






Environmental Risk Factors in Allergic Diseases
Environmental risk Factors in Airway Allergic Diseases
Prof. H Paramesh1
- Pediatric Pulmonologist and Environmentalist; Physician Scientist Divecha Centre for Climate Change; Indian Institute of Science Bangalore.
OPEN ACCESS
PUBLISHED: 30 October 2024
CITATION: Paramesh, H. 2024. Environmental risk Factors in Airway Allergic Diseases. Medical Research Archives. doi:10.18103/mra.v12i7.2197
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI: https://doi.org/10.18103/mra.v12i10.5799
ISSN 2375-1924
ABSTRACT
Our environment is the natural surroundings we exist in relation to the weather condition. Air pollution, global warming and climate change are interrelated causing weather changes. 70% of environmental pollution is from air pollution and 70% of non-communicable diseases are from air pollution. The earliest onset non communicable environmental diseases are airway allergic diseases in particular asthma with significant psycho-socio economic burden.[1,2]
The reason for the increase in allergic diseases, in particular asthma is an imbalance in our environment. Firstly, we are losing the threshold of our protection by depriving the protective germs in our environment, changing our traditional food habits and adopting the western lifestyle in living, Secondly from higher exposure to triggers- air pollution, global warming and climate change, increase in viral respiratory infections and less access to health care facilities.[3]
The recent World Health Organisation (W.H.O) report in May 2024 says that asthma is affected nearly 262 million people with mortality of 4,55,000 in the year 2019. It is observed more in lower- and middle-income countries and under diagnosis with undertreatment are the cause. Air pollution is the important risk factor for asthma hence it is included in the W.H.O. global action plan to prevent and control with United Nations by 2030.[4]
In this article we tend to highlight the environmental risk factors that influence the allergic diseases and its comorbidities in relation to air pollution, temperature change and sunlight; change in humidity and seasons; thunderstorm; draught; occupation; artificial bright light and sensitize on the measures to mitigate airway allergies.
Introduction
Airway allergic diseases are global pandemic causing high morbidity and mortality from environment pollution. The intension of this article is to sensitize the various environmental risk factors which initiates and triggers allergic airway diseases and to help the clinicians to update. Airway allergies like asthma, allergic rhinitis are the earliest onset environmental non communicable chronic respiratory diseases with significant psycho socio economic burden globally1,21,2.
The reason for the increase in allergic diseases is due to losing our threshold of protection from depriving the protective germs in our environment, changing our traditional food habits and western lifestyle of living. In addition, there is higher exposure to triggers to air pollution, global warming, climate change, increase in viral respiratory infections and less access to healthcare facilities33.
Recent worldwide reveals that asthma is observed more in lower- and middle-income countries affecting 262 million people with mortality of 4,55,000 cases in the year 2019 with under diagnosis and undertreatment. Air pollution is the major risk factor. W.H.O included it in global health plan of United Nations by 203044.
Impact of air pollution allergic airway diseases and comorbidities
Air pollution is an invisible killer having an impact from womb to tomb. The global mortality shows 43% of chronic lung disease; 29% of lung cancer; 25% of heart diseases; 24% of stroke55.
Air pollutants are aero biologicals, chemical pollutants like particles and gases. The Aerobiologicals which trigger or initiate asthma in our observation are – dust mites- 50%; cockroaches -25%; Fungi -7.5%; pollens -7.5%; pet danders -5%; virus and bacteria -40%66.
The chemical components are from outdoor and indoor air pollutants like particulate matter (pm) Nitrogen oxide (NOx); Volatile organic compounds (VoC); Carbon monoxide (CO); Sulphur dioxide (SO₂); Ozone at ground level (O₃), ptbutyl styrene (TBS), Diesel exhaust particles (DEP). The primary chemical pollutants are NOX, VOC, CO, SO₂, TBS, PM. The secondary pollutants are PM, O₃ and DEP77.
When we are talking about chemical pollutants it is important to know the size of the particulate matter (PM) and water solubility of the gas to predict their impact on the respiratory tract.
The PM 10µ and above predominantly deposit on upper airway, PM 2.5µ to 10 µ deposit in lower airways, PM less than 2µ cross the lung tissue and enter the blood stream and distribute all over the body as confirmed by radioisotope study. While water soluble gases SO₂, Chlorine, Ammonia and Aldehydes deposit in upper airways. Medium water-soluble gas Ozone (O₃) deposit in lower airways. Low water-soluble gas Nitrogen dioxide (NO₂) will cross the lungs tissue and enter the blood stream and impact all organs.
Vulnerable groups from air pollution
The children are the most vulnerable group since their immune and antioxidant defense is in developing phase, they breath more air and spend more time to play outside.
The elderly who have respiratory comorbidities and high prevalence of chronic cough are the next vulnerable group. One should recollect that the lung functions start decreasing by 15–20 ml per year in vital capacity, after the age of 25 years.
The urban population living in high rise buildings, working in ill ventilated offices and their mode of transport tend to suffer more with poor air quality and poor ventilation. The affected population for air pollution initially show no symptoms with subclinical effect as the pollution increases then they start showing symptoms with decline in lung function with increase in usage of medicine, increase in hospital visits, emergency visits and hospitalization followed by death88. It is also interesting to know that the healthcare industry contributes 4.4% of the air pollution for global climate change from incinerators, boilers, generators, sterilization units, refrigeration, laboratory fume hood and anesthesia department with nitrous oxide and halogenated anesthetic agents99.
The traffic derived air pollution exposure to pregnant mothers has its impact on fetus with SPM <2.5µ which crosses the lung layers to blood stream creates small clots with platelet aggregation and get deposited in the placenta depriving the fetal nutrition. This placental coagulopathy problem depending on the severity will lead to still births, prematurity and small for date children. These children are born with fixed airway obstruction causing persistent asthma and chronic obstructive pulmonary diseases (COPD) later in life. The ante natal exposure synergizes with post-natal exposure causing recurrent wheeze, bronchiolitis and asthma1010.
The increased air quality index values from PM2.5 is significantly exaggerating asthma and decrease the pulmonary function testing in the absence of provoking viral infection causing epithelial tissue Kallikreins, mucus hyper secretions and barrier functions. The asthma is exacerbated by 33% in urban impoverished area compared to suburban population with 11% exacerbations. The mortality from Ozone (O₃) is increased by 46% between 2000–20191111.
Local magnitude of allergic airway diseases and comorbidities12
The diagnosis of allergic rhinitis and comorbidities are made on clinical evaluation as pertaining to the ADEX module prepared by allergy immunology chapter of Indian Academy of Pediatrics, Asthma was diagnosed by proving reversible airway by pulmonary function before and after salbutamol inhalation1919.
Allergic rhinitis: In general pediatric population the allergic rhinitis is increased from 22.5% to 50% between 1994 to 2022 and in asthmatic children it is increased from 75% to 100% between 1999 to 2022 in the city of Bengaluru as shown in Fig 1.
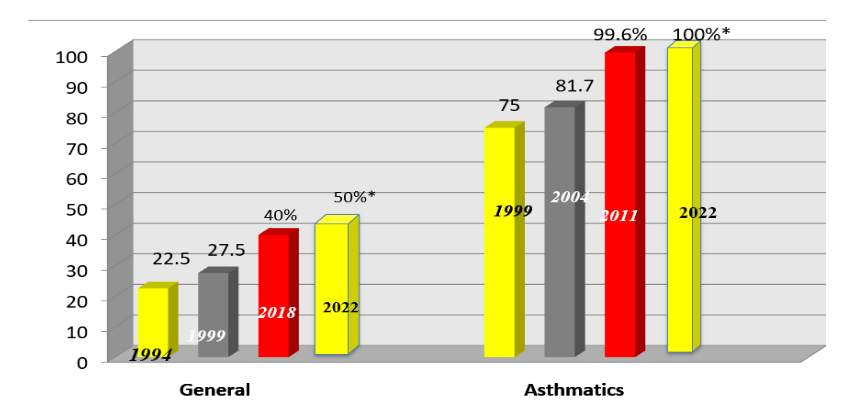
Fig – 1: Allergic rhinitis in general pediatrics population and in asthmatic children
The comorbidities of allergic rhinitis are otitis media, in general pediatric population is 9%; In children with allergic rhinitis is 22.5%; 1 in 5 children have glue ear and is the most common cause for deafness. Regarding sinusitis the prevalence is in general pediatrics is 1% in allergic rhinitis children it is 34.8%,[13,14]. The prevalence of asthma in children was 9% in 1979 steadily gone up to 29.5% in 2 decades in 1999. It was hypothesized due to change in the demography of the city and air pollution from increased number of industries, increased density of population and increased vehicular emission. 5 Years later in the year 2004 asthma prevalence dropped to 26.7%. Similar observation is made in other countries. The consensus of global experts was the genetically inherited population is saturated, in future one can see small spikes but continued exposure of population can lead to increase in persistent asthma and persistent severe asthma. For sure we have observed the persistent asthma and persistent severe asthma increased from 22.5% to 72.5% and persistent severe asthma from 6.5% to 11% between 1999 to 2009 respectively1515 as shown in Fig–2.
Figure 2: Prevalence of asthma in Bangalore from 1972 to 2009
Fig – 2: Prevalence of asthma in Bangalore from 1979 to 2009
Round the world preschool wheeze
The preschool wheeze in children is a global burden. All the global experts felt that under five wheeze is increasing. Our observation is that 77.5% in children under 5 and 26.3% in children less than 1 year are wheezers and further increasing1616. It is also observed that the prenatal exposure of SPM from 35.5µ to 53.4µ in the air resulted in four fold increase in the wheeze in infants1717.
Living close to busy roads in Switzerland increase the sensitization by 2 folds to pollens1818. The risk of positive skin tests increased by 70% in people living in moderately polluted towns against neighboring country area1919. .
Chronic cough as a comorbidity in airway allergies
Chronic cough lasting more than 2 weeks in children is a major comorbidity in asthma and allergic rhinitis.The prevalence was 8% in 1999 and gone up to 21.25% in 2017, and there is 0.5% increase of prevalence per year2020 as shown in Fig–3. Evaluation of chronic cough we found that asthma was the cause in 79.21% while allergic rhinosinusitis 10.52% in the year 1999. Now it has changed in the year 2017 where allergic rhinosinusitis was 70.25%, asthma was 45.25% as shown in the Figure – 4 It is noted that air pollution induced allergic rhinitis and nasal health in India is a concern. The expert consensus/opinion was to take steps to reduce allergens at home/office include improving ventilation, bedroom hygiene and smart cleaning. Keeping indoor plants and expose them to sunlight once a week which also help in improving air quality2121.
Impact of increase temperature / summer season on asthma:
Our observation in the city of Bengaluru, is that in summer season with increased temperature, 2.8% of children use to suffer from asthma in the year 1994, it is steadily increased to 19.8% in the year 2004. We hypothesized that it is due to secondary ozone production by the action of sunlight on vehicular emission. Ozone is a secondary pollutant and potent airway inflammatory agent with cumulative effect2222.

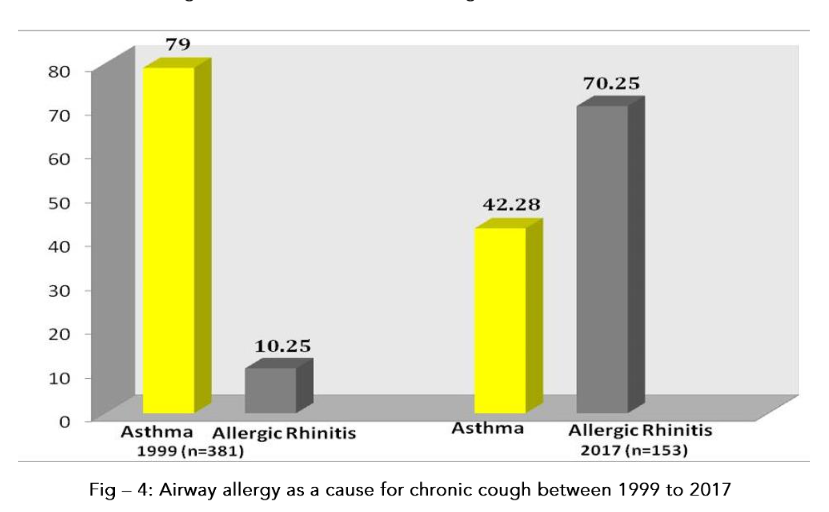
Fig – 4: Airway allergy as a cause for chronic cough between 1999 to 2017
Global warming enhanced pollen allergies globally from three reasons – By increase carbon dioxide in atmosphere, there is prolonged flowering season causing prolonged asthma symptoms. New weed Ambrosia is seen in Scandinavian countries causing new allergies. Heat and sunlight increase the ozone production from vehicular emission and stress on plants produces potent allergens. If the pollens are coated with diesel particles, they are 50 times more potent⁽²³⁾.
Impact of Outdoor Air Pollution on Allergic Diseases
Our airway doctors 1045 traffic police officers and 1160 non traffic officers show, the traffic police have 26.12% asthma traffic and 27% chronic cough compared to non-traffic police having asthma 10.6% and chronic cough 20%.
Impact of change in humidity and temperature:
The increase in humidity and warm temperature will increase the allergic airway diseases from dust mites.
Decrease humidity increase temperature increase the pollen allergies. The tree pollens concentration will increase from April to June, grass pollens from July to November and weeds pollen from November to January. 7.5% of children are sensitive to pollens and fungi as proved by skin testing.
The increased humidity and decreased temperature increase fungal allergies. Fungi are both outdoor and indoor aerobiological pollutant commonly found in wet, ill ventilated places in a shower curtains and basements2121.
Impact of thunderstorm on allergic disease:
During thunder storms in wet conditions the pollen grains will rupture by osmotic shock and release part of their cytoplasmic content into the atmosphere and trigger asthma leading to increase in visits to emergency room of the hospital2424. In addition, the Didymella fungus will release spores during thunderstorms.
Impact of draught on airway diseases:
During draught time the asthma is increased from more dust particles in the air. In addition, during wildfires season allergic airway diseases are doubled in number and intensity of the smoke will increase allergic rhinitis and asthma. Wildfire in Tundra (Rolling treeless ground found in cold regions) is increased 9 times between 1996-2015 and the smoke triggers more asthma2525.
Impact of occupation on allergic disease:
-
Cooking indoor in ill ventilated huts using agricultural waste in the rural areas 8 km away from main road resulted in girls suffering more asthma who are helping the mother in cooking while boys are out helping the father in the agriculture farm66.
-
Children of heavy traffic school area – 19.36% of them suffer asthma while in less traffic school area – 11.15%66.
-
It is also noted that children working in the auto garages get more asthma with decrease lung functions from lead poisoning. The frequency respiratory symptoms correlate with blood and Urine lead level2626.
-
Exposure to organophosphates pesticides and herbicides rodenticide is associated with increase asthma both atopic and non atopic phenotypes2727.
-
Rag picking children with asthma: It is observed that the rag picking children have higher incidence of asthma from inhalation of smoke and dust exposure from burning of garbage disposal, in addition exposure to smoke from burning of the garbage disposal.
-
Poultry farm workers: People working in poultry farming area have asthma prevalence of 67% due to inhalation fungus grown in bird droppings where the cleaning happens once or twice a week and their pet ownership is only 1%2828.
-
Pets rearing in the house and airway allergy:
The pet ownership in Bengaluru was 4.25%; 5% and 5.4% correspondingly asthma was 9%; 29.5% and 25.5% during 1979; 1999, and 2009 respectively. 68% are dogs, 24.2% are cats and 7.8% are birds. There is no correlation in relation to pet ownership and prevalence of asthma2929 as shown in Table – 1.
In the year 2018 GINA recommended having 2 pets in the house to reduce asthma episodes since pets are stress busters, the endotoxin helps in TH₁ stimulation instead of TH₂ stimulation and protects the people from allergy3131.
Table 1: Prevalence of Asthma / Pet Ownership
| Population | No. Studied | % of Asthma | % Pet Ownership |
|---|---|---|---|
| Urban school children | 5570 | 16.63 | 5.12 |
| Rural school children | 990 | 5 | 7.5 |
| Traffic police | 1045 | 26.12 | 6.2 |
| Non-Traffic police | 1160 | 14.9 | 2.4 |
| Agri-farm workers | 59 | 15.6 | 42.3 |
| Poultry farm workers | 54 | 68.5 | 1.0 |
I have started pet therapy in children with persistent asthma who have stressful situation and having satellite families. It was counselled that the child should take care of the pets this lessens the addiction of videogames, with excellent feed backs.
Impact of air pollution on allergic airway diseases in traffic police officers:
Our study on 1045 traffic police officers and 1160 non traffic officers shows, the traffic police have 26.12% asthma, 10.7% allergic rhinitis and 27% chronic cough compared to non-traffic police having asthma 14.9%, allergic rhinitis 4% and chronic cough 14% respectively3131.
This was discussed in the parliament and recommended face masks for traffic police personnel in the year 1999.
Impact of tobacco smoke on allergic airway diseases:
The prevalence of asthma in a non-smoking house is 8% while one person smokes in the house it is 22.8%. The tobacco smoking habit is 41% of urban children in the age group of 10–17 years (n=3078), in rural children, 21.8% (n=2194) of agriculture farm workers 28% and 2% of rural farm working women; 36% of urban club going women of high society. This work helped to ban tobacco smoking in public places in our state Karnataka in the year 2001, and later National policy in 20033232.
Impact of chemicals used to clean swimming pool on asthma:
Use of Chlorine to clean swimming pools generate harmful byproducts like Chloramine, Trihalomethane which triggers asthma. Ozone molecules are 3500 times faster in killing bacteria and viruses and not been linked to respiratory problems like asthma and bronchitis. The Ozone cleaned pool is always better for asthmatic children3333.
Impact of artificial light pollution (ALP) on allergic diseases:
Artificial light pollution severely disrupts the biological cycle (Circadian Rhythm) of plants, insects, nocturnal animals and humans as well. The airway diameter is directly controlled by circadian rhythm and can exacerbate asthma and other allergic diseases. The night shift work group have been associated with worsened asthma condition3434.
Preventive measures to control allergic diseases in general and specific issues:
General Issues:
Environmental issues with clean air for maternal environment, placental health, fetal health, children and adolescent environment, encouraging traditional food habits and living in good cross ventilated house. To tackle driving forces – Industrialization: Rapid urbanization, safe energy, excess population growth, pervasive poverty and inequality, non-sustainable consumption and transboundary chemical transport.
Specific issues:
Avoid maternal obesity and weight gain. 1 kg/m² increase in BMI is associated with 2 to 3% risk of asthma in newborn children. Avoid maternal smoking, encourage natural delivery and avoid ‘C’ section. Avoid use of antibiotics in pregnancy and young children. Avoid frequent use of paracetamol which depletes the glutathione in airways and increases oxidative stress. Avoid maternal distress during pregnancy and child’s early life. Avoid obesity in children, recommend pets to relieve stress and traditional food habits3535.
Obesity is a risk factor for asthma, one has to be cautious in eating Ultra Processed Foods (UPF). The ultra processed food are being energy rich poor in nutritional profiles. We need to focus on vulnerable children and low income group who are disproportionately affected by consumption of ultra processed food3434.
The future climate change depends on how effectively we reduce the anthropogenic greenhouse gases. Our concern should focus on preventing airway allergic diseases.
“Children’s are disproportionately vulnerable suffering most of the effects now and later in the future.”
Conflict of Interest
None
Acknowledgements
None
References
1. H Paramesh, Air pollution and allergic airway diseases: Social determinants and sustainability in the control and prevention. Indian J pediatric (April 2018) 85 (4): 284-294
2. Paramesh Haralappa, Air pollution: Impact on children Health: Knowledge into action, Jourl child Adolesc Health 2020; 4 (2):32-37
3. H Paramesh, Social determinants of health: Past, present and Future. Current Science 2019: 116 (7)
4. W.H.O, UN report n asthma https//wwwint;Newsroom.2024 , May 6th
5. W.H.O, UN Breath of life : Clean air, healthy future 2017 https://breathelife2030.org/flat-html/
6. H Paramesh, Epidemiology of asthma in India Ind J Pediatrics 2002 Apr;69(4):309-12. doi: 10.1007/BF02723216.
7. Naclerio R, Ansolguib Int, Bosquet J etal International expert consensus on the management of allergic rhinitis (AR) aggravated by air pollutants 2020 Mar; 13(3): 100106. Published online 2020 Apr 3. doi: 10.1016/j.waojou.2020.100106
8. Vannan Kandi Vijayan, H Paramesh, Sandeep Salvi, Anilkumar Dalal. Enhancing indoor air quality -The air filter advantage Lung India Sep – Oct 2015, Vol 32, Issue 5
9. H Paramesh, DJ Christopher, Jyothi S Menon, Chapter 13 on Air pollution climate change and the health sector: Linkage and solutions 2021
10. Norrice M Liu, Jonathan Grigg. Diesel, children and respiratory disease. B.M.J Pediatric open 2018; doi:10.1136/bmjpo-2017-000210
11. Matthew C Altman 1, Meyer Kattan 2, George T O’Connor 3 et al Associations between outdoor air pollutants and non-viral asthma exacerbations and airway inflammatory responses in children and adolescents living in urban areas in the USA: a retrospective secondary analysis 2023 Jan; Lancet 7(1):e33-e44. doi: 10.1016/S2542-5196(22)00302-3
12. H Paramesh Air pollution climate change on lung health editorial Current Science 2022 Vol 122 No.5
13. H Paramesh Indoor Air pollution and human health editorial Current Science 2023,vol 124; No.1
14. H Paramesh Indian Academy of Pediatric textbook 7th edition 2019 publisher Jaypee Brothers pages 654- 667
15. H Paramesh et al Lancet respiratory 2017 www. www.thelancet.com/respiratory
16. Weislow Jedry Chowski et al Intl. Jourl. of Environment and health : 2008 Vol 2, issue 3-4
17. Wyler C et al Exposure to Motor Vehicle Traffic and Allergic Sensitization epidemiology 2000; Vol. 11, No. 4, Jul., 2000
18. Braback L, et al Atopic sensitization and respiratory symptoms among Polish and Swedish school children clinical and exp. Allergy 1994; 24: 826-835
19. H Paramesh, Nimain C Mohanty, Remesh kumar, Pramod kumar et al chronic cough in pediatric practice (ADEX NEXT).NIJP Index Copernicus International Dec 2017, Vol 6, Issue 4; Page 230-243
20. Paramesh H, Asok Mahashur, Deepak Talwar, Sameer Bhargava et al pollution induced rhinitis and nasal health in India. Journal of the Indian Medical Association Dec 2021; Vol 119; No.12
21. Haralappa Paramesh Asthma in children: Seasonal variations Int. Jour, Environment and Health 2008;Vol2, No 3-4
22. Tibbets J.H Air quality and climate change: A delicate balance environm health perspect 2015; 123;A 48-53
23. D’Amato G et al Environmental risk factors and allergic bronchial asthma September 2005 https://doi.org/10.1111/j.13652222.2005.02328.x
24. Intergovernmental panel on climate change (IPCC report 2021) https//www.ipcc.ch>report sept 2016
25. Robert A.EHI, Harvard annual endowment report -https://finance.harvard.edu/endowment
26. Md.Raza Khazdir Et al. Respiratory Symptoms and Pulmonary Function Testes in Lead Exposed Workers Iran Red Crescent Med.J 2012 Nov.14 (11):737-742
27. H Paramesh Environmental Health of Children: Time to Translate Knowledge into Action Ind J. Pediatrics 2018’ 85 (4) 249-294
28. H Paramesh Outdoor and Indoor air pollution on respiratory health. Advances in respiratory medicine. Academy respiratory medicine 2013 Pg 1-10
29. H Paramesh. Asthma and the Environment. Supplement-Indian J Pediatr 2006, 73: 551-555
30. Global Strategy for Asthma Management and Prevention Updated 2018 – Global Initiative for Asthma (GINA 2018)
31. H Paramesh, Allergic disorders in the working environment of traffic and non traffic police personnel. XI National symposium on environment BARC- 2002 Pg 156-157
32. H Paramesh International conference on Environment and Child Health (INCHES) I Bengaluru proceedings 2010
33. Roda pool services. Why ozone is the healthiest option for your pool 10 Aug 2022. https://wwwrodapools.com,au/whyc ozone is the pool
34. H. Paramesh* and Joshitha Sankam Implications of light pollution on human health and the environment: insights for the Indian medical and scientific community Current Science, September 2023 Vol. 125, No. 5, 10
35. Global Initiative of Asthma 2024 https://ginasthma.org/2024-report/
36. Besley M, Sraut B; Mejean S et al. Ultra processed food intake in association with BMI change and risk of overweight and obesity. A prospective analysis of the French Nutrient-Sante Cohort Plos Med. 2020, 17(8)e 1003256.