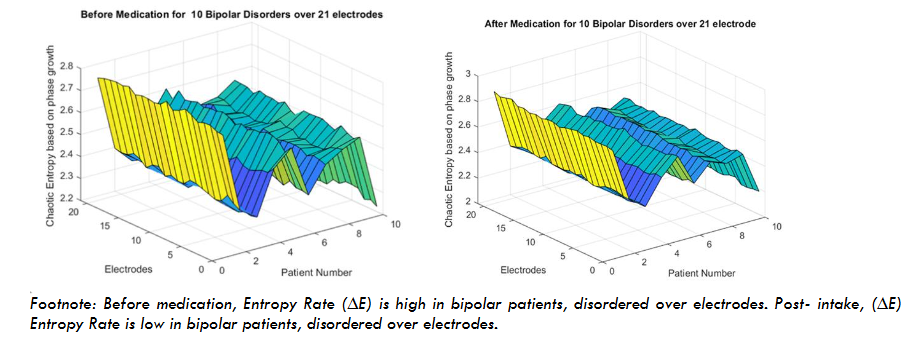
In our another study, we showed how the entropy change in chaotic phase transitions in cases diagnosed with bipolar disorder is regulated by lithium. We propose a Schwarzian derivative which is invariant under von Bertalanffy’s model of phase growth. This model is a family of unimodal inverse transformation map as which it can be used to determine the EEG dynamics of higher derivatives.
The brain operates phase synchronization in a similar way in healthy processes: i) in sudden situations, ii) when past memories are remembered, iii) in decision-making processes. Chaos occurs between the beginning and end of these synchronizations. It is a simultaneous action on all wavelengths, just as an orchestra participates with all its elements. It is a wave motion in which small frequencies are distributed over large frequencies and vice versa, with 1 Hz being a cycle. A wave motion in which dozens of springs of different diameters spread over each other.
Entropy is the name of the energy change between the beginning and the end of chaos. The more homogenized a scrambled egg is, the lower the entropy will be.
Conclusion
A holistic approach put forward in this article and tried to be proven through research will provide more consistent and comprehensive data than a cross-sectional evaluation predicted our current diagnostic systems. While EEG-based examinations are rare, quantitative evaluations of EEG and calculations of entropy will increase the strength of the limited evidence. In this article, three planes are tried to be brought together with their projections on each other: Self pathology on the mental plane, mood disorder on the brain plane, medical comorbidity on the body plane.
In conclusion, according to our results, cross-frequency coupling delta-beta seems to be a neurophysiological biomarker for affective dysregulation. The GABA shunt is like a mitochondrial projection of the energy dysregulation in mood disorders. The reflection of mitochondrial dysfunction on bodily functions causes medical comorbidity. Difficulties in regulating mood and energy both play a role in self-pathology.
Conflict
The author declares no conflict of interest.
Funding
This article did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
- Duman R.S., Sanacora G., Krystal J.H. Altered Connectivity in Depression: GABA and Glutamate Neurotransmitter Deficits and Reversal by Novel Treatments. Neuron. 2019;3;102(1):75-90.
- Holmes S.E., Scheinost D., Finnema S.J., Naganawa M., Davis M.T., DellaGioia N., Nabulsi N., Matuskey D., Angarita G.A., Pietrzak R.H., Duman R.S., Sanacora G., Krystal J.H., Carson R.E., Esterlis I. Lower synaptic density is associated with depression severity and network alterations. Nat Commun. 2019; 4;10(1):1529.
- Sanacora G., Frye M.A., McDonald W., Mathew S.J., Turner M.S., Schatzberg A.F., Summergrad P., Nemeroff C.B., American Psychiatric Association (APA) Council of Research Task Force on Novel Biomarkers and Treatments. A Consensus Statement on the Use of Ketamine in the Treatment of Mood Disorders. JAMA Psychiatry. 2017;1;74(4):399-405.
- Kesebir S. The two new biomarker in Mood Disorder: Bipolar EEG, Bipolar Self. Medical Research Archives. 2024;12(2) https://doi.org/10.18103/mra.v12i2.5071.
- Kesebir S., Koc M.I., Yosmaoglu A. Bipolar Spectrum Disorder May Be Associated With Family History of Diseases. J Clin Med Res. 2020;12(4):251-254. doi: 10.14740/jocmr4143.
- Krapelin E. Manic depressive Insanity and Paranoia. E&S Livingstone, 1921. Edinburgh.
- Kesebir S., Yosmaoğlu A. QEEG in affective disorder: about to be a biomarker, endophenotype and predictor of treatment response. Heliyon. 2018;22;4(8): e00741.
- Kesebir S., Yosmaoğlu A. QEEG – spectral power density of brain regions in predicting risk, resistance and resilience for bipolar disorder: A comparison of first degree relatives and unrelated healthy subjects. Heliyon. 2020; 6;6(6):e04100. doi: 10.1016/j.heliyon.2020.e04100.
- Vogel F. The genetic basis of the normal human EEG. Hum. Genet. 1970;10:91–114. doi: 10.1007/BF00295509.
- Kohut H., Wolf E.S. The disorders of the self and their treatment: An outline. The İntl J Psychoanalysis. 1978;59: 413-426.
- Kesebir S. Metabolic syndrome and childhood trauma: Also comorbidity and complication in mood disorder. World J Clin Cases. 2014;16;2(8):332-7. doi: 10.12998/wjcc.v2.i8.332.
- Yüncü Z., Kesebir S., Akdeniz F., Vahip S. Anticipation in bipolar disorder: A comparison between two generations. Turk Psikiyatri Derg. 2008;19(4):349-57.
- Kesebir S, Vahip S, Akdeniz F, Yüncü Z. (2005) The relationship of affective temperament and clinical features in bipolar disorder. Türk Psikiyatr Derg, 16: 164-9.
- Kesebir S. (2025) Self psychology and Mood Disorder. Curr Psychiatr Appr, 32: 11-27.
- Karova Z.Y., Kesebir S. (2021) Is there a relationship between self and mood? Bipolar Disord. 23: 68.
- Qin P., Northoff G. How is our self related to midline regions and the default-mode network? Neuroimage. 2011;1;57(3):1221-33.
- Northoff G., Sibille E. Cortical GABA neurons and self-focus in depression: a model linking cellular, biochemical and neural network findings. Mol Psychiatry. 2014;19(9):959.
- Wolff A., Berberian N., Golesorkhi M., Gomez-Pilar J., Zilio F., Northoff G. Intrinsic neural timescales: temporal integration and segregation. Trends Cogn Sci. 2022;26(2):159-173.
- Morris G., Berk M. The many roads to mitochondrial dysfunction in neuroimmune and neuropsychiatric disorders. BMC Med. 2015;1:13:68.
- Salminen A., Jouhten P., Sarajärvi T., Haapasalo A., Hiltunen M. Hypoxia and GABA shunt activation in the pathogenesis of Alzheimer’s disease. Neurochem Int. 2016;92:13-24. doi: 10.1016/j.neuint.2015.11.005.
- Bouche N., Fait A., Bouchez D., Møller S.G., Fromm H. Mitochondrial succinic-semialdehyde dehydrogenase of the gamma-aminobutyrate shunt is required to restrict levels of reactive oxygen intermediates in plants. Proc Natl Acad Sci U S A. 2023; 27;100(11):6843-8. doi: 10.1073/pnas.1037532100.
- Ravasz D., Kacso G., Fodor V., Horvath K., Adam-Vizi V., Chinopoulos C. Catabolism of GABA, succinic semialdehyde or gamma-hydroxybutyrate through the GABA shunt impair mitochondrial substrate-level phosphorylation. Neurochem Int. 2017;109:41-53. doi: 10.1016/j.neuint.2017.03.008.
- Kato T. Mitochondrial dysfunction and bipolar disorder. Curr TOP Behav Neurosci. 2011;5:187-200.
- Lamigeon C., Prod’Hon C., De Frias V., Michoudet C., Jacquemont B. Enhancement of neuronal protection from oxidative stress by glutamic acid decarboxylase delivery with a defective herpes simplex virus vector. Exp Neurol. 2003;184(1):381-92. doi: 10.1016/s0014-4886(03)00400-x.
- Kesebir S., HaJiyeva G., Guliyev E., Yosmaoğlu A. Bipolarity Trait Index. Bipolar Disord. 2022; 24: 47-48.
- Cavalcanti-de-Albuquerque J.P., de-Souza-Ferreira E., de Carvalho D.P., Galina A. Coupling of GABA Metabolism to Mitochondrial Glucose Phosphorylation. Neurochem Res. 2022;47(2):470-480. doi: 10.1007/s11064-021-03463-2.
- Kesebir S., Tatlıdil Yaylacı E., Süner O., Gültekin B.K. Uric acid levels may be a biological marker for the differentiation of unipolar and bipolar disorder: the role of affective temperament. J Affect Disord. 2014;165:131-4. doi: 10.1016/j.jad.2014.04.053.
- Kesebir S. (2022) Bipolarity Trait Index. Bipolar Disorder, 21: 72.
- Kesebir S., Demirer R.M. Reclassification of Mood Disorders with Comorbid Medical Diseases based on Sinai-Ruelle-Bowen/ SRB Entropy Measures. Medical Research Archives. 2023;11(12) https://doi.org/10.18103/mra.v11i12.4881.
- Martínez-Cagigal V. Multiple Testing Toolbox. MATLAB Central File Exchange (2021) (https://www.mathworks.com/matlabcentral/fileexchange/70604-multiple-testing-toolbox).
- Goodwin, F.K, Jamison, K.R. Manic-Depressive Illness. Second Edition. Oxford University Press. 2007; Newyork.
- Kappelmann N., Lewis G., Dantzer R., Jones P.B., Khandaker G.M. Antidepressant activity of anti-cytokine treatment: a systematic review and meta-analysis of clinical trials of chronic inflammatory conditions. Mol Psychiatry. 2018;23(2):335–343.
- Binks S. Distinct HLA associations of LGI1 and CASPR2-antibody diseases. Brain. 2018;141(8):2263–2271.
- Mass E. A somatic mutation in erythro-myeloid progenitors causes neurodegenerative disease. Nature. 2017;549(7672):389–393.
- Kesebir S. Depresyonda nörobiyolojik açıdan tanı ve tedavide yeni gelişmeler. Psikiyatride Güncel. 2022; 12(3): 244-52.
- Tatlidil Yaylaci E., Kesebir S., Güngördü Ö. The relationship between impulsivity and lipid levels in bipolar patients: does temperament explain it? Compr Psychiatry. 2014; 55(4):883-886.
- Turan C., Kesebir S., Süner O. Are ICAM, VCAM and E-selectin levels different in first manic episode and subsequent remission? J Affect Disord. 2014;163:76-80. doi: 10.1016/j.jad.2014.03.052.
- Dargél A.A., Volant S., Saha S., Etain B., Grant R., Azorin J.M., Gard S., Bellivier F., Bougerol T., Roux P., Aubin V., Courtet P., Leboyer M. & FACE-BD collaborators, Scott J., Henry C. Activation Levels, Cardiovascular Risk, and Functional Impairment in Remitted Bipolar Patients: Clinical Relevance of a Dimensional Approach. Psychother Psychosom. 2019;88(1):45-47.
- Robert H., Cornier M.A. Update on the NCEP ATP-III emerging cardiometabolic risk factors. BMC Med. 2014;12: 115.
- Kesebir S. Epigenetics of Metabolic Syndrome as a Mood Disorder. J Clin Med Res. 2018;10(6):453-460. doi: 10.14740/jocmr3389w.
- Güven S., Kesebir S,, Demirer R.M., Bilici M. Electroencephalography Spectral Power Density in First-Episode Mania: A Comparative Study with Subsequent Remission Period. Noro Psikiyatr Ars. 2015;52(2):194-197. doi: 10.5152/npa.2015.7180.
- Kesebir S., Demirer R.M., Tarhan N. CFC delta-beta is related with mixed features and response to treatment in bipolar II depression. Heliyon. 2019;13e01898. doi: 10.1016/j.heliyon.2019.e01898.
- Kesebir S., Vahip S., Akdeniz F., Yüncü Z., Alkan M., Akiskal H. Affective temperaments as measured by TEMPS-A in patients with bipolar I disorder and their first-degree relatives: a controlled study. J Affect Disord. 2005;85(1-2):127-33. doi: 10.1016/j.jad.2003.10.013.
- Vahip S., Kesebir S., Alkan M., Yazici O., Akiskal K.K., Akiskal H.S. Affective temperaments in clinically-well subjects in Turkey: initial psychometric data on the TEMPS-A. J Affect Disord. 2005;85(1-2):113-25. doi: 10.1016/j.jad.2003.10.011.
- Kesebir S. Comorbid impulse control disorder in bipolar disorder: the role of antidepressants. Turk Psikiyatri Derg. 2012;23(1):71.
- Kesebir S., Yosmaoglu A., Tarhan N. A dimensional approach to affective disorder: The relations between Scl-90 subdimensions and QEEG parameters. Front Psychiatry. 2022;15;13:651008. doi: 10.3389/fpsyt.2022.651008.
- Demirer R.M., Kesebir S. The entropy of chaotic transitions of EEG phase growth in bipolar disorder with lithium carbonate. Sci Rep. 2021;4;11(1):11888. doi: 10.1038/s41598-021-91350-9.
- Tsuda I., Fujii H. A complex systems approach to an interpretation of dynamic brain activity I: chaotic itinerancy can provide a mathematical basis for information processing in cortical transitory and nonstationary dynamics. In Summer School on Neural Networks (2003).