





Eleven-Year Analysis of Left Ventricular Endocardial Pacing
Left ventricular endocardial pacing in the real world: Eleven years of experience at a single center
Juan J. García Guerrero1*, Joaquín Fernández de la Concha Castañeda1, Antonio Chacón Piñero1, Manuel Doblado Calatrava1, Manuel Durán Guerrero1
1.Department of Cardiology at Hospital Universitario de Badajoz, Badajoz, Spain.
e-mail: [email protected]
OPEN ACCESS
PUBLISHED: 30 November 2024
CITATION: Guerrero, JJG., Castañeda, JFC, et al., 2024. Left ventricular endocardial pacing in the real world: Eleven years of experience at a single centre. Medical Research Archives, [online] 12(11).
https://doi.org/10.18103/mra.v12i11.5954
COPYRIGHT: © 2024 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v12i11.5954
ISSN 2375-1924
ABSTRACT
Background. Left ventricular (LV) endocardial lead implantation is feasible for cardiac resynchronization therapy when conventional implantation fails due to anatomical or technical issues or when venous implantation is performed but the patient does not respond to therapy.
Methods. Data, including age, sex, clinical characteristics, anticoagulant use, previous device implantations, indications, technique used, lead model, complications, and clinical and echocardiographic outcomes as well as electrical LV lead measurements were analysed for all patients who underwent endocardial LV lead implantation for biventricular pacing due to failed conventional implantation or nonresponse between April 2011 and April 2022.
Results. An active endocardial LV lead was implanted in 55 patients during the study period, without significant complications. No dislodgements or severe complications related to the implantation procedure occurred during the follow-up period (64±35 months), and a high percentage of patients responded to therapy, as assessed by several indicators.
Conclusions. Endocardial LV lead implantation is feasible when the conventional technique fails or is not effective. Most patients responded to the therapy without significant complications.
Keywords: Left ventricular endocardial pacing; Transseptal approach; Cardiac resynchronization therapy.
Introduction
Cardiac resynchronization therapy (CRT) reduces the risks of morbidity and mortality in patients with heart failure and a wide QRS. However, 20–30% of patients are considered nonresponders¹–³. The standard technique involves the implantation of a left ventricular (LV) lead into one of the tributary veins of the coronary sinus (CS), but the benefits of CRT depend on the correct implantation of an atrio-biventricular pacing system to achieve effective resynchronization. Even with the use of appropriate tools by an experienced operator, 3.6% to 8.4% of attempts to successfully implant a lead into the CS fail⁴–⁶, and the final location of the lead can vary on the basis of the venous anatomy of the heart. Moreover, despite the successful implantation of the lead for CRT, complications that may require the discontinuation of CRT or even the extraction of the entire system may occur. In many of these patients, the second attempt fails, and subsequent attempts are not recommended on the basis of increased risks for the patient, resulting in a poor outcome⁷. Although surgery under general anaesthesia is considered a high-risk procedure, it is considered an alternative approach for direct LV lead placement⁴. In the ALSYNC study, researchers reported that, of the patients who underwent endocardial LV lead placement, 55% experienced a ≥15% reduction in the left ventricular end-systolic volume (LVESV), and 64% experienced a ≥5% increase in the left ventricular ejection fraction (LVEF). Moreover, patients who were considered nonresponders to venous CRT exhibited improvements similar to those whose previous CRT failed⁸.
The aim of this study was to describe the usefulness and safety of LV endocardial pacing as part of our usual practice. Over time, we used four different techniques and hypothesized that, regardless of the aspects of each one, the benefits, implant success and complication rates would be similar among all four surgical procedures. Thus, we present the outcomes of and experience with the endocardial approach over an eleven-year period in our centre. We began using the technique in April 2011.
Methods
Patients with dilated cardiomyopathy from any cause, an LVEF ≤35%, a wide QRS (≥120 ms) and considered New York Heart Association (NYHA) class II, III, or IV on an optimal medical treatment underwent endocardial LV lead implantation. In all cases, implantation of a conventional venous CRT system had failed, or the patients had not responded to therapy; nonresponse was defined as a <15% reduction in end-systolic LV volume, persistent NYHA class III–IV, and a nonlateral position of the previous LV lead. All patients were informed about the need for and alternatives to the procedure and provided written informed consent.
IMPLANT PROCEDURE. We recorded the baseline characteristics (age, sex, clinical characteristics, anticoagulant use) and the details of the implantation procedure (indication, technique used, lead model, complications) for all patients who underwent endocardial LV lead implantation between April 2011 and April 2022.
Four different techniques were used: three were used to puncture the interatrial septum (IAS), as described by Van Gelder⁹, Elencwajg¹⁰, and Calvo¹¹, and one was used to puncture the interventricular septum (IVS), as described by Gamble¹². A description of the characteristics of each technique is shown in Table 1.
Table 1. Characteristics of the implantation techniques used
Technical detail — Number of cases (n = 55)
Type of access
Femoral — 12
Superior — 43
Septal puncture site
IAS — 13
IVS — 42
Tools for septal puncture
Brockenbrough needle (IAS) — 12
LA-Crosse system (IAS) — 1
Stiff side of the Agilis guidewire (IVS) — 42
Lead recovery system
Femoral-subclavian sheath — 6
Silk suture — 5
Recovery not needed — 44
IAS: Interatrial septum; IVS: Interventricular septum
Briefly, the IAS techniques described by Van Gelder⁹ and Elencwajg¹⁰ are very similar. First, the interatrial septum is punctured via the usual femoral approach, with a Brockenbrough needle. A transseptal sheath, which was modified to be easily split, is passed over the wire inside the left atrium to the LV cavity, crossing the mitral valve. A long active fixation lead was implanted into the LV lateral endocardial tissue. Once the sheath is removed, the lead must be pulled back to the subclavian area to be attached to the generator. The technique described by Van Gelder involves passing a long sheath through the subclavian vein, emerging at the femoral aspect and fixing the pin of the lead to an inner catheter. The catheter is retrieved at the same time as the long sheath, and then the lead is extracted through the subclavian vein. In the Elencwajg technique, the snare, which hooks the suture attached to the connector pin on the LV lead, is pulled back until the pin passes through the skin of the subclavian aspect.
The LA-Crosse system (St. Jude Medical. St. Paul, Minnesota, USA) is used in the third IAS technique described by Calvo¹¹. This special tool can cross the interatrial septum via the usual left subclavian vein approach and has a screw that perforates the septum and facilitates the insertion of a wire into the left atrium. A slittable sheath able to cross the mitral valve is then inserted to deliver the lead to the LV endocardium. As a standard upper approach is used as part of this technique, lead recovery is not needed.
Finally, in the IVS technique described by Gamble¹², an Agilis steerable sheath (St. Jude Medical) is introduced into the RV cavity, where its tip is steered to the interventricular septum. Once the tip is correctly positioned against the septum, the stiff end of the wire can be inverted and used to perforate the septum. Once the catheter is inside the LV cavity, a high-support wire is introduced, the Agilis catheter is removed, and a steerable, slittable sheath is inserted, allowing delivery of the lead to the lateral LV endocardium. The location of the LV lead crossing the septum and inside the LV cavity was monitored with intracardiac echocardiography (ICE) in every transventricular case to ensure the correct position of the wire inside the LV. The final position of the LV lead was classified using 3 X-ray views: lateral, right anterior oblique (RAO) and left anterior oblique (LAO), dividing the cardiac silhouette in every view into 3 equal sectors (lateral: anterior, posterior).
Table 2. Baseline patient characteristics (n = 55)
General characteristics
Sex (male), n (%) — 38 (69%)
Age (years) — 79 ± 8.9
Medical history and medication
Aetiology, n (%)
Idiopathic — 41 (74.5%)
Ischaemic — 11 (20%)
Valvular — 3 (5.5%)
Atrial fibrillation, n (%) — 12 (21.8%)
CHA₂DS₂-VASc — 3.5 ± 1.4
Anticoagulants, n (%) — 23 (41.8%)
QRS morphology
True LBBB — 45 (81.8%)
LBBB POST-RVP — 8 (14.5%)
Narrow QRS — 2 (3.6%)
QRS duration (ms) — 161 ± 28
NYHA class, n (%)
II — 4 (7.2%)
III — 43 (78.1%)
IV — 4 (7.3%)
IV-Inotropic therapy — 4 (7.3%)
LVEF — 28.2 ± 7.0
LVESV (mL) — 141 ± 70.4
LBBB: Left bundle branch block. LBBB POST-RVP: LBBB due to right ventricle pacemaker stimulation. NYHA: New York Heart Association. IV-Inotropic therapy: patients with NYHA class IV intravenous inotropic agents. LVEF: Left ventricular ejection fraction. LVESV: Left ventricular end-systolic volume
Implantation Characteristics
Fifty-five patients underwent the procedure, and the LV endocardial lead was successfully implanted in all of them, although two patients required a second attempt. We used the Van Gelder technique in 7 patients, Jurdham in 5 patients, Calvo in 1 patient, and Gamble in 42 patients. The mean implantation time was 95 ± 44.6 min (range 225–30), and the mean fluoroscopy time was 20 ± 14.3 min (range 90–2). A defibrillator system was implanted in 49 patients (89%) who underwent CRT. A total of 55 electrodes manufactured by St. Jude Medical (St. Jude Medical, Inc., Sylmar, CA, USA) and Medtronic (Medtronic, Inc., Minneapolis, MN, USA) were implanted. Three different LV lead models were used: Medtronic 3830 in 7 patients, Medtronic 5076-85 in 2 patients, and St. Jude 2088TC-100 in 46 patients. The LV lead electrical measurements at the end of implantation were as follows: mean impedance, 679 ± 184 ohm (range, 1185–310); mean R wave, 11.1 ± 4.8 mV (range, 23–4.8); and mean threshold (at 0.4 ms), 0.8 ± 0.27 V (range, 1.9–0.50). The final position of the tip of the LV lead is shown in Table 3.
Table 3. Left ventricular lead position (X-ray views, n = 49*)
LATERAL (n = 49)
Anterior — 2 (4.1%)
Medium — 11 (22.5%)
Posterior — 36 (73.4%)
RAO (n = 43 #)
Apical — 2 (4.6%)
Mid-V — 29 (67.4%)
Basal — 12 (27.9%)
LAO (n = 43 #)
Superior — 13 (30.2%)
Lateral — 28 (65.1%)
Inferior — 2 (4.6%)
RAO: Right anterior oblique view. LAO: Left anterior oblique view.
*: Six patients had no postimplant X-ray.
#: Nine patients whose X-ray images were available had no RAO or LAO views.
The right femoral vein was punctured in 13 patients (interatrial septum puncture), and the LV lead was placed alongside the generator in the left subclavian aspect in 9 patients and the right aspect in 2 patients. The generator was placed in the right upper thigh in 2 patients, with no need to recover the lead. Venous access was established through the upper venous tree (i.e., axillary or subclavian veins) in 42 patients (interventricular septum puncture), on the left side in 33, and on the right side in 9.
No deaths or severe complications (i.e., those that required an intervention procedure or prolonged hospitalization for proper management) occurred as a result of the implantation procedure. One patient required oral intubation prior to the procedure due to respiratory arrest. One patient experienced decompensated left ventricular failure and was treated per protocol without additional problems. Ventricular fibrillation developed as the guidewire crossed the interventricular septum in one patient, who was successfully defibrillated. There was one case of acute LV electrode dislodgement at the end of the implant procedure, and the electrode was later successfully reimplanted in a second procedure. One patient experienced unstable angina during the procedure before the septum was punctured. The intervention was halted, and a second attempt two months later was successful. One patient had a small pericardial effusion without any haemodynamic consequences, which disappeared within a few days without treatment.
Thirty-eight patients were treated with acenocoumarol, a traditional oral anticoagulant (OAC) widely used in Spain. The first dose of acenocoumarol was administered on the day after the procedure with the aim of achieving an INR of 2–3. Fourteen patients were treated with new OACs, as this type of treatment was first administered in 2017. Two mild pocket haematomas and one moderate pocket haematoma were treated with conservative measures.
Three patients died before discharge; however, these deaths were not considered related to the implant procedure. All of the patients had previously received intravenous inotropic therapy. One patient died due to electromechanical dissociation (post-implantation complications were ruled out during resuscitation), and the remaining 2 deaths were due to refractory right heart failure. Most patients (34/52) were discharged ≤4 days after implantation. The mean time to discharge after implantation was 3.8±2.4 days (range 12–1). Prolonged hospital stays were mainly due to decompensated heart failure treatment and close follow-up of patients not previously treated with OACs.
FOLLOW-UP
The data of 51 patients were extracted from our database; one patient was lost to follow-up less than 1 year after the implantation procedure and was not included in the analysis.
CLINICAL OUTCOMES
Of the 51 discharged patients analysed, 23 (45.9%) had an uneventful outcome. 14 (27.4%) were readmitted to the hospital at least once, 7 (13.7%) were readmitted due to malignant arrhythmias properly treated by the defibrillator, and 7 (13.7%) patients were readmitted due to decompensated heart failure.
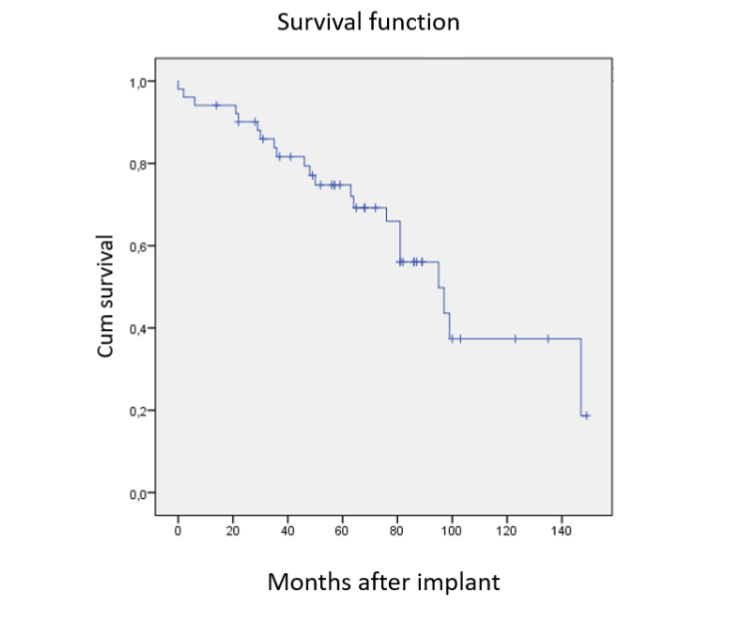
Twenty-two patients (43.1%) died during the follow-up period: 3 due to decompensated heart failure, 1 after multiple defibrillator shocks due to an arrhythmic storm, 3 due to myocardial infarction, 2 due to pneumonia, 3 due to cancer, 3 due to multiorgan failure, 2 due to COVID-19, 6 due to unknown causes, and 1 due to an unexplained sudden death two days after implantation. Among the patients who died, eleven did not have any previous complications. The overall mortality plot is shown in Figure 1.
The mean length of follow-up was 64±35 months (range 149–0) overall, 61±34 months (range 100–6) in patients who experienced events, 73±38 months (range 149–14) in patients who did not experience events, and 48±32 (range 99–0) months in patients who died during the follow-up period. Of the 23 patients who did not experience events, 7 required surgery for scheduled battery replacement; the mean time from implantation to battery replacement was 82±31.2 (range 47–135) months. One patient underwent two replacement surgeries, one at 56 months and one at 135 months after implantation. It was not necessary to replace the electrodes in either of these cases.
Figure 1. Kaplan–Meier curve depicting overall mortality
Among the three nonresponders who underwent implantation, two improved from NYHA class III to I and were responders according to the LVEF and LVESV criteria. The third patient exhibited improvement in terms of the NYHA class but experienced an arrhythmic storm three months after implantation, with multiple defibrillator shocks, and died due to refractory cardiogenic shock.
Mitral regurgitation impairment related to endocardial LV lead implantation was observed. The clinical, electrocardiographic and echocardiographic outcomes are shown in Table 4.
Table 4. Clinical and echocardiographic outcomes
| Baseline | 6–12 months | Change | P value | Response rate | |
|---|---|---|---|---|---|
| NYHA (n: 53) III/II/IV/IV-in (%) | 7.2/78.2/7.2/7.2 | 41.5/47.2/5.6/1.9/3.8 | 88.7% | ||
| QRS width | 161±27 ms | 111±6 ms | -49.5±28 | <0.0001 | |
| LVEF (n:44) | 28.5±7% | 41.9±14% | -13±11 | <0.0001 | 81.8% |
| LVESV (n:23) | 133±76 mL | 72±87 mL | -60.3±38 | <0.0001 | 82% |
| MR (n:30) | 0/I/II/III (n) 4/14/8/4 | 0/I/II/III (n) 4/15/8/4 |
NYHA: New York Heart Association class. IV-in: NYHA class IV intravenous inotropic agents. LVEF: Left ventricular ejection fraction. LVESV: Left ventricular end-systolic volume. MR: Mitral regurgitation
There were no differences in outcomes related to the technique used. None of the patients experienced septic episodes, lead dislodgement or fracture.
Three patients suffered a transient ischaemic attack without permanent sequelae: one patient on the day after implantation, which was attributed to left carotid subtotal stenosis and was successfully treated with surgery several days after the episode with no more incidents, and two patients whose OAC treatment was incorrectly stopped. These patients did well after the treatment was resumed.
ELECTRICAL OUTCOME
The electrical performance of the LV lead during the follow-up period is shown in Table 5. There were no significant differences in the performances of the three lead models used.
Table 5. Follow-up LV lead electrical performance (n = 51)
Impedance (Ohms) — 412±107 (684–130)
Threshold (Volts) — 1.2±0.54 (3.5–0.3)
Threshold (ms) — 0.31±0.10 (1.0–0.1)
Output (Volts) — 2.0±0.49 (5.0–1.0)
Output (ms) — 0.31±0.10 (1.0–0.2)
Discussion
Cardiac resynchronization therapy significantly reduces the incidences of morbidity and mortality in patients with advanced heart failure, a wide QRS and optimal medical treatment, but a substantial proportion of patients whose implantation procedure was successful do not experience any clinical benefits¹–³, and 2.4–5.4% of coronary sinus lead implantation procedures are unsuccessful⁶. When the lead is implanted after device extraction, the implant failure rate is 11.9%⁷.
In an effort to implant LV leads using the easiest method and via the shortest pathway, we used 4 different techniques⁹–¹¹,¹⁹, and selected the one we considered the most effective with the most reliable results.
Endocardial LV lead implantation was successful in 100% of the patients in our series, and only 2 required a second attempt (due to LV electrode dislodgement and unstable angina, respectively, during the initial procedure). The rate of successful implantation was also 100% in several large published series²⁰–²³; however, the ALSYNC series⁸ was the largest and had an 89.4% success rate. We used ICE to monitor the position of the LV lead in the 42 procedures we performed and considered it helpful²⁴ during IVS puncture; nevertheless, the researchers who reported the first procedure using this technique¹² and those who performed the procedure in a series of 20 patients achieved similar success rates (100%) without this additional element²⁰. The outcomes of endocardial LV lead implantation in a series of 20 or more patients have been recently reported²⁰–²³. Our mean implantation and fluoroscopy times were comparable to those of the procedures performed in the abovementioned series of patients.
The LV leads implanted in our series of patients were stable and had quite low output values, indicating extended battery longevity (Table 5).
Overall, our patients could be considered a very high-risk group (85% were NYHA class III–IV, the mean LVEF was 28%, and the mean CHA₂DS₂-VASc score was 3.5). Eight patients (15.6%) were NYHA class IV, four of whom received intravenous inotropic agents, 3 of whom experienced cardiogenic shock, and endocardial LV pacing was considered a last-resort therapy. These 3 very sick patients died in the hospital after the procedure.
Our patients remained free of severe procedure-related complications (LV lead dislodgements or fractures or infective complications) throughout the 12-year study period (mean follow-up period of 64±35 months). Infective complications requiring extraction of the LV endocardial lead are of particular concern because a surgical procedure is recommended²⁵ to avoid possible embolic complications. Notably, Bahadorani et al.²⁶ reported a case in which 2 leads, wrongly located in the left cardiac chambers, were extracted via a complete cerebral embolic protection system without complications.
The response rate in our discharged patients was quite high, on the basis of the predefined values: 88.7% improved by ≥1 NYHA class, 82% experienced a decrease in their LVESV ≥15% and 81.8% exhibited an increase in their LVEF ≥5%. This outcome was reflected in a significantly reduced QRS width (49.5±28 ms, p<0.0001), which is related to a good chance of a clinically relevant response²⁷ and is comparable to previous reports²⁰–²³. Most (66.6%) of our discharged patients did well, with no further admissions and improved NYHA class; fourteen (27.4%) of our patients were readmitted due to decompensated heart failure or malignant ventricular arrhythmias, and 5 of them eventually died (3 due to refractory heart failure). These outcomes resemble those in other reports²⁰–²³ in which the procedure was 100% successful and there were no important complications. As we hypothesized, we did not find any significant differences in outcomes, complications or benefits related to the implantation technique used.
It is likely that the final position of our LV leads (95.9% in the medium or posterior position in the lateral view, 95.3% in the nonapical position in the RAO view and 100% in the lateral position in the LAO view) had an impact on our patients’ good clinical results.
Our series included only three previous nonresponders, and two of them had a good response to therapy. These successful outcomes concurred with the findings of the ALSYNC study by Morgan et al.⁸, in which the rate of successful endocardial LV lead implantation in nonresponders was similar to that in patients whose previously placed CS-epicardial implant failed. The percentage of nonresponders (5.4%) included in our series of patients we enrolled as of April 2011 was smaller than that included in the ALSYNC study (23%) because we only began to include previous nonresponders in late 2015. The decision to include previous nonresponders was initially based on a case report published by Bracke et al.²⁸ and then supported by the good results observed in the nonresponders in the ALSYNC study⁸; additional evidence was provided by Biffi et al. in 2018, as the ALSYNC team noted that they made LV lead location decisions empirically in nonresponders, with the goal of avoiding scarring²⁹. In our series, we used anatomical criteria for endocardial LV lead placement in 3 patients who were previously nonresponders and whose LV leads were placed in suboptimal locations. Numerous other methods have been described. Bracke et al. published a successful protocol (using dP/dTmax measurements) to assess the acute haemodynamic (AHR) response associated with alternative endocardial LV pacing sites, comparing the success of the published protocol with that of one implanted CS-epicardial system in one nonresponder²⁸. The same team studied 24 clinical nonresponders via improvements in dP/dTmax and Q-LV interval to measure the AHR associated with different LV endocardial sites³⁰. Behar et al.³¹ combined magnetic resonance imaging, electroanatomic contact mapping, and AHR studies and reported the superiority of endocardial pacing over epicardial venous pacing when both were optimized using AHR. In other studies, researchers tested a guided LV lead implantation in an effort to correlate the best AHR with a previous real-time X-MRI study³² or cardiac computed tomography imaging³³ and thereby identified sites outside the scar area that showed the latest mechanical activation. Although the latter studies involved a small sample of patients (14 and 18, respectively), these methods of guided LV lead implantation were associated with a good correlation between the predicted LV stimulation site and the electrical outcome³² or AHR³³. More research is needed to determine how to reliably select the best site for LV lead pacing in previously nonresponders.
Some studies have revealed a significant benefit of LV endocardial pacing over CS-epicardial pacing, especially when pacing at the optimal site, which is usually patient-specific³⁴–³⁵. In a recent meta-analysis, Gamble et al.⁶ reported that only a few studies involved a sample of patients larger than our sample of 55 patients and reported the outcomes of the transvenous LV lead technique. In their analysis, the position of the lead was revealed in only 29% of the studies, and the authors reported that 68% of the LV leads were in a lateral or posterolateral location in the early period of CRT, with a shift to 81% in the late period. These data indicate the probable rather common suboptimal placement of LV leads and therefore a suboptimal haemodynamic response in a high percentage of the few studies that incorporated this variable. In our opinion, avoiding the limitations of conventional LV lead implantation via the tributary veins is the main advantage of LV endocardial pacing.
The overall mortality rate during the 12-year study period was 43%, which was much higher than that reported in the ALSYNC study (28.1%)⁸, by Gamble (15.0%)⁶, by Elencwajg (29%)¹⁰, and by our own group in 2019 (19%)³, but less than that reported by Gellér (50%)²¹. We can explain these differences in our much longer mean follow-up period (64±35 months), which is, to our knowledge, the longest reported to date in a study involving more than 20 patients with an endocardial LV lead²⁰–²³. Notably, the mean follow-up time to death was 55±37 months, the longest of these series.
Inadvertent LV pacing has been related to thromboembolic episodes³⁶–³⁷. These leads are exposed to the systemic circulation, increasing the risk of systemic thromboembolism. Three of our patients (5.8%) suffered transient ischaemic attacks, all of whom recovered well; two cases were suspected to have an embolic source. The mean CHA₂DS₂-VASc score (3.5±1.4) suggests a potentially high thromboembolism event rate in our population, but only 2 cases of embolic episodes occurred, both of which were associated with inappropriate…
Cessation of OAC therapy. Similarly, many studies have confirmed that most strokes and transient ischaemic events occur in periods of reduced OAC effects²⁸,³⁰,³⁸. A retrospective dual-centre study by Rademakers et al.³⁹ was designed to determine the long-term incidence of thromboembolism in LV endocardial patients. At a median follow-up of 24 months, the 51 included patients had 6.1 thromboembolic events per 100 patient-years, with 1 death due to post-stroke complications. Treatment with OACs appeared to be effective in reducing thromboembolic risk when an adequate INR was maintained. In a recent meta-analysis, Graham et al.³⁸ gathered 15 studies comprising 362 patients with LV endocardial leads and reported a stroke rate of 3.3–4.2 per 100 patient-years, suggesting a potentially higher rate of stroke than that in similar cohorts, but this high incidence of stroke was only noted in transapical LV endocardial leads. Additional studies are needed to explain the differences in the rates of thromboembolism reported in the literature to date, including the low rate reported in our series. Recently, we have added new OACs to the treatment regimen for these patients owing to their well-known stable effect and ability to significantly reduce the embolic episode rate.
Recently, some techniques called “physiological pacing” have been used to treat patients with an indication for CRT, and left bundle branch pacing (LBBP) has been compared with biventricular standard pacing (BiVP)⁴⁰,⁴¹. This type of procedure is designed to directly pace the conduction system, with the aim of bypassing the blockage area, thus provoking electrical–mechanical dyssynchrony and detrimental haemodynamic effects. Some authors may wonder whether this new technique should be considered the new gold standard for CRT⁴². However, there are still significant procedural limitations and complexities that warrant the modification of current techniques or the development of new techniques. Caveats, such as a high rate of high pacing threshold revisions, have limited the use of His pacing, and recent comparisons of LBBP outcomes and BiVP outcomes have revealed encouraging results; however, there is currently a lack of sufficient evidence to support its use instead of BiVP. Moreover, the rate of successful implantation via this technique is approximately 80%⁴². According to recent guidelines on cardiac physiologic pacing for the avoidance and mitigation of heart failure, BiVP is recommended for patients with an indication for CRT, and physiological pacing is recommended only when BiVP fails⁴³. Derndorfer et al.⁴² believe that BiVP can “coexist peacefully” with “conduction pacing” techniques in CRT. If BiVP fails, we believe that an endocardial lead should be implanted owing to its 100% success rate in several series, good response rate, and low number of complications. We hope that this technique can be considered an alternative for failed BiVP or nonresponders.
Limitations
Definitive conclusions could not be drawn because of the small number of patients and insufficient evidence. Our analysis is based on clinical data and clinical judgement, which introduces the potential for selection bias because patients were not recruited according to a prespecified protocol; furthermore, there was no control group. This precludes the comparison of patient outcomes in our study with those of similar studies in which an endocardial LV lead was not implanted and therefore limits the use of our findings in selecting patients for LV endocardial procedures.
Conclusions
Endocardial LV lead implantation is feasible and beneficial for patients whose previous conventional CS-epicardial lead implantation failed and those considered nonresponders. In our opinion, an appropriately trained and experienced operator can successfully implant endocardial LV leads, leading to a good response rate and few complications. However, the long-term outcomes and complications have yet to be revealed, and new studies addressing these issues are needed to thoroughly assess the benefits and safety of the procedure.
Conflict of Interest:
None.
Funding Statement:
None.
Acknowledgements:
Berry van Gelder, F.A. Bracke, and Tim Betts, for being so kind to come to our hospital to teach us their techniques.
Disclosure:
JJGG and JFCC received fees for lectures and advice from St. Jude Medical, Medtronic and Boston Scientific.
Abbreviations.
LV: Left ventricle. CRT: Cardiac resynchronization therapy.
CS: Coronary sinus. OAC: Oral anticoagulation.
INR: International normalized ratio.
References
1. Bristow MR, Saxon LA, Boehmer J, et al. Cardiac-resynchronization therapy with or without an implantable defibrillator in advanced chronic heart failure. N Engl J Med 2004;350:2140-50. DOI: 10.1056/NEJMoa032423
2. Cleland J, Daubert J, Erdmann E, et al. The effect of cardiac resynchronization on morbidity and mortality in heart failure. N Engl J Med 2005;352:1539-49. DOI: 10.1056/NEJMoa050496
3. Moss AJ, Jackson Hall, Cannom DS. Cardiac-resynchronization therapy for the prevention of heart-failure events. N Engl J Med 2009;361:1329-38. DOI: 10.1056/NEJMoa0906431
4. León AR, Abraham WT, Curtis AB, et al. Safety of transvenous cardiac resynchronization system implantation in patients with chronic heart failure: Combined results of over 2,000 patients from a multicenter study program. J Am Coll Cardiol 2005; 46:2348- 2356. DOI: 10.1016/j.jacc.2005.08.031
5. Gras D, Böcker D, Lunati M, et al. Implantation of cardiac resynchronization therapy systems in the CARE-HF trial: Procedural success rate and safety. Europace 2007; 9:516-522. DOI: 10.1093/europac e/eum080
6. Gamble JHP, Herring N, Ginks M, et al. Procedural success of left ventricular lead placement for cardiac resynchronization therapy: A meta-analysis. J Am Coll Cardiol EP 2016;2:69-77. DOI: 10.1016/j.jacep.2015.08.009
7. Rickard J, Tarakji K, Cheng A, et al. Survival of Patients With Biventricular Devices After Device Infection, Extraction, and Reimplantation. J Am Coll Cardiol HF 2013;1:508-513. DOI: 10.1016/j.jc hf.2013.05.009
8. Morgan JM, Biffi M, Gellér L, et al. ALternate Site Cardiac ResYNChronization (ALSYNC): A prospective and multicentre study of left ventricular endocardial pacing for cardiac resynchronization therapy. Eur Heart J 2016; 37:2118-2127. DOI: 10.1093/eurheartj/ehv723
9. Van Gelder BM, Houthuizen P, Bracke F. Transseptal left ventricular endocardial pacing: preliminary experience from a femoral approach with subclavian pull-through. Europace 2011;13:14 54-1458. DOI: 10.1093/europace/eur136
10. Elencwajg B, López Cabanillas N, Cardinali EL, et al. The Jurdham procedure: Endocardial left ventricular lead insertion via a femoral transseptal sheath for cardiac resynchronization therapy pectoral device implantation. Heart Rhythm 2012; 9:1798-1804. DOI: 10.1016/j.hrthm.2012.07.010
11. Calvo N, Arguedas H, Canepa JP, et al. Endocardial left ventricular lead placement from the left subclavian vein approach. Europace 2014; 16:1857-1859. DOI: 10.1093/europace/euu123
12. Gamble JHP, Bashir Y, Rajappan K, et al. Left ventricular endocardial pacing via the interventricular septum for cardiac resynchronization therapy: First report. Heart Rhythm 2013; 10:1811. DOI: 10.1016 /j.hrthm.2013.07.033
13. Elliott M, Mehta V, Sidhu B, et al. Endocardial left ventricular pacing. Herz 2021;46:526-532. DOI: 10.1007/s00059-021-05074-7
14. Santos H, Santos M, Almeida I, et al. A systemic review of endocardial left ventricular pacing. Heart & Lung 2022; 51:82-86. DOI: 10.1016/j.hrtlng. 2021.10.003
15. Gamble JHP, Herring N, Ginks M, et al. Endocardial left ventricular pacing for cardiac resynchronization: systematic review and meta-analysis. Europace 2018; 20:73-81. DOI: 10.1093 /europace/euw381
16. Jaïs P, Douard H, Shah DC, Barold S, Barat JL, Clémenty J. Endocardial biventricular pacing. Pacing Clin Electrophysiol 1998; 21:2128-2131. DOI: 10.1111/j.1540-8159.1998.tb01133.x
17. Pasquié JL, Massin F, Macia JC, et al. Long-term follow-up of biventricular pacing using a totally endocardial approach in patients with end-stage cardiac failure. Pacing Clin Electrophysiol 2007; 30:S31-S33. DOI: 10.1111/j.1540-8159.2007 .00599.x
18. Moriña-Vázquez P, Roa-Garrido J, Fernández-Gómez JM, et al. Direct left ventricular endocardial pacing: An alternative when traditional resynchronization via coronary sinus is not feasible or effective. Pacing Clin Electrophysiol 2013;36: 699-706. DOI: 10.1111/pace.12125
19. Betts TR, Gamble JHP, Khiani R, et al. Development of a technique for left ventricular endocardial pacing via puncture of the interventricular septum. Circ Arrhythmia Electrophysiol 2014;7:17-22. DOI: 10.1161/CIRCE P.113.001110
20. Gamble HP, Herring N, Ginks MR, et al. Endocardial left ventricular pacing across the interventricular septum for cardiac resynchronization therapy: Clinical results of a pilot study. Heart Rhythm 2018;15:1017-1022. DOI: 10.1016/j.hrthm. 2018.02.032
21. Gellér L, Sallo Z, Molnár L, et al. Long-term single-centre large volume experience with transseptal endocardial left ventricular lead implantation. Europace 2019; 21:1237-1245. OI: 10.1093/europace/euz116
22. Elencwajg B, López-Cabanillas N, Fischer A, et al. Multicenter prospective observational long-term follow-up study of endocardial cardiac resynchronization therapy using the Jurdham procedure. Heart Rhythm 2019;16:1453-1461. DOI: 10.1016/j.hrthm.2019.07.017
23. García Guerrero JJ, Fernández de la Concha Castañeda J, Doblado Calatrava, et al. Left ventricular endocardial pacing in the real world: Five years of experience at a single center. Pacing Clin Electrophysiol. 2019;42:153-160. DOI: 10.111 1/pace.13591
24. Doblado-Calatrava M, Sánchez-Quintana D, García Guerrero JJ, et al. Use of intracardiac echocardiography as a guide during interventricular septum puncture in a patient undergoing cardiac resynchronization therapy. Heart Rhythm Case Reports 2015; 1:345-347. DOI: 10.1016/j.hrcr.2015.06.003
25. Whinnett Z, Bordachar P. The risks and benefits of transseptal endocardial pacing. Curr Opin Cardiol 2012; 27:19-23. DOI: 10.1097/HCO.0b0 13e32834dc3d4
26. Bahadorani JN, Schricker AA, Pretorius VG, et al. Percutaneous extraction of inadvertently placed left-sided pacemaker leads with complete cerebral embolic protection. Catheter Cardiovasc Interv 2015;86:777-785. DOI: 10.1002/ccd.25826
27. Rickard J, Popovic Z, Verhaert D, et al. The QRS narrowing index predicts reverse left ventricular remodelling following cardiac resynchronization therapy. Pacing Clin Electrophysiol 2011; 34:604-611. DOI: 10.1111/j.1540-8159.2010.03022.x
28. Bracke F, Patrick Houthuizen, Rahel B, et al. Left ventricular endocardial pacing improves the clinical efficacy in a nonresponder to cardiac resynchronization therapy: role of acute haemodynamic testing. Europace 2010;12:1191-1192. DOI: 10.1093/ europace/euq043
29. Biffi M, Defaye P, Jaïs P, et al. Benefits of left ventricular endocardial pacing comparing failed implants and prior nonresponders to conventional cardiac resynchronization therapy: A subanalysis from the ALSYNC study. Int J Cardiol. 2018;15:2 59:88-93. DOI: 10.1016/j.ijcard.2018.01.030
30. Van Gelder BM, Nathoe R, Bracke FA. Haemodynamic evaluation of alternative left ventricular endocardial pacing sites in clinical non-responders to cardiac resynchronisation therapy. Neth Heart J 2016;24:85-92. DOI: 10.1007/s12471 -015-0773-7
31. Behar JM, Jackson T, Hyde E, et al. Optimized left ventricular endocardial stimulation is superior to optimized epicardial stimulation in ischemic patients with poor response to cardiac resynchronization therapy. J Am Coll Cardiol EP 2016; 2:799-809. DOI: 10.1016/j.jacep.2016.04.006
32. Behar JM, Mountney P, Toth D, et al. Real-time X-MRI-guided left ventricular lead implantation for targeted delivery of cardiac resynchronization therapy. J Am Coll Cardiol EP 2017;3:803-814. DOI: 10.1016/j.jacep.2017.01.018
33. Behar JM, Rajani R, Pourmorteza A, et al. Comprehensive use of cardiac computed tomography to guide left ventricular lead placement in cardiac resynchronization therapy. Heart Rhythm 2017;14:1364-1372. DOI: 10.1016 /j.hrthm.2017.04.041
34. Padeletti L, Pieragnoli P, Ricciardi G, et al. Acute hemodynamic effect of left ventricular endocardial pacing in cardiac resynchronization therapy: Assessment by pressure-volume loops. Circ Arrhythmia Electrophysiol 2012; 5:460-467. DOI: 10.1161/CIRCEP.111.970277
35. Sohal M, Shetty A, Niederer S, et al. Delayed trans-septal activation results in comparable hemodynamic effect of left ventricular and biventricular endocardial pacing. Insights from electroanatomical mapping. Circ Arrhythmia Electrophysiol 2014;7:251-258. DOI: 10.1161/CIR CEP.113.001152
36. Sharifi M, Sorkin R, Sharifi V, et al. Inadvertent malposition of a transvenous-inserted pacing lead in the left ventricular chamber. Am J Cardiol 1995; 76:92-95. DOI: 10.1016/s0002-9149(99)80812-1
37. Van Gelder BM, Bracke F, Oto A, et al. Diagnosis and management of inadvertently placed pacing and ICD leads in the left ventricle: a multicenter experience and review of the literature. Pacing Clin Electrophysiol 2000;23:877-883. DOI: 10.1111/j.1540-8159.2000.tb00858.x
38. Graham A, Providenica R, Honarbakhsh S, et al. Systematic review and meta-analysis of left ventricular endocardial pacing in advanced heart failure: Clinically efficacious but at what cost? Pacing Clin Electrophysiol. 2018;41:353-361. DOI: 10.1111/pace.13275
39. Rademakers LM, Van Gelder BM, Scheffer MG, et al. Mid-term follow up of thromboembolic complications in left ventricular endocardial cardiac resynchronization therapy. Heart Rhythm 2014; 11:609-613. DOI: 10.1016/j.hrthm.2014.01.031
40. Wang Y, Zhu H, Hou X, et al. Randomized trial of left bundle branch vs biventricular pacing for cardiac resynchronization therapy. J Am Coll Cardiol 2022;80:1205-1216. DOI: 10.1016/j.jacc. 2022.07.019
41. Zhu H, Qin C, Du A, et al. Comparisons of long-term clinical outcomes with left bundle branch pacing, left ventricular septal pacing, and biventricular pacing for cardiac resynchronization therapy. Heart Rhythm 2024;21:1342-1353. DOI: 10.1016/j.hrthm.2024.03.007
42. Derndorfer M, Kollias G, Martinek M, et al. Is conduction system pacing going to be the new gold standard for cardiac resynchronization therapy? J Clin Med 2024;13:4320. DOI: 10.3390/ jcm13154320
43. Chung MK, Patton KK, Lau C-P, et al. 2023 HRS/APHRS/LAHRS guideline on cardiac physiologic pacing for the avoidance and mitigation of heart failure. Heart Rhythm 2023;20 :e17-e83. DOI: 10.1016/j.hrthm.2023.03.1538