





Emergency Management of Acute Lower GI Bleeding
Emergency Management of Acute Lower Gastrointestinal Bleeding
Matthew G Dunckley, FRCS¹
- Department of General Surgery, Dartford & Gravesham NHS Trust, Dartford, UK
[email protected]
OPEN ACCESS
PUBLISHED: 31 March 2026
CITATION: Dunckley, MG., 2026. Emergency Management of Acute Lower Gastrointestinal Bleeding. Medical Research Archives, [online] 14(3).
COPYRIGHT: © 2026 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
ISSN 2375-1924
Abstract
Acute episodes of lower GI bleeding normally generate attendance at hospital emergency departments and require admission depending on bleeding severity. The differential diagnoses are extensive so diagnosis can be challenging but modern radiological, endoscopic and medical techniques have transformed diagnosis, treatment and outcomes. In modern practice, very few patients presenting with acute lower gastrointestinal haemorrhage now require surgical intervention as endoscopic or interventional radiological techniques have high success rates. Outcomes depend more significantly on co-morbidities, especially for elderly patients on anticoagulant drugs, as well as the ease of access to early diagnostic and therapeutic facilities. This review outlines the evidence base for the diagnosis and optimal management of acute lower gastrointestinal bleeding with reference to modern national and international guidelines.
Keywords
- Acute lower gastrointestinal bleeding
- Emergency management
- Endoscopy
- Interventional radiology
- Co-morbidities
Introduction
The majority of gastrointestinal bleeds originate from the oesophagus, stomach and jejunum but approximately 30% of bleeds occur in the lower gastrointestinal tract. Although this technically refers to all bowel distal to the ligament of Treitz, at least 90% of lower gastrointestinal bleeding arises from the colon and rectum. Most cases of lower gastrointestinal bleeds are chronic and asymptomatic, only being discovered during investigations for iron-deficiency anaemia or after a positive test for faecal occult blood in bowel cancer screening programmes. Iron deficiency anaemia due to gastrointestinal bleeding requires a blood loss greater than 5ml per day. Small bleeds may proceed for long periods of time until anaemia is sufficiently severe to cause clinical symptoms, such as dyspnoea, fatigue or cardiac arrhythmias. In many cases, the stool may appear macroscopically normal until lower gastrointestinal haemorrhage exceeds 100ml per day.
This review will focus on acute lower gastrointestinal bleeding, defined as the onset of bleeding within the previous 3 days of presentation. Such acute bleeds represent around 3% of all referrals to emergency clinicians and affect 20-33/100,000 adults per annum. Of these patients, around 70% stop bleeding spontaneously or with simple medical intervention and fewer than 10% patients become haemodynamically unstable. However, the quality of emergency management of these most severe patients has a major impact on their morbidity and mortality. Moreover, as acute lower gastrointestinal bleeding is significantly more common in the elderly population, having a median age of 74 years, it is unsurprising that their clinical outcomes are strongly influenced by co-morbidities, especially the use of anti-coagulant or anti-platelet medications. Up to 4% of high risk patients die during their acute admission. Patients who develop lower gastrointestinal bleeding while admitted to hospital for another reason are at particularly high risk of death, with up to a 13% mortality rate.
The aim of this review is to provide an evidence-based overview of acute lower gastrointestinal bleeding in order to improve the prompt diagnosis, effective treatment and overall outcomes for these patients.
Aetiology of lower gastrointestinal bleeding
Following the urgent assessment of a patient’s haemodynamic stability and their adequate resuscitation, the clinical priority for patients presenting to the emergency department with acute gastrointestinal haemorrhage is to identify the bleeding source. Due to the large length of bowel potentially involved this can be a significant diagnostic challenge. Indeed, a major study found that up to 23% of acute cases of lower gastrointestinal bleeds who spontaneously stop bleeding are discharged without a precise diagnosis. The classification guide in Table 1 offers a schematic for identifying aetiologies.
| Classification | Examples |
|---|---|
| Anorectal | Haemorrhoids, varices, fissures, ulcers |
| Diverticulae | Colonic diverticulosis, Meckel’s |
| Vascular | Angiodysplasia, Dieulafoy lesions |
| Inflammatory | Ulcers, colitis, endometriosis |
| Neoplastic | Benign, malignant |
| Traumatic | Direct, pressure, explosion |
Commonly, a digital rectal examination or rigid sigmoidoscopy may reveal acute anorectal pathology such as haemorrhoids, fissures or rectal tumours, normally associated with bright red blood on the surface of stool. Anal fissures are associated with severe pain on defaecation and never cause significant bleeding, but vascular haemorrhoids account for 15 – 30% of acute lower gastrointestinal bleeds and can occasionally cause major haemorrhage. However, brisk rectal bleeding could be the first clinical presentation of rectal varices, especially in patients with known portal hypertension. More intermittent yet severe rectal bleeding in the absence of palpable anorectal lesions may suggest a Dieulafoy lesion, a rare submucosal end arterial defect. These bleed from very small erosions of the mucosa and are often difficult to detect.
In the absence of anorectal pathology, frank bright red bleeding or covering stool generally arises from the left colon. Alternatively, dark rectal bleeding, normally integrated within stool and accompanied by blood clots, is generally from right-sided colonic haemorrhage and is often described as “haematochezia”. Between 25 – 40% of all acute lower gastrointestinal bleeds arise from left colonic diverticular disease. Up to 80% of patients with diverticular bleeding are stable but 3 – 5% require admission to hospital, especially the elderly. Bleeding occurs due to rupture of the vasa recta at the base of diverticulae, probably secondary to vascular distortion or erosion. Contrary to common assumptions, such bleeds are not normally associated with episodes of acute diverticulitis and can lead to major spontaneous acute haemorrhage, especially in patients taking anticoagulants. Fortunately, the majority of diverticular bleeds stop spontaneously, especially once any anticoagulants have been suspended. However, 20 – 30% develop a rebleed during their inpatient stay and 15% bleed again after discharge from hospital. The cause of acute gastrointestinal bleeding is normally confirmed by urgent inpatient or early outpatient colonoscopy and treated by therapeutic endoscopic techniques, medical therapies, or interventional radiology.
Ischaemic colitis tends to occur at watershed areas of compromised lower gastrointestinal vasculature due to arteriosclerosis or embolism. Impacted stool against the colonic mucosa can cause ischaemia with bleeding and/or perforation. Hypervascularity and vascular fragility associated with inflammatory colitis may also cause acute haemorrhage. Lower gastrointestinal bleeds are more common in Crohn’s disease (CD) than in ulcerative colitis (UC) as CD causes deeper penetrating ulcers and has up to a 35% rebleeding rate.
Angiodysplasia refers to arteriovenous malformations in the bowel mucosa or submucosa. Defects are more common in the elderly, often in the caecum, and are associated with aortic stenosis, scleroderma, and use of non-steroidal anti-inflammatory drugs (NSAIDs). A diverse range of rare haemangiomas and telangiectasias are also occasionally identified and are likely to require further specialist investigations to exclude vascular defects elsewhere.
Large numbers of colonoscopies are performed daily as part of investigations for bowel dysfunction, bowel cancer screening programmes and polyp surveillance. Up to 7% of colonic polypectomies can lead to an acute lower gastrointestinal bleed, influenced by patient factors, polyp size and whether diathermy or endo-clips were deployed during the procedure. Urgent colonoscopies investigating acute bleeding also identify colon cancers in approximately 2 – 9% of emergency patients, where either the tumour is directly bleeding or is eroding the adjacent colonic vasculature. Importantly, up to 15% of major acute upper gastrointestinal haemorrhages may manifest as dark or even bright red rectal bleeding without the classic features of melaena, as the rapid transit of intraluminal blood through the gastrointestinal tract occurs before its digestion into acid hematin. For this reason, an emergency upper gastrointestinal endoscopy may be indicated especially in the unstable patient in order to exclude a proximal aetiology and ensure rapid haemostasis.
Assessment of bleeding severity
Rapid estimates of bleeding severity can be obtained from the patient’s haemodynamic status and haemoglobin levels in the emergency department, classifying at risk patients with tools such as the BLEED criteria (see Table 2). If a patient has any BLEED criteria they are classified as high risk, requiring admission to hospital and urgent treatment.
| B | L | E | E | D |
|---|---|---|---|---|
| Bleeding (ongoing) | Low systolic BP | Elevated prothrombin time | Erratic mental state | Disease (unstable, comorbidities) |
Although only around 2 – 3% of patients with acute lower gastrointestinal bleeding present with collapse and severe haemorrhagic shock, up to 25% receive a red blood cell transfusion during admission. The number of transfused units required to stabilise a patient can provide a surrogate estimate of blood loss. A simple guide for intervention relative to estimated bleeding severity is outlined in Table 3, but more discriminatory and accurate scores have been adopted. Scoring systems offer practical guidance for clinical decision making as well as standardised data for audit and improving patient outcomes. For example, the NoBLADS score predicts the risks of acute bleeding severity.
| Severity of bleeding | Intervention |
|---|---|
| Minor | Conservative management |
| Acute on chronic intermittent | Observation +/- early intervention |
| Intermittent with shock | Mandatory urgent intervention |
| Persistent major haemorrhage | Immediate intervention |
Table 4 describes the “Oakland Score” derived from a large UK audit. In this system, a score of less than or equal to 8, in the absence of any other reason for admission, accurately predicts a 95% chance that patients may be discharged safely for subsequent investigations in an early outpatient setting. As a result, acute resources can be optimised, costs limited, and lengths of stay reduced.
| Predictor | Score value |
|---|---|
| Age | |
| <40 | 0 |
| 40-69 | 1 |
| >70 | 2 |
| Gender | |
| Female | 0 |
| Male | 1 |
| Previous LGIB admission | |
| No | 0 |
| Yes | 1 |
| DRE findings | |
| No blood | 0 |
| Blood | 1 |
| Heart rate (HR) | |
| <70 | 0 |
| 70-89 | 1 |
| 90-109 | 2 |
| >110 | 3 |
| Systolic BP (mmHg) | |
| <90 | 5 |
| 90-119 | 4 |
| 120-129 | 3 |
| 130-159 | 2 |
| >160 | 0 |
| Haemoglobin (g/L) | |
| <70 | 22 |
| 70-89 | 17 |
| 90-109 | 13 |
| 110-129 | 8 |
| 130-159 | 4 |
| >160 | 0 |
Role of Radiological Imaging
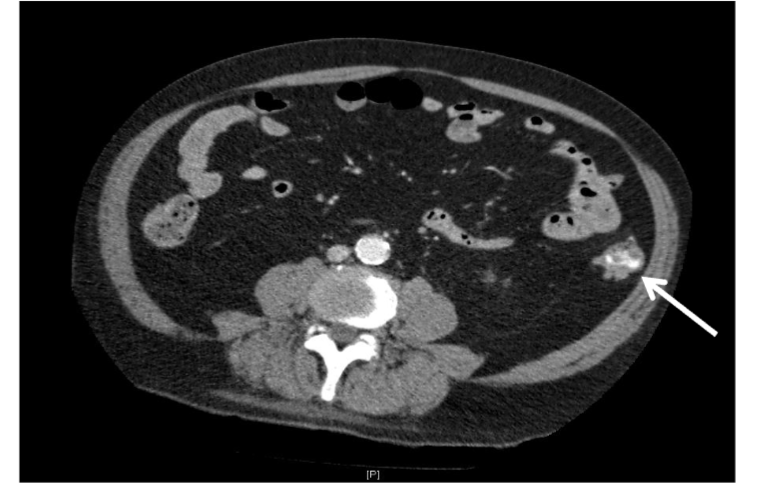
Following clinical assessment, the precise localisation of acute lower gastrointestinal bleeding is now commonly identified radiologically. In the past, radioisotopes such as 99Tc Technecium were used to label red cells for scintigraphy. This technique can detect bleeding as low as 0.1ml/min, but it is no longer widely used as it is time-consuming, labour intensive and does not identify bleeding points as precisely as modern imaging. Most hospitals now have ready access to high quality contrast computer-aided tomography (CT) imaging or diagnostic multi-detector CT angiography for localising bleeding sources. In addition to identifying active bleeding, CT angiography may more accurately clarifies anatomy and can identify tumours >2cm diameter. Extravasated contrast typically appears as diffuse pools of high signal within the lumen of the bowel (see Figure 1). Active bleeding identified by CT angiography can be followed by direct trans-catheter angiography (TAA). Major advances in the speed and quality of software have significantly improved performance. For this reason, contrast-enhanced CT scanning is now the most common radiological modality for the detection of acute lower gastrointestinal bleeding. Three-dimensional software reconstructions of intra-abdominal vessels can also diagnose associated vascular causes, such as mesenteric aneurysms or aorto-enteric fistulas, enabling rapid referral for endoscopic or angio-therapeutic interventions.
The main disadvantage of CT imaging is that the threshold for detection requires a bleeding rate of over 0.5ml/minute and that it is only a diagnostic rather than a therapeutic tool. In addition, some patients may develop anaphylaxis to contrast agents. Previous concerns that large volumes of intravascular contrast may be particularly hazardous to patients with renal impairment are now generally considered lower risk than previously thought.
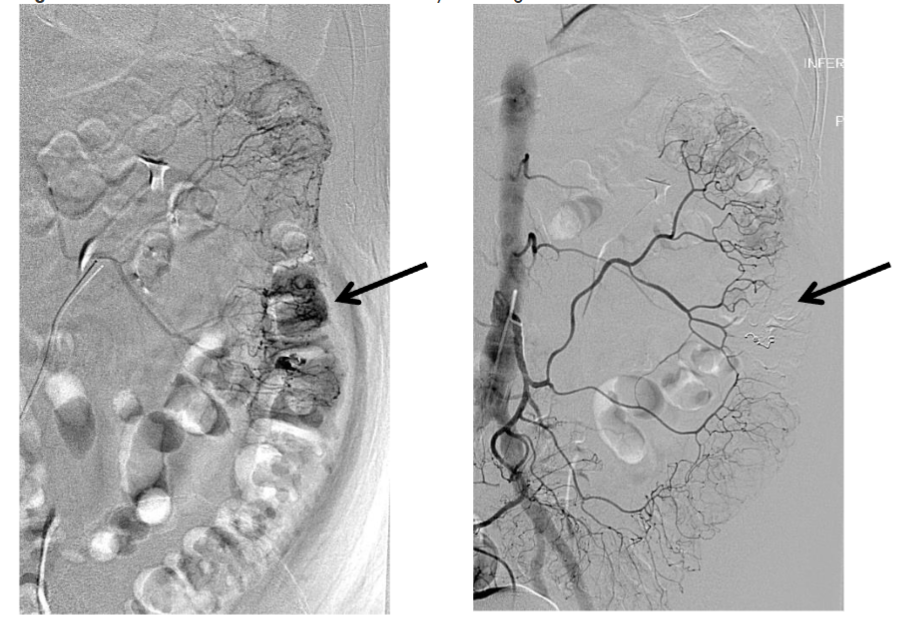
Direct trans-arterial angiography (TAA) is a procedure performed by interventional radiologists so is less widely available than CT angiography, especially out of hours, but has several advantages. The detection of a bleeding point by TAA is still reliant on the patient actively bleeding at a rate of over 0.3ml/minute. However, it accurately localises bleeding to a specific blood vessel in up to 75% of cases and allows minimally invasive therapeutic interventions by super-selective embolization (see Figure 2). This technique normally utilises micro-coils and agents such as N-Butyl cyanoacrylate (NBCA) which rapidly polymerises in contact with blood. Although TAA has an approximately 86 – 98% success rate with complication rates such as ischaemia and rebleeding under 15%, it depends on the availability of the service. Nevertheless, interventional radiology is becoming increasingly adopted in acute hospitals so this technique for treating acute lower gastrointestinal bleeding is likely to rise.
Role of Endoscopy
Upper and lower gastrointestinal endoscopies identify the bleeding source in 42 – 90% of patients with gastrointestinal haemorrhage, so remain the gold standard investigation of acute lower GI bleeds. Acutely, endoscopy is recommended as soon as possible to increase the likelihood of identifying the bleeding source as well as achieving haemostasis, but more stable patients can normally be investigated in an early outpatient setting. Flexible sigmoidoscopy is most commonly employed for bright red rectal bleeding or for suspected diverticular bleeds as it does not require extensive purgation. Where an urgent full colonoscopy is required, visualisation of intra-luminal bleeding points may be improved by the administration of bowel prep orally, via a nasogastric tube, or by local irrigation during the procedure. Effective endoscopic therapies include submucosal adrenaline injections, deployment of metallic clips, thermal or laser ablation, and pro-coagulant sprays. Successful therapeutic endoscopy reduces the need for subsequent angiographic embolization or surgery to under 5% of cases, reduces transfusion requirements, and reduces median length of hospital stay by at least 50%. While some studies have indicated that early colonoscopy may offer little or limited benefits for acute lower gastrointestinal bleeding in general, others have identified which subgroups of patients are most likely to benefit.
Selected stable patients in whom colonoscopy suggests that bleeding is arising proximal to the ileo-caecal junction may be suitable for diagnostic capsule endoscopy. This technique requires the patient to swallow a wireless video capsule which passes through the entire gastrointestinal tract and downloads digital video images for interpretation by an experienced endoscopist. The capsule is generally passed uneventfully but there is up to a 2.5% risk of the capsule becoming entrapped in a stricture or diverticulum. As capsule endoscopy is costly, labour intensive, and non-therapeutic, it is very rarely used for acute lower GI bleeding.
Role of Surgery
With the major improvements in less invasive treatments, emergency surgery for acute lower gastrointestinal bleeding is reserved for unstable patients who have failed alternatives and is now rare. Limited segmental resections are preferred but require accurate localisation of a bleeding point by CT or angiography. Emergency resections have a mortality rate of 5 – 33% and a risk of rebleeding during their hospital admission greater than 40%, mainly due to failure to accurately target the vessel. In the absence of a known bleeding point, a more radical subtotal colectomy can be lifesaving but is associated with a mortality rate of up to 25% as these most haemodynamically unstable patients have normally been delayed getting to the operating theatre while attempting less invasive treatments. Nevertheless, if surgery successfully stops life-threatening haemorrhage and patients survive, subtotal resections often have a complication rate of under 15% and a low risk of rebleeding within 1 year.
Patients on antiplatelets or anticoagulants
A large number of patients presenting with severe acute lower gastrointestinal bleeding have major comorbidities. In a large UK audit, 29.4% of acute patients were taking antiplatelet agents and 15.9% taking other anticoagulants. Bleeding patients on warfarin with mechanical heart valves are particularly challenging and require close collaboration with cardiology and haematology specialists. However, the majority of patients on chronic thromboprophylaxis are taking direct oral anticoagulants (DOACs). These drugs offer more convenient, fixed dose alternatives to warfarin with similar effectiveness at preventing strokes or other embolic events but still have an increased risk of lower GI bleeding. DOACs normally become ineffective after 24 – 48 hours, so patients presenting with acute lower GI bleeding should be admitted, stabilised and managed haematologically by red cell transfusions, fresh frozen plasma and/or cryoprecipitates until safe to proceed. Most patients will stop bleeding without further intervention and can be evaluated for the risks of restarting anticoagulation.
The CRASH2 trial of acute bleeding in trauma patients found that early delivery of the fibrinolytic inhibitor tranexamic acid (TXA) significantly reduced haemorrhagic mortality with no significant increase in thromboembolic complications. As a result, similar studies examined if TXA would be similarly effective for acute gastrointestinal bleeding. However, several studies, such as the large HALT-IT double-blind clinical trial, failed to demonstrate any value of TXA in this context and also raised concerns of an increased risk of seizures. Therefore, TXA is not recommended as a treatment agent for acute lower gastrointestinal bleeding.
Conclusion
Acute lower gastrointestinal bleeding is a major emergency health problem with a wide range of differential diagnoses. Relatively few patients require active treatments and are safe to be diagnosed with outpatient follow up. However, most patients presenting to hospital with acute lower gastrointestinal bleeding are elderly and have a high burden of comorbidities with common antiplatelet or anticoagulant use. Therefore, adverse outcomes in these patients with lower gastrointestinal bleeds are more related to their underlying non-intestinal pathologies rather than the severity of haemorrhage.
Dedicated evidence-based scoring systems are helpful to triage patients presenting with acute lower GI bleeding. These ensure that a larger number of patients avoid admission to hospital, obtain urgent outpatient investigations and optimise resources. Localising the source of acute lower GI bleeding is a clinical priority, so optimised radiological and endoscopic investigations are critical. Therapeutic endoscopies and trans-catheter embolization are becoming more widespread therapeutic tools for persistent lower gastrointestinal haemorrhage, ensuring rapid treatment and avoiding surgery.
Undoubtedly, protocol-driven practice improves outcomes so a number of national and international guidelines have been produced to aid management of patients with acute lower GI bleeds and improve outcomes. Hospitals which regularly admit these patients should have clear pathways for their management and ideally have rapid access to emergency endoscopy and interventional radiology. Further work should generate more validated predictive tools for rebleeding risks, mortality and surgical management. In this regard, modern artificial intelligence programs may play an important role in generating robust protocols.
Conflict of Interest Statement
The author has no conflict of interest to declare.
Funding Statement
None.
Figures
All Figures in this article are from the author’s personal collection of radiological images for teaching purposes and have not been published elsewhere.
References
- Cotter J, Baldaia C, Ferreira M, Macedo G, Pedroto I. Diagnosis and treatment of iron-deficiency anemia in gastrointestinal bleeding: a systematic review. World J Gastroenterol. 2020; 26(45):7242-7257.
- Rockey DC. Occult gastrointestinal bleeding. N Engl J Med. 1999; 341:38-46.
- Zuckerman GR, Prakash C, Askin MP, Lewis BS. AGA technical review on the evaluation and management of occult and obscure gastrointestinal bleeding. Gastroenterology. 2000; 118(1):201-21.
- Oakland K, Guy R, Uneroi R, Hogg R, Mortensen N, et al. Acute lower GI bleeding in the UK: patient characteristics, interventions and outcomes in the first nationwide audit. Gut 2018; 67:654-662.
- Lanas A, Garcia-Rodriquez LA, Polo-Tomas M, Ponce M, Alonso-Abreu I, Perez-Aisa MA, Perez-Gisbert J, Bujanda L, Castro M, Munoz M, Rodrigo L, Calvet X, Del-Pino D, Garcia S. Time trends and impact of upper and lower gastrointestinal bleeding and perforation in clinical practice. Am J Gastroenterol. 2009; 104(7):1633-1641.
- Moss AJ, Tuffaha H, Malik A. Lower GI bleeding: a review of current management, controversies and advances. Int J Colorectal Dis. 2016; 31(2):175-188.
- Singh M, Chiang J, Seah A, Liu N, Mathew R, Mathur S. A clinical predictive model for risk stratification of patients with severe acute lower gastrointestinal bleeding. World J Emerg Surg. 2021; 16(1):58.
- Siebenhüner K, Blaser J, Nowak A, Cheetham M, Mueller BU, Battegay E, Beeler PE. Comorbidities associated with worse outcomes among inpatients admitted for acute gastrointestinal bleeding. Dig Dis Sci. 2022; 67(8):3938-3947.
- Newman J, Fitzgerald JEF, Gupta S, von Roon AC, Sigurdsson HH, Allen-Mersh TG. Outcome predictors in acute surgical admissions for lower gastrointestinal bleeding. Colorectal Dis. 2012; 14:1020-1026.
- Nagata N., Niikura R., Aoki T. et al. Risk factors for adverse in-hospital outcomes in acute colonic diverticular haemorrhage. World J Gastroenterol. 2015; 21:10697-10703.
- Strate LL, Ayanian JZ, Kotler G, Syngal S. Risk factors for mortality in lower intestinal bleeding. Clin Gastro Hepatol. 2008; 6:1004-1010.
- Fujita M, Manabe N, Murao T, Suehiro M, Tanikawa T, Nakamura J, Ishii K, Monden S, Uji E, Misawa H, Ninomiya T, Sasahira M, Chikaishi M, Yo S, Osawa M, Katsumata R, Ayaki M, Ishii M, Kawamoto H, Shiotani A, Hata J, Haruma K. Differences between patients with inpatient-onset and outpatient-onset acute lower gastrointestinal bleeding: an observational study. J Gastroenterol Hepatol. 2023; 38(5):775-782.
- Khan A, Kanters AE. Management of acute haemorrhoidal crisis: evaluation, treatment, and special considerations. Clin Colon Rectal Surg. 2023; 37(6):381-386.
- Al Khalloufi K, Laiyemo AO. Management of rectal varices in portal hypertension. World J Hepatol. 2015; 7(30):2992-2998.
- Inayat F, Hussain A, Yahya S, Weissman S, Sarfraz N, Faisal MS, Riaz I, Saleem S, Saif MW. Rectal Dieulafoy’s lesion: a comprehensive review of patient characteristics, presentation patterns, diagnosis, management, and clinical outcomes. Transl Gastroenterol Hepatol. 2022; 7(10): doi:10.21037/tgh.2020.02.17.
- Ilyas MIM, Szilagy EJ. Management of diverticular bleeding: evaluation, stabilisation, intervention, and recurrence of bleeding and indications for resection after control of bleeding. Clin Colon Rectal Surg. 2018; 31(4):243-250.
- Shimomura A, Nagata N, Shimbo T, Sakurai T, Moriyasu S, Okubo H, Watanabe K, Yokoi C, Akiyama J, Uemara N. New predictive model for acute gastrointestinal bleeding in patients taking oral anticoagulants: a cohort study. J Gastroenterol Hepatol.
- Sato Y, Aoki T, Sadashima E, Nakamoto Y, Kobayashi K, Yamauchi A, Yamada A, Omori J, Ikeya T, Aoyama T, Tominaga N, Kishino T, Ishii N, Sawada T, et al. Long-term risks of recurrence after hospital discharge for acute lower gastrointestinal bleeding: A large nationwide cohort study. Clin Gastroenterol Hepatol. 2023; 21(13):3258-3269.
- Cirrochi R, Grassi V, Cavaliere D, Renzi C, Tabola R, Poli G, Avenia S, Farinella E, Arezzo A, Vettoretto N, D’Andrea V, Binda GA, Fingerhut A. New Trends in Acute Management of Colonic Diverticular Bleeding: A Systematic Review. Medicine. 2015; 94(44):1710.
- Mosli M, Aldabbagh A, Aseeri H, Alqusair S, Jawa H, Alsahafi M, Qari Y. The diagnostic yield of urgent colonoscopy in acute lower gastrointestinal bleeding. Acta Gastroenterol Belg. 2020; 83(2):265-270.
- Meine GC, Santo P, Delgado LM, Brennan GT. Endoscopic therapies for colonic diverticular bleeding: a systematic review and meta-analysis. Surg Endosc. 2025; doi: 10.1007/s00464-025-12520-8.
- Newman J, Cooper MA. Lower gastrointestinal bleeding and ischaemic colitis. Can J Gastroenterol. 2002; 16(9):597-600.
- Kim DS, Yoon J, Kim YJ, Lee JW, Hong SW, Hwang HW, Park SH, Yang DH, Ye BD, Byeon JS, Myung SJ, Yang SK. Risk factors for rebleeding in Crohn’s disease patients with acute severe lower gastrointestinal bleeding: with special reference to the role of anti-tumour necrosis factor therapy. J Gastroenterol Hepatol. 2021; 36(9):2455-2462.
- Tu T, Chen M, Zeng Z, Lin J, Chen L, Liu C, Zhuang X. A comprehensive review and update on acute severe lower gastrointestinal bleeding in Crohn’s disease: a management algorithm. Gastroenterol Report. 2024; doi.org/10.1093/gastro/goae099.
- Bermont A, Abu-Freha N, Cohen DL, Galion FA, Aminov R, Shirin H. Epidemiology and risk factors for angiodysplasia of the upper and lower gastrointestinal tract: a large population-based study. Dig Liver Dis. 2025; 57(1):220-224.
- Tsoutsouki J, Faidon-Marios L, Mason S, Smith M, Sinha L. A rare cause of GI bleeding in a patient with cutaneous vascular malformations. Gut 2016; 65:1792.
- Li JA, Zhong LL, Li B, Jiang DQ, Zhao YL. Diffuse telangiectasia of the colon: a case report. Medicine. 2020; 99(34):21106.